
Abstract
Purpose of Review
The COVID-19 pandemic changed people’s lifestyles and such changed lifestyles included the potential of increasing addictive behaviors. The present systematic review and meta-analysis aimed to estimate the prevalence of different behavioral addictions (i.e., internet addiction, smartphone addiction, gaming addiction, social media addiction, food addiction, exercise addiction, gambling addiction, and shopping addiction) both overall and separately.
Recent Findings
Four databases (PubMed, Scopus, ISI Web of Knowledge, and ProQuest) were searched. Peer-reviewed papers published in English between December 2019 and July 2022 were reviewed and analyzed. Search terms were selected using PECO-S criteria: population (no limitation in participants’ characteristics), exposure (COVID-19 pandemic), comparison (healthy populations), outcome (frequency or prevalence of behavioral addiction), and study design (observational study). A total of 94 studies with 237,657 participants from 40 different countries (mean age 25.02 years; 57.41% females). The overall prevalence of behavioral addiction irrespective of addiction type (after correcting for publication bias) was 11.1% (95% CI: 5.4 to 16.8%). The prevalence rates for each separate behavioral addiction (after correcting for publication bias) were 10.6% for internet addiction, 30.7% for smartphone addiction, 5.3% for gaming addiction, 15.1% for social media addiction, 21% for food addiction, 9.4% for sex addiction, 7% for exercise addiction, 7.2% for gambling addiction, and 7.2% for shopping addiction. In the lockdown periods, prevalence of food addiction, gaming addiction, and social media addiction was higher compared to non-lockdown periods. Smartphone and social media addiction was associated with methodological quality of studies (i.e., the higher the risk of boas, the higher the prevalence rate). Other associated factors of social media addiction were the percentage of female participants, mean age of participants, percentage of individuals using the internet in country, and developing status of country. The percentage of individuals in the population using the internet was associated with all the prevalence of behavioral addiction overall and the prevalence of sex addiction and gambling addiction. Gaming addiction prevalence was associated with data collection method (online vs. other methods) that is gaming addiction prevalence was much lower using online methods to collect the data.
Summary
Behavioral addictions appeared to be potential health issues during the COVID-19 pandemic. Healthcare providers and government authorities should foster some campaigns that assist people in coping with stress during COVID-19 pandemics to prevent them from developing behavioral addictions during COVID-19 and subsequent pandemics.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Numerous research studies have been conducted since the advent of the COVID-19 pandemic to identify the various effects and impacts of this new disease [1]. The COVID-19 pandemic has had a rapid and varied impact on many aspects of the personal, family, social, occupational, and economic lives of many people [2,3,4,5,6]. Social, financial, health, job, and other epidemic-related stressors may motivate individuals to engage in potentially addictive behaviors, including internet use [7], gambling [8], online shopping [9•], online gaming [10], eating [11], exercise [12], and even work [13]. Such addictive behaviors could be viewed as a type of coping strategies for individuals to shift their attention from fear, anxiety, and/or worry about COVID-19 to other activities. Moreover, given that some strong and unprecedented policies in COVID-19 infection control have been implemented (e.g., lockdowns, quarantine, and closures of educational and occupational buildings), individuals were forced to live in a lifestyle they had never experienced before [14,15,16]. Therefore, these potentially addictive behaviors may also have helped individuals to cope with the new lifestyles they experienced during the COVID-19 pandemic.
As proposed in the Interaction of Person-Affect-Cognition-Execution (I-PACE) model [17], individuals engage in problematic internet use behaviors (potentially a type of addiction) because they can use activities on the internet to cope with their psychological distress. Subsequently, individuals can get themselves into a vicious cycle where they engage in internet use to cope with psychological distress, but then being on the internet all the time causes conflicts in their lives, and the only way to deal with the conflicts is to spend more time on the internet. For a minority of individuals, this could develop into an internet addiction. The same mechanisms could also explain why other potentially addictive behaviors may have been used by individuals during the COVID-19 pandemic (i.e., they use these behaviors to cope with the high levels of psychological distress caused by COVID-19).
The COVID-19 pandemic has provided an unprecedented opportunity for researchers worldwide to study the impact of stressful life events on individuals’ psychological responses and addictive behaviors [18]. During the COVID-19 pandemic, various measures were taken to control the disease and reduce mortality, including travel restrictions and quarantine, as well as the closure of schools, public spaces, and workplaces [19]. During this period, young people were forced to spend large amounts of daily time in front of screens such as tablets, smartphones, desktops, and televisions just so that they could continue to be educated [20, 21].
Spending time online among young people has traditionally been leisure-related. According to a German study, children between the ages of 10 and 17 years played significantly more video games during quarantine vs. pre-pandemic times [22]. Moreover, other studies have reported the increased time spent on internet-related activities (such as gaming, social media use, and smartphone use) during the pandemic compared to time spent online before it [23,24,25,26]. This has been of concern in relation to the use of technology and subsequent addictive behaviors [27,28,29]. Therefore, it is important to understand the severity of such addictive behaviors during the COVID-19 pandemic.
Even before the COVID-19 pandemic, evidence has been cumulated to indicate the important issues of behavioral addictions. More specifically, evidence before the pandemic shows that internet addiction had a prevalence rate of 6.0% (95% CI 5.1–6.9) in a meta-analysis [30]; gaming addiction had a prevalence rate of about 6.0% in a meta-analysis [31]; gambling addiction had a prevalence rate between 2.7 and 4.2% in a meta-analysis [32]; shopping addiction had a prevalence rate of 4.9% (95% CI 3.4–6.9) [33]; food addiction had a prevalence rate of 16.2% (95% CI 13.6–19.3) in a meta-analysis [34]; exercise addiction had a prevalence rate about 3% in a narrative review [35]; social media addiction had a prevalence rate between 1.6 and 34.0% in a narrative review [36]; and smartphone addiction had a prevalence rate of 23.3% (95% CI 14.0–31.2) in a meta-analysis [37].
Apart from the rates of prevalence, empirical evidence and discussions prior to the COVID-19 pandemic show that examining these behavioral addictions is important. For example, the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) has begun to acknowledge the importance of behavioral addictions [38, 39], and the social impacts of behavioral addictions have led to growing interest that need further evidence investigating its pathophysiological mechanism [40,41,42], comorbidity between psychiatric disorders and behavioral addictions [43, 44], and the potential treatments of behavioral addictions [45, 46]. Therefore, the evidence and discussions prior to COVID-19 pandemic additionally support the importance of investigating behavioral addictions during the pandemic.
To the best of the present authors’ knowledge, there has been no previous systematic review and meta-analysis to estimate the overall prevalence of behavioral addictions during the COVID-19 pandemic (e.g., internet addiction, gambling addiction, shopping addiction, food addiction, exercise addiction, social media addiction, and smartphone addiction). The issues of these different types of behavioral addictions have been identified with several statements claiming the importance to take care of the time spent on these behaviors during the COVID-19 pandemic [47,48,49]. However, without empirical evidence showing how severe these behavioral addictions were during the COVID-19 pandemic, government authorities might not take such statements seriously. Therefore, the present study used a rigorous and robust method to search the literature reporting prevalence/frequency for different types of behavioral addiction during the COVID-19 pandemic. Moreover, in the present systematic review and meta-analysis, the term “addiction” was used. Although many studies used other terms (e.g., problematic use, dependence, and disorder) to indicate each behavior problem, “addiction” was used with the consideration of easy-understanding for all different behaviors assessed in the present study. That is, “behavioral addictions” itself is a well-recognized term and can be easily understood by all the experts in the field, although not everyone accepts using this term.
Methods
Design and Registration
The present systematic review and meta-analysis were carried out based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [50]. The protocol of the present study was prospectively registered within international prospective register of systematic reviews PROSPERO (Decree code: CRD42022330898) [51].
Search Strategy
Four major academic databases were systematically searched using the publication period between December 2019 and May 2022 (i.e., PubMed, Scopus, ISI Web of Knowledge, and ProQuest). Search syntax was developed using main search terms from PubMed Medical Subject Headings (MeSH). Main search terms were selected based on PECO-S search strategy (i.e., population, exposure, comparison, outcome, and study design) [52]. In the present study, two main components of exposure (COVID-19 pandemic) and outcome (each type of behavioral addiction) were selected. The main search terms were (internet OR “social media” OR smartphone OR “mobile phone” OR “cell phone” OR gaming OR “video gam*” OR “social network*” OR Twitter OR Instagram OR “YouTube” OR “Facebook” OR “WhatsApp” OR “TikTok” OR “WeChat” OR “SnapChat” OR “QQ” OR “Tinder” OR gambl* OR betting OR “electronic gaming machines” OR lotto OR casino OR poker OR bingo OR blackjack OR lottery OR “slot machine*” OR exercis* OR “physical activity” OR pornography OR sex* OR food OR “binge eating” OR mukbang OR shopping OR buying OR technolog*) AND (addict* OR problem* OR depend* OR disorder* OR obsess* OR excess* OR compuls* OR impuls* OR excess*) AND (“SARS-CoV-2” OR “coronavirus” OR “COVID-19” OR “2019-nCoV” OR “coronavirus disease-2019” OR covid OR coronavirus OR “2019-ncov” OR “sars-cov-2” OR “cov-19”). Search strategy was customized for each database according to its advanced search attributes (provided in Supplementary Materials 1). To increase comprehensiveness of search, reference lists of included studies and published systematic reviews as well as the first ten pages of Google Scholar for each type of behavioral addiction were hand searched.
Eligibility Criteria
The eligibility criteria were constructed based on PECO-S components:
-
Population: Individuals with any age or gender group (in other words, no limitation regarding participants’ characteristics).
-
Exposure: COVID-19 pandemic.
-
Comparison: Healthy population.
-
Outcome: Frequency or prevalence of any type of behavioral addiction. However, behavioral addictions should be assessed using valid and reliable measures.
-
Study design: Observational studies reporting data on frequency or prevalence of any type of behavioral addiction among participants.
Eligible papers were those published between December 2019 and July 2022 using English language and had been published in peer-reviewed papers.
Outcomes
Primary Outcome
Estimates of behavioral addiction prevalence during the COVID-19 pandemic were the primary outcome. Behavioral addiction could be considered as a specific condition that involves mental and behavioral disorders [53]. Therefore, behavioral addiction is defined as a set of coercive behaviors in which a person feels compelled to do something, although the individual knows that engaging in such behaviors may harm them and causes clinical impairment of individuals’ day-to-day activities [54]. There are different types of behavioral addiction, such as internet use, gambling, gaming, shopping, binge eating/food eating, sex, smartphone use, exercise, and work [55]. The primary outcome combined all the types of behavioral addiction for prevalence estimation.
Secondary Outcomes
-
i.
Prevalence of each type of behavioral addictions.
-
ii.
Assessing the possible sources of heterogeneity.
-
iii.
Investigating the predictor variables of behavioral addiction prevalence.
Study Screening and Selection
Two independent reviewers screened the title and abstract of retrieved papers based on the eligibility criteria. The full texts of potentially relevant studies were further examined based on the aforementioned criteria. In this process, relevant studies were selected for further analysis.
Quality Assessment
The methodological quality of included studies was assessed using the Newcastle Ottawa Scale (NOS). Three main methodological characteristics of selection, comparability, and outcome assessment are examined with the NOS checklist. There are three versions of the checklist for evaluating cross-sectional studies (7 items), case–control (8 items), and cohort (8 items). Despite a slight difference in the number and content of these items, each item is rated with one point (except for comparability, which can have two points) for a maximum possible score of 9. Studies with less than 5 points are classified as having a high risk of bias [56]. No studies were excluded based on the quality rating. However, the impact of quality on pooled effect size was assessed via meta-regression.
Data Extraction
A pre-designed Excel spreadsheet was prepared to extract data. The following items were extracted: first author’s name, publication and data collection dates, study design, country (or countries) where data were collected, number of participants, mean age, scales used to assess behavioral addiction, data collection method, countries’ developmental and income status based on world bank reports, and numerical results regarding the frequency of both overall behavioral addiction and types of specified behavioral addiction. It should also be noted that study selection, quality assessment, and data extraction were processes performed independently by two reviewers. Disagreements were resolved through discussion.
Data Synthesis
Evidence from included studies was quantitatively synthesized using STATA software version 14. As included studies were from different populations, meta-analysis using a random effects model was conducted to account for both within-study and between-study variances [57]. Severity of heterogeneity was estimated using the I2 index [58]. Prevalence of behavioral addiction and its 95% confidence intervals (CI) were the selected key measure for the present study. To investigate predictor variables for behavioral addiction, meta-regression was conducted. Funnel plot and Begg’s Test were used to assess publication bias [59]. Meta-trim with the fill and trim method was used to correct probable publication bias [60]. The Jackknife method was used for sensitivity analysis and probable single study effect on pooled effect size [61]. Uni-variable and multivariable meta-regression was used to assess moderators of behavioral addiction prevalence. When values of adjusted R2 were considerable for examined variable in uni-variable regression, they were entered in multivariable meta-regression models.
Results
Study Screening and Selection Process
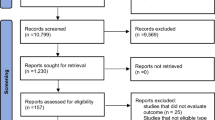
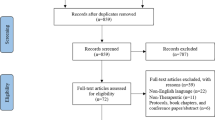
The initial search in four academic databases resulted in 28,381 papers: PubMed (n = 6,634), Scopus (n = 11,011), ISI Web of Knowledge (n = 9654), and ProQuest (n = 1082). After removing duplicates (n = 12,342), the remaining papers were screened based on their title and abstract. Finally, 372 papers appeared to be potentially eligible and their full-texts were reviewed. In this process, 94 studies met the eligibility criteria and were pooled in the meta-analysis. Figure 1 shows the search process based on the PRISMA flowchart.

Identification of studies via databases and registers
Study Description
A total of 94 studies with 237,657 participants from 40 different countries (Argentina, Australia, Bangladesh, Brazil, Chile, China, Costa Rica, Croatia, Dominican Republic, Ecuador, Egypt, Guyana, Honduras, Hungary, India, Indonesia, Iran, Italy, Japan, Jordan, Kuwait, Lebanon, Lithuania, Malaysia, Mexico, Pakistan, Peru, Poland, Russian, Saudi Arabia, Spain, Sudan, Sweden, Switzerland, Taiwan, Turkey, UK, USA, Uruguay, and Vietnam) were included. A total of 27 studies gathered data during the national lockdown period in their respective countries. The smallest sample size was 42 (from the USA), and the largest sample size was 51,246 (from Japan). The mean age of participants was 25.02 years with age range between 5 and 82 years. Almost all studies used a cross-sectional design. One study was a longitudinal study with three waves in COVID-19 pandemic; data regarding each wave was extracted as a separate study. Three papers reported the results from multi-countries and 27 studies were population-based. Most studies (49 out of 94) were conducted in developed countries. All studies had participants from both gender groups with 57.41% female. The main behavioral addictions studied were internet use (39 studies), gaming (19 studies), gambling (18 studies), smartphone use (13 studies), social media use (10 studies), food addiction (five studies), exercise (four studies), sex addiction (four studies), and shopping addiction (two studies). Fourteen studies reported more than one type of behavioral addiction. No study was retrieved regarding the prevalence of work addiction. Table 1 provides the summary characteristics of all included studies.
Quality Assessment
Most of the studies (75 out of 94) were categorized as being high-quality (or low risk of bias) studies. The total score of methodological quality is provided in Table 1 with details in Fig. 2. The main methodological problems were:
-
i.
Most studies (89 out of 94) did not report the description of the response rate or the characteristics of the responders and the non-responders.
-
ii.
Most studies (77 out of 94) did not provide an explanation regarding sample size estimation and justification.
-
iii.
Some studies (44 out of 94) did not recruit a representative sample (i.e., they used a selected group of population or did not provide description regarding the sampling strategy).

Details of methodological quality assessment based on NOS checklist within included studies
Outcome Measures
Pooled Prevalence
The pooled estimated prevalence of all types of behavioral addictions was 33% (94 studies, 95% CI: 28 to 38%, I2: 99.94%, τ2: 0.06). Figure 3 provides the forest plot regarding the pooled prevalence. The pooled prevalence rates of specific behavioral addictions are listed below:
-
i.
Internet addiction: 30% (39 studies, 95% CI: 26 to 34%, I2: 99.86%, τ.2: 0.02)
-
ii.
Gaming addiction: 24% (19 studies, 95% CI: 14 to 33%, I2: 99.92%, τ.2: 0.04)
-
iii.
Gambling addiction: 24% (18 studies, 95% CI: 17 to 31%, I2: 99.74%, τ.2: 0.02)
-
iv.
Smartphone addiction: 48% (13 studies, 95% CI: 36 to 61%, I2: 99.73%, τ.2: 0.05)
-
v.
Social media addiction: 52% (10 studies, 95% CI: 30 to 73%, I2: 99.93%, τ.2: 0.12)
-
vi.
Food addiction: 21% (five studies, 95% CI: 10 to 32%, I2: 99.30%, τ.2: 0.02)
-
vii.
Sex addiction: 34% (five studies, 95% CI: 19 to 49%, I2: 99.86, τ.2: 0.03)
-
viii.
Exercise addiction: 7% (four studies, 95% CI: 3 to 12%, I2: 96.24%, τ.2 < 0.001)
-
ix.
Shopping addiction: 10% (two studies, 95% CI: 9 to 12%, I2: not applicable, τ.2: not applicable)

Forest plot regarding the pooled prevalence of all types of behavioral addiction
Publication Bias
The probability of publication bias was assessed using Begg’s test (p = 0.002) and funnel plot. Based on asymmetric funnel plot (Fig. 4), publication bias seems probable.

Funnel plot assessing the publication bias among included studies
Correction for Publication Bias
The fill-and-trim method was used to correct probable publication bias. In this method, 41 studies were imputed, and the corrected pooled prevalence of all types of behavioral addictions was 11.1% (95% CI: 5.4 to 16.8%; τ2: 0.11; p < 0.001). The resultant funnel plot after trimming is provided in Fig. 5. The corrected type specific prevalence rates of behavioral addictions are listed below:
-
i.
Internet addiction: 10.6% (39 studies, 18 imputed studies, 95% CI: 6.2 to 15.1%, τ.2: 0.03)
-
ii.
Gaming addiction: 5.3% (19 studies, 10 imputed studies, 95% CI: 0 to 15.3%, τ.2: 0.07)
-
iii.
Gambling addiction: 7.2% (18 studies, 8 imputed studies, 95% CI: 0 to 15.4%, τ.2: 0.05)
-
iv.
Smartphone addiction: 30.7% (13 studies, six imputed studies, 95% CI: 16.3 to 45.2%, τ.2: 0.10)
-
v.
Social media addiction: 15.1% (10 studies, five imputed studies, 95% CI: 0 to 36.5%, τ.2: 0.18)
-
vi.
Sex addiction: 9.4% (five studies, two imputed studies, 95% CI: 0 to 24.6%, τ.2: 0.04)
-
vii.
Shopping addiction: 7.2% (two studies, one imputed study, 95% CI: 0 to 54.3%, τ.2: 0.17)

Corrected funnel plot based on the fill and trim method
Food addiction and exercise addiction were not affected by publication bias.
Sensitivity Analysis
Sensitivity analysis (based on the one-out or Jack-knife method) showed that the pooled effect size was not affected by a single study effect.
Moderator Analysis
Moderators of prevalence for all type and specific behavioral addictions were assessed using uni-variable meta-regression (Table 2) and multivariable meta-regression (Table 3).
All Types of Behavioral Addiction
Based on uni-variable meta-regression, the percentage of individuals using the internet in the country was the only significant moderator in all types of behavioral addictions, accounting for 4.23% of variance. Each percentage increase of individuals using the internet in the country was associated with 0.3% decrease in all types of behavioral addiction prevalence rates. Other examined variables did not affect pooled prevalence or heterogeneity.
Internet Addiction
Based on uni-variable meta-regression, none of the examined variables affect pooled prevalence or heterogeneity of internet addiction.
Gaming Addiction
Based on multivariable meta-regression, data collection method (online vs. other methods, p = 0.04) and lockdown period (yes vs. no, p = 0.03) were significant predictors of gaming addiction during the COVID-19 pandemic. The prevalence rate of gaming addiction was 24% lower in studies with online data collection method vs. studies using other data collection methods. The prevalence rate of gaming addiction was 21% higher during lockdown period vs. non-lockdown period. These variables explained 31.01% variance in the prevalence of gaming addiction.
Gambling Addiction
Based on multivariable meta-regression, the percentage of individuals using the internet in the country was the only significant moderator in gambling prevalence (p = 0.03), accounting for 34.28% of variance in prevalence of gambling. Each 1% increase of individuals using the internet in each country was associated with a 1.6% decrease in gambling prevalence.
Smartphone Addiction
Based on uni-variable meta-regression, country income level (high, upper-middle, lower-middle, p = 0.04), percentage of individuals using the internet in the country (p = 0.05), and methodological quality (low vs. high risk of bias, p = 0.02) were moderators of smartphone addiction. Based on multivariable meta-regression models, the prevalence of smartphone addiction in low risk of bias studies was 41% lower than in high risk of bias studies. The prevalence rate of smartphone addiction was 27% (95% CI: 24 to 29%) in high-income countries, 45% (95% CI: 32 to 58%) in upper intermediate income countries, and 84% (95% CI: 82 to 86%) in lower intermediate income countries. Each 1% increase of individuals using the internet in the country was associated with a 0.3% decrease in smartphone addiction prevalence. These variables accounted for 34.53% of variance in the prevalence of smartphone addiction.
Social Media Addiction
Based on multivariable meta-regression, the female percentage of participants (each 1% increase in female participants was associated with a 4.6% decrease in social media addiction, p = 0.03); being in lockdown period (two times higher than in non-lockdown period, p = 0.06); mean age of participants (each year increase was associated with 1.1% decrease in social media addiction, p = 0.19); percentage of individuals using the internet in country (each 1% increase of individuals using the internet in the country was associated with an 8.3% decrease in social media addiction prevalence, p = 0.13); developing status of country (52.5% higher in developed vs. developing countries, p = 0.19); and methodological quality of studies (1.5 times lower in low risk of bias vs. high risk of bias studies, p = 0.10) were predictors of social media addiction, accounting for 93.67% of the variance.
Food Addiction
Based on uni-variable meta-regression, being in lockdown period (yes vs. no, p < 0.001) was the only significant predictor of food addiction which accounted for 100% of the variance. The prevalence rate of food addiction was 32% higher during the lockdown period vs. non-lockdown period.
Sex Addiction
Based on uni-variable meta-regression, the percentage of individuals using the internet in the country (p = 0.002) was the only significant predictor of sex addiction which accounted for 96.90% of the variance. Each 1% increase of individuals using the internet in the country was associated with a 9% increase in sex addiction prevalence.
Exercise addiction (four studies) and shopping addiction (two studies) did not have sufficient data for moderator analysis.
Discussion
Due to the COVID-19 pandemic, human behaviors have changed substantially [149]. Therefore, it is important for healthcare providers and government authorities to understand the changed behaviors, especially addictive behaviors, during the COVID-19 pandemic. Therefore, healthcare providers and government authorities could consider appropriate programs to respond to behavioral addiction issues. The present systematic review and meta-analysis therefore used a rigorous methodology to estimate the prevalence of overall behavioral addictions (comprising internet addiction, smartphone addiction, gaming addiction, social media addiction, food addiction, exercise addiction, gambling addiction, and shopping addiction) during the COVID-19 pandemic and associated factors using meta-regression. Moreover, the prevalence rate of each individual behavioral addiction was reported and tested for its associated factors.
The findings showed that the corrected pooled prevalence of overall behavioral addictions was 11.1% (95% CI: 5.4% to 16.8%), and the corrected prevalence rates of each behavioral addiction varied between 7% (exercise addiction) and 30.7% (smartphone addiction). Moreover, the female percentage of participants, mean age of participants, percentage of individuals using the internet in the country, and the developing status of the country were moderators of social media addiction prevalence. Methodological quality of studies was associated with social media addiction and smartphone addiction prevalence. Being in lockdown period was a moderator of the prevalence rates for food addiction, gaming addiction, and social media addiction. Individuals using the internet (percentage of the population) were associated with overall prevalence rates for behavioral addiction, sex addiction, and gambling addiction. Data collection method (online vs. other methods) was associated with the prevalence of gaming addiction.
Before the COVID-19 pandemic, addictive behaviors had been identified as an important factor affecting individuals’ health, such as sleep quality and quality of life [150,151,152,153,154,155,156,157,158,159]. Among the different types of addictive behaviors, internet addiction has been studied with growing interest because of technology advancement [160]. Moreover, the internet has been considered as a medium for individuals to engage in different activities. With the convenience of internet use, especially the technology advancement in smartphones (i.e., smartphones are user-friendly with internet access and power apps functions), individuals are likely to become addicted to different types of activities (e.g., social media use, online shopping, and online gaming). Smartphone use is similar to internet use because it provides another medium for individuals to easily engage in different activities and provides the potential for smartphone addiction [161]. Therefore, the high prevalence rates of internet addiction (10.6%) and smartphone addiction (30.7%) found in the present systematic review and meta-analysis are likely explained by the nature of being a 24/7 medium.
In contrast, prevalence rates of shopping addiction (7.2%) and exercise addiction (7.0%) were not high (relatively) in the present study’s findings. The main reason could be the countries’ policies in COVID-19 infection control. More specifically, governments encouraged citizens and residents to reduce outdoor activities and many closed facilities for commercial or exercise purposes (e.g., mall and gym closure) [14,15,16]. Therefore, individuals who had a problem of shopping addiction or exercise addiction were somewhat restricted in their addictive behaviors (i.e., shopping and exercise). However, some are likely to have adapted their addictive behaviors to satisfy their cravings (e.g., physical shopping changing to online shopping; exercise in a gym changing to home exercise); the changed environments might somewhat decrease their desire in engaging in such addictive behaviors.
The present systematic review and meta-analysis further identified that the lockdown period was a significant factor associated with prevalence of several behavioral addictions (including food addiction, gaming addiction, and social media addiction). The finding that lockdown period had higher prevalence rate of overall behavioral addiction than non-lockdown period could be explained by the internet advancement and individuals’ coping strategies during the lockdown period. More specifically, lockdown may have increased individuals’ psychological distress and individuals may have engaged in some potentially addictive behaviors to cope with their psychological distress. Therefore, some individuals are likely to develop behavioral addictions to cope with their psychological distress, and this mechanism echoes the I-PACE model proposed by Brand et al. [17].
Individuals using the internet (as a percentage of the population) were found to be another significant factor contributing to the behavioral addictions. This finding could be explained by the peer effect [162]. More specifically, when individuals found that their friends and family members were all constantly using the internet, they may have felt that using internet constantly was socially acceptable. Such a feeling may motivate those who have behavioral addictions via an internet platform to keep engaging in their online behavioral addictions. As a result, when the country has a higher percentage of individuals using the internet, the society is likely to have a higher rate of prevalence in behavioral addictions.
Based on the findings of the present systematic review and meta-analysis, there are several implications. First, if a lockdown is needed to control infection and disease, healthcare providers and government authorities should pay special attention to the possibility of increased behavioral addictions among their citizens. Different programs such as online cognitive behavioral therapy and online mindfulness programs may be provided to help individuals go through the tough lockdown period without increasing their craving for their addictive behavior of choice. Second, governments should be alerted when they observe a high percentage of individuals using internet. Appropriate programs or policies may be designed for those countries with a high percentage of individuals using the internet to prevent consequent behavioral addiction problems.
Limitations
The present study has a number of limitations. First, some of the analyzed studies did not have representative samples. Therefore, the estimated prevalence reported in the present systematic review and meta-analysis might not have good generalizability to the entire population worldwide. Additionally, the response rates were unclear for most of the analyzed studies. Therefore, the representativeness of the studied samples is arguably problematic. Second, most of the studies used online surveys to collect the data, which may cause selection bias in sampling. More specifically, individuals without internet access or those who did not use internet during the survey period were unable to complete the survey assessing their behavioral addictions. Therefore, the estimations on internet-related addictive behaviors could be overestimated (because those who did not use internet were not included in the present study). Third, almost all the studies analyzed in the present systematic review and meta-analysis used a cross-sectional design, which lacks the ability to determine causal relationships between the study variables. Lastly, the information was imbalanced between different types of behavioral addictions (e.g., most studies reported for addictions to internet use and smartphone use, and only two studies reported addictions to shopping). Therefore, the prevalence rates of the behavioral addictions reported from few studies have the issue of small sample sizes and probable low heterogeneity.
Conclusion
Behavioral addictions are potential health issues during the COVID-19 pandemic. High prevalence rates of different types of behavioral addictions have been estimated with the use of a rigorous methodology in the present meta-analysis. Given that behavioral addictions are associated with a variety of health issues and subsequently cause care burden for the societies, healthcare providers and government authorities should pay attention to the issue of behavioral addictions during the COVID-19 pandemic. Indeed, several statements have been announced for government authorities and related stakeholders to take care of the issues of behavioral addictions [47, 49, 163]. The findings in the present systematic review and meta-analysis echo the importance of these statements. Therefore, designing appropriate programs to reduce behavioral addictions during the COVID-19 pandemic (and for subsequent pandemics) is highly recommended.
Data Availability
All tables and figures are original and have been produced by the authors for this publication. Tables and figures have not previously been published.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Chang K-C, Hou W-L, Pakpour AH, Lin C-Y, Griffiths MD. Psychometric testing of three COVID-19-related scales among people with mental illness. Int J Ment Health Addiction. 2022;20:324–36.
Alimoradi Z, Abdi F, Gozal D, Pakpour AH. Estimation of sleep problems among pregnant women during COVID-19 pandemic: a systematic review and meta-analysis. BMJ Open. 2022;12(4): e056044.
Alimoradi Z, Broström A, Tsang HW, Griffiths MD, Haghayegh S, Ohayon MM, et al. Sleep problems during COVID-19 pandemic and its’ association to psychological distress: a systematic review and meta-analysis. EClinicalMedicine. 2021;36: 100916.
Alimoradi Z, Gozal D, Tsang HW, Lin CY, Broström A, Ohayon MM, et al. Gender-specific estimates of sleep problems during the COVID-19 pandemic: systematic review and meta-analysis. J Sleep Res. 2022;31(1): e13432.
Alimoradi Z, Ohayon MM, Griffiths MD, Lin C-Y, Pakpour AH. Fear of COVID-19 and its association with mental health-related factors: systematic review and meta-analysis. BJPsych Open. 2022;8(2):1–26.
Khorshidi M, Alimoradi Z, Bahrami N, Griffiths MD. Predictors of women’s sexual quality of life during the COVID-19 pandemic: an Iranian cross-sectional study. Sexual and Relationship Therapy. 2022:1–14.
Masaeli N, Farhadi H. Prevalence of Internet-based addictive behaviors during COVID-19 pandemic: a systematic review. J Addict Dis. 2021;39(4):468–88.
Brodeur M, Audette-Chapdelaine S, Savard A-C, Kairouz S. Gambling and the COVID-19 pandemic: a scoping review. Prog Neuropsychopharmacol Biol Psychiatry. 2021;111: 110389.
• Zamboni L, Carli S, Belleri M, Giordano R, Saretta G, Lugoboni F. COVID-19 lockdown: impact on online gambling, online shopping, web navigation and online pornography. Journal of public health research. 2021;10(1):1–6. (This is a methodological high-quality, population-based study with considerable sample size assessing different kinds of behavioral addictions.)
Zhu S, Zhuang Y, Lee P, Li JC-M, Wong PW. Leisure and problem gaming behaviors among children and adolescents during school closures caused by COVID-19 in Hong Kong: quantitative cross-sectional survey study. JMIR Serious Games. 2021;9(2):e26808.
Miniati M, Marzetti F, Palagini L, Marazziti D, Orrù G, Conversano C, et al. Eating disorders spectrum during the COVID pandemic: a systematic review. Frontiers in Psychology. 2021:1–61.
Trott M, Johnstone J, Pardhan S, Barnett Y, Smith L. Changes in body dysmorphic disorder, eating disorder, and exercise addiction symptomology during the COVID-19 pandemic: a longitudinal study of 319 health club users. Psychiatry Res. 2021;298: 113831.
Ayar D, Karaman MA, Karaman R. Work-life balance and mental health needs of health professionals during COVID-19 pandemic in Turkey. Int J Ment Heal Addict. 2022;20(1):639–55.
Pakpour AH, Liu C-h, Hou W-L, Chen Y-P, Li Y-P, Kuo Y-J, et al. Comparing fear of COVID-19 and preventive COVID-19 infection behaviors between Iranian and Taiwanese older people: early reaction may be a key. Front Public Health. 2021;9:1–8.
Alijanzadeh M, Harati T. The role of social capital in the implementation of social distancing during the COVID-19 pandemic. Asian J Soc Health Behav. 2021;4(1):45–6.
Shirali GA, Rahimi Z, Araban M, Mohammadi MJ, Cheraghian B. Social-distancing compliance among pedestrians in Ahvaz, South-West Iran during the COVID-19 pandemic. Asian J Soc Health Behav. 2021;4(4):131.
Brand M, Young KS, Laier C, Wölfling K, Potenza MN. Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: an Interaction of Person-Affect-Cognition-Execution (I-PACE) model. Neurosci Biobehav Rev. 2016;71:252–66.
Dong H, Yang F, Lu X, Hao W. Internet addiction and related psychological factors among children and adolescents in China during the coronavirus disease 2019 (COVID-19) epidemic. Front Psychiatry. 2020:751.
McKibbin W, Fernando R. The global macroeconomic impacts of COVID-19: seven scenarios. Asian Econ Papers. 2021;20(2):1–30.
Montag C, Elhai JD. Discussing digital technology overuse in children and adolescents during the COVID-19 pandemic and beyond: on the importance of considering affective neuroscience theory. Addict Behav Rep. 2020;12: 100313.
Korhonen L. The good, the bad and the ugly of children’s screen time during the COVID-19 pandemic. Acta Paediatrica (Oslo, Norway: 1992). 2021;110(10):2671.
DAK-Studie. DAK-Studie: gaming, social-media & corona. 2020. https://www.dak.de/dak/gesundheit/dak-studie-gaming-social-media-und-corona-2295548.html. Accessed 10 Jul 2022.
Chen I-H, Chen C-Y, Liu C-H, Ahorsu DK, Griffiths MD, Chen Y-P, et al. Internet addiction and psychological distress among Chinese schoolchildren before and during the COVID-19 outbreak: a latent class analysis. J Behav Addict. 2021;10(3):731–46.
Fung XC, Siu AM, Potenza MN, O'Brien KS, Latner JD, Chen C-Y, et al. Problematic use of internet-related activities and perceived weight stigma in schoolchildren: a longitudinal study across different epidemic periods of COVID-19 in China. Front Psychiatry. 2021;12:1–10, Article ID: 675839.
Chen C-Y, Chen I-H, Hou W-L, Potenza MN, O’Brien KS, Lin C-Y, et al. The relationship between children’s problematic internet-related behaviors and psychological distress during the onset of the COVID-19 pandemic: a longitudinal study. J Addict Med. 2022;16(2): e73.
Chen I-H, Chen C-Y, Pakpour AH, Griffiths MD, Lin C-Y, Li X-D, et al. Problematic internet-related behaviors mediate the associations between levels of internet engagement and distress among schoolchildren during COVID-19 lockdown: a longitudinal structural equation modeling study. J Behav Addict. 2021;10(1):135–48.
Cuan-Baltazar JY, Muñoz-Perez MJ, Robledo-Vega C, Pérez-Zepeda MF, Soto-Vega E. Misinformation of COVID-19 on the internet: infodemiology study. JMIR Public Health Surveill. 2020;6(2): e18444.
Karthik L, Kumar G, Keswani T, Bhattacharyya A, Chandar SS, Bhaskara RK. Protease inhibitors from marine actinobacteria as a potential source for antimalarial compound. PLoS ONE. 2014;9(3): e90972.
Kennedy GJ, Kelman HR, Thomas C. The emergence of depressive symptoms in late life: the importance of declining health and increasing disability. J Community Health. 1990;15(2):93–104.
Cheng C, Li AY-l. Internet addiction prevalence and quality of (real) life: a meta-analysis of 31 nations across seven world regions. Cyberpsychol Behav Soc Netw. 2014;17(12):755–60.
Ferguson CJ, Coulson M, Barnett J. A meta-analysis of pathological gaming prevalence and comorbidity with mental health, academic and social problems. J Psychiatr Res. 2011;45(12):1573–8.
Lorains FK, Cowlishaw S, Thomas SA. Prevalence of comorbid disorders in problem and pathological gambling: systematic review and meta-analysis of population surveys. Addiction. 2011;106(3):490–8.
Maraz A, Griffiths MD, Demetrovics Z. The prevalence of compulsive buying: a meta-analysis. Addiction. 2016;111(3):408–19.
Burrows T, Kay-Lambkin F, Pursey K, Skinner J, Dayas C. Food addiction and associations with mental health symptoms: a systematic review with meta-analysis. J Hum Nutr Diet. 2018;31(4):544–72.
Berczik K, Szabó A, Griffiths MD, Kurimay T, Kun B, Urbán R, et al. Exercise addiction: symptoms, diagnosis, epidemiology, and etiology. Subst Use Misuse. 2012;47(4):403–17.
Andreassen C. Online social network site addiction: a comprehensive review. Curr Addict Rep. 2015;2(2):175–84.
Sohn SY, Rees P, Wildridge B, Kalk NJ, Carter B. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: a systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry. 2019;19(1):1–10.
Banz BC, Yip SW, Yau YH, Potenza MN. Behavioral addictions in addiction medicine: from mechanisms to practical considerations. Prog Brain Res. 2016;223:311–28.
Derevensky JL, Hayman V, Gilbeau L. Behavioral addictions: excessive gambling, gaming, Internet, and smartphone use among children and adolescents. Pediatr Clin. 2019;66(6):1163–82.
Marazziti D, Presta S, Baroni S, Silvestri S, Dell’Osso L. Behavioral addictions: a novel challenge for psychopharmacology. CNS Spectr. 2014;19(6):486–95.
Clark L, Limbrick-Oldfield EH. Disordered gambling: a behavioral addiction. Curr Opin Neurobiol. 2013;23(4):655–9.
Sixto-Costoya A, Castelló-Cogollos L, Aleixandre-Benavent R, Valderrama-Zurián JC. Global scientific production regarding behavioral addictions: an analysis of the literature from 1995 to 2019. Addictive behaviors reports. 2021;14:100371.
Karaca S, Saleh A, Canan F, Potenza MN. Comorbidity between behavioral addictions and attention deficit/hyperactivity disorder: a systematic review. Int J Ment Heal Addict. 2017;15(3):701–24.
Varo C, Murru A, Salagre E, Jiménez E, Solé B, Montejo L, et al. Behavioral addictions in bipolar disorders: a systematic review. Eur Neuropsychopharmacol. 2019;29(1):76–97.
Fernandez DP, Kuss DJ, Griffiths MD. Short-term abstinence effects across potential behavioral addictions: a systematic review. Clin Psychol Rev. 2020;76:101828.
Fong TW, Reid RC, Parhami I. Behavioral addictions: where to draw the lines? Psychiatric Clinics. 2012;35(2):279–96.
Gjoneska B, Potenza MN, Jones J, Corazza O, Hall N, Sales CM, et al. Problematic use of the internet during the COVID-19 pandemic: good practices and mental health recommendations. Compr Psychiatry. 2022;112:152279.
Thase ME, Mahableshwarkar AR, Dragheim M, Loft H, Vieta E. A meta-analysis of randomized, placebo-controlled trials of vortioxetine for the treatment of major depressive disorder in adults. Eur Neuropsychopharmacol. 2016;26(6):979–93.
King DL, Achab S, Higuchi S, Bowden-Jones H, Müller KW, Billieux J, et al. Gaming disorder and the COVID-19 pandemic: treatment demand and service delivery challenges. J Behav Addict. 2022;11(2):243–8
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
Alimoradi Z, Pakpour A. Estimation of behavioral addiction during the Covid-19 pandemic and its association with psychological distress.: International prospective register of systematic reviews; PROSPERO; 2022 [23/6/2022]. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022330898. Accessed 7 Jul 2022.
Morgan RL, Whaley P, Thayer KA, Schünemann HJ. Identifying the PECO: a framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int. 2018;121(Pt 1):1027.
Demetrovics Z, Griffiths MD. Behavioral addictions: past, present and future. J Behav Addict. 2012;1(1):1–2.
Du J, Fan N, Zhao M, Hao W, Liu T, Lu L, et al. Expert consensus on the prevention and treatment of substance use and addictive behaviour-related disorders during the COVID-19 pandemic. Gen Psychiatry. 2020;33(4):1–6.
Billieux J, Schimmenti A, Khazaal Y, Maurage P, Heeren A. Are we overpathologizing everyday life? A tenable blueprint for behavioral addiction research. J Behav Addict. 2015;4(3):119–23.
Luchini C, Stubbs B, Solmi M, Veronese N. Assessing the quality of studies in meta-analyses: advantages and limitations of the Newcastle Ottawa Scale. World J Meta-Anal. 2017;5(4):80–4.
Hox JJ, De Leeuw ED. Multilevel models for meta-analysis. InMultilevel modeling. London: Psychology Press; 2003. p. 87–104.
Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, Botella J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods. 2006;11(2):193.
Rothstein HR, Sutton AJ, Borenstein M. Publication bias in meta-analysis. Publication bias in meta-analysis: Prevention, assessment and adjustments. 2007:269–71.
Duval S, Tweedie R. Trim and fill: a simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–63.
Hedges L, Olkin I. Statistical methods for meta-analysis. New York: Academic press; 2014.
Truzoli R, Pirola V, Celebre L, Piccoli E, Vanzetto S, Conti D, et al. Intrapersonal and social factors for problematic Internet use among students during the COVID-19 pandemic. Psychiatr Danub. 2021;33(suppl 10):144–54.
• Tahir MJ, Malik NI, Ullah I, Khan HR, Perveen S, Ramalho R, et al. Internet addiction and sleep quality among medical students during the COVID-19 pandemic: a multinational cross-sectional survey. PLoS ONE. 2021;16(11): e0259594. (This is a methodological high-quality, population-based study with considerable sample size assessing Internet addictions. The other strength of this study is gathering data from multi countries with cultural differences.)
Ozturk FO, Ayaz-Alkaya S. Internet addiction and psychosocial problems among adolescents during the COVID-19 pandemic: a cross-sectional study. Arch Psychiatr Nurs. 2021;35(6):595–601.
Aközlü Z, Kolukısa T, Öztürk Şahin Ö, Topan A. Internet addiction and stressors causing internet addiction in primary school children during the COVID-19 pandemic: a descriptive and cross-sectional study from Turkey. Addicta: The Turkish Journal on Addictions. 2021;8(1):65–72.
Kamaşak T, Topbaş M, Ozen N, Esenülkü G, Yıldız N, Şahin S, et al. An investigation of changing attitudes and behaviors and problematic Internet use in children aged 8 to 17 years during the COVID-19 pandemic. Clin Pediatr. 2022;61(2):194–205.
Perez-Siguas R, Matta-Solis H, Matta-Solis E. Excessive Internet use during the covid-19 pandemic in a population of north lima. J Med Pharm Allied Sci. 2021;10(6, 1582):3743–6.
Gansner M, Nisenson M, Lin V, Pong S, Torous J, Carson N. Problematic Internet use before and during the COVID-19 pandemic in youth in outpatient mental health treatment: App-Based Ecological Momentary Assessment Study. JMIR Mental Health. 2022;9(1):e33114.
Lakkunarajah S, Adams K, Pan AY, Liegl M, Sadhir M. A Trying time: Problematic Internet Use (PIU) and its association with depression and anxiety during the COVID-19 pandemic. Child Adolesc Psychiatry Ment Health. 2022;16(1):1–8.
Siste K, Hanafi E, Sen LT, Murtani BJ, Christian H, Limawan AP, et al. Implications of COVID-19 and lockdown on Internet addiction among adolescents: data from a developing country. Front Psychiatry. 2021;12:1–11, Article ID: 665675.
Siste K, Hanafi E, Sen LT, Christian H, Siswidiani LP, Limawan AP, et al. The impact of physical distancing and associated factors towards internet addiction among adults in Indonesia during COVID-19 pandemic: a nationwide web-based study. Front Psych. 2020;11:580977.
Jiang M, Zhao Y, Wang J, Hua L, Chen Y, Yao Y, et al. Serial multiple mediation of the correlation between internet addiction and depression by social support and sleep quality of college students during the COVID-19 epidemic. Psychiatry Investig. 2022;19(1):9.
• Li YY, Sun Y, Meng SQ, Bao YP, Cheng JL, Chang XW, et al. Internet addiction increases in the general population during COVID-19: evidence from China. Am J Addict. 2021;30(4):389–97. (This is a methodological high-quality, population-based study with considerable sample size assessing prevalence of internet addiction.)
Zhu K, Xie X, Liu Q, Meng H, Song R. Internet addiction: prevalence and relationship with academic burnout among undergraduates during widespread online learning. Perspect Psychiatric Care. 2022. https://doi.org/10.1111/ppc.13060.
Li Z-L, Liu R, He F, Li S-Y, Zhao Y-J, Zhang W-Y, et al. Prevalence of internet addiction disorder and its correlates among clinically stable adolescents with psychiatric disorders in China during the COVID-19 outbreak. Front Psychiatry. 2021;12, Article ID: 686177
Wu Q, Chen T, Zhong N, Bao J, Zhao Y, Du J, et al. Changes of internet behavior of adolescents across the period of COVID-19 pandemic in China. Psychol Health Med. 2021:1–11. https://doi.org/10.1080/13548506.2021.2019809.
Liang L, Li C, Meng C, Guo X, Lv J, Fei J, et al. Psychological distress and Internet addiction following the COVID-19 outbreak: fear of missing out and boredom proneness as mediators. Arch Psychiatr Nurs. 2022;40:8–14.
Cai H, Xi HT, Zhu Q, Wang Z, Han L, Liu S, et al. Prevalence of problematic Internet use and its association with quality of life among undergraduate nursing students in the later stage of COVID-19 pandemic era in China. Am J Addict. 2021;30(6):585–92.
Sun Y, Li Y, Bao Y, Meng S, Sun Y, Schumann G, et al. Brief report: increased addictive internet and substance use behavior during the COVID-19 pandemic in China. Am J Addict. 2020;29(4):268–70.
Zhao Y, Jiang Z, Guo S, Wu P, Lu Q, Xu Y, et al. Association of symptoms of attention deficit and hyperactivity with problematic internet use among university students in Wuhan, China during the COVID-19 pandemic. J Affect Disord. 2021;286:220–7.
Liu S, Zou S, Zhang D, Wang X, Wu X. Problematic Internet use and academic engagement during the COVID-19 lockdown: the indirect effects of depression, anxiety, and insomnia in early, middle, and late adolescence. J Affect Disord. 2022;309:9–18.
Xia Y, Fan Y, Liu T-H, Ma Z. Problematic Internet use among residential college students during the COVID-19 lockdown: a social network analysis approach. J Behav Addict. 2021;10(2):253–62.
Xie X, Zhu K, Xue Q, Zhou Y, Liu Q, Wu H, et al. Problematic Internet use was associated with psychological problems among university students during COVID-19 outbreak in China. Front Public Health. 2021;9:1–10, Article ID:675380.
Shehata WM, Abdeldaim DE. Internet addiction among medical and non-medical students during COVID-19 pandemic, Tanta University, Egypt. Environ Sci Pollut Res. 2021;28(42):59945–52.
AlSumait L, AlHeneidi H, Smith AP, editors. Exploring the effects of loneliness and internet addiction on adults’ well-being during COVID-19 quarantine. International Conference on Bioengineering and Biomedical Signal and Image Processing. 2021. Springer, pp 491–501.
Jahan I, Hosen I, Al Mamun F, Kaggwa MM, Griffiths MD, Mamun MA. How has the COVID-19 pandemic impacted internet use behaviors and facilitated problematic internet use? A Bangladeshi study. Psychol Res Behav Manag. 2021;14:1127.
Nakayama H, Matsuzaki T, Mihara S, Kitayuguchi T, Higuchi S. Change of Internet use and bedtime among junior high school students after long-term school closure due to the coronavirus disease 2019 pandemic. Children. 2021;8(6):480.
Lin M-P. Prevalence of Internet addiction during the COVID-19 outbreak and its risk factors among junior high school students in Taiwan. Int J Environ Res Public Health. 2020;17(22):8547.
Prakash S, Yadav JS, Singh T. An online cross-sectional study to assess the prevalence of internet addiction among people staying at their home during lockdown due to COVID-19. Int J Indian Psychol. 2020;8(3):424–32.
Meitei SY, Pao P, Baite K, Konjengbam H. Prevalence of insomnia and Internet dependence amidst the COVID 19 among the Northeast Indian population: a preliminary study. Sleep and Vigilance. 2021;5(2):245–50.
Gecaite-Stonciene J, Saudargiene A, Pranckeviciene A, Liaugaudaite V, Griskova-Bulanova I, Simkute D, et al. Impulsivity mediates associations between problematic internet use, anxiety, and depressive symptoms in students: a cross-sectional COVID-19 study. Front Psych. 2021;12: 634464.
Vejmelka L, Matković R. Online interactions and problematic internet use of croatian students during the COVID-19 pandemic. Information. 2021;12(10):399.
Volpe U, Orsolini L, Salvi V, Albert U, Carmassi C, Carrà G, et al. COVID-19-related social isolation predispose to problematic Internet and online video gaming use in Italy. Int J Environ Res Public Health. 2022;19(3):1539.
Ismail N, Tajjudin AI, Jaafar H, Nik Jaafar NR, Baharudin A, Ibrahim N. The relationship between internet addiction, Internet gaming and anxiety among medical students in a malaysian public university during COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(22):11870.
Oka T, Hamamura T, Miyake Y, Kobayashi N, Honjo M, Kawato M, et al. Prevalence and risk factors of internet gaming disorder and problematic Internet use before and during the COVID-19 pandemic: a large online survey of Japanese adults. J Psychiatr Res. 2021;142:218–25.
Ballarotto G, Marzilli E, Cerniglia L, Cimino S, Tambelli R. How does psychological distress due to the COVID-19 pandemic impact on internet addiction and Instagram addiction in emerging adults? Int J Environ Res Public Health. 2021;18(21):11382.
Duan L, Shao X, Wang Y, Huang Y, Miao J, Yang X, et al. An investigation of mental health status of children and adolescents in China during the outbreak of COVID-19. J Affect Disord. 2020;275:112–8.
Saritepeci M, Yildiz Durak H, Atman Uslu N. A latent profile analysis for the study of multiple screen addiction, mobile social gaming addiction, general mattering, and family sense of belonging in university students. Int J Ment Health Addict. 2022:1–22. https://doi.org/10.1007/s11469-022-00816-y.
Çakıroğlu S, Soylu N, Görmez V. Re-evaluating the digital gaming profiles of children and adolescents during the COVID-19 pandemic: a comparative analysis comprising 2 years of pre-pandemic data. Addicta: Turkish J Addict. 2021;8(1):51–7.
Nugraha YP, Awalya A, Mulawarman M. Predicting video game addiction: the effects of composite regulatory focus and interpersonal competence among Indonesian teenagers during COVID-19 pandemic. Islam Guid Couns J. 2021;4(1):66–77.
Chang CI, Fong Sit H, Chao T, Chen C, Shen J, Cao B, et al. Exploring subtypes and correlates of Internet gaming disorder severity among adolescents during COVID-19 in China: a latent class analysis. Curr Psychol. 2022:1–12. https://doi.org/10.1007/s12144-022-03133-8.
Wu Q, Luo T, Tang J, Wang Y, Wu Z, Liu Y, et al. Gaming in China before the COVID-19 pandemic and after the lifting of lockdowns: a nationwide online retrospective survey. Int J Ment Health Addict. 2022:1–13. https://doi.org/10.1007/s11469-022-00792-3.
Teng Z, Pontes HM, Nie Q, Griffiths MD, Guo C. Depression and anxiety symptoms associated with internet gaming disorder before and during the COVID-19 pandemic: a longitudinal study. J Behav Addict. 2021;10(1):169–80.
Galán JG, Pérez CL, López JÁM. Exploratory study on video game addiction of college students in a pandemic scenario. NAER: J New Approaches Educ Res. 2021;10(2):330–46.
Duong X-L, Liaw S-Y. Determinants of online shopping addiction among Vietnamese university students. J Hum Behav Soc Environ. 2022;32(3):402–14.
Zaman M, Babar MS, Babar M, Sabir F, Ashraf F, Tahir MJ, et al. Prevalence of gaming addiction and its impact on sleep quality: a cross-sectional study from Pakistan. Ann Med Surg. 2022;78: 103641.
Fazeli S, Zeidi IM, Lin C-Y, Namdar P, Griffiths MD, Ahorsu DK, et al. Depression, anxiety, and stress mediate the associations between internet gaming disorder, insomnia, and quality of life during the COVID-19 outbreak. Addict Behav Rep. 2020;12: 100307.
She R, Wong K, Lin J, Zhang Y, Leung K, Yang X. Profiles of stress and coping associated with mental, behavioral, and Internet use problems among adolescents during the COVID-19 pandemic: a stratified random sampling and cluster analysis. Front Public Health. 2022;10:1–11, Article ID: 826911.
Forster M, Rogers CJ, Sussman S, Watts J, Rahman T, Yu S, et al. Can adverse childhood experiences heighten risk for problematic internet and smartphone use? Findings from a college sample. Int J Environ Res Public Health. 2021;18(11):5978.
• Koós M, Demetrovics Z, Griffiths MD, Bőthe B. No significant changes in addictive and problematic behaviors during the COVID-19 pandemic and related lockdowns: a three-wave longitudinal study. Front Psychol. 2022;13:1–12, Article ID: 837315. (This is a high methodological quality, population-based study with considerable sample size assessing different kinds of behavioral addictions. This is notable that this study used a longitudinal study with three wave assessment.)
Claesdotter-Knutsson E, André F, Håkansson A. Gaming activity and possible changes in gaming behavior among young people during the COVID-19 pandemic: cross-sectional online survey study. JMIR Serious Games. 2022;10(1): e33059.
Amerio A, Stival C, Lugo A, Fanucchi T, Gorini G, Pacifici R, et al. COVID-19 lockdown: the relationship between trait impulsivity and addictive behaviors in a large representative sample of Italian adults. J Affect Disord. 2022;302:424–7.
Salerno L, Pallanti S. COVID-19 related distress in gambling disorder. Front Psych. 2021;12:620661.
Xuereb S, Kim HS, Clark L, Wohl MJ. Substitution behaviors among people who gamble during COVID-19 precipitated casino closures. Int Gambl Stud. 2021;21(3):411–25.
Håkansson A. Impact of COVID-19 on online gambling–a general population survey during the pandemic. Front Psychol. 2020;11:1–8, Article ID: l. 11:568543.
Månsson V, Wall H, Berman AH, Jayaram-Lindström N, Rosendahl I. A longitudinal study of gambling behaviors during the COVID-19 pandemic in Sweden. Front Psychol. 2021;12:1–9, Article ID:708037.
Claesdotter-Knutsson E, Håkansson A. Changes in self-reported web-based gambling activity during the COVID-19 pandemic: cross-sectional study. JMIR Serious Games. 2021;9(4): e30747.
Håkansson A, Widinghoff C. Changes of gambling patterns during COVID-19 in Sweden, and potential for preventive policy changes. A second look nine months into the pandemic. Int J Environ Res Public Health. 2021;18(5):2342.
Håkansson A, Jönsson C, Kenttä G. Psychological distress and problem gambling in elite athletes during COVID-19 restrictions—a web survey in top leagues of three sports during the pandemic. Int J Environ Res Public Health. 2020;17(18):6693.
Håkansson A. Changes in gambling behavior during the COVID-19 pandemic—a web survey study in Sweden. Int J Environ Res Public Health. 2020;17(11):4013.
Wardle H, Donnachie C, Critchlow N, Brown A, Bunn C, Dobbie F, et al. The impact of the initial COVID-19 lockdown upon regular sports bettors in Britain: findings from a cross-sectional online study. Addict Behav. 2021;118:106876.
Sharman S, Roberts A, Bowden-Jones H, Strang J. Gambling in COVID-19 lockdown in the UK: depression, stress, and anxiety. Front Psych. 2021;12:621497.
Lischer S, Steffen A, Schwarz J, Mathys J. The influence of lockdown on the gambling pattern of Swiss casinos players. Int J Environ Res Public Health. 2021;18(4):1973.
Gainsbury SM, Swanton TB, Burgess MT, Blaszczynski A. Impacts of the COVID-19 shutdown on gambling patterns in Australia: consideration of problem gambling and psychological distress. J Addict Med. 2021;15(6):468.
Serra G, Scalzo LL, Giuffrè M, Ferrara P, Corsello G. Smartphone use and addiction during the coronavirus disease 2019 (COVID-19) pandemic: cohort study on 184 Italian children and adolescents. Ital J Pediatr. 2021;47(1):1–10.
Indrakusuma AABP, Sayoga IMA, Surya SC, Indrayani AW, Artini IGA. The association between smartphone addiction and insomnia incidence in students of the faculty of medicine Udayana University batch of 2020 during the coronavirus disease-19 pandemic. Open Access Maced J Med Sci. 2021;9(B):1207–14.
Zhang C, Zeng P, Tan J, Sun S, Zhao M, Cui J, et al. Relationship of problematic smartphone use, sleep quality, and daytime fatigue among quarantined medical students during the COVID-19 pandemic. Front Psychiatry. 2021;12:1–10, Article ID:755059.
Hu T, Wang Y, Lin L, Tang W. The mediating role of daytime sleepiness between problematic smartphone use and post-traumatic symptoms in COVID-19 home-refined adolescents. Child Youth Serv Rev. 2021;126: 106012.
Zhao L, Hounnaklang N, editors. Association between smartphone addiction and mental health during the COVID-19 pandemic 2021 among inner mongolia medical university students, China. 2021 the 3rd Int Conf Intell Med Health; 2021;115–24.
Elhai JD, Yang H, McKay D, Asmundson GJ. COVID-19 anxiety symptoms associated with problematic smartphone use severity in Chinese adults. J Affect Disord. 2020;274:576–82.
Duan L, He J, Li M, Dai J, Zhou Y, Lai F, et al. Based on a decision tree model for exploring the risk factors of smartphone addiction among children and adolescents in China during the COVID-19 pandemic. Front Psych. 2021;12: 652356.
Saadeh H, Al Fayez RQ, Al Refaei A, Shewaikani N, Khawaldah H, Abu-Shanab S, et al. Smartphone use among university students during COVID-19 quarantine: an ethical trigger. Front Public Health. 2021;9:1–11, Article ID:600134.
Hosen I, Al Mamun F, Sikder MT, Abbasi AZ, Zou L, Guo T, et al. Prevalence and associated factors of problematic smartphone use during the COVID-19 pandemic: a Bangladeshi study. Risk Manag Healthc Policy. 2021;14:3797.
Sfeir E, Hallit S, Akel M, Salameh P, Obeid S. Smartphone addiction and personality traits among Lebanese adults: the mediating role of self-esteem. Psychol Health Med 2021:1–11. https://doi.org/10.1080/13548506.2021.1995886.
Perez-Siguas R, Seminario-Unzueta R, Matta-Solis H, Yauri-Machaca M, Matta-Solis E. Problematic use of mobile phones during the COVID-19 pandemic in Peruvian University students, 2020. Int J Adv Comput Sci Appl. 2020;11(12):445–50.
Duran S, Kaynak S. Insomnia in adults during COVID-19 pandemic and its association with social media addiction. Journal of Turkish Sleep Medicine. 2022;9:180–5.
Luo T, Chen W, Liao Y. Social media use in China before and during COVID-19: preliminary results from an online retrospective survey. J Psychiatr Res. 2021;140:35–8.
Lin C-Y, Broström A, Griffiths MD, Pakpour AH. Investigating mediated effects of fear of COVID-19 and COVID-19 misunderstanding in the association between problematic social media use, psychological distress, and insomnia. Internet Interv. 2020;21:100345.
• Panno A, Carbone GA, Massullo C, Farina B, Imperatori C. COVID-19 related distress is associated with alcohol problems, social media and food addiction symptoms: insights from the Italian experience during the lockdown. Front Psych. 2020;11: 577135. ((This is a methodological high quality, population based study with considerable sample size assessing different kinds of behavioral addictions).)
Borisenkov MF, Popov SV, Smirnov VV, Gubin DG, Petrov IM, Vasilkova TN, et al. Association between food addiction and time perspective during COVID-19 isolation. Eat Weight Disord-Stud Anorexia, Bulimia Obes. 2022;27(5):1585–91.
da Silva Júnior AE, de Lima Macena M, de Oliveira ADS, Praxedes DRS, de Oliveira Maranhão Pureza IR, de Menezes Toledo Florêncio TM, et al. Prevalence of food addiction and its association with anxiety, depression, and adherence to social distancing measures in Brazilian university students during the COVID-19 pandemic: a nationwide study. Eat Weight Disord-Stud Anorexia, Bulimia Obes. 2022;27:2027–35.
Schulte EM, Kral TV, Allison KC. A cross-sectional examination of reported changes to weight, eating, and activity behaviors during the COVID-19 pandemic among United States adults with food addiction. Appetite. 2022;168: 105740.
Zielińska M, Łuszczki E, Bartosiewicz A, Wyszyńska J, Dereń K. The prevalence of “Food Addiction” during the COVID-19 pandemic measured using the Yale Food Addiction Scale 2.0 (YFAS 2.0) among the adult population of Poland. Nutrients. 2021;13(11):4115.
Caponnetto P, Maglia M, Prezzavento GC, Pirrone C. Sexual addiction, hypersexual behavior and relative psychological dynamics during the period of social distancing and stay-at-home policies due to COVID-19. Int J Environ Res Public Health. 2022;19(5):2704.
Ceci F, Di Carlo F, Burkauskas J, Salone A, De Luca I, Cicconcelli D, et al. Physical activity and exercise addiction during the COVID-19 pandemic in Italy. Int J Ment Health Addict. 2022:1–21. https://doi.org/10.1007/s11469-022-00815-z.
Cataldo I, Burkauskas J, Dores AR, Carvalho IP, Simonato P, De Luca I, et al. An international cross-sectional investigation on social media, fitspiration content exposure, and related risks during the COVID-19 self-isolation period. J Psychiatr Res. 2022;148:34–44.
• de la Vega R, Almendros LJ, Barquín RR, Boros S, Demetrovics Z, Szabo A. Exercise addiction during the COVID-19 pandemic: an international study confirming the need for considering passion and perfectionism. Int J Ment Health Addict. 2020:1–12. (This is a methodological high-quality, population-based study with considerable sample size assessing exercise addictions. The other strength of this study is gathering data from multi countries with cultural differences.)
Berengüí R, López-Gullón JM, Angosto S. Physical sports activities and exercise addiction during lockdown in the Spanish population. Int J Environ Res Public Health. 2021;18(6):3119.
Hussain MW, Mirza T, Hassan MM. Impact of COVID-19 pandemic on the human behavior. Int J Educ Manag Eng. 2020;10(8):35–61.
Alimoradi Z, Lin C-Y, Broström A, Bülow PH, Bajalan Z, Griffiths MD, et al. Internet addiction and sleep problems: a systematic review and meta-analysis. Sleep Med Rev. 2019;47:51–61.
Patel VK, Chaudhary P, Kumar P, Vasavada DA, Tiwari DS. A study of correlates of social networking site addiction among the undergraduate health professionals. Asian J Soc Health Behav. 2021;4(1):30.
Kadavala BN, Vasavada DA, Kumar P, Bhatt RB, Patel VK, Tiwari DS. A multicenter study on problematic pornography consumption: prevalence and correlates among undergraduate medical students. Asian J Soc Health Behav. 2021;4(3):122.
Kwok C, Leung PY, Poon KY, Fung XC. The effects of internet gaming and social media use on physical activity, sleep, quality of life, and academic performance among university students in Hong Kong: a preliminary study. Asian J Soc Health Behav. 2021;4(1):36.
Pengpid S, Peltzer K. Anxiety-induced sleep disturbances among in-school adolescents in the United Arab Emirates: prevalence and associated factors. Asian J Soc Health Behav. 2022;5(1):18.
Yekaninejad MS, Badrooj N, Vosoughi F, Lin CY, Potenza MN, Pakpour AH. Prevalence of food addiction in children and adolescents: a systematic review and meta-analysis. Obes Rev. 2021;22(6): e13183.
Lin C-Y, Imani V, Griffiths MD, Pakpour AH. Validity of the Yale Food Addiction Scale for Children (YFAS-C): classical test theory and item response theory of the Persian YFAS-C. Eat Weight Disord-Stud Anorexia, Bulimia Obes. 2021;26(5):1457–66.
Lin C-Y, Cheung P, Imani V, Griffiths MD, Pakpour AH. The mediating effects of eating disorder, food addiction, and insomnia in the association between psychological distress and being overweight among Iranian adolescents. Nutrients. 2020;12(5):1371.
Ahorsu DK, Lin CY, Imani V, Griffiths MD, Su JA, Latner JD, et al. A prospective study on the link between weight-related self-stigma and binge eating: role of food addiction and psychological distress. Int J Eat Disord. 2020;53(3):442–50.
Snagowski J, Brand M. OR-82: Approach and avoidance tendencies in cybersex addiction: adaption of an Approach-Avoidance-Task with pornographic stimuli. J Behav Addict. 2015;4(S1):37–9.
Kamolthip R, Chirawat P, Ghavifekr S, Gan WY, Tung SE, Nurmala I, et al. Problematic Internet use (PIU) in youth: a brief literature review of selected topics. Curr Opin Behav Sci. 2022;46: 101150.
Chang K-C, Chang Y-H, Yen C-F, Chen J-S, Chen P-J, Lin C-Y, et al. A longitudinal study of the effects of problematic smartphone use on social functioning among people with schizophrenia: mediating roles for sleep quality and self-stigma. J Behav Addict. 2022;11(2):567–76.
Escardíbul J-O, Mora T, Villarroya A. Peer effects on youth screen media consumption in Catalonia (Spain). J Cult Econ. 2013;37(2):185–201.
Jiménez-Murcia S, Fernández-Aranda F. COVID-19 and behavioral addictions: worrying consequences? Eur Neuropsychopharmacol. 2022;56:77.
Funding
Open access funding provided by Jönköping University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects.
Additional information
Preregistration
This study’s design and analysis plan were preregistered; see https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=330898.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Emotion and Addiction
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alimoradi, Z., Lotfi, A., Lin, CY. et al. Estimation of Behavioral Addiction Prevalence During COVID-19 Pandemic: A Systematic Review and Meta-analysis. Curr Addict Rep 9, 486–517 (2022). https://doi.org/10.1007/s40429-022-00435-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40429-022-00435-6