
Abstract
Background
A successful pandemic response in populated geographies and resource-limited settings like India relies on informed decision making. Knowledge, attitudes, and practices (KAP) studies performed during these times are crucial to illustrate how well a community adopts prevention strategies.
Objective
The present study, conducted during the peak months of the first wave of the COVID-19 pandemic, aimed at assessing the KAP levels of internet-savvy Indians.
Methods
This observational cross-sectional study was conducted between 20 May and 10 October 2020. We employed a self-reported questionnaire using Google Forms, containing two parts—demographics and KAP evaluation—with the latter having three subsections of 10, 5, and 5 questions each. Data from completed questionnaires were extracted and exported from Google Forms and coded. Descriptive statistics and first-order analysis were conducted. Binary logistic regression was performed with a 95% confidence interval to determine significant associations between categorical dependent and independent variables.
Results
We received responses from 1154 participants (58.84% male). Most respondents had good knowledge of the disease transmission course (92.55%), showed seriousness towards the emerging illness (91.07%), had a good attitude towards personal hygiene and physical distancing (93.76%), and had followed good safety/hygienic practices (93.76%). Good attitudes differed significantly between Karnataka and Tamil Nadu provinces (OR 1.053; 95% CI 0.588–1.886; p = 0.0439). The survey participants did not show any significant gender differences in any question types (p > 0.05).
Conclusions
The results obtained add significant value to the existing KAP literature on COVID-19 in India and may help policymakers achieve public compliance with preventive measures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Resource-limited countries like India have faced massive crises during the COVID-19 pandemic. |
People’s adherence to preventive measures is critical for effective response plans. |
Knowledge, attitudes, and practices (KAP) levels reflect how well the governmental institutions convey risk messaging. |
Locality, province, and designation played a crucial role in the study population. |
Findings give policymakers insights into public perceptions during the second wave. |
Introduction
As of January 21, 2022, India had recorded over 38 million cases of 2019 coronavirus disease (COVID-19). With over 488 thousand deaths to date, the country is ranked second only to the United States [1]. The Institute for Health Metrics and Evaluation projects over 3 million estimated deaths attributable to COVID-19 (including unreported deaths) by May 1, 2022 [2]. The May 2021 Editorial of a leading international medical journal warned about the emerging dangers of exponential disease spread in India [3].
While COVID-19 has shattered health systems and overburdened healthcare workers worldwide; the impact is much worse in populated geographies and resource-limited settings [4]. Even the leaders of developed economies made policy mistakes and showed inept governance in tackling the outbreak [5]. Irrespective of some laudable efforts by certain governmental bodies, public support is crucial in halting the ‘super spreaders’. A successful pandemic response relies on informed decision making at all levels—governmental, societal, and individual. Thus, people’s adherence to preventive measures is critical for an effective response plan [6].
The hunt for pharmacological solutions to end the pandemic is being prioritized, with new vaccines and repurposed use of existing drugs. However, non-pharmacological interventions aimed at preventing infection are still proven methods of restricting new outbreak clusters [7]. Movement control measures are deemed necessary to curb the viral spread, but panic buying and a sudden rise in crowded transportation during the short, restriction-free, pre-lockdown phase, and mass gatherings after the initial spread from China, significantly helped to hike case numbers throughout the world [8]. It became vital to recognize people’s frustration and encourage informed protective strategies to lessen panic scenarios and expedite pandemic control. Publicizing correct information and listening to people’s concerns are two sides of the same coin that both help achieve the desired objective [9].
Cultural attributes, knowledge, personal control, scientific uncertainty, faith in government, trust in health system capabilities, and communication channels all influence people’s perception of and response to risk messaging [10]. Social isolation, social stigma, psychological impact, economic barriers, and health equity significantly affect willingness to support institutional measures [10]. Ample public knowledge on the disease course, chief signs and symptoms, and transmission patterns have proven effective in infection control throughout history. Positive attitudes towards following physical distancing, taking precautionary measures against community spread, and relying on science-driven evidence help people resist false propaganda or misinformation during this unprecedented time. Appropriate practicing of preventive tactics and accepting local behavioral recommendations may substantially assist the globally synchronized mitigation efforts [11].
Recently, a good number of studies on knowledge, attitudes, and practice (KAP) towards COVID-19 among the public have emerged across India. Conducting KAP studies in such fragile situations is crucial since these studies illustrate how well a community embraces behavioral change strategies by governmental agencies and support decision making and implementation plans designed for the rising infection caseload. These findings help authorities to understand public perception and pinpoint societal characteristics to inform health promotion activities and prevention efforts [6]. Hence, we conducted the present study during the peak months of the first wave of the COVID-19 pandemic to assess the KAP levels of internet-savvy Indians. The study aimed to add significant value to the existing but slowly growing KAP literature on COVID-19 among the Indian population. Since the country is currently facing a massive second wave, these findings provide policymakers with profound insights into public perceptions and values.
Materials and methods
Study design and setting
This self-reported, questionnaire-based, observational, cross-sectional study was conducted between 20 May and 10 October 2020 among participants from various states of India.
Participants and sampling
Adult (aged ≥ 18 years) internet users who could access our survey questionnaire using any electronic device, who resided in any states/provinces of India, and who could understand and communicate in English were considered the target population for the survey. The following categories of population were excluded: (i) children, (ii) non-resident Indians or foreign citizens, (iii) those who could not understand or communicate in English, and (iv) non-internet users or those who could not access the electronic survey. A snowball technique was used for sampling, with initial responders helping to recruit further participants. Participation in the survey was voluntary, and no monetary or non-monetary incentives were provided.
Measurement tool and validation
We developed a self-reported KAP questionnaire based on a comprehensive literature search for similar documented studies across the globe. Two authors (JM and OR) performed a thorough review to check for validity and relevance. A third author (KR) assisted when there were issues with arriving at a consensus. All three tweaked the questionnaire further to include only the key points. A reliability coefficient analysis was conducted for KAP questions with 10 participants as a pre-test, and the overall Cronbach’s alpha coefficient was found to be > 0.7, suggesting acceptable internal consistency.
Questionnaire administration and data collection
The final version of the questionnaire used for the online survey was conducted through Google Forms (https://docs.google.com/forms/d/e/1FAIpQLSctk7gyUa3kUv1tVYt0ANSoJGAjRIRcIMRHqFsTkM5D5kTeg/viewform?usp=sf_link). The data from the pilot study were not included in the final analysis. Because of the state-imposed pandemic-related movement restrictions, community-based in-person interviews were not considered workable. Social media applications such as WhatsApp and Telegram were used for distribution alongside direct email communications.
The opening part of the online questionnaire conveyed the research aims and sought informed consent while detailing the voluntary nature of participation, confidentiality, and protection of personal information. Participants could not proceed to survey questions unless they provided voluntarily consent.
Questionnaire content, scoring method, and variables
The questionnaire instrument was broadly divided into two parts: demographics and KAP evaluation, with the latter having three subsections with 10, 5, and 5 questions each. We followed a modified version of the scoring method published elsewhere [12]. Figure 1 depicts the characteristics and scoring pattern of the questionnaire. Variables were summarized as frequency and percentage. The knowledge-related section included questions on virus spread, disease severity, public fear, viral transmission through surfaces of objects, symptoms and manifestations, prevention, and physical distancing. Attitude-based questions included pandemic handling, transmission prevention, and other pandemic-related attitudes. Practice-based questions covered topics on mask wearing, taking natural remedies, going to crowded places, and covering nose and mouth while sneezing or coughing.

Characteristics and scoring pattern of the questionnaire
All participants who completed the survey were given an electronic appreciation certificate. We also provided a two-page COVID-19 awareness brochure developed using evidence-based content from the World Health Organization and Ministry of Health and Family Affairs (MoHFW), Government of India (GoI).
Sample size and bias mitigation
Raosoft® (http://www.raosoft.com/samplesize.html) was used for sample size estimation. A sample of 289 was considered sufficient (95% confidence interval [CI], 5% margin of error); however, we allowed for maximum responses until the end of the data collection period, as suggested by a similar KAP study on COVID-19 [6]. Being an electronic survey with snowball sampling, there is a chance the sample population would mainly be distributed within the researchers’ network. To prevent that, we tried to circulate the questionnaire link through social media platforms.
Data handling and statistical analysis
Incomplete questionnaires were not considered for analysis. Data from completed questionnaires were extracted and exported from Google Forms and coded using Microsoft Excel 2016 (v16.0). SAS version 9.4 was used for statistical analyses. Descriptive statistics (frequencies, percentages) and first-order analyses (i.e., chi-square tests) were performed. Binary logistic regression was performed with a 95% CI to determine significant associations between categorical dependent and independent variables.
Results
Participant characteristics
During the data collection period of over 4.5 months, we received responses from 1154 participants. Most of them were female (58.84%), students (80.68%) in undergraduate courses (67.94%), aged between 18–28 years (89.77%), hailing from the southern state of Tamil Nadu (TN, 78.68%), and from a rural locality (62.22%). Table 1 provides the demographic characteristics of the survey participants.
Knowledge of COVID-19 among study participants
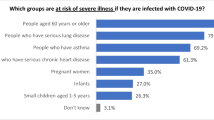
Table 2 presents the knowledge results of the KAP questions on COVID-19. Most respondents knew the correct information on the disease transmission course (92.55%) and showed seriousness towards the emerging illness (91.07%). Many had good knowledge about the chief respiratory manifestations of COVID-19, such as cold, cough and shortness of breath (97.31%), and 72.70% believed in the potential impact of wearing face masks to limit COVID-19 transmission. Sixty-three percent of participants accurately answered when asked about whether the infection was airborne. Seventy-one percent concurred that the elderly, those with chronic diseases, and obese people are vulnerable. Furthermore, 95.84% of participants understood that COVID-19 infection spreads through contacts, and that physical isolation for at least 14 days is required post-infection. No statistical significance was observed between male and female participants in relation to the knowledge questions.
Attitude towards COVID-19 among study participants
Table 3 lists the results of the attitude survey. Most respondents (93.76%) had a good attitude towards personal hygiene and physical distancing, and 47.83% disagreed that COVID-19 is the first pandemic that the world has faced. Most participants considered COVID-19 as a bio-war (61.09%), but only 26.08% disagreed that this pandemic will be successfully controlled. Sixty-eight percent agreed that the GoI had handled the health crisis well. There were no significant gender differences observed for questions related to attitude.
Behavioral intentions and prevention practices of study participants
Table 4 displays the survey results on prevention practices against COVID-19. The majority of participants (93.76%) had followed good personal safety hygienic practices during the study period, with 83.36% avoiding crowded places during the relaxation of movement control procedures by the state. Eighty-nine percent of respondents wore a mask while away from their place of residence. Interestingly, 77.04% of participants took natural remedies as a preventive measure, while the proper disposal of used tissues was strictly followed by 84.84%. Similar to the knowledge and attitude questions, the survey participants did not show any significant gender differences in responding to practice-related questions.
Distribution and risk factors
Table 5 provides the distribution of KAP responses relevant to demographic factors such as gender, age, academic qualification, locality, state, and designation. The proportion of good knowledge was significantly higher in survey participants from Karnataka (100% vs 93.28% for TN; p = 0.0086) but Karnataka participants had a lower proportion of good attitude (13.89% vs 16.52%, p = 0.0401) than those from TN. Good attitude differed significantly between Karnataka and TN provinces (OR 1.053; 95% CI 0.588–1.886; p = 0.0439). The proportion of good practice was significantly higher among participants living in an urban locality (87.84% vs 82.03% in rural areas; p = 0.0086) and those with a faculty designation (93.83% vs 78.18% with other designations; p = 0.0228). For practice-related questions, locality (rural vs urban: OR 0.632; 95% CI 0.448–0.892; p = 0.0090) and designation (faculty vs others: OR 4.244; 95% CI 1.503–11.981; p = 0.0306) were found to be significantly different.
Discussion
The present study assessed KAP levels of internet-savvy Indians during the high-caseload period of the current pandemic’s first wave. The findings offer important insights into people’s response to COVID-19, and stress the need to understand population behavior in order to create uncompromised risk messaging strategies.
Internet users were our survey population. In the current technological era, people seek medical information through internet searches; some even develop ‘cyberchondria’—the anxiety of knowing ones health status through such means. Notably, over 60% of the study sample (n = 767) in a remote northeastern Indian province preferred using social media platforms to find out COVID-19-related information, with over 50% of them spending around an hour daily using this medium [13].
The KAP levels of a community reflect how well the governmental institutions convey risk messaging. Governmental actions against the pandemic in India primarily involved a stringent lockdown; however, the economic impacts on society resulted in a less successful exit strategy, causing high case rates and tougher resource utilization [14]. On September 19, 2021, the Oxford COVID-19 Government Response Tracker reported a stringency level of 65.28 for India [15]. Interestingly, in our study, only 14.5% disagreed that the GoI had performed well. The MoHFW took several commendable steps. ‘Arogya Setu,’ the mHealth app, was a prominent initiative for disease containment, featuring COVID-19 tracking and advice on infection management. The GoI’s first participatory disease surveillance offers geotagging of cases, helps risk assessment, and necessitates precautionary measures. It was well received by the population, with more than 50% of users offering 4+ ratings [16, 17]. In addition, as of October 19, 2021, about 98,67,69,411 doses of a COVID-19 vaccine had been administered in the country [18].
The MoHFW also issued several health guidelines, travel advisories, training and awareness materials, promotional audio-visuals, and inspirational messages on tackling COVID-19 [18]. All these knowledge-building resources have educated the public. A significantly higher portion of our survey respondents (over 90%) had good knowledge of disease spread, contact handling, and physical isolation. The fact that students were the dominant sample (80.68%) may be the reason for such a significant response to knowledge-related questions, and they might have benefited from these resources. The results of a large randomized controlled trial with over 8000 younger Indians suggested that such educational interventions needed to be longer and science-based [19]. In contrast, a study from neighboring Bangladesh reported that slum dwellers (n = 406) showed inadequate knowledge and poor attitude toward handling the pandemic [20]. All our survey respondents received a comprehensive awareness brochure on COVID-19; as health care professionals and public health enthusiasts, this is a small but essential step to ensure our shared efforts in implementing measures to curtail the disease spread.
Our study had more responders (62.22%) from rural localities. It is worth noting that over 50% of the Indian population lives in rural areas [21]. Participants from urban areas had a better practice score (87.84% vs 82.03% in rural areas; p = 0.0086). Urban localities faced hard times during the first-wave lockdowns and were the first to encounter the significant threats of COVID-19 [22]. However, the urban-to-rural transmission of the infection was considered a substantial reason for the countrywide case increase. The misery caused by the pandemic was doubled by economic strangulation. Many domestic migrants walked long distances from industrial cities to their rural hometowns, which became a cause for concern [21, 23]. Unfortunately, the rural communities have unique difficulties in managing disease mitigation with not-so-proficient health infrastructure and endemic poverty [24].
An extensive survey of over 20,000 Indian adults highlighted the need to extend the knowledge base to improve livelihood resilience and societal behavioral response in the battle against COVID-19 [25]. Another study with a sample of 1666 Indians reported that there were knowledge differences between men and women; the results emphasized the need for gender-sensitive risk messaging for better behavioral change [26]. We did not find any gender differences in any of the question types.
Asirvatham et al. conducted a fatality analysis from TN, where our study sample was the largest, and warned that older men living in densely populated areas and those with pre-existing comorbidities were vulnerable to COVID-19 [27]. The authors hinted that the time interval between symptom onset and hospitalization might affect mortality rates [27]. In our sample, there were no significant age differences observed for any question types. However, the increase in positive attitude with increasing age was observed in another online-based COVID-19-related KAP study (n = 1008) from TN [28]. Another KAP study from South India (n = 6119) conducted during the initial months of COVID-19 spread noted that high-risk elderly populations and individuals with poor educational backgrounds had lower knowledge scores [29]. In the present work, participants with a faculty designation (93.83% vs 78.16% with other designations; p = 0.0228) had better practice scores.
Most of our study population showed good safety/hygienic practices (93.76%), avoided crowded places (83.36%), wore a mask (89.08%), and properly disposed of used tissues (84.84%). These pandemic-appropriate preventive, self-care procedures, along with routine exercises including yoga and positive mental health, are crucial in this delicate situation [30]. Remarkably, the MoHFW has introduced a toll-free helpline for psychosocial assistance to citizens to enhance behavioral health and relieve mental stress during the pandemic. The current vaccine drive may assist the GoI’s efforts alongside these existing measures to speed up the fight to end the pandemic [18].
The study has several limitations. Self-reported surveys may pose issues of bias, exaggeration or deception. Only English-speaking internet users took part, and hence the sample might not represent the entire country. This is a general restraint for any electronic survey. Despite adopting a comparatively lengthy study period (over 4 months), we had limited sample representativeness, unlike one Indian study that collected data from a similar sample population in only 3 days [31]. The lockdown restrictions and their associated psychosocial effects might be the reason behind the slow turnaround. Importantly, the findings may not be generalized due to the sampling method, electronic administration of the instrument, and sample population being internet users. Most of the study participants were from TN (78.68%), suggesting a biased sample population selection that might have generated from the researchers’ networks. Also, the KAP assessment may be imprecise due to the scant variables. A detailed study may be required to identify and rectify such issues. We did not cover KAP questions on COVID-19 vaccines since they were not readily available during the first wave. Knowledge and preferences towards vaccine usage may require a dedicated survey. Lastly, the pandemic scenarios in India are entirely different between waves; the currently occurring second wave is more complicated with an increased struggle for hospital beds, oxygen, drugs, and medical equipment. The KAP levels of the public and their opinion about GoI functioning may therefore vary over time. Assessing the KAP levels again during the subsequent waves and comparing them with the first wave would be of interest.
Conclusions
We comprehensively evaluated the KAP scores of internet-savvy Indians during the first wave of COVID-19 in the country. The findings suggested that the study population had good knowledge of the pandemic and was associated with better practice measures during the crisis. Locality, province and designation played a crucial role in mean KAP scores. Attitudes towards addressing the pandemic need to be improved. These KAP scores may direct policy makers to plan and execute more people-centric preventive and intervention strategies. Health education programs and efficient risk messaging may be essential to promote optimistic attitudes, behavioral changes, and to avoid misconceptions.
References
Worldometer. Reported cases and deaths by country or territory. https://www.worldometers.info/coronavirus/#countries (updated: January 21, 2022; accessed: January 21, 2022).
Institute for Health Metrics and Evaluation. COVID-19 projections: India—cumulative deaths. https://covid19.healthdata.org/india?view=cumulative-deaths&tab=trend (updated: January 14, 2022; accessed: January 21, 2022).
Lancet T. India’s COVID-19 emergency. Lancet. 2021;397(10286):1683.
Ebrahim SH, Ahmed QA, Gozzer E, et al. Covid-19 and community mitigation strategies in a pandemic. BMJ. 2020;368:m1066.
Memish ZA, Ebrahim SH, Kattan RF, et al. Leadership to prevent COVID-19: Is it the most important mitigation factor? Travel Med Infect Dis. 2020;38: 101925.
Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Health. 2020;8:217.
Chowdhury R, Luhar S, Khan N, et al. Long-term strategies to control COVID-19 in low and middle-income countries: an options overview of community-based, non-pharmacological interventions. Eur J Epidemiol. 2020;35(8):743–8.
Azlan AA, Hamzah MR, Sern TJ, et al. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS ONE. 2020;15(5): e0233668.
Al-Hasan A, Yim D, Khuntia J. Citizens’ adherence to COVID-19 mitigation recommendations by the government: a 3-country comparative evaluation using web-based cross-sectional survey data. J Med Internet Res. 2020;22(8): e20634.
Malecki KMC, Keating JA, Safdar N. Crisis communication and public perception of COVID-19 risk in the era of social media. Clin Infect Dis. 2021;72(4):697–702.
Ghaderi E, Mahmoodi H, Sharifi Saqqezi P, et al. Knowledge, attitudes, practices and fear of COVID-19 among Iranians: a quick online survey. Health Soc Care Community. 2021. https://doi.org/10.1111/hsc.13382.
Ferdous MZ, Islam MS, Sikder MT, et al. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS One. 2020;15(10): e0239254.
Bala R, Srivastava A, Ningthoujam GD, et al. An observational study in Manipur state, India on preventive behavior influenced by social media during the COVID-19 pandemic mediated by cyberchondria and information overload. J Prev Med Public Health. 2021;54(1):22–30.
Goel I, Sharma S, Kashiramka S. Effects of the COVID-19 pandemic in India: an analysis of policy and technological interventions. Health Policy Technol. 2021;10(1):151–64.
Oxford University. Oxford COVID-19 Government Response Tracker: Stringency Scatter for India. https://covidtracker.bsg.ox.ac.uk/stringency-scatter (updated: September 19, 2021; accessed: October 19, 2021).
Garg S, Bhatnagar N, Gangadharan N. A case for participatory disease surveillance of the COVID-19 pandemic in India. JMIR Public Health Surveill. 2020;6(2): e18795.
Kodali PB, Hense S, Kopparty S, et al. How Indians responded to the Arogya Setu app? Indian J Public Health. 2020;64(Supp):S228–30.
Ministry of Health and Family Welfare, Government of India. COVID-19 Resources. https://www.mohfw.gov.in/ (updated: October 19, 2021; accessed: October 19, 2021).
Mistree D, Loyalka P, Fairlie R, et al. Instructional interventions for improving COVID-19 knowledge, attitudes, behaviors: evidence from a large-scale RCT in India. Soc Sci Med. 2021;276: 113846.
Islam S, Emran GI, Rahman E, et al. Knowledge, attitudes and practices associated with the COVID-19 among slum dwellers resided in Dhaka City: a Bangladeshi interview-based survey. J Public Health (Oxf). 2021;43(1):13–25.
Mishra S, Mohapatra A, Kumar R, et al. Restricting rural-urban connect to combat infectious disease epidemic as India fights COVID-19. J Family Med Prim Care. 2020;9(4):1792–4.
Pandey A, Saxena NK. Effectiveness of government policies in controlling COVID-19 in India. Int J Health Serv. 2022;52:30–7.
Kumar R. Migrant in my own country: the long march of migrant workers in India during the COVID-19 pandemic 2020—failure of postcolonial governments to decolonize Bihar and rebuild Indian civilization after 1947. J Family Med Prim Care. 2020;9(10):5087–91.
Dutta A, Fischer HW. The local governance of COVID-19: disease prevention and social security in rural India. World Dev. 2020;138: 105234.
Kaushik M, Agarwal D, Gupta AK. Cross-sectional study on the role of public awareness in preventing the spread of COVID-19 outbreak in India. Postgrad Med J. 2021;97:777–81.
Pinchoff J, Santhya KG, White C, et al. Gender specific differences in COVID-19 knowledge, behavior and health effects among adolescents and young adults in Uttar Pradesh and Bihar, India. PLoS One. 2020;15(12): e0244053.
Asirvatham ES, Sarman CJ, Saravanamurthy SP, et al. Who is dying from COVID-19 and when? An analysis of fatalities in Tamil Nadu, India. Clin Epidemiol Glob Health. 2021;9:275–9.
Kanagavelu AKS. Knowledge, attitude and practice towards COVID-19 among the general public in Tamil Nadu, India. Int J Community Med Pub Health. 2021;8(4):1935–44.
Christy JS, Kaur K, Gurnani B, et al. Knowledge, attitude and practise toward COVID-19 among patients presenting to five tertiary eye care hospitals in South India—a multicentre questionnaire-based survey. Indian J Ophthalmol. 2020;68(11):2385–90.
Joshi SR. COVID-19 care in India: evolving paradigms from public health to critical care. J Assoc Physicians India. 2020;68(10):56–8.
Dkhar SA, Quansar R, Saleem SM, et al. Knowledge, attitude, and practices related to COVID-19 pandemic among social media users in J&K, India. Indian J Public Health. 2020;64(Supp):S205–10.
Acknowledgements
We want to thank the management of JKK College of Pharmacy and staff of the Department of Pharmacy Practice, including the Head, Research Supervisor, Faculty, and Support Staff, for their support in the execution of this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The authors did not receive grants from any commercial, governmental, or non-profit organizations related to this work.
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
The study protocol, questionnaire, informed consent, and study participation and publication details, COVID-19 awareness brochure, and appreciation certificate were reviewed and approved by the JKK Nataraja Institutional Ethics Committee (IEC) with an ethical clearance certificate (number: JKKNCP/ETHICS_PRACTICE/020PDS11) on 17 Apr 2020.
Consent to participate/consent to publish
IEC-approved consent statements to participate and publish were introduced at the beginning of the questionnaire. Participants who voluntarily agreed to participate/publish proceeded further to answer the survey questions.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
Disclaimers
The opinions expressed in this article are the authors’ personal views and do not represent that of their affiliated organizations or associations.
Author contributions
KR and SR conceived the research idea. JM and OR designed the questionnaire, and KR helped to validate it. JM and OR conducted the pre-test analysis. SM performed the statistical analysis and interpreted the findings with inputs from KR and SR. JM and OR drafted the manuscript. HI reviewed, edited, and revised the manuscript and added substantial intellectual content. All authors read and approved the final version and agreed to submit it to Drugs & Therapy Perspectives for consideration.
Rights and permissions
About this article

Cite this article
Marudachalam, J., Ravichandhiran, O., Ramalingam, K. et al. Peak months of pandemic’s first-wave in India: a cross-sectional assessment of knowledge, attitudes and practice towards COVID-19 among internet-savvy individuals. Drugs Ther Perspect 38, 93–102 (2022). https://doi.org/10.1007/s40267-022-00899-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40267-022-00899-6