
Abstract
Background and Objective
Clavulanic acid is a commonly used β-lactam inhibitor in pediatrics for a variety of infections. Clear insight into its mode of action is lacking, however, and a target has not been identified. The dosing of clavulanic acid is currently based on that of the partner drug (amoxicillin or ticarcillin). Still, proper dosing of the compound is needed because clavulanic acid has been associated with adverse effects. In this systematic review, we aim to describe the current literature on the pharmacokinetics of clavulanic acid in the pediatric population
Methods
We performed a systematic search in MEDLINE, Embase.com, Cochrane Central, Google Scholar, and Web of Science. We included all published studies reporting pharmacokinetic data on clavulanic acid in neonates and children 0–18 years of age.
Results
The search resulted in 18 original studies that met the inclusion criteria. In general, the variation in drug exposure was large, which can be partly explained by differences in disease state, route of administration, or age. Unfortunately, the studies’ limited background information hampered in-depth assessment of the observed variability.
Conclusion
The pharmacokinetics of clavulanic acid in pediatric patients is highly variable, similar to reports in adults, but more pronounced. Significant knowledge gaps remain with regard to the population-specific explanation for this variability. Model-based pharmacokinetic studies that address both maturational and disease-specific changes in the pediatric population are therefore needed. Furthermore, additional pharmacodynamic studies are needed to define a clear target. The combined outcomes will eventually lead to pharmacokinetic-pharmacodynamic modeling of clavulanic acid and targeted exposure.
Clinical Trial Registration
PROSPERO CRD42020137253.
Similar content being viewed by others


This review illustrates the highly variable pharmacokinetics of clavulanic acid in the pediatric population. |
The observed variability can in part be explained by the maturational aspects that characterize these patients, in addition to the disease-specific aspects. |
Both the maturational and disease-specific aspects need to be further addressed, with currently available techniques, as the first step towards pharmacokinetic-pharmacodynamic modeling and subsequent targeted exposure of a very commonly used drug in pediatrics. |
1 Introduction
Infections remain one of the major causes of childhood morbidity and mortality worldwide [1]. Consequently, antibiotics are among the most commonly prescribed drugs, both in newborns and children [2, 3]. Although they are potentially life saving in many cases, increasing antibiotic resistance is one of the major downsides of the high prescription rate [4].
The first discovered natural antibiotic in the modern antibiotic era was penicillin, in 1928 by Fleming [5]. The period thereafter (1940–70) is considered to be ‘the golden era’ of antibiotic development as new antibiotics were discovered at a significantly higher pace [6]. Only a few classes of antibiotics have been discovered since then, including the oxazolidinones, pleuromutilins, and lipopeptides [7,8,9]. Unfortunately, reports on bacterial resistance already appeared in that same time period and have been increasing over time, being responsible for a substantial number of deaths each year [10].
β-Lactam antibiotics exhibit their bactericidal effect through the inhibition of cell wall synthesis, thereby causing cell lysis that eventually leads to bacterial death. Bacteria can acquire resistance against β-lactam antibiotics through the production of β-lactamase, which cleaves the β-lactam ring and thereby inactivates the drug [4]. The first β-lactamase, penicillinase, was identified in 1940 and today more than 850 β-lactamases have been reported [11]. Clavulanic acid is the first developed β-lactamase inhibitor, isolated from Streptomyces clavuligerus. It is considered a “suicide inhibitor” as it can permanently inactivate β-lactamase through secondary chemical reactions and complex formation [12]. Clavulanic acid on its own has a poor antimicrobial effect on its own but combining it with amoxicillin or ticarcillin can restore the efficacy spectrum against β-lactamase-producing bacteria. Different formulations are commercially available in varying ratios depending on the route of administration, the targeted pathogen, and availability in a country.
The mode of action of clavulanic acid is still poorly understood. It is thought that the β-lactamase inhibitor should reach the target site prior to or simultaneously with the partner antibiotic, thereby allowing maximum inhibition and preventing degradation of the partner drug. Therefore, in the case of oral administration, absorption should be fast and, for all routes of administrations, the distribution profile should be similar to that of the partner drug. The elimination rate should ideally also be comparable between both compounds, as this will influence the ratio between both compounds during the course of the dosing interval. Published pharmacokinetic studies on clavulanic acid in adults report a substantial variability in both healthy subjects and intensive care unit patients, as summarized in Table 1 of the Electronic Supplementary Material (ESM). Clavulanic acid is well absorbed after oral ingestion in adult men, with a mean bioavailability of 60%. Peak concentrations are reached on average 0.7–2.0 h after ingestion. Its metabolism is partly hepatic with plasma protein binding up to 30% and it is cleared through both renal and non-renal pathways [13, 14]. Clearance varies substantially, which cannot solely be explained by disease state. Given that the pediatric population represents a very heterogeneous population in whom developmental aspects related to maturation are present, one could expect that the pharmacokinetics of clavulanic acid in this population is even more variable than in adults. Current treatment strategies, both in adults and children, are mostly based on the amoxicillin component; and clavulanic acid-specific dosing regimens are lacking.
This, together with the lack of a clear pharmacodynamic clavulanic acid target hampers dose optimization of this extensively used drug in pediatrics. Awaiting better pharmacodynamic guidance, insight into the population-specific pharmacokinetic aspects of clavulanic acid would be the first step towards dose optimization. We therefore reviewed the available literature on the pharmacokinetics of clavulanic acid in the pediatric and neonatal population.
2 Methods
2.1 Search Strategy and Study Selection
This systematic review was performed in accordance with the Preferred Reported Items for Systematic Reviews and Meta-Analysis (PRISMA) [15]. We conducted a systematic search in MEDLINE, Embase.com, Cochrane Central, Google Scholar, and Web of Science up to 3 February, 2022. The search strategies, created with help of two biomedical information specialists, are presented in the ESM. Two reviewers (FK and GTS) independently screened titles and abstracts and reviewed the full text of potentially relevant articles. Disagreements were resolved by discussion or through consultation of a third investigator (KA). We included all studies and case reports reporting pharmacokinetic data on clavulanic acid in pediatric patients (preterm age to 18 years of age), and screened congress abstracts, reference lists, and reviews for additional studies. There were no restrictions on language or year of publication. Studies in participants > 18 years of age from which pediatric data could not be separated, in vitro studies, or studies performed in animals were excluded. The protocol has been registered in PROSPERO CRD42020137253.
2.2 Quality Assessment
FK and KA independently performed the quality assessment using the ClinPK statement, a descriptive tool without grading system, which has been developed for the assessment of quality and validity of clinical pharmacokinetic studies [16].
2.3 Data Extraction
Two authors (FK and KA) independently extracted data in a predefined extraction form. Extracted variables included study design, information on study population (age, body weight, indication for antibiotics, and disease severity), information on clavulanic acid dosing, co-administered β-lactam antibiotic and ratio, mode and route of administration, co-medication, sampling schedule, collected fluids, methods of analysis, data analysis, pharmacokinetic parameters, and side effects or adverse events. When data were provided in figures, observations were extracted using a digital tool (WebPlot Digitizer, Ankit Rohatgi, available online: https://automeris.io/WebPlotDigitizer) [17].
2.4 Data Analysis
We provide a formal narrative synthesis of the studies’ and patients’ characteristics. We extracted reported serum concentrations over time following administration of clavulanic acid and report these data in a descriptive manner for each individual study. If reported, mean concentrations over time are described. To harmonize data, all concentrations and area under the curve (AUC) values were corrected for dose (mg/kg) and converted to milligram per liter (mg/L) and mg × h/L, respectively. Clearance values were converted to L/h/kg if feasible. Urine concentrations or fraction of administered dose recovered in urine were extracted as well.
3 Results
3.1 Search and Included Studies
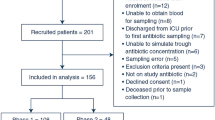
The search strategy yielded 2773 records of which 63 full texts were considered relevant based on title/abstract and screened for eligibility for this review. Eighteen articles were included in this systematic review. The flowchart in Fig. 1 shows the study selection. Included studies were published between 1982 and 2017, the majority before 2000, as illustrated in Fig. 2. The majority of studies solely reported pharmacokinetic findings. Some studies did also assess efficacy and safety aspects (adverse events). Characteristics of included studies are provided in Table 1.

Flowchart of the inclusion process. PK pharmacokinetics

Publications on the pharmacokinetics (PK) of clavulanic acid in pediatrics in time
3.2 Quality Assessment
Based on the application of the ClinPK tool, we concluded that most of the included papers reported relevant variables with regard to the drug preparation and dosing schedule as well as the pharmacokinetic sampling method and method of analysis. Yet, some reports were quite brief and lacked crucial information, especially with regard to patient characteristics and background. The complete assessment is included in the ESM. Assessing quality of the included studies following the current reporting guidelines is somewhat unfair as many aspects currently required in publications were not required in the past, and therefore probably not yet mentioned.
3.3 Study Population
Thirteen studies concerned children, with a range from 1 month to 18 years of age [18,19,20,21,22,23,24,25,26,27,28,29,30]. Five studies concerned neonates (gestational age range 24–43 weeks) [31,32,33,34,35]. The age range within each study varied substantially (Table 1). The total age range covered in this review is 0–18 years. The population size ranges from 10 to 112 subjects in the individual studies.
In most studies, antibiotic therapy was indicated for a suspected or confirmed infectious disease, including pyelonephritis, pneumonia, sepsis, acute otitis media, urinary tract infection, or dermatological infections, with different degrees of illness. In one study, neonates received antibiotics prophylactically [32]. One study evaluated the pharmacokinetics of clavulanic acid in children admitted for a non-infectious reason [20]. In the majority of studies, subjects were admitted to the pediatric (n = 9) or neonatal ward (n = 4). One study was performed on the pediatric intensive care [24], in one study, patients received home-based treatment [25]. In the remaining three studies, the setting was unknown.
3.4 Antibiotic Regimen
Eight studies combined clavulanic acid with ticarcillin [18, 21, 22, 31,32,33,34,35]. Ten studies evaluated the pharmacokinetics of clavulanic acid in co-administration with amoxicillin [19, 20, 23,24,25,26,27,28,29,30]. Drugs were administered in varying ratios and dosing schedules. Ticarcillin/clavulanic acid was administered intravenously in all studies, including those performed in neonates. The clavulanic acid dose, co-administered with ticarcillin, ranged from 2.25 to 5 mg/kg. Seven studies evaluated the pharmacokinetics of oral amoxicillin/clavulanic acid (patients > 1 month of age). The clavulanic acid dose, co-administered orally with amoxicillin, ranged from 1.6 to 5 mg/kg. Two studies used fixed dosages based on age ranges instead of dose per kilogram bodyweight [28, 29]. The remaining three studies evaluated the pharmacokinetics of intravenous amoxicillin/clavulanic acid. None of those was performed in neonates. The clavulanic acid dose, co-administered intravenously with amoxicillin, ranged from 3.5 to 7 mg/kg. Detailed information on the dosage regimens is provided in Table 2 and in Table 2 of the ESM.
3.5 Sampling Methods
All studies collected blood; seven studies also collected urine samples. One study collected both blood and middle ear fluid. In most studies, sampling took place after the first dose. Three of these studies, however, were single-dose studies. Seven studies also sampled during steady state, usually between treatment days 3 and 7.
3.6 Sample Analysis
Fifteen out of 18 studies reported sample management; samples were centrifuged and cooled immediately after collection; and stored at – 70 to 80 °C for a maximum of 60 days before analysis. In three studies, a stabilizer (morpholinopropane sulfonic acid/sodium citrate) was added to the sample before storage [18, 20, 27]. Serum concentrations were often measured with the agar plate method. An overview of the sample management and methods of analysis is available provided in Table 3 of the ESM.
3.7 Methods for the Pharmacokinetic Analysis
The majority of included studies provide a descriptive analysis of the pharmacokinetic results and calculated basic non-compartmental parameters (AUC, volume of distribution [Vd], clearance, half-life [T1/2]). Five studies used pharmacokinetic-specific software (Adapt2, Nonmem, Lagran, Estrip/Kinonite) [21, 22, 24, 31, 34]. Pharmacokinetic parameters are presented in Tables 2 and 3. Four studies in which data were pooled from patients with a broad age range reported how maturation and/or bodyweight was accounted for in the scaling pharmacokinetic parameters [21, 22, 24, 34]. Other studies did report pharmacokinetic values per age group (i.e., neonates < 3 months of age and older children).
3.8 Pharmacokinetic Results
We extracted serum concentrations when provided. Figure 3a illustrates serum-time concentrations following oral administration of clavulanic acid. Figure 3b illustrates serum-time concentrations following intravenous administration (both after correction for dose [mg/kg]).

a Serum concentrations, corrected for dose, in time following oral clavulanic acid administration. b Serum concentrations, corrected for dose, in time following intravenous clavulanic acid administration. LBWI: low birth weight infants
Variation in pharmacokinetics was observed across studies; Table 3 presents the range of each parameter per included study, subdivided per mode of administration. Data for neonates specifically are presented separately. For all age groups, a large variability in maximum concentration (Cmax) is apparent, both following intravenous and oral administration. Maximum concentration following intravenous administration is substantially higher than Cmax following oral administration.
The mean T1/2 was provided in 13 studies, with a range from 0.78 to 2.9 h, with the longest T1/2 seen in preterm neonates. The T1/2 was comparable following intravenous and oral administration. The reported AUC differed significantly between the oral and intravenous group. The differences remained after correction for dose, differences remain present in AUC between oral and intravenous administration, with a higher AUC following intravenous administration, reflecting absorption characteristics. The Vd following intravenous administration is also significantly larger than that following oral administration.
3.9 Urine Excretion
Several papers reported urine excretion, of which four reported the percentage of administered dose recovered within a given sampling time interval. Clavulanic acid recovery after intravenous administration ranged from 50 to 59% 6 h after administration. The percentage of clavulanic acid recovered after oral administration is significantly lower within similar time intervals (range 8–32%).
3.10 Other Compartments
Jehl et al. [30] reported clavulanic acid penetration in middle ear fluid in children with otitis media; concentrations are reported in Table 2. Both serum and middle ear fluid concentrations were measured. Maximum concentration in middle ear fluid was reached later in time than Cmax in serum, reflecting a deep compartment pattern. Concentrations remain measurable 12 h after administration.
3.11 Adverse Events/Side Effects/Adverse Reactions
Most studies briefly mentioned treatment tolerance and the occurrence of adverse reactions or side effects, if any. The concepts adverse events, adverse reactions, and side effects were used interchangeably without a clear definition for each concept. All reported side effects and adverse events are presented in Table 4 of the ESM. Overall, very few adverse events have been reported. The most commonly reported adverse events are diarrhea and mild eosinophilia. Hoberman et al. reported that the incidence of diarrhea is dose dependent with higher rates in the 6.4-mg/kg/day clavulanic acid group compared with the 3.2-mg/kg/day and 2.85 mg/kg/day groups (26% vs 25% vs 17%; p = 0.10) [25].
4 Discussion
Clavulanic acid is a commonly used β-lactamase inhibitor, both in primary care and hospital settings for all age groups and for different types of infection. To our knowledge, this is the first review providing a complete literature overview of the reported pharmacokinetics of clavulanic acid in children from 0 to 18 years of age.
In general, the reported studies are quite old; only a few have been published after 2000. By that time, clavulanic acid was already widely used and found efficacious for a number of indications. Another possible reason for the paucity of recent studies could be that changes in legislation for drug research and sampling in children have complicating the execution of such studies. This does implicate, however, that the used techniques, such as the agar plate method, may have become obsolete, as the standard has shifted to direct quantification, preferably with techniques such as high-performance liquid chromatography or mass spectrometry. Moreover, pharmacokinetic values are mostly presented in a descriptive manner with individual pharmacokinetic estimates or naïve pooling, whereas population pharmacokinetics is currently encouraged. It could therefore be interesting to validate findings using high-performance liquid chromatography and explore whether reported raw data could be used for pharmacokinetic modeling.
Sampling and storage, when reported, were performed in an adequate manner, samples were immediately processed and stored at − 80 °C. A recent study from our group found clavulanic acid stability to be very poor when samples are not immediately stored. Samples should be stored at − 80 °C within 1 h after withdrawal. Samples can be stored for at least 6 months at − 80 °C, although frosting/defrosting severely affects the stability (unpublished data). The storage time did vary significantly between studies, which might have impacted results. Regarding drug storage, unfortunately none of the studies provided information about the storage conditions. Adequate storage conditions of the drug itself have proven relevant as well as the stability decreases substantially with increasing temperatures [36]. In our opinion, these aspects explain only part of the observed between-study variability, but should be considered when performing new pharmacokinetic studies.
The pharmacokinetics of clavulanic acid has been studied following oral (combined with amoxicillin) and intravenous (combined with amoxicillin or ticarcillin) administration. Studies have been performed in different populations, including special populations such as neonates and intensive care unit patients, thereby allowing insights into the possibly altered pharmacokinetics in immature or sick children. We have harmonized data by correcting concentrations for dose. However, the sampling schedule differed between studies; some studies reported single-dose concentrations, while others report steady-state concentrations. Moreover, pharmacokinetic findings were expressed in different measurement units, which we could not always transform as information was lacking. All this makes generalizability and pooling of results challenging, which should be kept in mind when interpreting results. We discuss the main findings in the next sections.
4.1 Absorption
Peak concentrations following oral administration were on average reached between 1 and 2 h after administration, which is comparable to findings in adults. A slower absorption could be expected in neonates, owing to immaturity of the gastrointestinal tract and a slower rate of gastric emptying. Unfortunately, none of the studies evaluating oral clavulanic acid included subjects younger than 1 month of age. A slightly slower absorption was seen in children 6–10 years of age with suspected or proven bacterial infection compared with younger or healthy children. However, as none of the oral studies included children with sepsis (biochemical results and clinical condition were reported to be normal), information on the effect of disease state on absorption was lacking.
As expected, the Cmax (corrected for dose) largely varied between studies, both following oral and intravenous administration in all populations. In general, higher peak concentrations were seen following intravenous administration. Fricke et al. [31] reported a lower Cmax (corrected for dose) in preterm and low birthweight infants compared with that in term infants. Contradictory, two studies reported a higher Cmax in infants < 3 months of age or weighing < 2 kg. In both studies, the Cmax was determined after the first dose, thus not influenced by elevated through concentrations due to altered clearance [33, 35]. Absorption following oral administration in healthy volunteers is also highly variable [37]. None of the studies provided both intravenous and oral data; determination of the bioavailability was therefore not possible. The bioavailability of clavulanic acid in adults is reported to be 60–70% [38].
4.2 Distribution
The Vd varied between studies. We could not compare the Vd between the two routes of administration as data on the Vd following oral administration were unfortunately lacking. One of the included studies evaluated the penetration in another compartment of interest: the middle ear reporting penetration with a lower concentration reached later in time compared with serum (reported AUC middle ear fluid 63% of that of serum. The authors concluded that these levels were sufficiently high for the inhibition of β-lactamase produced by Haemophilus influenzae and Moraxella catarrhalis. The mean half-life of clavulanic acid was longer than that in neonates compared with children and even longer in preterm and low birthweight neonates compared with term neonates. This is reflected in the adjusted dose frequency schedule in these patients; every 12 hours instead of every 8 hours. The T1/2 in older children was approximately that of adults.
4.3 Elimination
Clearance differed substantially between studies. This reflects the variability in patients (preterm-term-children) and thus maturational aspects (ontogeny), as well as differences in disease severity that do influence individual clearance. These aspects have not been addressed in the individual studies. Urine excretion 6 hours after dose administration ranged from 50 to 59% for intravenous administration and was even lower following oral administration, reflecting absorption. Given that detectable serum concentrations are measured 6–8 h after administration, one would expect the proportion of excretion in urine to be greater when increasing the sample interval.
4.4 Pharmacokinetic-Pharmacodynamic Target
As stated earlier, a clear target for clavulanic acid is currently lacking and dosing is targeted to the partner drug exposure. It could be that the target depends on the fraction of time that the free concentration exceeds the threshold concentration (%fT > CT), which has been described for tazobactam [39, 40] or the fAUC for relebactam [41]. To properly treat the infection, the actual exposure in children and adults should be comparable in order. As the actual pharmacodynamic target is not known, the only comparison that can be made with regard to the exposure of clavulanic acid in children is to compare it with that in adult humans. To that end, the AUCs (not corrected for body weight) are compared with the values described in adults. De Velde et al. described mean AUC values of 4.82 ± 1.53 [37]. These values are slightly higher than reported AUCs for children (range of reported means 1.66–5.66; Table 3).
4.5 Safety
Safety was not the primary objective of this review, and adverse events or reactions were co-collected as reported in the included papers. Consequently, we do not report a full and complete synthesis of adverse reactions/side effects related to clavulanic acid use. Moreover, it is known that when the occurrence of adverse events or side effects is not one of the primary objectives of a study, which was the case in most of the studies included in this review, these are poorly reported [42]. The reported events in the included studies are in line with the known side effects, of which gastrointestinal symptoms are the most common events [43].
Some limitations of this review need to be addressed. The first concerns the inclusion criteria. Our aim was to describe the available evidence on clavulanic acid; as we assumed that the number of relevant studies would be low, we did not apply strict eligible criteria. Consequently, the between-study variability in population, dosing regimen, and used methods was high, which made data harmonization difficult. A meta-analysis could, therefore, not been performed. Second, the used quality assessment tool, the ClinPK tool, has its limitations, as it does not cover all components of quality, including the risk of bias. However, a quality assessment tool available solely for pharmacokinetic studies is currently not available. The Grading and Assessment of Pharmacokinetic-Pharmacodynamic Studies (GAPPS) can only be used for pharmacokinetic-pharmacodynamic studies and was not appropriate for this review [44].
5 Conclusions and Relevance for Clinical Practice
Clavulanic acid is commonly used in the pediatric population and several studies have reported its pharmacokinetics. Similar to the adult population, the pharmacokinetics is highly variable in children of all age groups. This suggests that dose adjustments in relation to age or disease state could be beneficial to optimize treatment and prevent side effects and antimicrobial resistance. Moreover, it raises questions on the diversity of available suspensions and the ratio (penicillin/β-lactamase inhibitor) to be used. The pediatric population is hereby unique as developmental aspects impact pharmacokinetics. Additional pharmacokinetic research, including bioavailability studies, is therefore needed and should ideally be model based, addressing both maturational and disease-specific changes that characterize the pediatric population. Next, a clear pharmacodynamic target is currently lacking. Future research should therefore focus on gaining more insight into the pharmacodynamics of clavulanic acid, so that insights can lead to pharmacokinetic-pharmacodynamic modeling of clavulanic acid and targeted exposure in pediatrics.
References
Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, et al. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the sustainable development goals. Lancet. 2016;388(10063):3027–35. https://doi.org/10.1016/s0140-6736(16)31593-8.
Jackson C, Hsia Y, Bielicki JA, Ellis S, Stephens P, Wong ICK, et al. Estimating global trends in total and childhood antibiotic consumption, 2011–2015. BMJ Glob Health. 2019;4(1): e001241.
Schuller SS, Kramer BW, Villamor E, Spittler A, Berger A, Levy O. Immunomodulation to prevent or treat neonatal sepsis: past, present, and future. Front Pediatr. 2018;6:199.
Medernach RL, Logan LK. The growing threat of antibiotic resistance in children. Infect Dis Clin N Am. 2018;32(1):1–17.
Fleming A. On the antibacterial action of cultures of a penicillium, with special reference to their use in the isolation of B. influenzae. Br J Exp Pathol. 1929;10:226–36.
Brown ED, Wright GD. Antibacterial drug discovery in the resistance era. Nature. 2016;529(7586):336–43.
Slee AM, Wuonola MA, McRipley RJ, Zajac I, Zawada MJ, Bartholomew PT, et al. Oxazolidinones, a new class of synthetic antibacterial agents: in vitro and in vivo activities of DuP 105 and DuP 721. Antimicrob Agents Chemother. 1987;31(11):1791–7.
Leach KL, Brickner SJ, Noe MC, Miller PF. Linezolid, the first oxazolidinone antibacterial agent. Ann N Y Acad Sci. 2011;1222:49–54.
Butler MS, Paterson DL. Antibiotics in the clinical pipeline in October 2019. J Antibiot (Tokyo). 2020;73(6):329–64.
Abraham EP, Chain E. An enzyme from bacteria able to destroy penicillin. 1940. Rev Infect Dis. 1988;10(4):677–8.
Drawz SM, Bonomo RA. Three decades of beta-lactamase inhibitors. Clin Microbiol Rev. 2010;23(1):160–201.
Reading C, Cole M. Clavulanic acid: a beta-lactamase-inhiting beta-lactam from Streptomyces clavuligerus. Antimicrob Agents Chemother. 1977;11(5):852–7.
Huttner A, Bielicki J, Clements MN, Frimodt-Møller N, Muller AE, Paccaud JP, et al. Oral amoxicillin and amoxicillin-clavulanic acid: properties, indications and usage. Clin Microbiol Infect. 2020;26(7):871–9. https://doi.org/10.1016/j.cmi.2019.11.028.
Bolton GC, Allen GD, Davies BE, Filer CW, Jeffery DJ. The disposition of clavulanic acid in man. Xenobiotica. 1986;16(9):853–63. https://doi.org/10.3109/00498258609038967.
PRISMA. PRISMA transparent reporting of systematic reviews and meta-analyses. 2015. http://www.prisma-statement.org/. Accessed 7 Feb 2019
Kanji S, Hayes M, Ling A, Shamseer L, Chant C, Edwards DJ, et al. Reporting guidelines for clinical pharmacokinetic studies: the ClinPK statement. Clin Pharmacokinet. 2015;54(7):783–95.
Rohatgi A. WebPlotDigitizer web based tool to extract data from plots, images and maps. https://automeris.io/WebPlotDigitizer/. Accessed 8 Feb 2022
Reed MD, Yamashita TS, Blumer JL. Pharmacokinetic-based ticarcillin/clavulanic acid dose recommendations for infants and children. J Clin Pharmacol. 1995;35(7):658–65. https://doi.org/10.1002/j.1552-4604.1995.tb04105.x.
Bégué PQ, Nocquet F, Gaillard C, Safran C. Pharmacokinetics of augmentin in children. In: Proceedings of the European symposium on Augmentin; Scheveningen, 1982: p. 319–23
Schaad UB, Casey PA, Ravenscroft AT. Pharmacokinetics of a syrup formulation of amoxycillin-potassium clavulanate in children. J Antimicrob Chemother. 1986;17(3):341–5.
Feldman S, Bartlett AV, Jaffe N, Pickering LK. Clinical and pharmacokinetic evaluation of ticarcillin disodium plus clavulanate potassium in adolescent patients with malignancies. Am J Med. 1985;79(5 B):177–83. https://doi.org/10.1016/0002-9343(85)90156-1.
Jacobs RF, Trang JM, Kearns GL. Ticarcillin/clavulanic acid pharmacokinetics in children and young adults with cystic fibrosis. J Pediatr. 1985;106(6):1001–7. https://doi.org/10.1016/s0022-3476(85)80258-4.
Jones AE, Barnes ND, Tasker TCG, Horton R. Pharmacokinetics of intravenous amoxycillin and potassium clavulanate in seriously ill children. J Antimicrob Chemother. 1990;25(2):269–74.
De Cock PAJG, Standing JF, Barker CIS, De Jaeger A, Dhont E, Carlier M, et al. Augmented renal clearance implies a need for increased amoxicillin-clavulanic acid dosing in critically ill children. Antimicrob Agents Chemother. 2015;59(11):7027–35. https://doi.org/10.1128/aac.01368-15.
Hoberman A, Paradise JL, Rockette HE, Jeong JH, Kearney DH, Bhatnagar S, et al. Reduced-concentration clavulanate for young children with acute otitis media. Antimicrob Agents Chemother. 2017;61(7):e00238-e317. https://doi.org/10.1128/aac.00238-17.
Nelson JD, Kusmiesz H, Shelton S. Pharmacokinetics of potassium clavulanate in combination with amoxicillin in pediatric patients. Antimicrob Agents Chemother. 1982;21(4):681–2. https://doi.org/10.1128/aac.21.4.681.
Schaad UB, Casey PA, Cooper DL. Single-dose pharmacokinetics of intravenous clavulanic acid with amoxicillin in pediatric patients. Antimicrob Agents Chemother. 1983;23(2):252–5. https://doi.org/10.1128/aac.23.2.252.
Al Roomi LG, Sutton AM, Cockburn F, McAllister TA. Amoxycillin and clavulanic acid in the treatment of urinary infection. Arch Dis Child. 1984;59(3):256–9.
van Niekerk CH, van den Ende J, Hundt HK, Louw EA. Pharmacokinetic study of a paediatric formulation of amoxycillin and clavulanic acid in children. Eur J Clin Pharmacol. 1985;29(2):235–9.
Jehl F, Bobin S, Schatz P, Balouka JB, Rohmer D, Wagner B, et al. Middle ear fluid penetration of Augmentin® pediatric formulation (100 mg-12.5 mg/ml) at a dosage of 80 mg-10 mg kg−1 day−1, 3 times a day. Med Mal Infect. 2003;33(3):155–60. https://doi.org/10.1016/s0399-077x(03)00019-2.
Fricke G, Doerck M, Hafner D, Horton R, Kresken M. The pharmacokinetics of ticarcillin/clavulanate acid in neonates. J Antimicrob Chemother. 1989;24(Suppl. C):111–20.
Fayed SB, Sutton AM, Turner TL, McAllister TA. The prophylactic use of ticarcillin/clavulanate in the neonate. J Antimicrob Chemother. 1987;19(1):113–8.
Miall-Allen VM, Whitelaw AGL, Darrell JH. Ticarcillin plus clavulanic acid (Timentin®) compared with standard antibiotic regimes in the treatment of early and late neonatal infections. Br J Clin Pract. 1988;42(7):273–9.
Burstein AH, Wyble LE, Gal P, Diaz PR, Ransom JL, Carlos RQ, et al. Ticarcillin-clavulanic acid pharmacokinetics in preterm neonates with presumed sepsis. Antimicrob Agents Chemother. 1994;38(9):2024–8. https://doi.org/10.1128/aac.38.9.2024.
Begue P, Quiniou F, Quinet B. Efficacy and pharmacokinetics of Timentin in paediatric infections. J Antimicrob Chemother. 1986;17(Suppl. C):81–91.
Mack I, Sharland M, Brussee JM, Rehm S, Rentsch K, Bielicki J. Insufficient stability of clavulanic acid in widely used child-appropriate formulations. Antibiotics (Basel). 2021;10(2):225. https://doi.org/10.3390/antibiotics10020225.
De Velde F, De Winter BCM, Koch BCP, Van Gelder T, Mouton JW, Consortium CN. Highly variable absorption of clavulanic acid during the day: a population pharmacokinetic analysis. J Antimicrob Chemother. 2018;73(2):469–76.
Nilsson-Ehle I, Fellner H, Hedström SA, Nilsson-Ehle P, Sjövall J. Pharmacokinetics of clavulanic acid, given in combination with amoxycillin, in volunteers. J Antimicrob Chemother. 1985;16(4):491–8. https://doi.org/10.1093/jac/16.4.491.
VanScoy B, Mendes RE, Nicasio AM, Castanheira M, Bulik CC, Okusanya OO, et al. Pharmacokinetics-pharmacodynamics of tazobactam in combination with ceftolozane in an in vitro infection model. Antimicrob Agents Chemother. 2013;57(6):2809–14. https://doi.org/10.1128/aac.02513-12.
VanScoy BD, Tenero D, Turner S, Livermore DM, McCauley J, Conde H, et al. Pharmacokinetics-pharmacodynamics of tazobactam in combination with cefepime in an in vitro infection model. Antimicrob Agents Chemother. 2017;61(12):e01052-e1117. https://doi.org/10.1128/aac.01052-17.
Mavridou E, Melchers RJ, van Mil AC, Mangin E, Motyl MR, Mouton JW. Pharmacodynamics of imipenem in combination with β-lactamase inhibitor MK7655 in a murine thigh model. Antimicrob Agents Chemother. 2015;59(2):790–5. https://doi.org/10.1128/aac.03706-14.
Gillies M, Ranakusuma A, Hoffmann T, Thorning S, McGuire T, Glasziou P, et al. Common harms from amoxicillin: a systematic review and meta-analysis of randomized placebo-controlled trials for any indication. CMAJ. 2015;187(1):E21-31. https://doi.org/10.1503/cmaj.140848.
Salvo F, Polimeni G, Moretti U, Conforti A, Leone R, Leoni O, et al. Adverse drug reactions related to amoxicillin alone and in association with clavulanic acid: data from spontaneous reporting in Italy. J Antimicrob Chemother. 2007;60(1):121–6. https://doi.org/10.1093/jac/dkm111.
Gastine S, Rashed AN, Hsia Y, Jackson C, Barker CIS, Mathur S, et al. GAPPS (Grading and Assessment of Pharmacokinetic-Pharmacodynamic Studies) a critical appraisal system for antimicrobial PKPD studies: development and application in pediatric antibiotic studies. Expert Rev Clin Pharmacol. 2019;12(12):1091–8. https://doi.org/10.1080/17512433.2019.1695600.
Acknowledgements
We thank Wichor Bramer and Sabrina Meertens-Gunput, biomedical information specialists of the Erasmus University Medical Center, for their help with the literature search. We thank Ko Hagoort for his critical review of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported by The Netherlands Organization for Health Research and Development (ZonMw; Grant Number 848015005), the Innovatiefonds Zorgverzekeraars, and the Sophia Foundation for Scientific Research.
Conflicts of Interest/Competing Interests
The authors have no conflicts of interest that are directly relevant to the content of this article.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Material
Not applicable.
Code Availability
Not applicable.
Authors’ Contributions
FK and KA provided the concept for this systematic review. FK, KA, and GTS performed the literature search and data analysis. FK drafted the original manuscript. GTS, BK, IR, AM, RK, and KA critically reviewed and edited the manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Keij, F.M., Tramper-Stranders, G.A., Koch, B.C.P. et al. Pharmacokinetics of Clavulanic Acid in the Pediatric Population: A Systematic Literature Review. Clin Pharmacokinet 61, 637–653 (2022). https://doi.org/10.1007/s40262-022-01116-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-022-01116-3