
Abstract
Background
Although the costs of treating inflammatory bowel disease (IBD) in developed countries are well established, they remain largely unknown in countries with recent histories of socio-economic transition including Serbia.
Objective
To estimate the costs of treatment including the resources used by patients with IBD in Serbia from a societal perspective. This includes both Crohn’s disease and ulcerative colitis.
Methods
This cost-of-illness study was conducted to identify direct, indirect and out-of-pocket costs of treating patients with IBD in Serbia. Patients with IBD (n = 112) completed a semi-structured questionnaire with data concerning their utilisation of heath-care resources and illness-related expenditures. All costs were calculated in Republic of Serbia dinars (RSD) at a 1-year level (2014) and subsequently converted to Euros. Median values and ranges were reported to avoid potential distortions associated with mean costs.
Results
Median total direct costs and total indirect costs per patient per year in patients with Crohn’s disease were 192,614.32RSD (€1602.97) and 28,014.00RSD (€233.13) and 142,267.15RSD (€1183.97) and 21,436.00RSD (€178.39), respectively, in patients with ulcerative colitis. In both groups, the greatest component of direct costs was hospitalisation.
Conclusions
Costs of IBD in Serbia are lower than in more developed countries for two reasons. These include the fact that expensive biological therapy is currently under-utilised in Serbia and prices of health services are largely controlled by the State at a low level. The under-utilisation of biologicals may change with the advent of biosimilars at increasingly lower prices.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Cost-of-illness studies can provide useful information in patients with chronic diseases in countries with a recent history of socio-economic transition including Serbia, which are still economically challenged. |
We performed a cost-of-illness study to identify key direct, indirect and out-of-pocket costs of treatment of patients with IBD and its complications to help with future decision making in Serbia. |
Total direct costs are lower in this study compared with a number of other studies due to the limited prescribing of biological therapies among patients with IBD in Serbia. |
Immunomodulatory therapy is an efficient therapeutic strategy for IBD, but the prescribing of these medicines is limited among Central and Eastern Europe, including Serbia, due their current high costs, prescribing restrictions and often high co-payment levels. |
This will change with increasing availability of lower cost biosimilars starting with infliximab. |
1 Introduction
Inflammatory bowel disease (IBD) is a clinical entity that includes Crohn’s disease and ulcerative colitis. These are chronic conditions with different clinical courses, which affect the gastrointestinal system as well as other organs including the skin, joints and eyes [1–3]. Currently the aetiology of IBD remains unknown [2]. The clinical course of Crohn’s disease and ulcerative colitis varies from an asymptomatic phase to a very severe condition with potentially fatal outcomes [1, 3]. The prevalence of these chronic conditions has risen in Europe in recent years as well as in other continents [4], and both diseases are associated with high morbidity, reduced quality of life and potentially considerable costs [5–8]; consequently their management should be of interest to all key stakeholder groups, including health authorities, physicians, patients and patient associations.
The onset of Crohn’s disease and ulcerative colitis occurs in the majority of cases during the most economically productive phase of a person’s life. Following this, relapses and remissions occur through the remainder of a patient’s life until they die.
Managing patients with inflammatory bowel disease over the long term is associated with high costs, especially when relapsing. This is because treatment at this stage of the disease often includes hospitalisation, invasive diagnostic procedures, surgery and expensive biological medicines including the anti-tumour necrosis factor (TNF) alphas [9–12]. The chronic nature of IBD, and the frequent inadequacy of patients’ responses to therapy if not adequately managed, leads to increasing incidences of relapse, which further increases the resource burden [10, 13]. Immunomodulatory therapy is an efficient therapeutic strategy for IBD. However, due to its high costs and high patient co-payments, its utilisation is often limited in Central and Eastern European as well as less developed countries. This is similar to the situation seen in the management of patients with rheumatoid arthritis [2, 14, 15]. This may change with the advent of the first biosimilars for infliximab at considerably lower prices compared with the parent compound [10, 16].
The economic impact of IBD has been recognised as considerable in recent pharmacoeconomic literature [7, 8, 17]. However, the real costs of treatment of Crohn’s disease and ulcerative colitis within the Western Balkan countries, with recent histories of socio-economic transitions, remains ‘blurred’. This is because comprehensive patient registries are still lacking, and many patients remain untreated within state-owned health-care systems. Identifying all relevant costs of IBD, and the factors which may influence these costs, would provide comprehensive baseline data for future pharmacoeconomic analyses and health policy decisions among Balkan countries. Such studies would help inform relevant stakeholders about the most cost-effective treatment strategies for patients with IBD within the Balkan countries with their limited resources and growing health-care needs.
The aim of this study was to estimate the costs of treatment and utilisation of resources among patients with IBD (Crohn’s disease and ulcerative colitis) in Serbia principally from a societal perspective. In addition, we compared the costs of Crohn’s disease and costs of ulcerative colitis in Serbia with other countries.
2 Material and Methods
This study was designed as a cost-of-illness study conducted to identify direct, indirect and out-of-pocket costs of treatment of patients with IBD and its complications.
2.1 Settings, Perspective and Questionnaire Design
A questionnaire design study was chosen because there was no comprehensive patient level database including both hospital and ambulatory care, or register of IBD patients in Serbia, at the time the study was conducted. This is still the situation today, neither in written nor in electronic form. In addition, recent studies have shown a good correlation between self-reported health-care utilisation among patients with IBD and their medical records [18]. Consequently, we approached IBD patients via their association for help with ascertaining key resource items using a questionnaire methodology.
To help construct a robust questionnaire, we organised several meetings with the President and Vice President of the Patient Association. The objectives were to ascertain key topics of the survey and to agree to the content and methodology. The final questionnaire was approved by the Association and developed as a Word file. With the permission of the main Board of the Serbian Association of Patients with Crohn’s disease and Ulcerative Colitis, the word file was subsequently uploaded onto the main Internet page of the Association (see Electronic Supplementary Material). The patients could subsequently download the file, complete the questionnaire in their own time and on their own computers, and send the completed questionnaire back to the Association by e-mail. The responses were then entered manually onto an Excel file, where descriptive statistics could be made.
The questionnaire was constructed in such a way as to only collect data about health-care utilisation as well as indirect and other costs including data of what patients had actually spent for key items. There was no intention to collect qualitative information such as knowledge about the disease or attitudes to IBD, which would require additional activities including potential scales and testing their reliability and validity.
Since the association is active, and they communicate with their members mainly via their official web site, we thought patients would have enough skills and interest to participate via an online questionnaire. The main board of the Association also said they would discuss the questionnaire at their regular meetings to enhance the response rate. This would include the main topics of survey and how the questionnaire should be completed and returned. In this way, the need to go to the public to seek IBD patients willing to take part was negated, which we believed would be both costly and very time consuming. Consequently in agreement with the Association, we placed the questionnaire onto the main page of the Association.
Sampling was opportunistic, with the study population comprising patients who suffer from IBD and who are members of the Serbian Association of Patients with Crohn’s disease and ulcerative colitis (n = 510).
Patients were offered the opportunity to complete the questionnaire for 2 months during 2014 [19]. During this period, 59 patients with Crohn’s disease (43 % male/57 % female) and 53 patients with ulcerative colitis (46 % male/54 % female) took part and completed the semi-structured online questionnaire (see Electronic Supplementary Material). There was no further selection process, with no patient rejected from the subsequent analysis.
Patients subsequently entered their data anonymously into the questionnaire. In this way, their identities were protected.
We did not seek ethical approval. This is because our survey did not include any interventions with patients, only collecting and analysing data derived from IBD patients’ responses who voluntarily entered their data. For this type of study in Serbia, we do not need ethics committee approval. However, as mentioned, we obtained approval from the Scientific Board of the Serbian Association of Patients with Crohn’s disease and Ulcerative Colitis prior to commencing this study and patients gave their informed consent through actively completing the questionnaire. This was entirely voluntary with no pressure placed on patients to be part of the survey. In addition, no patient received a financial reward for taking part.
As also mentioned, the data from patients was collected and incorporated onto an Excel spreadsheet. The figures were subsequently broken down into median values as well as ranges. Median values were chosen for events and costs as mean values could be distorted by outliers at either end of the range. No statistical analyses were undertaken as we just wanted to record the actual costs incurred by IBD patients with either Crohn’s disease or ulcerative colitis in Serbia.
This study was performed from a societal perspective.
2.2 Demographic and Clinical Data
Demographic data included general information such as patient’s age, sex, occupation, average monthly income and lifestyle. Clinical data included information about the disease type (Crohn’s disease or ulcerative colitis), total length of disease, stage of the disease and data about any complications of the disease (surgery, colostomy and others).
2.3 Costs
The questionnaire was structured in such a way as to enable differentiation between direct, indirect and out-of-pocket costs. Intangible costs could not be measured with this questionnaire. Inpatient services were ascertained by questions concerning the number of hospitalisations in the last year, the ward type (intensive care or general type), total length of hospitalisation in the last year and total length of hospitalisation in the last 10 years. The questions about outpatient services included: the number and type of visits to physicians in the last year (visits to general practice and/ or specialists), the number of routine blood tests in the last year, number of other blood tests (biochemistry) in the last year, the number of radiological and endoscopic examinations in the last 5 years, the number of performed biopsies in the last five years and the number of rehabilitation programs in the last 5 years including the average length of any rehabilitation per program. Data about home visits, home care, transport of the patients and disability-related financial support received from Republic Fund for Health Insurance (RFHI) were also included.
Indirect and out-of-pocket costs were obtained through questions about lost wages for patients and their caregivers, job losses of either the patient or caregiver due to IBD, the costs for additional medical care, the costs of transport to-and-from health care facilities and adjustments in the home due to IBD. There were also questions about costs due to physical rehabilitation, alternative and complementary therapies, as well as over-the-counter medicines.
For the purpose of our study we used the official Tariff book [20] of the Republic Fund for Health Insurance and the prices from Official Gazette of Republic Serbia [21] to estimate costs of medical services (Table 1). All costs were collected as RSD. The consolidated costs were subsequently converted to Euros using the National Bank of Serbia rate at April 2015.
3 Results
Demographic and clinical characteristics of the patients with Crohn’s disease and the patients with ulcerative colitis are shown in Table 2.
Fifty-three patients with ulcerative colitis and 59 patients with Crohn’s disease took part (Table 1). The median age was 36 (range 20–59) years for patients with ulcerative colitis and 33 (range 13–55) years for patients with Crohn’s disease. The median duration of disease was 7 (range 1–20) years for patients with ulcerative colitis and 8 (range 1–38) years for those with Crohn’s disease. None of the patients with either ulcerative colitis or Crohn’s disease received biological therapy (Table 2). The patients with Crohn’s disease were maintained on azathioprine 2.5 mg/kg/day (100 % of patients), and the patients with ulcerative colitis were also on azathioprine at 2 mg/kg/day (100 % of patients).
Table 3 contains data on indirect and out-of-pocket expenses of patients with either ulcerative colitis or Crohn’s disease. These are typically recorded as median costs and ranges. ’Other costs’ are shown without a range since only three patients replied to this question, and they all entered the same amount.
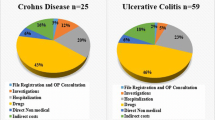
Table 4 contains data on the direct costs of surveyed patients with IBD in Serbia. Figure 1 contains details of the consolidated median costs for patients with either Crohn’s disease or ulcerative colitis.

Total median annual costs (direct and indirect) per patient with ulcerative colitis and Crohn’s disease in RSD
This showed that in Serbia, total median direct costs per patient per year in those with Crohn’s disease were 167,973.9RSD (range 39,559.9–2,040,319.8RSD) [€1397.9 (range €329.23–€16,980.02)] and total indirect costs per patient per year were 28,014.00RSD (range 3000.00–81,000.00RSD) [€233.1 (range €24.9–€674.1)] (Fig. 1). Total direct costs per patient per year in those with ulcerative colitis were 122,526.0RSD (range 49,037.9–761,916.3RSD) [€1019.6 (range €408.1–€6340.8)] and total indirect costs per patient per year were 21,436RSD (range 3500–68,000RSD) [€178.3 (range €29.1–€565.9)].
4 Discussion
We believe the costs of treating patients with ulcerative colitis and Crohn’s disease in a West Balkan country (with recent history of socio-economic transition) have not been previously reported in the literature. Our study contributes to the limited background knowledge to assist key stakeholders in the Balkans in their future decision making, which is a demanding task within limited health-care budgets and a rising incidence of IBD. Economic analyses of chronic diseases are crucial to help provide clear insight into the extent of direct and indirect costs and their impact on national health-care budgets. This is especially the case for IBD in view of the potential impact on indirect costs due to disability and decreased work productivity. However, we are aware different authorities throughout Europe use different cost components in their reimbursement and funding decision making [23].
These costs (see Fig. 1) are lower than those seen in some other countries. For example, the direct costs of treating ulcerative colitis in Germany and the UK were estimated as GB£3021 (€3871.0) per patient per year, whilst treating Crohn’s disease cost was GB£3416 (€4377.1) per patient per year; with half of the costs due to hospitalisation and surgery [24]. The results from a study conducted in patients from across Europe and Israel showed that the mean total costs per patient per year were higher in patients with Crohn’s disease at €2548 compared with an estimated total cost of €1524 for patients with ulcerative colitis, which was similar to our findings. The highest total costs per patient-year were recorded in Denmark at €3705, and the lowest in Norway at €888 [24]. Kappelman et al. [25] showed that the mean annual costs per patient are considerably higher in the USA than in Europe. This is because total annual direct costs were US$8265 (€7429.9) per patient with Crohn’s disease and US$5066 (€4554.1) per patient with ulcerative colitis.
Due to the chronic and progressive clinical course of IBD, we had expected a greater impact of indirect costs due to disability and decreased work productivity since the onset of IBD is mostly during the economically productive phase of an adult’s life. As a result, there should be appreciable indirect costs due to lost wages, work disability and early retirement in view of its relapsing and remitting nature. However, this was not found to be the case in our study.
Surgical treatment of IBD is a therapeutic option for those patients with severe Crohn’s disease and in those patients with ulcerative colitis where the response to medical treatment is inadequate [24]. In our study, the percent of patients undergoing surgical interventions were 8 % in those with ulcerative colitis and 46 % in those with Crohn’s disease, while 31 % of operated patients in both groups had a colostomy. These findings are similar to those from other European countries where patients with Crohn’s disease who experienced surgery and colostomy were 37 % among East European countries, 38 % in Norway, 50 % in Sweden, 61 % in Denmark and 52 % in Hungary. In patients with ulcerative colitis, surgery and colostomy rates were 8.7 % in East European countries, 9.8 % in Norway, 24 % in Denmark and 2.8 % in Hungary [24]. The risk of surgery and colostomy is lower today compared to the rates reported in studies prior to 1990 [24, 25]. This is due to a restrictive policy toward surgical procedures and the introduction of potent medical treatments such as the biological drugs [24].
Admission to hospital and the duration of treatment are mostly determined by local health-care policies and it is difficult to compare these parameters across European countries. For example, in some studies the average duration of hospitalisation for IBD patients was estimated at 10 days [24, 26]. Similar findings were obtained from the study of Bassi et al. [2] where patients with ulcerative colitis and Crohn’s disease lost 17 and 20 days from work during 6 months, respectively. The results of our study (Table 2) indicate that the duration of hospitalisation was longer, with a median of 31 days in those with ulcerative colitis and 34 days in those with Crohn’s disease.
Loss of function and the ability to fully engage in work and other activities is a serious consequence of IBD. This will negatively affect both patients’ income and their quality of life [24]. Unemployment and underemployment among patients with IBD has been the subject of many studies in Europe, Canada and United States [24, 27–29]. The reduction in working ability in patients with IBD reported in these studies ranged from 3 to 13 %, mostly in patients with ulcerative colitis (about 60 % of all patients with reduced working ability) [17, 24, 28, 29]. In our study, 31 % of patients with ulcerative colitis lost his/her job due to illness, with a median duration of unemployment of 3 years. Twenty-five percent of patients with Crohn’s disease lost his/her job due to illness, with a median duration of unemployment of 4 years. A reduction of working ability negatively correlates with the quality of life of these patients, and produces appreciable economic losses due to lost wages, decreased productivity and early retirement [24]. However, in our study (Table 3) only 2 % of patients with Crohn’s disease received disability pensions. This may be one of the key factors for lower than envisaged indirect costs in our study. This compares with a Norwegian population where 19 % of patients with IBD 10 years after diagnosis received a disability pension [28]. We accept that the ability of countries to provide income assistance programmes for IBD and other patients varies among European countries. This primarily depends on the economic welfare and health-care polices of these countries. We also accept that wages are appreciably lower in Serbia than among Western countries, which will also affect the level of indirect costs.
Since IBD also affects the ability of patients to undertake everyday activities, patients may need assistance, which is provided by caregivers. In the recent literature, it has been estimated that caregivers spend on average 30 hours per week with patients with inflammatory bowel disease [28]. In our study (Table 3), the median number of hours that a caregiver spent with both groups of patients was 56 per week. The median duration of unemployment of patients was 4 years in those with ulcerative colitis and 6 years in those with Crohn’s disease. However, we recognise that this was a selected population with increased likelihood of having more severe disease than the average of all patients with IBD in Serbia. However, this did not always translate into indirect costs as seen by lower than expected figures (Fig. 1).
The out-of-pocket expenses include costs due to housekeeping or modifications to the home due to illness, special nutritional products and complementary and alternative medicines [28]. These costs per patient-year in our study were estimated at 28,014 RSD (€233.13) in those with ulcerative colitis and 21,436RSD (€178.39) in those with Crohn’s disease. In the UK, these costs were lower in patients with IBD at approximately £80 (€102.5) per patient and £132 (€169.1) per patient for ulcerative colitis and Crohn’s disease, respectively [2].
Overall our study indicates that patients with ulcerative colitis and Crohn’s disease from a Western Balkan country are comparable with those in other European countries in many socio-economic regards. However, biological therapy is currently under-utilised in Serbia in comparison to Western European countries as seen by the fact that none of the patients in this study were on biological therapies. Other studies have also shown the low use of biological therapies in immunological diseases among Central and Eastern European countries compared to Western European counties, enhanced by restrictions, high co-payments and a lack of reimbursement [10, 15]. Whilst this decreases direct medical costs due to lower drug acquisition costs, this can increase hospitalisation costs as well as indirect costs due to work absenteeism.
The next stage of our research will be to estimate the cost-effectiveness of biological medicines on total costs, building on our comprehensive catalogue of actual resource consumption. The case for the biological medicines and their cost-effectiveness has been demonstrated in a number of countries and studies [11, 12]. The case of improving patient care in a cost-efficient manner should be strengthened by the availability of biosimilars. For example, infliximab is now available at approximately 30 % of the price of the originator in Norway [16], with a recent study demonstrating the potential for considerable savings with the biosimilar infliximab in patients with Crohn’s disease among a number of Central and Eastern European countries [8]. There have been concerns about the effectiveness and safety of biosimilar infliximab. However, ongoing studies in patients in Central, Eastern and Western European countries as well as South Korea are showing that biosimilar infliximab is effective and well tolerated [8, 16, 30]. This provides hope for the future.
We accept that a major limitation of this study is the selection of patients for costing purposes. We undertook this approach, with its inherent selection bias due to the need for online access and computer literacy, as the most efficient way of contacting patients with IBD. We also acknowledge a low response rate (22 %). This low rate was not expected since the Association is active and in regular contact with its members via electronic and other means. We must acknowledge this low sample size, which limits the representativeness and generalisability of the study findings. We also accept that our survey involved the reporting of all medical examinations and other key events over a 5-year period, which could generate recall bias. However, as stated earlier, recent studies have shown a good correlation between self-reported health-care utilisation among patients with IBD and their medical records [18]. Despite these limitations, we believe our findings are a good start to addressing the lack of information regarding current resource utilisation among patients with IBD in countries such as Serbia.
We have also sought to address some of the concerns with studies such as cost-of-illness studies and budget impact analysis [31] by using patient-level data, local costings and avoiding conflicts of interest. We acknowledge though that we did not check the accuracy of respondent answers. However, we would not expect these to be falsified as it is in the interest of these patients to accurately record the resources they consume as far as they are able to.
In conclusion, we believe we have documented the total costs of treating patients with IBD in a Balkan country, adding to the literature for Western European countries. This is particularly important for countries similar to Serbia with their recent socio-economic history. We also believe that this study provides important insight for all key stakeholder groups in the future to help shape future policy decisions. We will be building on the findings.
References
Loftus EV. Clinical epidemiology of inflammatory bowel disease: incidence, prevalence, and environmental influences. Gastroenterology. 2004;126(6):1504–17.
Bassi A, Dodd S, Williamson P, Bodger K. Cost of illness of inflammatory bowel disease in the UK: a single centre retrospective study. Gut. 2004;53(10):1471–8.
Bodger K. Cost of illness of Crohn’s disease. Pharmacoeconomics. 2002;20:639–52.
Williams JG, Roberts SE, Ali MF, Cheung WY, Cohen DR, Demery G, Edwards A, Greer M, Hellier MD, Hutchings HA, Ip B, Longo MF, Russell IT, Snooks HA, Williams JC. Gastroenterology services in the UK. The burden of disease, and the organization and delivery of services for gastrointestinal and liver disorders: a review of the evidence. Gut. 2007;56:1–113.
Longobardi T, Jacobs P, Bernstein CN. Work losses related to inflammatory bowel disease in the United States: results from the National Health Interview Survey. Am J Gastroenterol. 2003;98:1064–72.
Cohen RD. The quality of life in patients with Crohn’s disease. Aliment Pharmacol Ther. 2002;16:1603–9.
Ganz ML, Sugarman R, Wang R, Hansen BB, Hakan-Bloch J. The economic and health-related impact of Crohn’s disease in the United States: evidence from a nationally representative survey. Inflamm Bowel Dis. 2016;22(5):1032–41.
Burisch J, Vardi H, Pedersen N, Brinar M, Cukovic-Cavka S, Kaimakliotis I, et al. Costs and resource utilization for diagnosis and treatment during the initial year in a European inflammatory bowel disease inception cohort: an ECCO-EpiCom Study. Inflamm Bowel Dis. 2015;21(1):121–31.
Buchanan J, Wordsworth S, Ahmad T, Perrin A, Vermeire S, Sans M, Taylor J, Jewell D. Managing the long term care of inflammatory bowel disease patients: the cost to European health care providers. J Crohns Colitis. 2011;5(4):301–16.
Brodszky V, Rencz F, Pentek M, Baji P, Lakatos PL, Gulacsi L. A budget impact model for biosimilar infliximab in Crohn’s disease in Bulgaria, the Czech Republic, Hungary, Poland, Romania, and Slovakia. Expert Rev Pharmacoecon Outcomes Res. 2016;16(1):119–25.
Strik AS, Bots SJ, D’Haens G, Lowenberg M. Optimization of anti-TNF therapy in patients with inflammatory bowel disease. Expert Rev Clin Pharmacol. 2016;9(3):429–39.
Huoponen S, Blom M. A systematic review of the cost-effectiveness of biologics for the treatment of inflammatory bowel diseases. PLoS One. 2015;10(12):e0145087.
Feagan BG. Review article: economic issues in Crohn’s disease—assessing the effects of new treatments on health-related quality of life. Aliment Pharmacol Ther. 1999;13(s4):29–37.
Kostić M, Jovanović S, Tomović M, Milenković MP, Janković SM. Cost-effectiveness analysis of tocilizumab in combination with methotrexate for rheumatoid arthritis: a Markov model based on data from Serbia, country in socioeconomic transition. Vojnosanit Pregl. 2014;71(2):144–8.
Putrik P, Ramiro S, Kvien TK, Sokka T, Pavlova M, Uhlig T, et al. Inequities in access to biologic and synthetic DMARDs across 46 European countries. Ann Rheum Dis. 2014;73(1):198–206.
Matusewicz W, Godman B, Pedersen HB, Furst J, Gulbinovic J, Mack A, et al. Improving the managed introduction of new medicines: sharing experiences to aid authorities across Europe. Expert Rev Pharmacoecon Outcomes Res. 2015;15(5):755–8.
Stark R, König HH, Leidl R. Costs of inflammatory bowel disease in Germany. Pharmacoeconomics. 2006;24(8):797–814.
Severs M, Petersen RE, Siersema PD, Mangen MJ, Oldenburg B. Self-reported health care utilization of patients with inflammatory bowel disease correlates perfectly with medical records. Inflamm Bowel Dis. 2016;22(3):688–93.
Questionnaire. Available at: http://www.ukuks.org/anketa/poruka.php. Accessed 18 Nov 2014.
Anonymous. Tariff Book of Health Care Services in Health Facilities of Republic of Serbia. Belgrade: Republic Institute for Health Insurance; 2014.
The Prices of Medication in Serbia, from december/2014; Official Gazette of Republic of Serbia 133/2014.
Pension and Disability Insurance Fund, Republic of Serbia; Available at: http://www.pio.rs/lat/novcane-naknade.html.
Paris V, Belloni A. Value in pharmaceutical pricing. Available at URL: http://www.oecd-ilibrary.org/docserver/download/5k43jc9v6knx.pdf?expires=1454876546&id=id&accname=guest&checksum=87065DEF51331D5A659CC1917CCFCEC7.
Burisch J, Jess T, Martinato M, Lakatos PL, ECCO—EpiCom. The burden of inflammatory bowel disease in Europe. J Crohns Colitis 2013;7(4):322–37.
Kappelman MD, Rifas-Shiman SL, Porter CQ, Ollendorf DA, Sandler RS, Galanko JA, Finkelstein JA. Direct health care costs of Crohn’s disease and ulcerative colitis in US children and adults. Gastroenterology. 2008;135(6):1907–13.
Monstad I, Hovde O, Solberg IC, Moum BA. Clinical course and prognosis in ulcerative colitis: results from population-based and observational studies. Ann Gastroenterol. 2014;27(2):95–104.
Hovde Ø, Huppertz-Hauss G, Høivik ML, Moum B. Clinical course, treatment strategies, social and economic impact of ulcerative colitis: an overview. Austin J Gastroenterol. 2014;1(4):1017.
Høivik ML, Moum B, Solberg IC, Henriksen M, Cvancarova M, Bernklev T, IBSEN Group. Work disability in inflammatory bowel disease patients 10 years after disease onset: results from the IBSEN Study. Gut. 2013;62:368–375.
Rocchi A, Benchimol EI, Bernstein CN, Bitton A, Feagan B, Panaccione R, Glasgow KW, Fernandes A, Ghosh S. Inflammatory bowel disease: a Canadian burden of illness review. Can J Gastroenterol. 2012;26(11):811–7.
Mack A. Norway, biosimilars in different funding systems. What works? Generics Biosimilars Initiat J (GaBI J). 2015;4(2):90–2.
Faleiros DR, Alvares J, Almeida AM, de Araujo VE, Andrade EI, Godman BB, et al. Budget impact analysis of medicines: updated systematic review and implications. Expert Rev Pharmacoecon Outcomes Res. 2016;16(2):257–66.
Author contributions
Marina Kostić contributed to the study design, collection of data, statistical analysis and writing of the manuscript. Ljiljan Djakovic contributed to the study design, collection of data and statistical analysis. Raša Šujić contributed to the study design, preparing the online questionnaire, collection of data and statistical analysis. Brian Godman contributed to the study design and the writing of the manuscript. Slobodan M. Janković contributed to the study design, collection of the data, preparing the online questionnaire, statistical analysis and the writing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was partially funded by Grant No. 175007 given by the Serbian Ministry of Education. The authors Brian Godman, Marina Kostić, Ljiljan Djakovic, Slobodan M Janković and Raša Šujić have no conflict sof interest in regard to this article, although two of the authors (LD and RS) are members of the Association of Patients with Crohn’s Disease and Ulcerative Colitis.
Approval from the Scientific Board of the Serbian Association of Patients with Crohn’s disease and Ulcerative Colitis was obtained prior to commencing this study. The study was performed in accordance with the ethical standards of the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study by the very nature of data collection.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kostić, M., Djakovic, L., Šujić, R. et al. Inflammatory Bowel Diseases (Crohn´s Disease and Ulcerative Colitis): Cost of Treatment in Serbia and the Implications. Appl Health Econ Health Policy 15, 85–93 (2017). https://doi.org/10.1007/s40258-016-0272-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-016-0272-z