
Abstract
Background
Inflammatory bowel disease (IBD) is a chronic inflammatory condition involving individuals across all age groups. Recent data suggests the increase in the prevalence of IBD and the surge in applying the biologic drugs in which both change the cost of IBD in recent years. Comprehensive assessment of direct and indirect cost profiles associated with IBD in our area is scarce. This study aimed to determine the economic burden of IBD in Iran from a societal perspective, using cost diaries.
Methods
Patients available on clinic registry and hospital information system (HIS), who were diagnosed with IBD, were invited to take part in this study. Demographic and clinical data, the healthcare resource utilization or cost items, absenteeism for the patients and their caregivers were obtained. The cost of the used resources were derived from national tariffs. The data regarding premature mortality in IBD patients was extracted from HIS. Productivity loss was estimated based on the human capital method. Then, cost date were calculated as mean annual costs per patient.
Results
The cost diaries were obtained from 240 subjects (Ulcerative colitis: n = 168, Crohn’s disease, n = 72). The mean annual costs per patient were 1077 US$ (95% CI 900–1253), and 1608 (95% CI 1256, 1960) for the patients with ulcerative colitis and Crohn’s disease, respectively. Of the total costs, 58% and 63% were in terms of the indirect costs for the patients with ulcerative colitis and Crohn’s disease, respectively. The cost of illness for country was found to be 22,331,079 US$ and 15,183,678 US$ for patients with ulcerative colitis and Crohn’s disease, respectively. Highest nationwide economic burden of IBD was found for patients older than 40 years were estimated to be 8,198,519 US$ and 7,120,891 US$, for ulcerative colitis and Crohn’s disease, respectively.
Conclusion
The medication was found to be the greatest contributor of direct medical costs. Productivity loss in terms of long-term disability and premature mortality were major components of IBD’s economic burden in Iran.
Similar content being viewed by others

Introduction
Ulcerative colitis (UC) and Crohn’s disease (CD) are included in the spectrum of disorder defined as inflammatory bowel disease (IBD), the relapsing–remitting and chronic inflammatory condition in which the gastrointestinal tract is affected [1]. IBD has lower prevalence compared to other common gastrointestinal-related disorders, such as irritable bowel syndrome, gastroesophageal reflux, and colorectal cancer; however, it is one of the gastrointestinal-related disorders with the most economic burden [1]. Data from many countries, including India [2], China [3], Scotland [4], and Turkey [5] showed an unprecedented growth of IBD worldwide. Concurrently, the incidence of the disease is increasing in Asia [6] and Iran [7]. Low mortality of the disease, the diagnosis at early ages, and its chronic nature have driven this increase in the disease's prevalence. Using biological medications in the treatment of IBD changed the need for hospitalization and surgeries and also changed the cost of the disease in recent years. So, these highlight the importance of the economic burden evaluation of the disease [8, 9]. As stated before, in Iran, the IBD incidence is rising while information on its cost is scarce. Two studies have evaluated direct medical cost and hospitalization cost of the disease [10, 11]. Nevertheless, health policy makers should have reliable information regarding the cost of illness to quantify the impact of the disease on a society. This can inform healthcare cost projection, as well as resource allocation [12]. Regarding the mentioned points, it is necessary to assess the cost of IBD, including direct medical costs, direct non-medical costs, and indirect costs to determine the economic burden of IBD in Iran. In our study, we aim to evaluate the cost of IBD in a multicenter setting.
Methods
Participants and data collection
This cost of illness analysis was conducted on the patients diagnosed with IBD in 2021. For data collection, we used the phone records available in Shiraz’ hospital information systems (HIS) and IBD clinic at Faghihi hospital, which is referral IBD clinic affiliated to the Shiraz University of Medical Sciences. Using the convenient sampling method, patients were invited to take part the study through phone calls. Then, the data was obtained through a face-to-face interview while the patients were referred to the clinic. This clinic and referral hospitals all provide the care to the IBD patients, mostly from Fars province and sometimes from neighboring provinces. Our study as a partial economic evaluation technique, aimed to calculate the total costs of IBD in Iran from the society perspective. The IBD diagnosis was confirmed based on clinical, endoscopic, and histological criteria, as described elsewhere [13]. Demographic data (including sex, age, marital status, educational level, educational level, income, and hours of paid work), clinical data (including disease duration, disease progression, and extra-intestinal involvement) were obtained from all participants, and they were interviewed to fill out the cost diary. The disease progression was defined by calculating Mayo score and Crohn’s disease activity index (CDAI) in patients with UC, and CD, respectively. To obtain an estimated prevalence of IBD in Fars province, the population ratio of Fars province in Iran was multiplied by an estimated prevalence of IBD in Iran in 2021 [14, 15], which found to be 1800. The sample volume was determined to be 233 patients for estimation of costs of illness based on 95% CI, margin error of 6%, and the estimated prevalence of IBD in Fars province (http://www.raosoft.com/samplesize.html).
Cost diary
Cost diary is an instrumental method which is developed by Goosens et al. and is used to estimate the cost of a condition. Since no significant difference has been found among the patients’ report and medical records, there is no need to check medical reports when the cost diary is used [16].
In order to prevent recall bias, the number of physician visits, physiotherapy, purchased drugs dosage, and all other related disease ‘s costs during 3-month prior to the interview were asked from patients, which were scaled up by a factor of four to extrapolate to the mean number of each item during 1-year. Only for hospitalization and surgeries, the duration of 1- year was considered in cost diary. To minimize missing information and partial responses, telephone contacts were made after the initial visit, whenever it was needed. We had a protocol for phone calls. We made phone calls, in case of none- response we considered maximum number of three phone calls in different hours of day and variable days of week to make telephone contacts. Diary records were used to estimate resource used. The cost of the used resources were derived from national tariffs. The costs were recorded in Rial and then we converted to US dollars based on the moving average of the exchange rate in the 2021 252,000:1 (Rial:US) (Additional file 1: Table S1) .
Death registration database
We extracted death data of patients with IBD, who were died because of IBD-related causes, from HIS during 2013–2021 to estimate economic burden of premature mortality for UCCD.
Direct medical costs
Direct medical costs included physician visits, physiotherapy sessions, nutrition sessions, purchased medication, surgeries, and para-clinical tests. The cost of each item expected on medication was estimated by the mean number of each item, multiplied by the contemporary tariff of the Ministry of Health and Medical Education (MoHME). The contemporary tariff is defined for each unit of healthcare service item by the MoHME annually in two forms of private and public services. In our study, we used the weighted average of these two forms based on the last national utilization survey [17]. The cost of purchased medication was calculated by the number of each item, multiplied by the unit cost of each item defined by Food and Drug Administration (http://irc.fda.gov.ir/nfi#).
Direct nonmedical costs
Transportation, self-help group, hours of paid household help, and goods-related to the condition (including alternative medicine, assistive devices, special diet, and books) were considered the components of direct nonmedical costs. Transportation cost was obtained from the sum of public and personal transportation. Public transportation cost was calculated based on the mean number of public transportation service use multiplied by the tariff of transportation defined by Municipal. Personal transportation and other items were calculated based on the real reported costs by patients in the cost diary.
Indirect costs
The human capital approach was used to estimate indirect costs. Productivity losses because of disability and premature mortality were considered components of indirect costs in our study. We divided disability into short- and long-term disability.
Productivity losses due to short-term disability
Productivity losses in terms of short-term disability were obtained from temporary absenteeism from work for patients with the disease, and the caregivers. To calculate productivity loss because of temperament absenteeism of patients from work for therapy appointments, the hourly wage of lowest-paid unskilled government workers (LPUGW) of the Ministry of Labor was multiplied by the number of absence hours for each patient. For calculation of the productivity loss because of absenteeism of the caregiver the number of hospitalization days for the patients who were hospitalized during 1-year was added to 14 days per hospitalization. Then, the calculated number was multiplied by the LPUGW. It was assumed that work productivity loss was experienced by caregivers during hospitalization days to fulfill the responsibility of caregiving.
Productivity losses due to long-term disability
Early retirement of patients, permanent absenteeism from work because of disability, and unpaid household work for caregivers of disabled patients were considered estimating productivity losses due to long-term disability. To estimate the cost of early retirement, the amount of lost pension, compared to the full pension, was calculated for any patient who had early retired. To calculate the cost of permanent absenteeism from work, the annual wage of LPUGW was considered for patients who completely could not work, and were not paid a defined benefit pension. To estimate unpaid household work for caregivers of disabled patients, the number of patients who could not take care of themselves were multiplied by the annual wage of LPUGW because of unpaid permanent caregiver responsibility.
Premature mortality
Standard expected years of life lost (SEYLL) was used to predict the productivity loss due to premature mortality. We used the following formula to estimate SEYLL [18]:
where N identifies the number of deaths at a certain age, and Lx refers to the remaining life-expectancy at the age of death. Based on many arguments and the last update of global health estimates by WHO, we decided not to take into account time discounting and age-weighting [19,20,21,22]. We obtained mean number of annual deaths by age, gender, and type of disease. The gender-specific remaining life-expectancy at the age of death was calculated based on the 2020 Iran lifetable from World Health Organization [23], and subsequently SEYLL for each disease was calculated by the sum of the two obtained gender-specific SEYLL for the type of disease. Then, the calculated SEYLL was multiplied by gross domestic production (GDP) per capita for Iran, which is defined by World Bank [24], to estimate the total economic burden of premature mortality for each disease. To obtain the mean cost per patient, the total cost of premature mortality was divided by the estimated prevalence of the disease in Fars Province.
Statistical analysis
All statistical analyses were performed using SPSS 26.0. Mean, and the standard deviation was used to present continuous variables, while categorical variables were shown as frequency and percentage. Costs were reported as mean costs with 95% CI estimated using non-parametric boodstrap sampling.
Results
Demographic characteristics
Among 286 patients who were initially invited, 240 patients accepted to take part. The mean ± Standard deviation (SD) age of participants was 41 ± 13 and 39 ± 14 for UC and CD, respectively. Majority of patients were married, and reside in the cities. The gender was approximately equal between males and females in the both diseases, and UC was predominant disease among participants. Descriptive results based on gender, marital status, employment status, disease type, and other variables are summarized in Table 1.
Direct medical costs
Cost items are categorized in Table 2. Number [%] of participants using resources, and mean annual cost for each category are shown in the table for UC and CD, separately.
Drugs, which were taken by patients, are classified into six categories (Table 3). Number [%] of participants taking each medication’s type, and mean annual cost for each type are shown in the table based on the disease type.
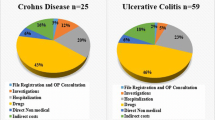
Medication had the greatest share of direct medical costs in both types of IBD, accounting for 31.6% and 23.0% of the total costs in the patients with UC and CD, respectively (445.52$ per patient in UC, and 586.96$ per patient in CD). Among types of medication, aminosalicylates contributed to the most prescription proportion in both diseases (66.2% in UC and 63.9% in CD). It shared the highest cost of medication types in patients with UC, accounting for 244.63$ per patient. Less than twenty percent of patients consumed biological agent; however, this type of medication accounted for the highest and the second highest medication costs in patients with CD (235.11$), and UC (100.72$), respectively (Table 3). Hospitalization was another important contributor of direct medical costs, especially in the patients with CD, responsible for 10% of the total costs (161.29$) per patient. Physiotherapy and nutrition consult almost did not impose cost to the studied IBD patients (Table 2).
Direct nonmedical costs
Although the proportion of using nonmedical resources were high by participants, the related costs accounted for less than 1% of the total costs in both diseases (8.92$ per patient in UC, and 4.67$ per patient in CD). They were mostly driven by transportation (Table 2).
Indirect costs
Indirect costs were major contributors of the total costs, responsible for more than a half of the costs (622.46$ per patient in UC, and 1016.62$ per patient in CD). Productivity losses induced by short-term disability were more frequent among participants, as compared with the losses due to long-term disability, and were almost equally formed by two components of temporary absenteeism for patients and caregivers. Despite the lower frequency of productivity losses due to long-term disability (13.7% in UC patients, and 19.4% CD patients), they imposed a large share of the total costs (266.50$ per patient in UC, and 436.40$ per patient in CD). Permanent absenteeism from work was predominant compartment of productivity losses induced by long-term disability in both disease types (174.60$ per patient in UC, and 261.91$ per patient in CD). Productivity loss because of premature death was another important contributor of the total costs, accounting for almost a quarter of the costs in both diseases (276.47$ per patient in UC, and 387.22$ per patient in CD) (Table 2).
Cost of illness for country
The characteristics of participants, including age, sex, disease type and age at diagnosis were almost equivalent to those described for the recent pilot feasibility study of first nation-wide IBD registry in Iran, which enabled us to extrapolate the mean annual total costs regarding disease type and age group for the country [17]. An estimated prevalence of IBD in Iran in 2021 was used for the calculation [15]. The cost of illness for country was found to be 22,331,079 and 15,183,678 for UC and CD, respectively (Table 4).
Discussion
In this retrospective cohort study, we aimed to determine the economic burden of IBD, and to compare the profiles of costs in UC and CD patients. There are barriers to study the economic burden of specific diseases in Iran, as diagnostic data is not ordinarily coded for outpatient visits, and the patients’ resource utilization are not recorded. Thus, there is the paucity of information on resource utilization consumed by patients with specific diseases. However, to the best of our knowledge this study is among the first comprehensive studies in Iran assessing both direct and indirect cost profiles associated with IBD.
Several studies have evaluated the economic burden of IBD in other countries [25,26,27,28,29,30,31,32,33,34,35,36,37]. Consistent with their findings, we found that the CD patients’ resource utilization was higher than that of UC patients, and this difference was more considerable in hospitalization, surgeries, and laboratory sectors. Variations in the pathogenesis of the two diseases can explain this difference, as UC might not lead to irreversible and systemic damage observed in CD patients [38]. However, the amount of difference among the annual mean costs of UC and CD differs from a study to another, based on the design and population of study, as inconsistencies are created in the results of cost of illness studies when comparing one to another due variations in method [30]. Annual mean costs per patient for UC and CD were between 6217–11,477 US$, and 11,034–18,932 US$ in the USA, respectively. The corresponding ranges were 8949–10,395 euros, and 2898–6742 euros in European countries [39, 40]. In our study, annual mean costs per patient for UC and CD were found to be 1077 US$ (95% CI 900–1253), and 1068 (95% CI 1256, 1960) respectively, which is in line with the results of studies in UK and Germany in terms of CD: UC costs ratio [25, 34]. These two studies have applied a similar method of using patient-reported resource utilization to estimate economic burden of the disease (bottom-up approach). The difference of total costs per patient between Iran and European countries could be explained by the fluctuations in Iran’s currency exchange rate to dollar in the last few years.
According to our findings, the medication use represents the major source of direct medical costs (76.4% and 63.0% of direct medical costs in UC and CD patients), while costs related to surgery and hospitalization have not a large share of direct cost. The results of more recent studies are consistent with our results [30,31,32,33]. The widespread application of biological agents in the treatment of IBD patients has changed the healthcare outlook, leading to a substantial shift in cost profiles [33]. The effect of this type of medication was significant on the reduction of colectomy in UC patients [41,42,43]. According to findings, despite the relatively low proportion of patients who received biological agents (8.3% and 26.4% of UC and CD patients); they shaped a significant contributor of the total costs in both diseases. This highlights the importance of better insurance coverage for such drugs to make them affordable. According to results, none of the participants used the nutritional consultation and assessment. Considering the importance of supportive nutritional therapy in the clinical care of IBD patients [44, 45], routine assessment and monitoring of nutritional status in IBD patients in Iran is highly encouraged.
Direct nonmedical costs were minor contributors to the total costs, as compared with direct medical and indirect costs. Based on our findings, none of participants had been a member of self-help groups. In these groups, patients share their own experiences, which can lead to applying executable strategies for management of chronic disease by other patients [46]. Therefore, it is pivotal to design self-help groups for IBD patients in Iran which fit for their need; subsequently, they should be encouraged to enroll in such groups.
Short- and long-term productivity losses because of disability were also evaluated. We found that productivity losses because of disability handled 33.0% and 39.1% of the total costs in UC and CD, respectively. According to a German study, long term productivity losses shared 32% and 49% of the total costs in UC and CD, respectively [34]. In a more recent study in the Netherlands, productivity losses due to IBD-related absenteeism were found to be 16% and 39% of the total costs, respectively [33]. It seems that biological agents have had an effective role in reducing productivity losses because of disability in CD patients. However, due to different methodologies in measurement of productivity losses due to disability, we have limitations for a more detailed comparison with the results of other studies. In our study, we considered absenteeism and unpaid household work for caregivers, which were important contributors to costs for CD patients, accounting for 6.5% and 9.0% of the total costs, respectively. We did not evaluate presenteeism in our study, since no validated questionnaire is available to evaluate presenteeism with a recall time of over 7 days [33].
The premature mortality was another major contributor of costs in both diseases, which is in line with findings of systematic analysis of the global burden of inflammatory bowel disease. It shows the fact that IBD-associated premature mortality forms a great share of disease burden in countries with low socio-demographic index (SDI) [47]. There is insufficient population-based data evaluating the causes of premature mortality in IBD patients in Iran. In a study assessing the trend of colectomy in the country, colorectal cancer was found to be the leading cause of death in IBD patients undergoing colectomy. In this regard, cancer screening protocols should be routinely performed in IBD patients [9]. Cancer and cardiovascular disease were found to be leading causes of mortality in IBD patients in the USA. Therefore, healthy lifestyle behaviors should be routinely assessed in IBD patients, and adherence to such lifestyle should be encouraged to reduce contributing risk for cancer and cardiovascular disease, and subsequently the risk of premature mortality and related costs in IBD patients [48].
Limitations
This study provided a more comprehensive view of the costs of illness for IBD in the Iran. However, this study was limited by the small sample size and prevalence approach for cost diaries. Furthermore some aspects of estimation might be affected by purchasing power of participants.
Conclusion
The medication was found to be the greatest contributor to direct medical costs. Productivity loss due to long-term disability and premature mortality were major components of inflammatory bowel disease burden in Iran.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Beard JA, Franco DL, Click BH. The burden of cost in inflammatory bowel disease: a medical economic perspective and the future of value-based care. Curr Gastroenterol Rep. 2020;22(2):1–7.
Desai H, Gupte P. Increasing incidence of Crohn’s disease in India: is it related to improved sanitation? Indian J Gastroenterol. 2005;24:23–4.
Zheng JJ, Zhu XS, Huangfu Z, Gao ZX, Guo ZR, Wang Z. Crohn’s disease in mainland China: a systematic analysis of 50 years of research. Chin J Dig Dis. 2005;6(4):175–81.
Armitage E, Drummond HE, Wilson DC, Ghosh S. Increasing incidence of both juvenile-onset Crohn’s disease and ulcerative colitis in Scotland. Eur J Gastroenterol Hepatol. 2001;13(12):1439–47.
Can G, Poşul E, Yılmaz B, Can H, Korkmaz U, Ermiş F, et al. Epidemiologic features of ınflammatory bowel disease in Western Blacksea region of Turkey for the last 10 years: retrospective cohort study. Korean J Intern Med. 2019;34(3):519.
Hu P-J. Inflammatory bowel disease in Asia: the challenges and opportunities. Intest Res. 2015;13(3):188.
Malekzadeh MM, Vahedi H, Gohari K, Mehdipour P, Sepanlou SG, Ebrahimi Daryani N, et al. Emerging epidemic of inflammatory bowel disease in a middle income country: a nation-wide study from Iran. Arch Iran Med. 2016;19:2–15.
van Linschoten RCA, Visser E, Niehot CD, van Der Woude CJ, Hazelzet JA, van Noord D, et al. Systematic review: societal cost of illness of inflammatory bowel disease is increasing due to biologics and varies between continents. Aliment Pharmacol Ther. 2021;54(3):234–48.
Ghahramani S, Paparisabet M, Sayari M, Hosseini SV, Lankarani KB. Colectomy in ulcerative colitis: trends in southern iran in a decade. Arch Iran Med. 2021;24(9):665.
Balaii H, Olfatifar M, Narab SO, Hosseini AA, Salehi AS, Shahrokh S. Estimation the direct cost of inflammatory bowel disease in Iranian patients; the one-year follow-up. Gastroenterol Hepatol Bed Bench. 2019;12(Suppl1):S87.
Lankarani KB, Ghahramani S, Hadipour M, Pourhashemi M, Mahmoodi A, Zeraatpishe M, et al. Determinants of hospital costs of inflammatory bowel disease. Govaresh. 2019;24(4):230–7.
Greenberg D, Ibrahim MIBM, Boncz I. What are the challenges in conducting cost-of-illness studies? Value Health Reg Issues. 2014;4:115–6.
Lennard-Jones J. Classification of inflammatory bowel disease. Scand J Gastroenterol. 1989;24(sup170):2–6.
National Portal of Statistics: Statistical Center of Iran; 2021. https://www.amar.org.ir.
Olfatifar M, Zali MR, Pourhoseingholi MA, Balaii H, Ghavami SB, Ivanchuk M, et al. The emerging epidemic of inflammatory bowel disease in Asia and Iran by 2035: a modeling study. BMC Gastroenterol. 2021;21(1):1–8.
Goossens ME, Rutten-van Mölken MP, Vlaeyen JW, van der Linden SM. The cost diary: a method to measure direct and indirect costs in cost-effectiveness research. J Clin Epidemiol. 2000;53(7):688–95.
Malekzadeh MM, Sima A, Alatab S, Sadeghi A, Daryani NE, Adibi P, et al. Iranian Registry of Crohn’s and Colitis: study profile of first nation-wide inflammatory bowel disease registry in Middle East. Intest Res. 2019;17(3):330.
Plass D, Chau PYK, Thach TQ, Jahn HJ, Lai PC, Wong CM, et al. Quantifying the burden of disease due to premature mortality in Hong Kong using standard expected years of life lost. BMC Public Health. 2013;13(1):863.
Parsonage M, Neuburger H. Discounting and health benefits. Health Econ. 1992;1(1):71–6.
Brouwer WB, Niessen LW, Postma MJ, Rutten FF. Need for differential discounting of costs and health effects in cost effectiveness analyses. BMJ. 2005;331(7514):446–8.
McA AK. Understanding DALYs (disability-adjusted life years). J Health Econ. 1997;16: 703730.
Cheng L, Zhang L, Yue L, Ling J, Fan M, Yang D, et al. Expert consensus on dental caries management. Int J Oral Sci. 2022;14(1):1–8.
Shanafelt TD, Kaups KL, Nelson H, Satele DV, Sloan JA, Oreskovich MR, et al. An interactive individualized intervention to promote behavioral change to increase personal well-being in US surgeons. Ann Surg. 2014;259(1):82–8.
Ruíz-López del Prado G, Blaya-Nováková V, Saz-Parkinson Z, Álvarez-Montero ÓL, Ayala A, Muñoz-Moreno MF, et al. Design and validation of an oral health questionnaire for preoperative anaesthetic evaluation. Braz J Anesthesiol. 2017;67(1):6–14.
Bassi A, Dodd S, Williamson P, Bodger K. Cost of illness of inflammatory bowel disease in the UK: a single centre retrospective study. Gut. 2004;53(10):1471–8.
Hay JW, Hay AR. Inflammatory bowel disease: costs-of-illness. J Clin Gastroenterol. 1992;14(4):309–17.
Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology. 2012;143(5):1179-1187.e3.
Blomqvist P, Ekbom A. Inflammatory bowel diseases: health care and costs in Sweden in 1994. Scand J Gastroenterol. 1997;32(11):1134–9.
Hay AR, Hay JW. Inflammatory bowel disease: medical cost algorithms. J Clin Gastroenterol. 1992;14(4):318–27.
Pillai N, Dusheiko M, Maillard MH, Rogler G, Brüngger B, Bähler C, et al. The evolution of health care utilisation and costs for inflammatory bowel disease over ten years. J Crohns Colitis. 2019;13(6):744–54.
Park K, Ehrlich OG, Allen JI, Meadows P, Szigethy EM, Henrichsen K, et al. The cost of inflammatory bowel disease: an initiative from the Crohn’s & Colitis Foundation. Inflamm Bowel Dis. 2020;26(1):1–10.
van der Valk ME, Mangen M-JJ, Severs M, van der Have M, Dijkstra G, van Bodegraven AA, et al. Evolution of costs of inflammatory bowel disease over two years of follow-up. PLoS ONE. 2016;11(4): e0142481.
van der Valk ME, Mangen M-JJ, Leenders M, Dijkstra G, van Bodegraven AA, Fidder HH, et al. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFα therapy: results from the COIN study. Gut. 2014;63(1):72–9.
Stark R, König H-H, Leidl R. Costs of inflammatory bowel disease in Germany. Pharmacoeconomics. 2006;24(8):797–814.
Juan J, Estiarte R, Colome E, Artés M, Jiménez F, Alonso J. Burden of illness of Crohn’s disease in Spain. Dig Liver Dis. 2003;35(12):853–61.
Odes S, Vardi H, Riis L, Moum B, Politi P, Tsianos N, et al. Cost-analysis and cost-determinants in inflammatory bowel disease. Gastroenterology. 2005;128(4): A324-A.
Feagan BG, Vreeland MG, Larson LR, Bala MV. Annual cost of care for Crohn’s disease: A payor perspective. Am J Gastroenterol. 2000;95(8):1955–60.
Le Berre C, Ananthakrishnan AN, Danese S, Singh S, Peyrin-Biroulet L. Ulcerative colitis and Crohn’s disease have similar burden and goals for treatment. Clin Gastroenterol Hepatol. 2020;18(1):14–23.
Cohen R, Yu A, Wu E, Xie J, Mulani P, Chao J. Systematic review: the costs of ulcerative colitis in Western countries. Aliment Pharmacol Ther. 2010;31(7):693–707.
Peng YuA, Cabanilla LA, Qiong WuE, Mulani PM, Chao J. The costs of Crohn’s disease in the United States and other Western countries: a systematic review. Curr Med Res Opin. 2008;24(2):319–28.
Sandborn WJ, Rutgeerts P, Feagan BG, Reinisch W, Olson A, Johanns J, et al. Colectomy rate comparison after treatment of ulcerative colitis with placebo or infliximab. Gastroenterology. 2009;137(4):1250–60.
Clemente V, Aratari A, Papi C, Vernia P. Short term colectomy rate and mortality for severe ulcerative colitis in the last 40 years. Has something changed? Dig Liver Dis. 2016;48(4):371–5.
Barnes EL, Jiang Y, Kappelman MD, Long MD, Sandler RS, Kinlaw AC, et al. Decreasing colectomy rate for ulcerative colitis in the United States between 2007 and 2016: a time trend analysis. Inflamm Bowel Dis. 2020;26(8):1225–31.
Lucendo AJ, De Rezende LC. Importance of nutrition in inflammatory bowel disease. World J Gastroenterol: WJG. 2009;15(17):2081.
Balestrieri P, Ribolsi M, Guarino MPL, Emerenziani S, Altomare A, Cicala M. Nutritional aspects in inflammatory bowel diseases. Nutrients. 2020;12(2):372.
Huh J, Ackerman MS, editors. Collaborative help in chronic disease management: supporting individualized problems. In: Proceedings of the ACM 2012 Conference on Computer Supported Cooperative Work; 2012.
Alatab S, Sepanlou SG, Ikuta K, Vahedi H, Bisignano C, Safiri S, et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–30.
Lo C-H, Khalili H, Song M, Lochhead P, Burke KE, Richter JM, et al. Healthy lifestyle is associated with reduced mortality in patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2021;19(1):87-95.e4.
Acknowledgements
We are grateful to all patients who participated in this study.
Funding
This study was funded by Shiraz University of Medical Sciences (SUMS).
Author information
Authors and Affiliations
Contributions
Conceptualization, Visualization, and Methodology: KBL, LZ, SG. Supervision, and Project administration: KBL, SG. Investigation: MP, SG. Writing, reviewing, and editing: MP, LZ, SG. Data curation, and Software: MP. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained from all participants, their anonymity was guaranteed, and the study protocol was approved by approved by Ethical Committee of Shiraz University of Medical Sciences approved with Reg. No: IR.SUMS.REC.1400.637. The study protocol followed the ethical guidelines of the 2013 Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors confirm that there is no conflict of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Unit Costs of Medical Resources Consumed by Patients/*: For Nurition Consult, Imaging, Laboratory, and Surgery constant of k should be multipled by given data; k = 13600.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pakdin, M., Zarei, L., Bagheri Lankarani, K. et al. The cost of illness analysis of inflammatory bowel disease. BMC Gastroenterol 23, 21 (2023). https://doi.org/10.1186/s12876-023-02648-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-023-02648-z