
Abstract
Background
We investigated the safety, tolerability, and pharmacokinetics of intravenous recombinant human Neuregulin-1 (rhNRG-1), a DNA recombinant protein for the treatment of chronic heart failure, in healthy Chinese volunteers following single and multiple dose administration.
Methods and Results
To evaluate the safety and tolerance after single-dosing escalation, 28 subjects were divided into six groups (0.2, 0.4, 0.8, 1.2, 1.6, and 2.4 μg/kg) to receive an intravenous (IV) infusion of rhNRG-1 over 10 min by a randomized, open-label design. Only the 1.2 μg/kg dose group obtained pharmacokinetic parameters: Cmax was 7.645 (24.21) ng/mL, AUC0–t was 97.088 (21.41) min·ng/mL. To assess the safety and pharmacokinetics after multiple-dosing, 32 subjects were divided into four groups (0.2, 0.4, 0.8, and 1.2 μg/kg) to receive a 10-min IV infusion of rhNRG-1 for five consecutive days. After multiple dosing of 1.2 μg/kg, the Cmax value at day 5 was 8.838 (51.6) ng/mL and the AUC0–t value at day 5 was 109.890 (32.99) min·ng/mL. RhNRG-1 is rapidly cleared from the blood and has a short t1/2 of about 10 min. The adverse events related to rhNRG-1 mainly included flat or inverted T wave and gastrointestinal reactions, all of which were mild.
Conclusions
It is concluded that rhNRG-1 is safe and well tolerated in healthy Chinese subjects at the dosing levels used in this study. The severity and frequency of adverse events did not increase with the prolongation of administration time.
Clinical Trial Registration
Chinese Clinical Trial Registry (http://www.chictr.org.cn) Identifier No. ChiCTR2000041107.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The first study showing pharmacokinetics in humans of recombinant human Neuregulin-1 (rhNRG-1), a DNA recombinant protein for the treatment of chronic heart failure. |
RhNRG-1 is safe and well tolerated in healthy Chinese subjects at the dosing levels used in this study via IV dosing. |
To date, no therapeutic agent has been approved in the global treatment of chronic heart failure that acts directly through the ErbB2/ErbB4 receptor tyrosine kinase on cardiomyocytes. RhNRG-1 is expected to become the international first-in-class new drug in the field of heart failure treatment. |
1 Introduction
Heart failure (HF) is a clinical syndrome consisting of cardinal symptoms that may be accompanied by signs. Due to aging, the overall incidence is increasing [1]. Despite current therapies, HF remains the leading cause of hospital admission among older patients.
Neuregulin (NRG) -1, also known as Neu Differentiation Factor (NDF) or Glial Growth Factor (GGF), is the ligand of ErbB3 and ErbB4 and belongs to the epidermal growth factor (EGF) family in structure. It can directly bind to ErbB4 receptor on cardiomyocytes, activate the receptor, and produce corresponding biological activity [2, 3]. NRG-1 has been found to have multiple and unique mechanisms of action in modulating the expression of proteins and enzymes involved in promoting cardiac contractility and sarcomere structure reorganization [4,5,6,7]. Cardiomyocytes lacking neuregulin signals cannot fully balance β-adrenergic activation by inhibiting parasympathetic activity. When NRG signaling is suppressed, this mechanism may lead to an increased risk of heart failure in injured human hearts [8]. NRG-1 is able to improve cardiac function and regulate the remodeling of sympathetic and vagus nerves after myocardial infarction, thereby achieving a new balance of the autonomic nervous system and protecting the heart from injury [9, 10]. On the basis of the results of animal experiments, it is speculated that exogenous supplementation of NRG-1 analogs may contribute to the recovery of cardiac function in patients with heart failure [11,12,13,14]. At present, two kinds of recombinant human NRG have been developed to therapeutic agents: recombinant human neuregulin-1β2 protein (rhNRG-1) and Cimaglermin (NRG-1β3). Both drugs have been shown in clinical trials to increase the cardiac function of patients with heart failure [15, 16]. To date, no therapeutic agent has been approved in the field of chronic heart failure treatment worldwide that acts directly through the ErbB2/ErbB4 receptor tyrosine kinase in cardiomyocytes. This makes recombinant human NRG a promising new drug for the treatment of CHF.
Pharmacokinetic data on the Neuregulin-1-related products in healthy subjects or patients with chronic heart failure have not been reported yet. This study is the first to demonstrate the tolerability, safety, and pharmacokinetic of rhNRG-1 in healthy subjects.
2 Methods
2.1 Study Design
The study comprises three parts as follows (Fig. 1): Part 1—safety evaluations with a single-dosing escalation; Part 2—pharmacokinetic study with a single dosing; Part 3—safety and pharmacokinetic evaluations with multiple dosing. Each subject received only one dose, and no dose escalation was conducted on the same subject.

Study flowchart
Part 1 and Part 3 were performed using a randomized, open-label, dose-escalation design. Dose escalation was performed after the safety profile of the preceding dose was evaluated. The trial was designed to begin with the 0.2 μg/kg dose group and not proceed to the higher dose group until the lower doses’ safety and tolerance were confirmed. Part 2 was performed using a randomized and open-label design.
In Part 1, 28 subjects were randomized to six dose groups, that is, 0.2, 0.4, 0.8, 1.2, 1.6, and 2.4 μg/kg, with 4–6 people in each group, and the ratio of male to female was about 1:1. In the higher three dose groups, it was hoped that six subjects would be included as far as possible, but as long as four subjects were included, the requirements of the trial design were met (28 cases were described according to the final number of enrolled cases). In Part 2, three dose groups (0.4, 0.8, and 1.2 μg/kg) were planned to be given in a single dose; each group consisted of ten subjects, with a male-to-female ratio of about 1:1. It was planned to carry out the 1.2 μg/kg dose group first and then decide whether to carry out the pharmacokinetic study of the 0.4 and 0.8 μg/kg dose groups according to the results. Finally, only ten subjects in the 1.2 μg/kg single-dose group were administered the drug. In Part 3, 32 subjects were divided into four dose groups, which were 0.2, 0.4, 0.8, and 1.2 μg/kg, 8 in each group. The ratio of male to female was about 1:1. Each subject was administered once daily from day 1 to day 5, and the drug was given at about 8:00 a.m. every day. Among them, 0.2 and 0.4 μg/kg dose groups only carried out safety tests, and 0.8 and 1.2 μg/kg dose groups carried out pharmacokinetic tests at the same time.
Subjects in Part 2 and Part 3 fasted for at least 8 h before each administration, and the amount of drinking water was limited to 240 mL from midnight to 2 h before administration. They were admitted to the clinical study unit on day −1, discharged after breakfast (on day 27 for Part 1, day 2 for Part 2, and day 6 for Part 3) and returned to the research unit for follow-up (on day 10 for Part 1, day 7 for Part 2, and day 13 for Part 3) after administration.
2.2 Volunteers
Seventy healthy Chinese subjects were enrolled. Inclusion criteria: healthy nonsmoker subjects 19–45 years old with a body mass index (BMI) of 20.0–27.0 kg/m2 without signs of clinical abnormalities on clinical examinations and laboratory analyses. Exclusion criteria included the following: allergic constitution or history of allergy to any drug; female subjects currently pregnant or lactating; intake of other preventive or therapeutic drugs; history of heart, pulmonary, neurological, endocrine, metabolic, or psychiatric disease; intake of any drug in the past 2 weeks (including Chinese medicine); blood donation or participation in other clinical trials in the past 3 months; drug abuse or alcoholism; or being considered unsuitable for the study by an investigator. Subjects were admitted to the ward of the Phase I clinical trial laboratory of Peking University First Hospital the night before scheduled dosing and underwent a clinical evaluation. Twenty-four hours before check-in and throughout the study period, no food or beverages were allowed unless specified in this program, and no vigorous exercise, drinking or smoking, caffeinated beverages, or high-purine-containing food were allowed.
2.3 Drug Preparation and Administration
RhNRG-1 for injection was obtained from Zensun (Shanghai) Sci&Tech Co., Ltd. Each sterile lyophilized powder contains 250 μg of rhNRG-1. A solution containing 25 μg/mL of rhNRG-1 was prepared by taking 1 mL of sterile water for injection and dissolving the lyophilized powder, and then adding 1 mL of the dissolved solution to 9 mL of a solution containing 5% glucose. The required amount of drug was diluted in 20 mL of 5% glucose solution according to the weight of the subject. The rhNRG-1 solution was injected over 10 min at a constant speed (2.0 mL/min) through the mid-elbow vein using a microinfusion syringe pump.
2.4 Blood sampling
To characterize the pharmacokinetics in Part 2 and Part 3, venous blood samples (approximately 5 mL) were collected in test tubes containing EDTA and without polystyrene particles before dosing (0 h), at 5 and 10 min during dosing, and 15, 20, 30, 45, 60, 90, 120, 180, and 240 min post-dosing. Blood samples were centrifuged immediately at 3000 rpm at room temperature for 10 min and stored at −20 °C until measurement.
2.5 Measurement of rhNRG-1
On the basis of the binding property of rhNRG-1 to the corresponding cell surface receptors, we established an in vitro radioimmune cell receptor competitive binding method for the determination of rhNRG-1 content in human plasma. Human breast cancer cell line SKBR3 cells (American Type Culture Collection, Manassas, VA, USA, no mycoplasma and virus contamination) highly express ErbB2/ErbB3 receptors on the surface, to which rhNRG-1 can bind. Moreover, the ability of rhNRG-1 to bind the corresponding receptors was unchanged after isotope (125I, Na125I, specific activity 14.5–37 MBq/µL, New England Nuclear Corporation, Boston, MA) labeling. Under a certain reaction system, equal amounts of SKBR3 cells, equal amounts of 125I-rhNRG-1, and different concentrations of rhNRG-1 standards and plasma samples to be tested were added. After reacting for a certain time, the radioactivity bound to the cells was measured using the γ-ray Counting System of Radio-Immunoassay (SN-682, Shanghai Nuclear Institute Rihuan Instrument Factory, Shanghai, China). The curve of rhNRG-1 concentration versus radioactivity was plotted, and the rhNRG-1 concentration in the samples was calculated.
The linear range of the method was 0.29–37.13 ng/mL with a correlation coefficient r2 of 0.99668. The recoveries ranged from 89% to 109%. The intra- and interbatch precision was 6–12% and 7–13%, respectively. The lower limit of quantification (LLOQ) of the method was 290 pg/mL, and the background level of blank human plasma was below the LLOQ. The results of stability were as follows: the high-performance liquid chromatography (HPLC) purity (including retention time and peak shape) and biological activity of rhNRG-1 stock solution stored at room temperature (22 °C) or 37 °C for 1 week did not change significantly. 125I-rhNRG-1 stored in different buffers (PBS and plasma) for 15 days showed no significant change in its radiochemical purity, indicating that 125I-rhNRG-1 was relatively stable. The standard rhNRG-1 stock solution was added to blank human plasma and stored at room temperature (22 °C), 4 °C, and −20 °C for 1 week, respectively, and the relative standard deviations of the relative recoveries were less than 15%, indicating that rhNRG-1 is relatively stable in human plasma and the enzymatic degradation of rhNRG-1 by various enzymes in plasma can be excluded.
2.6 Pharmacokinetic and Statistical Analysis
Descriptive statistics were performed using SAS software (Version 8.2, SAS Institute Inc., Cary, NC, USA) for security assessment and demographic characteristics. The frequency tables were used to summarize the adverse events, and the number of cases of adverse events and the incidence of adverse events were calculated separately. Given the exploratory nature of the study, no formal statistical hypothesis testing was performed.
The pharmacokinetic parameters of rhNRG-1 were calculated by noncompartmental analysis using WinNonLin Version 6.1 (Certara, St. Louis, MO, USA). The measured maximal concentration (Cmax) and the time to reach maximal concentration (Tmax) were obtained from the observed values. The elimination rate constant (λZ) was calculated by log-linear regression of the terminal portion of the concentration–time curve. The half-life (t1/2) was calculated as t1/2 = ln(2)/λZ. The area under the curve from time zero to the time of the last quantifiable concentration (AUC0–t) was calculated by the trapezoidal rule, and the area under the curve from time zero to infinity (AUC0–∞) was calculated using the formula AUC0–∞ = AUC0–t + Clast/λZ, where Clast is the last measurable concentration. Apparent clearance (Cl) was calculated by dose/AUC0–∞, and the apparent volume of distribution (Vz) was calculated by Cl/λZ.
2.7 Safety Evaluation
During the study, the safety of rhNRG-1 was evaluated by clinical laboratory analyses, physical examinations, vital signs, electrocardiogram (ECG) measurements, ultrasonic cardiogram, and adverse event reports. Blood and urine samples were collected for hematology, blood biochemical examination, specific antibody detection, myocardial enzymes, activated partial thromboplastin time (APTT), prothrombin time (PT), and urine human chorionic gonadotropin (HCG) at the screening stage and periodically after dosing. Adverse events (AEs) were evaluated for their intensity, seriousness, and relationship with the investigational drug by investigators. AEs in different groups were coded and counted in accordance with the system organ classification (SOC) and preferred terminology (PT) from MedDRA. The AEs and drug-related AEs were also classified and summarized on the basis of the SOC and PT.
3 Results
3.1 Subjects
Seventy subjects were recruited into this study, of whom 69 were Han and one was Manchu, and none had a history of allergy, smoking, or alcoholism. Except for one female subject in the multiple-dosing 1.2 µg/kg group who withdrew from the study due to adverse events after 2 days of administration, the other 69 subjects completed the study.
Table 1 presents the demographic data of the subjects. Seventy subjects with evaluable data were included in the safety analysis. In Parts 2 and 3, ten and eight subjects, respectively, were included in the pharmacokinetics analysis.
3.2 Safety and Tolerability
Single dose and multiple doses of rhNRG-1 were well tolerated in these healthy volunteers at doses up to 2.4 μg/kg for single dose and 1.2 μg/kg for multiple doses. All adverse events were mild, and no serious adverse events or other significant adverse events occurred in the subjects. Compared with the baseline data, the results of physical examination of subjects in each dose group in each visiting period did not change significantly, and the specific antibody of all subjects was negative. All subjects had no precordial distress, chest distress, chest pain, or dyspnea; blood pressure had no change at 2 and 24 h after the treatment; clinical laboratory analyses, myocardial enzymes, and ultrasonic cardiogram had no obvious abnormality. All of them recovered without treatment.
The number of subjects with adverse events in the three parts was 16 (57%), 6 (60%), and 23 (72%), respectively, and the number of subjects with adverse events related to the study drug was 14 (50%), 4 (40%), and 20 (63%), respectively. The results are presented in Tables 2 and 3, respectively. Common adverse events related to the study drug were ECG changes and gastrointestinal disorders.
ECG alterations included ST depression, T-wave flattening, and T-wave inversion, with the number of cases in the three parts being 9 (29%), 3 (30%), and 19 (44%), respectively. In the single-dose administration, three cases in the 0.2 μg/kg and 1.2 μg/kg dose groups of Part 1 had T-wave changes occurring at 2 h or 4 h after dosing, with durations of 2 h, 3 h, and 23 h, respectively. In the 1.6 μg/kg and 2.4 μg/kg dose groups, there were five cases with T-wave changes lasting for 5 or 6 days, including one case with T-wave changes occurring 2 h after dosing and the remaining four cases with T-wave changes occurring 24 h after dosing. The T-wave changes in the three cases of Part 2 occurred 24 h after dosing and lasted for 24 h. The changes of T wave in 19 cases of Part 3 occurred at the earliest 2 h after day 1 administration, and at the latest 30 h after day 5 administration, lasting from 2 h to 5 days. Among them, eight cases returned to normal within 24 h, and eight cases returned to normal within 4 or 5 days. No difference was observed in the high- and low-dose groups.
Gastrointestinal disorders were stomach pain, nausea, vomiting, and diarrhea, with the number of cases in the three parts being seven (25%), four (30%), and ten (28%), respectively. Other AEs related to the study drug in Part 3 were ventricular premature contractions (two cases, 6%) and skin rash (two cases, 6%).
One subject who was a 40-year-old woman in the 1.2 μg/kg dose group in Part 3 withdrew from the study due to abnormal ECG 2 days after administration. Her ECG did not change significantly 2 h after the first day of treatment. On the second day, her ECG showed a flat T wave of lead V1–V6. Two hours later, ECG showed that T wave of lead V3–V6 was inverted. The investigator judged that “sinus rhythm, occasionally atrial premature,” and the subject therefore withdrew from the study after the second day of dosing. After questioning the history, the subject stated that she had intermittent palpitation and discomfort in the precordial area that was exacerbated by weather change and tiredness, which did not exclude the possibility of cardiovascular system disease, so she stopped taking medicine and had 24-h Holter monitoring. During the whole medication and observation period, the subject did not feel discomfort in the precordial area, did not feel panic or shortness of breath, and had a normal diet, activity, and sleep. Twenty-four-hour ECG monitoring suggested sinus rhythm with occasional atrial and ventricular premature beats (1 beat/24 h), no ST changes, and flat T waves in the chest leads.
3.3 Pharmacokinetics
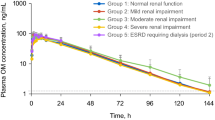
Plasma concentration–time curves are shown in Figs. 2 and 3. Peak time was when the infusion stopped 10 min after the administration. After 45 min of administration, the concentration of rhNRG-1 in plasma was lower than the lower limit of quantification (LLOQ). In Part 3, after continuous administration of 0.8 μg/kg dosing group (day 1, day 5) for 15–20 min, the concentration of rhNRG-1 in plasma was lower than the LLOQ. Table 4 presents the pharmacokinetic parameters of Part 2 and Part 3. From the above data, it can be seen that the half-life of rhNRG-1 in plasma is 13.01 min, and Cmax is 7.645 ng/mL after a single injection of 1.2 μg/kg. After five continuous days of administration, it can be seen that VZ and clearance (Cl ) of day 1 and day 5 are basically the same, VZ slightly decreased, and Cl has no change. The blood concentration of 0.8 μg/kg and 1.2 μg/kg dose did not reach steady state after 5 days of continuous administration, so the steady-state parameters such as Tmin, Cmin, Cavg, and RACC could not be given.

Average plasma concentration–time profiles following administration of rhNRG-1 at a single dose of 1.2 μg/kg (mean ± SD)—Part 2

Average plasma concentration–time profiles at day 1 and day 5 during multiple administrations rhNRG-1 at dose of 0.8 μg/kg (qd) and 1.2 μg/kg (qd) (mean ± SD)—Part 3
4 Discussion
At present, there are two kinds of recombinant human NRG of rhNRG-1 and Cimaglermin that work directly on the damaged cardiomyocytes and restore cardiac function. Studies have shown that the use of recombinant human NRG in patients with CHF can continue to improve cardiac pump function and inhibit or reverse ventricular remodeling [15, 16]. Concentration and metabolism data on the drug in vivo are essential for the efficacy of the drug. Still, there is no report on the pharmacokinetics of recombinant human NRG in humans. In this study, the safety, tolerability, and pharmacokinetics of rhNRG-1 were evaluated for the first time in healthy Chinese subjects by single or multiple daily dosing.
The dose setting of the conducted clinical trial was based on the results of a pharmacodynamic study in dogs (unpublished data): 3 μg/kg of rhNRG-1 was effective in treating cardiac function in dogs with congestive heart failure. The equivalent dose converted to human was 1.6 μg/kg, which is two to three times higher than the equivalent human dose converted via monkeys. That is, different species of animals have different sensitivity to rhNRG-1, and the more evolved, the higher the sensitivity. There is a certain possibility that human may be more sensitive to rhNRG-1. In addition, preliminary results from a pharmacokinetic pretest of a 0.8 μg/kg dose that had been conducted (unpublished data) showed that drug concentrations were no longer detectable in the serum of subjects 30 min after drug injection, and that Tmax was 10 min after drug injection, with Cmax below 10 ng/mL. In summary, to be able to reasonably and effectively assess the pharmacokinetic profile of rhNRG-1 in healthy subjects, a 1.2 μg/kg dose group trial is planned, and based on the results of the trial, a decision will then be made whether to proceed with a lower-dose pharmacokinetic study. Combined with the results of animal pharmacokinetic studies (unpublished studies) suggesting that the pharmacokinetic parameters are consistent with a linear kinetic metabolic profile below the 2.4 μg/kg dose level, the pharmacokinetic characteristics of the 1.2 μg/kg dose should be able to predict the metabolic characteristics of the drug below this dose. Therefore, pharmacokinetic studies at doses of 0.4 and 0.8 μg/kg were not performed in Part 2, and pharmacokinetic tests were performed only for the 1.2 μg/kg dose group.
During continuous dosing, healthy subjects received an intravenous injection of rhNRG-1 for five consecutive days. There was no significant difference in the peak plasma concentrations after the first and the fifth days (P > 0.05). The drug did not accumulate in the body under continuous medication. Continuous administration of rhNRG-1 for 5 days at doses from 0.2 to 1.2 μg/kg were safe and well tolerated. The peak time is about 5–10 min, and then it is quickly eliminated or distributed in the body. It cannot be detected after 45 min. From the 1.2 μg/kg dose group pharmacokinetic parameters, the half-life of rhNRG-1 is very short, only about 10 min, and the peak concentration is 7–8 ng/mL. No drug accumulation for rhNRG-1 was seen in the study.
The gastrointestinal disorders related to the investigational drug were nausea, vomiting, stomach pain, and diarrhea. The frequency and severity of related symptoms did not change with the increase of time of administration. Tissue distribution tests in rats (unpublished results) showed that the drug remained in the gastrointestinal tract for a longer time. A high concentration of drug was still detected in the stomach of rats 4 h after administration. In vitro, NRG-1 can balance β-adrenergic activation by stimulating parasympathetic activity [15]. Gastrointestinal reactions are also the main adverse events in other clinical trials [15,16,17].
By analyzing the dynamic changes of ECG, it was found that, in Part 3 (Table 3), the number of subjects with ECG changes was 4, 7, and 8 in the 0.4, 0.8, and 1.2 μg/kg dose groups, respectively. In Part 1 (Table 2), the number of subjects with ECG changes was 1, 1, 2, 2, and 4 in the 0.2, 0.8, 1.2, 1.6, and 2.4 μg/kg dose groups, respectively. Comprehensive analysis of the dynamic changes in ECG revealed that the number of subjects with ECG changes increased with increasing dose. The results showed that the effect of rhNRG-1 on the amplitude or polarity of T wave is indirect, which may be related to the change of autonomic nervous tension. The results suggested that the dose range of T wave without significant change was 0.2–1.2 μg/kg. After analyzing the changes of ECG parameters before and after administration in each dose group, it was found that PR, QT, QTc, and other parameters had no significant changes before and after administration, indicating that continuous administration did not affect the atrioventricular activation conduction, ventricular depolarization, and repolarization in healthy subjects. T-wave shape, ST-T change amplitude, PR, QT, QTc interval, and Tpeak-end time of each lead did not change regularly with the increase of dose and administration days. This is also consistent with the published clinical trial results [15, 16].
The analysis of the occurrence of ventricular premature beat showed that only two subjects in the lowest-dose group (0.2 μg/kg) had ventricular premature beat. Still, with the increase of administration days, the frequency of ventricular premature beat did not increase. More importantly, no premature beats were found in the high-dose group. The results showed that there was no potential risk of ventricular premature beat induced by rhNRG-1.
Animal studies (unpublished data) in vivo and in vitro showed that a large dose of rhNRG-1 (15 μg/kg, which is a human equivalent dosage of 8.3 μg/kg and five times the prospective clinical dosage) could induce T-wave flattening or minimal inversion by ECG. Still, it did not have effect on myocardial perfusion or coronary circulation and did not increase myocardial oxygen consumption, despite the alteration in the electrophysiological characteristic of cardiac myocytes. The effects of rhNRG-1 on the T-wave amplitude and polarity were most likely indirect, and probably related to autonomic nerve tension changes. Neither clinical trials nor animal experiments found any signs of arrhythmia caused by rhNRG-1. Clinical trials have shown that rhNRG-1 has the effect of reducing myocardial transmural dispersion of repolarization (TDR), indicating its anti-arrhythmic potential. This result was consistent with the results of a phase II trial in patients with CHF [15].
According to safety assessment, there were some differences in rhNRG-1 between men and women in this study. The total incidence of ECG adverse events in female subjects was higher than in male subjects (five females and three males in Part 1; eight females and six males in Part 3, respectively). In the 1.2 μg/kg group of Part 3, the ECG change in female subjects (100%) was significantly greater than that in male subjects (50%). The calculation of the incidence of gastrointestinal adverse events in gender showed that the frequency of gastrointestinal reactions in female subjects was higher than that in male subjects (five females and three males in Part 1; six females and three males in Part 3, respectively). There was no previous report of sex difference in recombinant human NRG study in patients with CHF [15,16,17]. The sex difference needs to be confirmed in clinical trials with larger sample sizes. The mechanisms responsible for the phenomenon are still under investigation. Although previous studies had indicated transient elevations in serum aminotransferases and total bilirubin observed in the phase I clinical trial of Cimaglermin (NRG-1β3) [17,18,19], there were no observed changes in the liver function of the subjects in this study or other clinical trials of rhNRG-1 to date.
5 Conclusion
This study evaluated the safety, tolerability, and pharmacokinetics of rhNRG-1 in healthy Chinese subjects. All dosing regimens and dosages were well tolerated. RhNRG-1 is rapidly cleared from the blood and has a short t1/2 of about 10 min. The adverse events related to rhNRG-1 mainly included flat T wave, inversed T wave, and gastrointestinal reactions, which were all mild and well tolerated. The severity and frequency of adverse reactions did not increase with the prolongation of administration time.
References
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. 2021. Eur Heart J. 2021;42(36):3599–3726.
Britsch S. The neuregulin-I/ErbB signaling system in development and disease. Adv Anat Embryol Cell Biol. 2007;190:1–65.
Geissler A, Ryzhov S, Sawyer DB. Neuregulins: protective and reparative growth factors in multiple forms of cardiovascular disease. Clin Sci (Lond). 2020;134(19):2623–43.
Ikeda Y, Hoshijima M, Chien KR. Toward biologically targeted therapy of calcium cycling defects in heart failure. Physiology. 2008;23:6–16.
Yamada M, Ikeda Y, Yano M, Yoshimura K, Nishino S, Aoyama H, et al. Inhibition of protein phosphatase 1 by inhibitor-2 gene delivery ameliorates heart failure progression in genetic cardiomyopathy. FASEB J. 2006;20(8):1197–9.
Kränkel N, Adams V, Gielen S, Linke A, Erbs S, Schuler G, et al. Differential gene expression in skeletal muscle after induction of heart failure: impact of cytokines on protein phosphatase 2A expression. Mol Genet Metab. 2003;80:262–71.
Meyer D, Birchmeier C. Multiple essential functions of neuregulin in development. Nature. 1995;378:386–90.
Okoshi K, Nakayama M, Yan X, Okoshi MP, Schuldt AJT, Marchionni MA, et al. Neuregulins regulate cardiac parasympathetic activity: muscarinic modulation of beta-adrenergic activity in myocytes from mice with neuregulin-1 gene deletion. Circulation. 2004;110:713–7.
Lai X, Zhong L, Fu HX, Dang S, Wang X, Zhang N, et al. Effects of neuregulin-1 on autonomic nervous system remodeling post-myocardial infarction in a rat model. Neural Regen Res. 2017;12:1905–10.
Lin Y, Liu H, Wang X. Neuregulin 1, a microvascular endothelial derived protein, protects against myocardial ischemia reperfusion injury (Review). Int J Mol Med. 2020;46(3):925–35.
Marks AR. Calcium cycling proteins and heart failure: mechanisms and therapeutics. J Clin Invest. 2013;123:46–52.
Guo YF, Zhang XX, Liu Y, Duan HY, Jie BZ, Wu XS. Neuregulin-1 attenuates mitochondrial dysfunction in a rat model of heart failure. Chin Med J (Engl). 2012;125:807–14.
Li B, Zheng Z, Wei Y, Wang M, Peng J, Kang T, et al. Therapeutic effects of neuregulin-1 in diabetic cardiomyopathy rats. Cardiovasc Diabetol. 2011;10:69.
Parry TJ, Ganguly A, Troy EL, Guerrero JL, Iaci JF, Srinivas M, et al. Effects of neuregulin GGF2 ( cimaglermin alfa) dose and treatment frequency on left ventricular function in rats following myocardial infarction. Eur J Pharmacol. 2017;796:76–89.
Gao R, Zhang J, Cheng L, Wu X, Dong W, Yang X, et al. A phase II, randomized, double-blind, multicenter, based on standard therapy, placebo-controlled study of the efficacy and safety of recombinant human neuregulin-1 in patients with chronic heart failure. J Am Coll Cardiol. 2010;55:1907–14.
Jabbour A, Hayward CS, Keogh AM, Kotlyar E, McCrohon JA, England JF, et al. Parenteral administration of recombinant human neuregulin-1 to patients with stable chronic heart failure produces favourable acute and chronic haemodynamic responses. Eur J Heart Fail. 2011;13:83–92.
Lenihan DJ, Anderson SA, Lenneman CG, Brittain E, Muldowney JAS 3rd, Mendes L, et al. A phase I, single ascending dose study of cimaglermin Alfa (neuregulin 1β3) in patients with systolic dysfunction and heart failure. JACC Basic Transl Sci. 2016;1:576–86.
Longo DM, Generaux GT, Howell BA, Siler SQ, Antoine DJ, Button D, et al. Refining liver safety risk assessment: application of mechanistic modeling and serum biomarkers to cimaglermin alfa (GGF2) clinical trials. Clin Pharmacol Ther. 2017;102(6):961–9.
Mosedale M, Button D, Jackson JP, Freeman KM, Brouwer KR, Caggiano AO, et al. Transient changes in hepatic physiology that alter bilirubin and bile acid transport may explain elevations in liver chemistries observed in clinical trials of GGF2 (Cimaglermin Alfa). Toxicol Sci. 2018;161(2):401–11.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Funding
This study was funded by Zensun (Shanghai) Sci&Tech Co., Ltd.
Conflict of interest
Xiaorui Wang, Xiaoyan Qin, and Mingdong Zhou are employees of Zensun (Shanghai) Sci&Tech Co., Ltd.
Author contributions
Yimin Cui, Mingdong Zhou, and Lei Meng contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Peihong Sun, Lei Meng, Xia Zhao, Ying Zhou, Junyu Xu, Xiaoyan Qin, and Xiaorui Wang. The first draft of the manuscript was written by Junyu Xu, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethics approval
This study was approved by Peking University First Hospital Ethics Committee (China). It was conducted under the Declaration of Helsinki and GCP.
Consent to participate
Before participation in the study, written informed consent was provided by all subjects.
Data availability statement
The datasets generated during and/or analyzed during the current study are not publicly available due to commercial reasons but are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Code availability
Not applicable.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Xu, J., Sun, P., Zhao, X. et al. Safety, Tolerability, and Pharmacokinetics of Recombinant Human Neuregulin-1 in Healthy Chinese Subjects. Am J Cardiovasc Drugs 23, 419–428 (2023). https://doi.org/10.1007/s40256-023-00585-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40256-023-00585-6