
Abstract
Introduction
The aim of this study was to investigate the 2-year postoperative efficacy of the XEN45 Gel Stent by evaluating the reduction of intraocular pressure (IOP) and the need for eye pressure-lowering medications in a multicenter setting in Switzerland.
Methods
Patients with various types of glaucoma who received a XEN45 Gel Stent with or without combined phacoemulsification cataract surgery at five hospitals in Switzerland were retrospectively enrolled. Pre- and postoperative IOP, the number of antiglaucoma medications, and the need of subsequent interventions to control IOP were assessed. The success rate was defined as a ≥ 20% reduction of IOP 2 years postoperatively without the need for subsequent glaucoma surgery.
Results
A total of 345 eyes were included: 44.3% with primary open-angle, 42.0% pseudoexfoliation, and 13.7% with other types of glaucoma. Of these, 206 patients were followed for 2 years. Preoperatively, the mean IOP was 26.3 ± 8.9 mmHg and the mean number of antiglaucoma medications administered was 3.0 ± 1.3. Two years postoperatively, the success rate was 66.0% (95% confidence interval 59.3–72.1%), the IOP had dropped by 43.8% to 14.8 ± 5.7 mmHg, and the number of medications was reduced by a mean of 2.0 ± 1.7 per day. Postoperative complications and the need for interventions remained low.
Conclusion
The XEN45 Gel Stent successfully reduced IOP and the number of antiglaucoma drugs in most patients at 2 years postoperatively.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
This study aimed to investigate the efficacy of the XEN45 Gel Stent. |
The implantation of XEN45 is a surgical procedure aiming to lower intraocular pressures (IOP) and prevent blindness among patients suffering from glaucoma. |
It was examined whether XEN45 can achieve ≥ 20% IOP reduction. |
The XEN45 can successfully reduce IOP. |
Introduction
Glaucoma is the primary cause for irreversible complete loss of vision worldwide [1, 2]. Its progression is multifactorial [3, 4]; however, the intraocular pressure (IOP) is the only proven risk factor that can be adjusted to slow disease progression. Multiple studies have shown that lower IOP values are associated with a lower risk for glaucoma progression [5, 6]. As a result, first-line therapy for treating glaucoma involves the application of IOP-lowering medication or laser treatment, such as selective laser trabeculoplasty (SLT), neodymium-doped yttrium aluminum garnet (Nd:YAG)-iridotomy or cyclophotocoagulation (CPC), depending on the glaucoma etiology. Second-line treatment consists of several surgical approaches [7, 8], which can be subcategorized into conventional filtration surgery, minimal invasive glaucoma surgeries (MIGS), or minimal invasive bleb surgeries (MIBS) [9,10,11]. One MIBS approach involves implanting the XEN45 Gel Stent (XEN45; Allergan-Abbvie, North Chicago, IL, USA), which is a 6-mm collagen-based gelatin implant cross-linked with glutaraldehyde designed to be surgically injected from the anterior chamber into the subconjunctival space in order to increase outflow of aqueous humor and hereby reduce IOP [12]. The use of cross-linked gelatin stent ab interno techniques in order to create drainage blebs was first described in 1995 by Prof. Yu [13]. This type of surgery is considered MIBS, because it is minimally invasive and creates an external subconjunctival fistula or bleb, similar to trabeculectomy (TE), without eliminating the option of conventional filtration surgery in the future [14].
Advantages of MIGS and MIBS procedures compared to conventional glaucoma surgeries are less tissue trauma and faster postoperative recovery and patient satisfaction [15, 16]. According to Sheybani et al. the XEN45 Gel Stent appears to be noninferior to trabeculectomy, per the percentage of patients achieving ≥ 20% IOP, while requiring fewer postoperative interventions, having better visual recovery, and fewer adverse events [17]. Thus, there has been a significant shift from conventional glaucoma surgeries to MIGS recently [18], which are commonly performed as standalone procedures or in combination with cataract surgery. However, despite their popularity during the last decade, the long-term efficacy of MIGS and MIBS is often debated.
Hence, the aim of this study was to investigate the 2-year postoperative efficacy of the XEN45 Gel Stent by evaluating the reduction of IOP and the need for eye pressure-lowering medications in a multicenter real-world setting in Switzerland. To our knowledge, this is the largest reported XEN study with a long observation period.
Methods
This retrospective multicenter study analyzed patients with glaucoma treated with the XEN45 Gel Stent in five tertiary ophthalmology referral centers in Switzerland (University Hospitals of Basel, Bern and Zurich and the Cantonal Hospitals of Aarau and St. Gallen). The study was approved by the corresponding ethics committee (Lead Ethics Committee: Ethics Committee Northwest and Central Switzerland; Swiss Ethics ID 2020-01143) and was conducted in accordance with the Declaration of Helsinki and national and international laws.
Patients diagnosed with glaucoma were retrospectively enrolled if they were older than 18 years and had received a primary XEN45 between January 1, 2016 and December 31, 2019. Patients who declined the use of their health data for research purposes were excluded from the study.
The total number of patients with available pre- and postoperative IOP data was referred to as the full analysis set (FAS). Patients whose postoperative IOP values could not be retrieved for the whole 2-year follow-up period were not excluded from the study; they remained in the FAS, as long as at least one postoperative IOP measurement was available. Patients with data for the whole 2-year postoperative period were referred to as the per protocol set (PPS). For patients who had both eyes surgically treated, one eye was randomly excluded from the analysis before defining FAS and PPS to avoid treating both eyes independently of each other.
The preoperative IOP was determined on the day surgery was indicated. IOP measurements were noted on the first postoperative day as well as 1 week, 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively. Additionally, the number of antiglaucoma medications was recorded preoperatively and at the last available follow-up examination. All complications and postoperative interventions were recorded.
All patients were treated with a XEN Gel Stent 45 μm through a classic ab interno approach as described previously in multiple publications, e.g., Fae et al. [19], Vera et al. [12] and Saletta et al. [20]. The XEN45 implantation was performed as a standalone surgery or in combination with phacoemulsification cataract surgery. Postoperative therapy included corticosteroids tapered for at least 3 months and local antibiotics.
The primary outcome of this study was the success rate of XEN45 surgery at 2 years postoperatively. Success was defined as ≥ 20% IOP reduction at the 2-year follow-up examination. Numerical hypotony (IOP ≤ 5 mmHg) or the need for subsequent glaucoma surgery was regarded as an unsuccessful outcome. We defined “total success” as successful cases without antiglaucoma medication or postoperative interventions within a 2-year postoperative period. Further we looked into the “total success allowing needling”, since needlings are expected after filtrating surgeries such as XEN45 surgery and should be regarded as part of the postoperative care rather than a complication and are therefore usually termed “needling procedure” [21]. The secondary outcomes included success rate of XEN45 surgery at the last available IOP measurement, the reduction in total number of antiglaucoma medications, and the evaluation of complication rates. As a supplementary analysis, we identified potential predictors for a successful XEN45 implantation. We also explored whether the success of XEN45 implantation in one eye could predict the success of the implantation in the other eye of a patient.
All analyses were performed in R version 4.2.1 (2022-06-23) or higher (R Core Team, 2022). For the primary analysis, the success rate of surgery was estimated on the basis of the PPS. In addition to the estimated success rate, a 95% confidence interval (CI; Wilson’s score interval) was reported. Spearman correlations were performed in the exploratory analysis to determine whether success in one eye was associated with success in the other eye. Univariate logistic regression models were used to identify potential predictors for a successful surgery. We looked for the multiple logistic regression model containing the set of most important determinants (among the considered predictors), using an automated variable selection based on the Akaike information criterion (AIC).
Results
The raw data comprised 408 eyes of 357 patients. Overall, 63 eyes were excluded including two because of duplication and one because of prior XEN45 glaucoma surgery. Additionally, nine eyes were excluded from all analyses because of missing preoperative IOP measurements and follow-up data. Finally, 51 patients were treated bilaterally, but only one eye was included in the final analysis. Thus, the final FAS database contained 345 eyes (345 patients) and the PPS dataset contained 206 eyes (206 patients; eyes with complete 2-year follow-up data). All analyses were performed for both the FAS and the PPS population. Baseline characteristics for the included patients are displayed in Table 1. Overall, 153 (44.3%) eyes of the FAS population had primary open angle glaucoma, 145 (42.0%) eyes had pseudoexfoliation glaucoma, and 47 (13.6%) eyes had other types of glaucoma.
In the PPS population the mean IOP decreased by 43.8%. The mean IOP reduced from 26.3 ± 8.9 mmHg preoperatively to 14.8 ± 5.7 mmHg at 2 years postoperatively. The postoperative IOP values in the PPS population were between 6 and 21 mmHg in 88.8% of cases (95% CI 83.8–92.4%), between 6 and 17 mmHg in 76.7% of cases (95% CI 70.5–82.0%]), and between 6 and 14 mmHg in 53.4% of cases (95% CI 46.6–60.1%) (Table 2). Boxplots of postoperative IOP measurements are displayed in Fig. 1.

Boxplots of IOP measurements (mmHg) over time in the FAS population. IOP intraocular pressure, FAS full analysis set
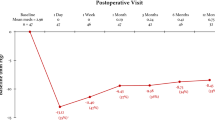
The mean number of preoperative IOP-lowering medications was 3.0 ± 1.3 in the FAS and the PPS population. Postoperatively mean number had reduced for both populations to 1.1 ± 1.3, while 53.7% of patients in the FAS did not need any IOP-regulating medication. The average change in number of antiglaucoma medications needed was − 2.0 ± 1.7 in the FAS and the PPS population (Fig. 2).

Number of drugs required preoperatively and at 2 years postoperatively (PPS population). The marginal distributions at each time point are also displayed
Surgery-related complications in the FAS population included choroidal detachment (9.3%), hyphema (5.2%), shallow anterior chamber (3.8%), dislocation of the XEN45 implant (3.2%), a positive Seidel test (1.4%), hypotony maculopathy (1.2%), endophthalmitis (0.3%), and extrusion of the implant (0.3%) (Table 3). Postoperative interventions included laser iridoplasty (0.6%), Nd:YAG laser to implant (2.9%) due to obstruction, open bleb revision (8.7%), anterior chamber (AC) deepening with buffered salt solution or viscoelastic device (1.7%), and subsequent glaucoma surgery (10.4%). In 37.1% of eyes in the FAS population, at least one needling with or without MMC or 5-FU was performed. An injection of MMC or 5-FU without needling was performed in 12.5% of eyes. In total 42.2% of the PPS population required needling within the 2-year period after surgery. In our study, eyes with successful XEN45 implantation needed fewer needlings than patients with unsuccessful XEN45 implantation (33.6% vs 44.0%). Generally, more postoperative interventions were needed for patients with unsuccessful XEN45 implantation surgery, except for the AC deepening with buffered salt solution or optical viscoelastic device, which was more common in eyes following successful surgery. The standard mean differences (SMD) are described in Table 4.
The success rate of surgery, which was the primary outcome of this study, was calculated on the basis of the PPS population. In the PPS population at 2 years postoperatively the success rate of surgery was 66.0% (95% CI 59.3–72.1%), while the “total success” rate was 23.5% (95% CI 18.1–29.5%). The “total success allowing needling” rate was 30.1% (95% CI 23.8–36.2%).
Finally, none of the analyzed potential factors showed a strong predictive value for successful XEN45 implantation (Table 5). The estimated odds ratios suggested that patients who underwent any glaucoma surgery other than SLT or TE prior to XEN45 implantation might have had lower chances of a successful XEN45 implantation (OR 0.4 [95% CI 0.1, 1.0]). Furthermore, a successful XEN45 implantation in the first eye had a positive predictive power on the postoperative outcome of the second eye.
Discussion
In this study, we investigated the efficacy of MIBS with the XEN Gel Stent 45 μm implant to treat glaucoma. We found that XEN45 surgery lowered IOP to the mid-teens and reduced the need for antiglaucoma medications.
The success rate of the XEN45 surgery at 2 years in our study (66.0%) is in line with the success rates reported in the literature (34–86%) [22]. The IOP reduction at 2 years in our study (43.8%) is comparable to the rates presented by Lenzhofer et al. (n = 64 eyes) [23] at 4 years postoperatively (40%); however, the reduction observed in this study is higher compared to other studies of a similar size at 2 years postoperatively such as the 27.8% reported by Reitsamer et al. (n = 202 eyes) [24] or 37% by Gillmann et al. (n = 149) [25]. The high success rate in our population could be due to a higher preoperative baseline IOP if one assumes that a successful XEN45 implantation sets the postoperative IOP at approximately 15 mmHg as described by Chen et al. [22] independently of the preoperative IOP values. The baseline IOP of this study was 26.3 mmHg, while that in the study by Reitsamer et al. [24] was 21.4 mmHg, and in the study by Gillmann et al. [25] it was 20.8 mmHg. The postoperative IOPs were all around 15 mmHg (14.8 ± 5.7 mmHg in this study, 15.2 mmHg in Reitsamer et al. [24], and 13.1 mmHg in Gillmann et al. [25]). It can be postulated that the decision-making for implanting a XEN45 Gel Stent should be based on the need to achieve a target IOP of about 15 mmHg, rather than the need to lower the IOP by a certain percentage.
In this study, 2 years postoperatively the IOP was regulated with approximately two (2.0 ± 1.7) antiglaucoma medications per day fewer compared to baseline. This reduction is slightly higher compared to other large studies such as Reitsamer et al., Gillmann et al., and Wanichwecharungruang et al. where the change in the mean number of IOP-lowering medications was between − 1.5 and − 1.7 [24,25,26]. However, these studies had a lower mean preoperative number of antiglaucoma medications than our study (2.7 and 2.2 vs 3.03) [24, 26]. In Gabbay et al. a similar reduction in medications compared to this study was seen; the mean number of medications dropped from 2.6 ± 1.1 at baseline to 0.5 ± 0.9 at 24 months [27]. In the study by Lenzhofer et al. a significant reduction in the mean number of IOP lowering medication was reported from 2.4 ± 1.3 preoperatively at baseline to 1.2 ± 1.3 (− 50%, n = 34) postoperatively [23].
The documented complication rates in this study, hyphema (5.2%), shallow AC rates (3.8%), and XEN45 dislocation (3.2%), were lower in comparison to other studies such as Scheres et al. where 22% of XEN45 treated eyes showed hyphema, 5% required reformation of AC due to hypotony, and migration of XEN45 was seen in 2% of eyes [28]. Inner obstruction of the implant, which could be resolved with Nd:YAG laser, was described by Lenzhofer et al. [23] in 3% (2 patients) of cases, which is similar to the 2.9% reported in this study. Although needlings with MMC or 5-FU are expected after filtrating surgeries like a XEN45 implantation [21], in this study the higher number of needlings was associated with unsuccessful XEN45 implantation. Yang et al. report that XEN45 implantation surgery requires a higher number of postoperative needlings than TE, which is a conventional ab externo filtrating surgery [29]. The high number of bleb needlings after XEN45 implantation might reflect the fact that during ab interno approach the conjunctiva is not being undermined.
As part of the supplementary analysis of this study, the potential predictors for a successful XEN45 surgery were investigated. The age at surgery did not affect the success of XEN45 surgery. POAG and PEX glaucoma showed similar postoperative success rates, which falls in line with an emerging amount of literature as seen in the review and meta-analysis by Yang et al. [29]. Whether the success for these two glaucoma types is superior or inferior to the other glaucoma types could not be reliably evaluated because of the low number in the latter group. The comparison between XEN45 as a standalone surgery or in combination with phacoemulsification cataract surgery did not show a statistically significant difference in the success of the surgery. Similar results are reported by the majority of studies between XEN and combined surgery (phaco-XEN) [29,30,31,32]. Previous SLT did not alter the success rates. Previous trabeculectomy showed a slightly reduced success rate. Other previous glaucoma surgeries such as CPC and tube shunt surgery were related to an even lower success rate. Similarly, Lewczuk et al. in 2021 reported no differences in success rates between XEN45 implantation in 43 surgery-naive patients with glaucoma and 43 patients after previous glaucoma surgeries [33].
Our real-world study has several strengths. One is the multicenter design and inclusion of various glaucoma types. Furthermore, to our knowledge, it is the largest study assessing the long-term (i.e., 2 years) success of the XEN45 implant in patients with glaucoma. Nevertheless, we acknowledge some limitations. First, it is a retrospective study design. Second, many patients opted for follow-up examinations at their ophthalmologist in private practice, which made it more difficult to obtain all data. Thus, a selection bias cannot be excluded. However, this bias would most likely be in favor of reporting worse success rates. For example, only complicated cases may have led patients to attend all follow-up examinations at a tertiary center. Third, most patients were white. Success rates are usually better and complication rates lower in white patients compared to patients with more pigmentation, e.g., African-Americans [34]. Finally, among hospitals and surgeons, slight variations with regard to MMC concentration used, the amount of time taken for its application, and the use of contact lens at the end of the surgery were seen. Therefore, the results might have varied between the hospitals and the surgical technique cannot be compared in every detail as reported in other studies.
Conclusion
XEN45 Gel Stent surgery successfully reduced IOP and the number of antiglaucoma medications in most patients up to 2 years postoperatively with a low complication rate. This favorable outcome in a real-world setting supports the effective glaucoma control by XEN45 Gel Stent surgery. This might influence clinical practitioners on the use of MIGS for the management of glaucoma and might contribute to the development of further filtrating implants possibly requiring even less postoperative care.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Bourne RRA, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet Glob Health. 2013;1:e339–49.
Tham Y-C, Li X, Wong TY, Quigley HA, Aung T, Cheng C-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040. Ophthalmology. 2014;121:2081–90.
Agarwal R, Gupta S, Agarwal P, Saxena R, Agrawal S. Current concepts in the pathophysiology of glaucoma. Indian J Ophthalmol. 2009;57:257.
Heijl A, Bengtsson B, Hyman L, Leske MC. Natural history of open-angle glaucoma. Ophthalmology. 2009;116:2271–6.
Heijl A. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120:1268.
Musch DC, Gillespie BW, Lichter PR, Niziol LM, Janz NK. Visual field progression in the collaborative initial glaucoma treatment study. Ophthalmology. 2009;116:200-207.e1.
Burr J, Azuara-Blanco A, Avenell A, Tuulonen A. Medical versus surgical interventions for open angle glaucoma. Cochrane Database Syst Rev. 2012. https://doi.org/10.1002/14651858.CD004399.pub3.
Schmidl D, Schmetterer L, Garhöfer G, Popa-Cherecheanu A. Pharmacotherapy of glaucoma. J Ocul Pharmacol Ther. 2015;31:63–77.
Saheb H, Ahmed IIK. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23:96–104.
Qidwai U, Jones L, Ratnarajan G. A comparison of iStent combined with phacoemulsification and endocyclophotocoagulation (ICE2) with the PreserFlo MicroShunt and XEN-45 implants. Ophthalmol Eye Dis. 2022;14:251584142211256.
Birnbaum FA, Neeson C, Solá-Del VD. Microinvasive glaucoma surgery: an evidence-based review. Semin Ophthalmol. 2021;36:772–86.
Vera V, Gagne S, Myers JS, Ahmed I. Surgical approaches for implanting Xen Gel Stent without conjunctival dissection. Clin Ophthalmol. 2020;14:2361–71.
Yu D-Y, Morgan WH, Sun X, et al. The critical role of the conjunctiva in glaucoma filtration surgery. Prog Retin Eye Res. 2009;28:303–28.
Schlenker MB, Gulamhusein H, Conrad-Hengerer I, et al. Efficacy, safety, and risk factors for failure of standalone ab interno gelatin microstent implantation versus standalone trabeculectomy. Ophthalmology. 2017;124:1579–88.
Gurnani B, Tripathy K. Minimally invasive glaucoma surgery. StatPearls. Treasure Island (FL): StatPearls; 2022.
Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS ONE. 2017;12:e0183142.
Sheybani A, Vera V, Grover DS, et al. Gel Stent versus trabeculectomy: the randomized, multicenter, Gold-Standard Pathway Study (GPS) of effectiveness and safety at 12 months. Am J Ophthalmol. 2023;252:306–25.
Luebke J, Boehringer D, Anton A, Daniel M, Reinhard T, Lang S. Trends in surgical glaucoma treatment in Germany between 2006 and 2018. CLEP. 2021;13:581–92.
Fea AM, Durr GM, Marolo P, Malinverni L, Economou MA, Ahmed I. XEN® Gel Stent: a comprehensive review on its use as a treatment option for refractory glaucoma. Clin Ophthalmol. 2020;14:1805–32.
Saletta G, Alexoudis A, Gatzioufas Z, et al. Retrospective analysis of 12 months glaucoma implant efficacy: XEN45 and PreserFlo microshunt. Klin Monbl Augenheilkd. 2022;239:429–34.
Olivari S, Cutolo CA, Negri L, et al. XEN implant fracture during needling procedure. J Glaucoma. 2019;28:1086–9.
Chen X, Liang Z, Yang K, et al. The outcomes of XEN gel stent implantation: a systematic review and meta-analysis. Front Med. 2022;9:804847.
Lenzhofer M, Kersten-Gomez I, Sheybani A, et al. Four-year results of a minimally invasive transscleral glaucoma gel stent implantation in a prospective multi-centre study. Clin Exp Ophthalmol. 2019;47:581–7.
The Apex Study Group, Reitsamer H, Sng C, et al. Two-year results of a multicenter study of the ab interno gelatin implant in medically uncontrolled primary open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol. 2019;257:983–96.
Gillmann K, Bravetti GE, Rao HL, Mermoud A, Mansouri K. Combined and stand-alone XEN 45 gel stent implantation: 3-year outcomes and success predictors. Acta Ophthalmol. 2021. https://doi.org/10.1111/aos.14605.
Wanichwecharungruang B, Ratprasatporn N. 24-month outcomes of XEN45 gel implant versus trabeculectomy in primary glaucoma. PLoS ONE. 2021;16:e0256362.
Gabbay IE, Goldberg M, Allen F, et al. Efficacy and safety data for the ab interno XEN45 gel stent implant at 3 years: a retrospective analysis. Eur J Ophthalmol. 2022;32:1016–22.
Scheres LMJ, Kujovic-Aleksov S, Ramdas WD, et al. XEN® Gel Stent compared to PRESERFLOTM MicroShunt implantation for primary open-angle glaucoma: two-year results. Acta Ophthalmol. 2021. https://doi.org/10.1111/aos.14602.
Yang X, Zhao Y, Zhong Y, Duan X. The efficacy of XEN gel stent implantation in glaucoma: a systematic review and meta-analysis. BMC Ophthalmol. 2022;22:305.
Nicolaou S, Khatib TZ, Lin Z, et al. A retrospective review of XEN implant surgery: efficacy, safety and the effect of combined cataract surgery. Int Ophthalmol. 2022;42:881–9.
Laborda-Guirao T. Efficacy and safety of XEN 45 gel stent alone or in combination with phacoemulsification in advanced open angle glaucoma patients: 1-year retrospective study. Int J Ophthalmol. 2020;13:1250–6.
Karimi A, Lindfield D, Turnbull A, et al. A multi-centre interventional case series of 259 ab-interno Xen gel implants for glaucoma, with and without combined cataract surgery. Eye. 2019;33:469–77.
Lewczuk K, Konopińska J, Jabłońska J, et al. XEN glaucoma implant for the management of glaucoma in naïve patients versus patients with previous glaucoma surgery. JCM. 2021;10:4417.
Nguyen AH, Fatehi N, Romero P, et al. Observational outcomes of initial trabeculectomy with mitomycin C in patients of African descent vs patients of European descent: five-year results. JAMA Ophthalmol. 2018;136:1106–13.
Funding
Financial support for the statistical analysis of this study came from the Research Council Cantonal Hospital Aarau, Aarau, Switzerland. The funding organization had no role in the design or conduct of this research. The journal’s Rapid Service Fee was funded by the authors.
Author information
Authors and Affiliations
Contributions
The authors who contributed to the study conception and design were Anthia Papazoglou, René Höhn, Konstantin Gugleta, Marc Töteberg-Harms, Markus Tschopp. Data collection was performed by Anthia Papazoglou, René Höhn, Megir Schawkat, Giulia Saletta, Milko Iliev, Margarita Todorova, Barabara Wagels and Iwona Krzyzanowska. Data analysis was undertaken by Andrea Wiencierz, Christoph Tappeiner and Markus Tschopp. The first draft of the manuscript was written by Anthia Papazoglou and Markus Tschopp and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of Interest
All authors (Anthia Papazoglou, René Höhn, Megir Schawkat, Christoph Tappeiner, Milko Iliev, Konstantin Gugleta, Giulia Saletta, Andrea Wiencierz, Barbara Wagels, Margarita Todorova, Iwona Krzyzanowska, Marc Töteberg-Harms, Markus Tschopp) declare that they have no competing interests.
Ethical Approval
The study was approved by the corresponding ethics committee (Lead Ethics Committee: Ethics Committee Northwest and Central Switzerland; Swiss Ethics ID 2020-01143) and was conducted in accordance with the Helsinki Declaration of 1964, and its later amendments and national and international laws. Patients who declined the use of their health data for research purposes were excluded from the study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Papazoglou, A., Höhn, R., Schawkat, M. et al. Swiss Multicenter Ab Interno XEN45 Gel Stent Study: 2-Year Real-World Data. Ophthalmol Ther 13, 1513–1525 (2024). https://doi.org/10.1007/s40123-024-00917-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-024-00917-y