
Abstract
Brachytherapy is widely used for the treatment of choroidal melanoma and has recently been explored for the treatment of wet age-related macular degeneration. We propose the use of low dose radiation via episcleral brachytherapy in refractory cases of central serous chorioretinopathy (CSCR). The pathogenesis of CSCR involves dilatation and hyperpermeability of large choroidal vessels. Low dose radiation can induce intimal proliferation in large choroidal vessels and decrease their hyperpermeability. Concerns about the use of brachytherapy in CSCR include damage to the choriocapillaris or the retinal vessels. This can be addressed with the use of a specialized device through which a very precise and appropriate dose can be delivered. The dose of the radiation delivered decreases exponentially at a depth of approximately 0.5–1.5 mm from the devise–sclera interface. Considering an increased choroidal thickness in cases of CSCR, delivery of a safe dose can be assured.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Brachytherapy is commonly used for the treatment of choroidal melanoma and recently it has been explored for the treatment of wet age-related macular degeneration. |
We propose the use of episcleral brachytherapy in refractory cases of central serous chorioretinopathy (CSCR). Low dose radiation can induce intimal proliferation in large choroidal vessels and decrease their hyperpermeability. |
Dose titration of the radiation will be the key to minimize the damage to the choriocapillaris and avoid radiation retinopathy, radiation maculopathy, radiation neuropathy, and cataract. Specialized devices for episcleral brachytherapy such as the SalutarisMD are promising additional safety and ease of performing the procedure, thus making it more practical. |
Thus, the role of brachytherapy in the treatment of refractory CSCR may be worth exploring. |
Central serous chorioretinopathy (CSCR) is a disease characterized by the neurosensory detachment with or without pigment epithelial detachment due to dysfunctional retinal pigment epithelium (RPE) and hyperpermeable choroid. Choroidal features of CSCR are choriocapillaris attenuation and dilatation of large vessels of the choroid. Whether dilated large vessels of the choroid cause a mechanical compression of the choriocapillaris layer, or atrophy of the choriocapillaris is the primary event, is still debatable [1]. Many studies have demonstrated a reduced stromal area in CSCR, which is indicative of atrophied stroma [1]. Lee et al. hypothesized that chronic low grade inflammation due to chronic venous congestion leads to extravasation of proinflammatory and prothrombotic proteins and mediators into the stroma which causes extracellular matrix destruction and stromal atrophy [1].
The acute, isolated event of CSCR mostly resolves spontaneously, but the chronic variant of the disease, which is also known as diffuse retinal pigment epitheliopathy, is progressive and can lead to severe bilateral visual impairment [2]. Many treatment options have been tried for this form of the disease and so far photodynamic therapy (PDT) is the treatment of choice. However, PDT shows limited success in 30–40% of cases with risk of complications including vision loss [3]. Limited availability of verteporfin and laser systems in many countries and an off-label indication are making PDT as a vanishing treatment option. The limited role of eplerenone, as reported by the VICI trial [4], further limits the treatment options for this debilitating disease. In our search to explore more treatment options for refractory cases of CSCR, we propose brachytherapy delivered by a radionuclide brachytherapy source (RBS) to be an alternative.
While aiming to treat refractory CSCR, our prime target will be the hyperpermeable choroidal vasculature. Studying the effect of radiation on the choroid vasculature will provide useful insight into its mechanism of action and thus evaluating its potential use. Amoaku et al. [5] performed an indocyanine green angiography study of choroidal vasculature in the irradiated peritumoral zone in eyes treated with 106Ru/106Rh brachytherapy for choroidal melanoma. The earliest alterations were observed in the RPE and choriocapillaris. Vaso-occlusion occurred in the normal choroid present in the peritumoral area within 3–4 months of brachytherapy. Although smaller vessels were involved initially, the process slowly progressed to involve larger vessels. The authors postulated that the initiating event was the radiation-induced localized endothelial cell loss which led to a cascade of events resulting in the vascular occlusion [5]. The authors had noted platelet aggregates in choriocapillaris in experimental studies on radiation choroidopathy [6]. These changes were secondary to high dosage (69.9 Gy) used to treat choroidal melanoma. Other concerns associated with plaque radiotherapy include development of choroidal neovascularization (CNV), radiation maculopathy, optic neuropathy, and radiation chorioretinopathy [5].
A lower dose of radiation is being investigated in the treatment of wet age-related macular degeneration (AMD) with the purpose of reducing the need for anti-vascular endothelial growth factor (VEGF) treatment and improving visual outcomes. Radionuclide strontium-90 (90Sr) emits only high energy beta particles which has highest attenuation in biological tissues making it more suitable for ocular use. Yttrium-90 (90Y) is the daughter product of 90Sr after beta decay and emits more energetic beta particles [7]. Epimacular brachytherapy has been used to deliver beta radiation after pars plana vitrectomy and positioning a probe over the CNV complex [7]. The end of the probe contains a source of 90Sr/90Y radiation [7]. The device is held in position for 5 min, which is long enough to deliver 24 Gy to the CNV lesion. Since beta radiation dose decreases as a function of 1/r2 with increasing distance from the source, the optic nerve receives about 2.4 Gy, and the lens only 0.56 mGy (threshold for cataract formation is 2 Gy) [8]. Stereotactic radiotherapy is another method of radiotherapy that provides stereotactic application of low energy X-ray to the CNV using three highly collimated beams that cross the inferior sclera to overlap at the macula [9]. Unlike epimacular brachytherapy, this outpatient-based radiotherapy does not require vitrectomy and thus is a more practical method of radiotherapy [9].
The background on the effect of high dose radiation on capillary vessels comes from studies of stereotactic radiosurgery on arteriovenous malformations (AVMs), where doses of 14–24 Gy are typically used. Histological studies on the effect of stereotactic radiosurgery (gamma knife radiosurgery) on the AVMs of the brain revealed four stages in irradiated vessels: (i) endothelial damage or intimal separation, (ii) concentric intimal-medial proliferation, (iii) concentric wall thickening with loss of cellularity and hyalinization (deposition of dense fibrillar collagen), and (iv) last stage of hyaline obliteration of vessel structure [10]. The effect on the vessel depended on the vessel size and the dose of radiation. The outcome of the treatment—decreased blood flow through arteriovenous malformation a few months to years after radiosurgery—has been demonstrated in many studies [11].
Our aim while exploring radiotherapy as a treatment option for refractory CSCR is to decrease the blood flow through the large choroidal vessels without obliteration of the choriocapillaris. The mechanism of action in this case would likely be due to the effect of radiation on the endothelial cells. Studies have shown that in vitro acute doses of 10 Gy or higher can cause apoptosis and senescence of endothelial cells, but this is highly organ dependent [12]. When higher doses of acute radiation (10 Gy or higher) are used, endothelial progenitor cells undergo a Bax-mediated apoptosis, whereas well-differentiated endothelial cells undergo cellular senescence similar to aging. The net effect of this process is fibrosis resulting in less vascular permeability [12]. The radiation dose can even be reduced further to attain the desired effect of producing intimal proliferation whereby the leakiness stops or is reduced. Unlike the effect on cancer cells where the objective is to create enough deoxyribonucleic acid (DNA) double-strand breaks to induce cell death, in its application for CSCR, the lower radiation dose will cause deposition of collagen around the leaky vessels thus changing their permeability over a period of months.
When an RBS is placed on or near the sclera, it may be possible for the radiation to affect the large choroidal vessel layer without adversely affecting the choriocapillaris as a result of its rapid dose fall-off (Fig. 1). The dose of the radiation is an exponential function for depths from approximately 0.5 mm to 1.5 mm, where the depth is measured from the front face of the device (the device–sclera interface has a depth of zero). Dose = Dn exp[− 0.846 (d − dn)], where the depth of interest is d. Dn is the dose at the depth dn which is the normalization depth (or treatment depth).

Depiction of exponential decline in radiation dose with depth from the device. a Graph showing exponential decline of the dose of radiation with increasing depth from the device. b In a normal eye, the dose of radiation delivered at the sclera–choroid interface is 12.4 Gy. The dose is 10 Gy at the interface of large choroidal vessels and medium vessels/choriocapillaris. c In an eye with central serous chorioretinopathy (CSCR), the dose of radiation delivered at the sclera–choroid interface would be less than 12.4 Gy considering increased scleral thickness in CSCR. The dose of radiation at the interface of large choroidal vessels and medium vessels/choriocapillaris will be 8 Gy because of the increased thickness of the large choroidal vessel layer
Studies have shown choroidal thickness at the macula is around 256 µm of which 204 µm is occupied by the large vessels (Haller layer) and 52 µm by the choriocapillaris/Sattler layer in normal eyes [13]. In CSCR, total choroidal thickness is increased (394 µm) because of increased thickness of the large vessel layer (307 µm) [14]. Scleral thickness at the posterior pole is around 1 mm [15]. Although scleral thickness at the posterior pole has not been measured in eyes with CSCR, scleral thickness 6 mm posterior to the scleral spur, as measured on anterior segment optical coherence tomography, is thicker than in normal eyes and an increased scleral thickness has been implicated in the pathogenesis of CSCR [16]. Thus, we expect the radiation dose delivered to choriocapillaris to be less than 10 Gy (Fig. 1 and Table 1). At this dose, it will be possible to induce the intimal proliferation in larger choroidal vessels and reduce hyperpermeability while minimizing damage to the choriocapillaris.
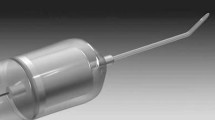
A novel episcleral brachytherapy device has been introduced by Salutaris Medical Devices, Inc. (SalutarisMD) to treat wet AMD with an accurate therapeutic dose [17]. It employs a 90Sr/90Y source RBS encapsulated in a stainless-steel holder which is loaded into the distal end of the applicator’s curved cannula. The device is introduced through the retrobulbar sub-Tenon route and radiation is delivered through the sclera to the CNV lesion over a matter of minutes [17] (Fig. 2). A clinical trial to assess the safety and feasibility of the device in patients with wet AMD has been started and is expected to complete in 2022 [18].

(Courtesy: SalutarisMD)
Episcleral brachytherapy device introduced via sub-Tenon route to deliver radiation to choroidal neovascular complex through sclera.
Hence, the role of brachytherapy in the treatment of refractory CSCR may be worth exploring. Dose titration of the radiation will be the key to minimize the damage to the choriocapillaris and avoid radiation retinopathy, radiation maculopathy, radiation neuropathy, and cataract. Specialized devices for episcleral brachytherapy such as the SalutarisMD are promising additional safety and ease of performing the procedure, thus making it more practical.
References
Lee M, Lee H, Kim HC, Chung H. Changes in stromal and luminal areas of the choroid in pachychoroid diseases: insights into the pathophysiology of pachychoroid diseases. Investig Ophthalmol Vis Sci. 2018;59(12):4896–908.
Daruich A, Matet A, Dirani A, et al. Central serous chorioretinopathy: recent findings and new physiopathology hypothesis. Prog Retin Eye Res. 2015;48:82–118.
van Rijssen TJ, van Dijk EHC, Yzer S, et al. Central serous chorioretinopathy: towards an evidence-based treatment guideline. Prog Retin Eye Res. 2019;73: 100770.
Lotery A, Sivaprasad S, O’Connell A, et al. Eplerenone for chronic central serous chorioretinopathy in patients with active, previously untreated disease for more than 4 months (VICI): a randomised, double-blind, placebo-controlled trial. Lancet. 2020;395(10220):294–303.
Amoaku WM, Lafaut B, Sallet G, De Laey JJ. Radiation choroidal vasculopathy: an indocyanine green angiography study. Eye (Lond). 1995;9(Pt 6):738–44.
Amoaku WM, Mahon GJ, Gardiner TA, Frew L, Archer DB. Late ultrastructural changes in the retina of the rat following low-dose X-irradiation. Graefes Arch Clin Exp Ophthalmol. 1992;230(6):569–74.
Avila MP, Farah ME, Santos A, et al. Twelve-month safety and visual acuity results from a feasibility study of intraocular, epiretinal radiation therapy for the treatment of subfoveal CNV secondary to AMD. Retina. 2009;29(2):157–69.
Casaroli-Marano RP, Alforja S, Giralt J, Farah ME. Epimacular brachytherapy for wet AMD: current perspectives. Clin Ophthalmol. 2014;8:1661–70.
Neffendorf JE, Jackson TL. Stereotactic radiotherapy for wet age-related macular degeneration: current perspectives. Clin Ophthalmol. 2015;9:1829–34.
Schneider BF, Eberhard DA, Steiner LE. Histopathology of arteriovenous malformations after gamma knife radiosurgery. J Neurosurg. 1997;87(3):352–7.
Yamamoto M, Jimbo M, Ide M, Lindquist C, Steiner L. Postradiation volume changes in gamma unit-treated cerebral arteriovenous malformations. Surg Neurol. 1993;40(6):485–90.
Venkatesulu BP, Mahadevan LS, Aliru ML, et al. Radiation-induced endothelial vascular injury: a review of possible mechanisms. JACC Basic Transl Sci. 2018;3(4):563–72.
Branchini LA, Adhi M, Regatieri CV, et al. Analysis of choroidal morphologic features and vasculature in healthy eyes using spectral-domain optical coherence tomography. Ophthalmology. 2013;120(9):1901–8.
Chung YR, Kim JW, Kim SW, Lee K. Choroidal thickness in patients with central serous chorioretinopathy: assessment of Haller and Sattler layers. Retina. 2016;36(9):1652–7.
Vurgese S, Panda-Jonas S, Jonas JB. Scleral thickness in human eyes. PLoS One. 2012;7(1):e29692.
Imanaga N, Terao N, Nakamine S, et al. Scleral thickness in central serous chorioretinopathy. Ophthalmol Retina. 2021;5(3):285–91.
Hamilton R, Cetas T, Gordon J, Lutz W, Marsteller L. SU-E-T-308: dosimetry of a new minimally invasive episcleral brachytherapy device. Med Phys. 2012;39(6 Part 14):3774.
Salutaris Medical Devices. Episcleral brachytherapy for the treatment of wet AMD (NEAMES). https://clinicaltrials.gov/ct2/show/NCT02988895?term=episcleral+brachytherapy&rank=1. Accessed 2 July 2022.
Acknowledgements
Funding
Funding for the journal’s Rapid Service fee was provided by SalutarisMD.
Author Contributions
All four authors contributed to the concept and design of the work, drafting the manuscript, revising it and finally approving it. Dr Supriya Arora and Dr Jay Chhablani contributed to the medical part of the project and Dr Baldassarre D. Stea and Dr Russell J. Hamilton contributed to the physics aspect of the project.
We would like thank Mary Drew, Ryan Lohrenz and George Mimura from SalutarisMD for their help with this proposal.
Disclosures
Dr Jay Chhablani is a consultant for Salutaris Medical Devices, Allergan, Novartis and Biogen. Dr Russell J. Hamilton is a founder and currently serves on the Scientific Advisory Board of Salutaris Medical Devices, Inc. Dr Baldassarre D. Stea currently serves on the Scientific Advisory Board of Salutaris Medical Devices, Inc.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Arora, S., Stea, B.D., Hamilton, R.J. et al. Brachytherapy for Central Serous Chorioretinopathy. Ophthalmol Ther 11, 1611–1616 (2022). https://doi.org/10.1007/s40123-022-00543-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-022-00543-6