
Abstract
Introduction
This study aimed to estimate risks of cardiovascular and cerebrovascular events in patients treated with lisdexamfetamine dimesylate (LDX) compared with patients previously treated with other attention-deficit/hyperactivity disorder (ADHD) medications (amphetamine, dexamphetamine, methylphenidate or atomoxetine).
Methods
This population-based cohort study used data from Danish and Swedish medical and administrative national registers. The LDX cohort included adult patients initiating LDX with at least 12 months’ data preceding first LDX dispensing (index date). A random sample of patients treated with at least one non-LDX ADHD medication in the 6–24 months (but not less than 6 months) before index date (previous-users cohort) were matched to LDX users on age, sex, region and calendar year. The primary outcome, a composite of major adverse cardiovascular and cerebrovascular events (MACE), included first hospitalisation for acute myocardial infarction or stroke and out-of-hospital coronary heart disease or cerebrovascular disease death. Incidence rates (IRs) and IR ratios (IRRs) with 95% confidence intervals (CIs) of MACE were estimated using Poisson regression.
Results
From Denmark/Sweden, 5516/40,163 LDX users and 27,494/200,389 previous users were included. In Denmark, IRs of MACE/1000 person-years (95% CI) were similar for LDX (1.63 [0.85–3.14]) and previous users (1.61 [1.28–2.01]). In Sweden, IRs (95% CI) were 1.40 (1.09–1.79) in LDX users and 1.17 (1.00–1.38) in previous users. Adjusted MACE IRRs (95% CI) for LDX versus previous use were 1.01 (0.48–2.13) in Denmark, 1.13 (0.75–1.71) in Sweden, and 1.10 (0.77–1.58) in the pooled analysis.
Conclusion
Our findings suggest little to no increased risk of cardiovascular and cerebrovascular events in patients treated with LDX compared with patients previously treated with other ADHD medications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Stimulants used in the treatment of attention-deficit/hyperactivity disorder (ADHD) in adults may be associated with elevation of blood pressure and heart rate, which have the potential to increase risks of serious cardiovascular and cerebrovascular events. |
What did the study ask? |
In this study, we estimated the risk of cardiovascular and cerebrovascular events in patients treated with the ADHD medication lisdexamfetamine dimesylate (LDX) compared with patients previously treated with other ADHD medications. |
What were the study outcomes/conclusions? |
The adjusted incidence rate ratios (IRRs) (95% confidence intervals [CIs]) of major adverse cardiovascular and cerebrovascular events (MACE) for LDX users versus previous users of other ADHD medications were 1.01 (0.48–2.13) in Denmark and 1.13 (0.75–1.71) in Sweden. |
The pooled estimate of 1.10 (0.77–1.58) indicated little to no increased risk of MACE in patients treated with LDX compared with patients previously treated with other ADHD medications. |
Introduction
Attention-deficit/hyperactivity disorder (ADHD) affects about 3% of adults worldwide [1] and is commonly treated with stimulant medication, such as methylphenidate or amphetamines, or with the non-stimulant atomoxetine. European treatment guidelines for adult ADHD recommend exercising caution in prescribing stimulants to individuals with known cardiac defects, given small increases in the risks of myocardial infarction (MI), sudden cardiac death (SCD) or ventricular arrhythmias with these medications [2]. Evidence from clinical trials indicates that stimulants used in ADHD treatment may be associated with elevation of blood pressure and heart rate in adults [3, 4]. While these treatment effects in turn may increase risks of serious cardiovascular and cerebrovascular events, those events are rare and typically not detectable in clinical trials, which rarely evaluate long-term adverse events [5].
The effects of ADHD medications on blood pressure and heart rate have also been reported in observational studies [6, 7]. These studies evaluated the association between atomoxetine, methylphenidate or amphetamines and the risk of serious cardiovascular and cerebrovascular events and have reported mixed findings [8,9,10,11,12,13]. An increased risk of transient ischaemic attack among patients treated with atomoxetine or stimulant medication was reported in a US study [10]; in another US study, an increased risk of sudden death or ventricular arrhythmia among patients treated with methylphenidate was reported [11]. Other studies reported no association between ADHD medication use and adverse cardiovascular and cerebrovascular outcomes [9, 10, 14]. Neither is there evidence from meta-analyses for an association between ADHD medications and an increased risk of all-cause death or serious cardiovascular and cerebrovascular events, such as cerebrovascular accident, MI, significant electrocardiogram changes or SCD/arrhythmia [7, 12].
Lisdexamfetamine dimesylate (LDX) is a therapeutically inactive amphetamine prodrug, indicated as part of a comprehensive treatment programme for ADHD in adult patients, including as a first-line pharmacotherapy. The safety profile of LDX is similar to that of other stimulants [15]. Cardiovascular adverse events observed in placebo-controlled clinical trials among adults treated with LDX 30 mg, 50 mg or 70 mg include increased heart rate (in 5–8% of LDX-treated patients and 0–2.5% of patients receiving placebo), increased systolic blood pressure (less than 1% to 3% of LDX-treated patients and 0 patients receiving placebo) or diastolic blood pressure (2–6% of LDX-treated patients and 0–3% of patients receiving placebo), and increased QT interval corrected by Fridericia’s formula (QTcF interval) (6–12% of LDX-treated patients and 5% of patients receiving placebo) [15,16,17]. LDX was initially approved in Europe in 2012 for the treatment of ADHD in children aged 6 years and older with insufficient response to previous methylphenidate treatment. Subsequently, LDX was approved, in 2015, for the treatment of ADHD in adults in several European countries, including Denmark and Sweden [18]; LDX is also approved for the treatment of ADHD in adults and children aged 6 years and older in the USA [19]. Under a European postmarketing regulatory commitment, a population-based cohort study has been conducted to examine the long-term cardiovascular and cerebrovascular safety of LDX in adults. The present study is the first to have evaluated the association between the use of LDX in routine clinical practice and risk of major adverse cardiovascular and cerebrovascular events (MACE).
The objective of this study was to estimate the risk of cardiovascular and cerebrovascular events in patients treated with LDX compared with patients previously treated with other ADHD medications (i.e. patients whose ADHD medication use ended 181 days to 24 months before initiation of the study).
Methods
Study Design and Setting
The study was conducted in Denmark and Sweden using national medical and administrative registries that capture patient-level prescription and health outcomes data: the Danish National Registers (study period from March 2013 to December 2017) and the Swedish National Registers (study period from September 2013 to December 2018). Both data sources have been used extensively in pharmacoepidemiologic studies [20] and were used with the permission of the responsible data holders. The study was registered in the European Union electronic register of postauthorisation studies in October 2017 (EU PAS Register Number EUPAS20546). The study was reviewed on ethical grounds and approved by the Swedish Ethical Committee, and was deemed exempt from review by the Danish Data Protection Agency and the RTI International Institutional Review Board.
In Denmark, all residents have access to a universal healthcare system that covers visits to general practitioners and specialists, hospital admissions, outpatient visits and partial reimbursement of most medications used outside the hospital setting [21]. The Danish Civil Registration System is a total population register that assigns an identifier to all Danish residents, enabling data linkage across all Danish registers [22]. The following Danish registers were used: the Danish Civil Registration System, the Danish National Patient Registry, the Danish Psychiatric Central Research Register, the Danish National Prescription Registry and the Danish Register of Causes of Death [20]. Data were accessed, managed and analysed on the servers of Statistics Denmark [23].
In Sweden, citizens have unrestricted access to health services, including visits to general practitioners and specialists, hospital admissions, outpatient visits, and partial or complete reimbursement of purchased medicines [20]. A centralised civil registration system allows for personal identification of each person in the entire population and for the possibility of linkage to all national registers. The following Swedish registers were used: the Swedish Register of the Total Population, the Swedish National Patient Register, the Swedish Prescribed Drug Register, the Swedish Cause of Death Register and the Swedish Cancer Register [20].
Study Population
The eligibility criteria for study inclusion were age at least 18 years at the index date and at least 12 months of data available before the index date. The study included two cohorts identified from all eligible individuals in the study data sources: the LDX cohort and the cohort of previous users of other ADHD medications. The LDX cohort included adult patients initiating LDX during the study period, and the date of the first-ever LDX prescription was the index date. The previous-users cohort, randomly sampled and matched with LDX users by age at index date, sex, region and calendar year of index date in a ratio of up to 5:1 (previous users to LDX users), included patients who had at least one medication indicated for ADHD (amphetamine, dexamphetamine, methylphenidate or atomoxetine) dispensed 6–24 months before the index date and who had not had dispensing for a medication indicated for ADHD within the 180 days before the index date. The index date of patients in the previous-users cohort was set as the index date of their matched LDX user. Patients could enter the previous-users cohort more than once if they fulfilled the inclusion criteria and were matched to more than one LDX user, and thus these individuals have more than one index date. However, LDX users were not allowed to enter the previous-users cohort at any time after they were included in the LDX cohort. By selecting patients with relatively recent use of ADHD drugs, we expected to have an adult patient population with ADHD that was more similar to the LDX cohort than if we had selected persons from the general population or never users or past users of ADHD medications with an ADHD diagnosis, thus minimising the risk of selection bias and confounding by indication. We also did not select as comparators patients that were currently treated with other ADHD drugs, since most are also amphetamines or other stimulants such as methylphenidate that would have the same suspected cardiovascular effects. Follow-up in both cohorts started at the index date and ended at the first occurrence of a MACE event, emigration or last available date in the administrative data (the Danish Civil Registration System and the Swedish Register of the Total Population), end of study (December 2017 in Denmark and December 2018 in Sweden) or death.
Variables
Exposure
Current use of LDX was considered the sum of all episodes (i.e. continuous dispensings) of current LDX use (Fig. 1). Post-LDX use was the sum of all time intervals starting after the end of an episode of current LDX use and ending at the earliest of the end of follow-up or the start of another episode of LDX use.

LDX use time periods. ADHD attention-deficit/hyperactivity disorder, LDX lisdexamfetamine dimesylate
Outcomes
The primary study outcome was MACE, a composite cardiovascular and cerebrovascular outcome defined as a first hospitalisation for acute MI or stroke, or an out-of-hospital death due to coronary heart disease or cerebrovascular disease, during the follow-up period.
The secondary outcomes were (1) an extended MACE (EMACE) outcome, comprising all MACE components and additionally hospitalisation for either unstable angina or transient ischaemic attack, (2) the composite coronary components of EMACE (hospitalisation for acute MI or unstable angina or out-of-hospital death due to coronary heart disease), (3) the composite cerebrovascular components of EMACE (hospitalisation for stroke or transient ischaemic attack or out-of-hospital death due to cerebrovascular disease) and (4) a composite outcome consisting of SCD and serious ventricular arrhythmia (SVA), including ventricular tachycardia, ventricular flutter and ventricular fibrillation.
Potential Confounders
Potential demographic confounders identified in the data sources included calendar year of index date, sex, age and highest completed education. Additional potential confounders identified using proxies (diagnostic codes and/or medication codes) included obesity, smoking and alcohol use. Measured potential clinical confounders, identified through inpatient and outpatient hospital diagnoses and dispensed medications, included comorbidities (cardiovascular or cerebrovascular diseases, diabetes or hyperlipidaemia, malignancy, kidney disease, liver disease, chronic obstructive pulmonary disease and psychiatric disorders including ADHD) any time before or on the index date, pharmacy-dispensed comedications (within 6 months before or at the index date for the cardiovascular medications, and ever before the index date for psychiatric medications) and ADHD-related history.
Statistical Analyses
We estimated crude and adjusted incidence rates (IRs) and crude and adjusted IR ratios (IRRs) with the corresponding 95% confidence intervals (CIs) for the comparison of the LDX cohort with the previous-users cohort. Crude and adjusted IRs, IRRs and 95% CIs were estimated using Poisson regression with robust estimation of the variance (since previous users could be matched to several LDX patients). We used the natural logarithm of the time at risk as the offset parameter.
Propensity score stratification was used for confounding adjustment. Using separate logistic regression models for the Danish and Swedish study populations, a propensity score including all potential confounders was estimated as the probability that a patient was a member of the LDX cohort, as opposed to being a member of the previous-users cohort. Patients in both cohorts with a propensity score below the first percentile of the LDX cohort distribution or above the 99th percentile of the previous-users cohort distribution were trimmed. We used propensity score quintiles of the LDX users to divide study cohorts into five non-overlapping strata. Distribution of the baseline characteristics within each propensity score stratum after trimming was considered balanced if the standardised mean difference was less than 0.2 [24, 25]. We included the propensity score quintiles as a covariable in the Poisson regression models [24]. All analyses were conducted separately for Denmark and Sweden. Pooled estimates of IRs and IRRs were obtained using random-effects meta-analysis with a restricted maximum-likelihood estimator [26].
In an exploratory analysis, we stratified IRRs by age, sex, history of cardiovascular disease, diagnosis of ADHD, and history of psychiatric disorder, and separately evaluated the impacts of long-term use of LDX (for at least 12 months) and concomitant use of LDX with other ADHD medications. We evaluated the robustness of the main results in a series of sensitivity analyses including the application of the same inclusion criteria to the LDX cohort and the previous-users cohort; investigating the effect of prior ADHD medication within 180 days before the index date; extending the carryover period to a full duration of prior dispensing; investigating MACE risk for post-LDX use (i.e. during the time at risk after current LDX use ended); using an intention-to-treat analysis; and evaluating the strength of unmeasured confounding in a quantitative bias analysis.
Results
Baseline Characteristics and Patterns of LDX Use During Follow-up
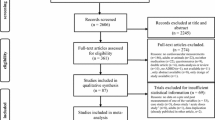
After matching and propensity score trimming, 5516 and 40,163 LDX users were included in the study in Denmark and Sweden, respectively (Fig. 2). These LDX users were matched to 27,494 patients/index dates (16,697 unique patients) in the previous-users cohort in Denmark and to 200,389 patients/index dates (44,516 unique patients) in the previous-users cohort in Sweden.

Cohort attrition. a Denmark. b Sweden. ADHD attention-deficit/hyperactivity disorder, LDX lisdexamfetamine dimesylate. aADHD drugs included in the study were amphetamine, dexamphetamine, methylphenidate and atomoxetine. bEligible patients had at least one dispensing ending 181 days through 24 months before the index date and had no other prescription of ADHD medications within (at least) the 180 days before the index date. cExclusion criteria are applied independently. dPatients in the previous-users cohort were counted as many times as index dates matched. Each previous user could have been matched to multiple LDX users
Approximately 50% of patients in each cohort were aged 18–29 years, and nearly 50% were female (Table 1). Nearly all patients in the LDX cohort and all patients in the previous-users cohort had a prior ADHD diagnosis or dispensing of ADHD medications (Table 2). The prevalence of psychiatric comorbidities was high in both LDX and previous users (Table 1). In both countries, the most prevalent psychiatric comorbidities were mood disorders and anxiety disorders, and these together with eating disorders were slightly more prevalent in LDX users than in previous users. Substance use disorders and psychotic disorders both were more prevalent in previous users than in LDX users. In both countries, the utilisation of comedications was higher in LDX users than in previous users. The history of any cardiovascular comorbidity was similar between LDX users and previous users in both countries and did not exceed 11%.
Median (Q1–Q3) time since first diagnosis of ADHD for LDX users was 2.2 (0.7–5.5) years in Denmark and 2.6 (0.7–5.7) years in Sweden. In Denmark, median (Q1–Q3) duration of time at risk was 1.9 (0.9–3.1) person-years for LDX users and 1.5 (0.6–2.7) person-years for previous users. In Sweden, median (Q1–Q3) duration of time at risk was 0.7 (0.2–1.7) and 0.6 (0.2–0.9) person-years for LDX users and previous users, respectively. Median (Q1–Q3) duration of current LDX use during follow-up was 0.5 (0.2–1.5) years in Denmark and 0.7 (0.2–1.7) years in Sweden (Table 2). Utilisation of LDX in Denmark and Sweden was comparable; the duration of current LDX use was shorter than 6 months for approximately 50% of Danish patients and 40% of Swedish patients and longer than 12 months for approximately 35% of Danish patients and 40% of Swedish patients. Nearly all LDX users had used methylphenidate before the first LDX dispensing (92.5% in Denmark and 86.2% in Sweden); a majority of LDX users received at least six LDX prescriptions (52.1% in Denmark and 58.1% in Sweden).
Incidence Rates and Incidence Rate Ratios
Primary Outcome: MACE
Crude and adjusted IRs for MACE are presented in Table 3. After propensity score adjustment, the IRs (95% CI) of MACE among current users of LDX were 1.62 (0.84–3.11) and 2.08 (1.62–2.66) per 1000 person-years in Denmark and Sweden, respectively. Among previous users of other ADHD medications, the adjusted IRs (95% CI) of MACE were 1.60 (1.27–2.03) and 1.84 (1.56–2.17) per 1000 person-years in Denmark and Sweden, respectively.
The adjusted IRRs (95% CI) of MACE for current LDX users versus previous users were 1.01 (0.48–2.13) in Denmark and 1.13 (0.75–1.71) in Sweden (Fig. 3). The pooled adjusted IRR (95% CI) for MACE for current LDX users versus previous users was 1.10 (0.77–1.58).

Adjusted incidence rate ratios for LDX users compared with previous users, trimmed population: primary analysis, primary and secondary outcomes. CI confidence interval, EMACE extended major adverse cardiovascular and cerebrovascular events, IRR incidence rate ratio, LDX lisdexamfetamine dimesylate, MACE major adverse cardiovascular and cerebrovascular events, SCD sudden cardiac death, SVA serious ventricular arrhythmia. IRRs are per 1000 person-years
Secondary Outcomes
Crude and adjusted IRs for the secondary outcomes are presented in Table 4. For both LDX users and previous users, adjusted IRs were approximately 2 for EMACE, approximately 1 for coronary heart disease and cerebrovascular disease, and approximately 0.5 for hospitalisation for SCD and SVA.
For EMACE, the adjusted IRRs (95% CI) for LDX users versus previous users were 0.92 (0.45–1.88) in Denmark and 0.98 (0.68–1.41) in Sweden. The adjusted IRRs (95% CI) for coronary heart disease were 1.11 (0.41–2.98) in Denmark and 1.37 (0.75–2.47) in Sweden, whereas the IRRs (95% CI) for cerebrovascular disease were 0.90 (0.35–2.30) in Denmark and 0.74 (0.46–1.19) in Sweden (Fig. 3). The IRRs for hospitalisation for SCD and SVA were below 1 in both countries.
Exploratory and Sensitivity Analyses
Incidence rate ratios for MACE investigated by age, sex and long-term use of LDX were similar to those obtained in the main analyses but were imprecise because of a low number of events (Fig. 4a; Table S1, Online Resource 1). Among patients with no history of cardiovascular disease, we found an increased, although imprecise, risk of MACE in LDX users compared with previous users (pooled adjusted IRR, 1.53; 95% CI 0.97–2.40) (Fig. 4a; Table S1). Although patients aged 50 years or older had a higher incidence of MACE than younger patients, when comparing within patients of the same age group (Table S1), the incidence rate ratio was not higher for the subgroup aged 50 years or older than for younger age groups (Fig. 4a). Overall, results from the sensitivity analyses were similar to those obtained in the main analysis (Fig. 4b; Table S2, Online Resource 1). Regarding the impact of unmeasured confounding, we observed that only an extreme unmeasured confounder that is strongly associated with MACE and much more prevalent among LDX users would meaningfully change the IRR estimates (see Online Resource 1).

Adjusted incidence rate ratios for LDX users compared with previous users, trimmed population: exploratory and sensitivity analyses. a Exploratory analyses. b Sensitivity analyses. ADHD attention-deficit/hyperactivity disorder, CI confidence interval, IRR incidence rate ratio, LDX lisdexamfetamine dimesylate, MACE major adverse cardiovascular and cerebrovascular events
Discussion
The clinical importance of this cohort study among adult new users of LDX and remote users of other ADHD medications is supported by the data. Long-term use of LDX in this study was fairly prevalent, with 35–40% of patients in the LDX cohort having current LDX use of longer than 12 months. We observed little to no increased risk of MACE among patients treated with LDX compared with patients previously treated with other ADHD medications (i.e. amphetamine, dexamphetamine, methylphenidate or atomoxetine). The adjusted IR of MACE in LDX users was 1.62 and 2.08 per 1000 persons-years in Denmark and Sweden, respectively. A weak association between the use of LDX and the risk of MACE, compared with previous users of other ADHD medications who were no longer treated with these medications, was observed, with adjusted IRRs (95% CI) of 1.01 (0.48–2.13) in Denmark, 1.13 (0.75–1.71) in Sweden and 1.10 (0.77–1.58) for the pooled population. No clinically meaningful association among LDX users compared with previous users was observed for any of the secondary outcomes. Results were generally consistent in exploratory and sensitivity analyses.
The prevalence of cardiovascular disease in adults with ADHD, regardless of whether and how they have been treated, has not been extensively researched [27]. Furthermore, evidence from previous evaluations of the cardiovascular and cerebrovascular risks associated with ADHD medications, mostly amphetamines (other than LDX) and methylphenidate, has been inconclusive and somewhat limited by potential unmeasured confounding and selection bias [9,10,11, 14]. The results of this study are in accordance with several studies investigating other cardiovascular and cerebrovascular outcomes among patients treated with stimulants indicated for ADHD. The IRs for MACE observed among current LDX users in our study (1.62 and 2.08 per 1000 person-years in Denmark and Sweden, respectively) are similar to IRs reported in two studies conducted in the USA. In a study conducted among US adults (aged 18 years or older) using claims data between 1999 and 2006, Schelleman et al. [9] reported that the IR for a composite score of stroke and MI among new users of amphetamine was 2.62 per 1000 person-years, while the IR for age- and sex-matched non-users of ADHD medications was 3.03. The resulting adjusted hazard ratio (HR) was 0.78 (95% CI 0.51–1.19), and the authors concluded that no increased risk of serious cardiovascular events was observed in patients initiating treatment with amphetamines compared with patients not initiating an ADHD medication. In a study including more than 440,000 adults from four US study populations (1986–2005), Habel et al. [14] reported rates of serious cardiovascular and cerebrovascular events (including MI, SCD or stroke) of 1.88 per 1000 person-years among current users of amphetamines (other than LDX), 2.51 per 1000 person-years among current users of methylphenidate and 3.60 per 1000 person-years among previous users (patients with more than 364 days since the end of the last days’ supply). The authors of the latter study concluded that current or new use of ADHD medications was not associated with an increased risk of serious cardiovascular events: the adjusted risk ratios for serious cardiovascular and cerebrovascular events were 1.03 (95% CI 0.86–1.24) when comparing current users of methylphenidate, amphetamine or atomoxetine with previous users and 0.83 (95% CI 0.72–0.96) when comparing current users with non-users (i.e. a general population of the same age and sex with no current and no previous use).
Another US study by Holick et al. [10] showed an increased risk (HR 3.44; 95% CI 1.13–10.60) of transient ischaemic attack but not of cerebrovascular accident (HR 0.71; 95% CI 0.34–1.47) among patients treated with atomoxetine or ADHD stimulant medication compared with the general population. However, in this secondary analysis, the authors used an intention-to-treat approach and did not match the cohorts by propensity score as they did in their primary analysis, where they found no association [10]. Another study by Schelleman et al. [11] found an increased risk of sudden death or ventricular arrhythmia (adjusted HR 1.84; 95% CI 1.33–2.55) and all-cause death (adjusted HR 1.74; 95% CI 1.60–1.89) when comparing methylphenidate users with the general population. A more recent meta-analysis including three trials conducted in adults concluded that no difference was detected in the number of adverse cardiac events (including cerebrovascular accidents, MI, SCD and significant electrocardiogram changes) between the participants treated with methylphenidate and those treated with placebo [12]. Another recent meta-analysis evaluating use of methylphenidate both in adults and in children and adolescents (which included the studies by Habel et al. [14] and Schelleman et al. [11]) also demonstrated no increased risk of stroke or MI [7]. Another study investigated new-onset heart failure or cardiomyopathy among initiators of lisdexamfetamine, methylphenidate and atomoxetine [13]. The event rates (per 1000 person-years) of heart failure/cardiomyopathy by age categories among patients treated with amphetamines during the first 90 days of use were 1.61 (less than 22 years), 2.42 (22–44 years), 9.22 (45–64 years) and 47.11 (65 years or older). Longer duration of amphetamine use was not associated with an increased rate of cardiovascular or cerebrovascular events. Outcome rates were slightly higher for all age groups of at least 22 years for 90 days’ use of methylphenidate products than for 90 days’ use of amphetamine products [13]. Finally, a study of patients treated with methylphenidate who had had an MI in South Korea, Taiwan and Hong Kong isolated MI risk by time period—before, during and after methylphenidate exposure—relative to a baseline period of non-exposure [28]. The highest risk of MI occurred during the pre-exposure period, suggesting that there is not a causal relationship between methylphenidate and MI [28].
Some limitations of this study are acknowledged. By design, different inclusion criteria were applied to LDX users and previous users, who required a “washout” period of at least 180 days from the end of the previous use of any of the other ADHD medications (amphetamine, dexamphetamine, methylphenidate or atomoxetine), potentially leading to immortal-time bias. Nonetheless, in the analysis evaluating previous exposure, in which patients in the LDX cohort were subject to the same washout period as was applied for previous users, the results remained consistent with the primary findings, suggesting that immortal-time bias may be minimal. Further, some patients may not have taken the dispensed LDX as prescribed, and the exact dosing regimen of prescribed medication was unavailable in this study. Nevertheless, data on redeemed prescriptions is considered to more closely reflect actual use by patients than prescription data. We assumed the use of one LDX capsule per day regardless of the strength and therefore may have overestimated the duration of LDX use. While evaluation of duration of use was focused on long-term use, and short-term use (e.g. less than 3 or 6 months) was not evaluated, we do not anticipate that an increased risk of MACE for LDX would have been detected with short-term use. Because the IRR estimate for MACE was 1.10 (95% CI 0.77–1.58) in the overall analysis including short-term and long-term users and was 1.59 (0.86–2.95) in the analysis of long-term use, the IRR point estimate for short-term use (less than 6 months), in theory, would have been lower than 1.10. The precision of the IRRs for several subgroup analyses was low since they were based on a low number of events; in particular, the number of events in the subgroups aged 18–29 and 30–39 were small, and thus risk estimates were imprecise (i.e. had wide 95% CIs) and should be interpreted with caution. It also was not possible to support an exploratory analysis for users aged 65 years or older because of an insufficient number of users within those age groups. An additional limitation is possible unmeasured confounding, though a quantitative bias analysis showed that the main results were robust to unmeasured confounding, except in extreme scenarios, where an unmeasured confounder was strongly associated with MACE and much more prevalent in LDX users than in previous users of other ADHD medications. Finally, although the inclusion of a comparator group of previous users of other ADHD medications reduced the potential for selection bias or confounding due to a healthy-user effect among patients from the general population or with chronically treated ADHD [14], it cannot be discounted that patients in the previous-users cohort were those for whom the ADHD treatment did not work or who may have had fewer symptoms, leading to confounding by indication by the comparison of untreated versus treated patients. However, the risk was considered minimal because the baseline characteristics of both cohorts were balanced using matching and propensity scores.
Conclusion
To our knowledge, this is the first population-based observational study using routinely collected administrative data from clinical practice to investigate the cardiovascular and cerebrovascular risk associated with exposure to LDX. Results of the current study suggest that there is little to no increased risk of cardiovascular and cerebrovascular events among patients treated with LDX compared with patients previously treated with other ADHD medications.
References
Fayyad J, Sampson NA, Hwang I, et al. The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. Atten Defic Hyperact Disord. 2017;9(1):47–65.
Kooij JJS, Bijlenga D, Salerno L, et al. Updated European Consensus Statement on diagnosis and treatment of adult ADHD. Eur Psychiatry. 2019;56:14–34.
Mick E, McManus DD, Goldberg RJ. Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur Neuropsychopharmacol. 2013;23(6):534–41.
Cortese S, Adamo N, Del Giovane C, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry. 2018;5(9):727–38.
Elliott J, Johnston A, Husereau D, et al. Pharmacologic treatment of attention deficit hyperactivity disorder in adults: a systematic review and network meta-analysis. PLoS ONE. 2020;15(10):e0240584.
Martinez-Raga J, Knecht C, Szerman N, Martinez MI. Risk of serious cardiovascular problems with medications for attention-deficit hyperactivity disorder. CNS Drugs. 2013;27(1):15–30.
Liu H, Feng W, Zhang D. Association of ADHD medications with the risk of cardiovascular diseases: a meta-analysis. Eur Child Adolesc Psychiatry. 2019;28(10):1283–93.
Westover AN, Halm EA. Do prescription stimulants increase the risk of adverse cardiovascular events? A systematic review. BMC Cardiovasc Disord. 2012;12:41.
Schelleman H, Bilker WB, Kimmel SE, et al. Amphetamines, atomoxetine and the risk of serious cardiovascular events in adults. PLoS ONE. 2013;8(1):e52991.
Holick CN, Turnbull BR, Jones ME, Chaudhry S, Bangs ME, Seeger JD. Atomoxetine and cerebrovascular outcomes in adults. J Clin Psychopharmacol. 2009;29(5):453–60.
Schelleman H, Bilker WB, Kimmel SE, et al. Methylphenidate and risk of serious cardiovascular events in adults. Am J Psychiatry. 2012;169(2):178–85.
Liang EF, Lim SZ, Tam WW, et al. The effect of methylphenidate and atomoxetine on heart rate and systolic blood pressure in young people and adults with attention-deficit hyperactivity disorder (ADHD): systematic review, meta-analysis, and meta-regression. Int J Environ Res Public Health. 2018;15(8):1789.
Mosholder AD, Taylor L, Mannheim G, Ortendahl L, Woodworth TS, Toh S. Incidence of heart failure and cardiomyopathy following initiation of medications for attention-deficit/hyperactivity disorder: a descriptive study. J Clin Psychopharmacol. 2018;38(5):505–8.
Habel LA, Cooper WO, Sox CM, et al. ADHD medications and risk of serious cardiovascular events in young and middle-aged adults. JAMA. 2011;306(24):2673–83.
Coghill DR, Caballero B, Sorooshian S, Civil R. A systematic review of the safety of lisdexamfetamine dimesylate. CNS Drugs. 2014;28(6):497–511.
Adler LA, Goodman DW, Kollins SH, et al. Double-blind, placebo-controlled study of the efficacy and safety of lisdexamfetamine dimesylate in adults with attention-deficit/hyperactivity disorder. J Clin Psychiatry. 2008;69(9):1364–73.
Adler LA, Dirks B, Deas PF, et al. Lisdexamfetamine dimesylate in adults with attention-deficit/ hyperactivity disorder who report clinically significant impairment in executive function: results from a randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2013;74(7):694–702.
MHRA. Public assessment report, decentralised procedure: Elvanse 30 mg, 50 mg and 70 mg capsules, hard (lisdexamfetamine dimesylate). February 2015. https://s3-us-west-2.amazonaws.com/drugbank/cite_this/attachments/files/000/002/365/original/con261790.pdf?1545166171. Accessed 28 Sept 2021.
FDA. Vyvanse (lisdexamfetamine dimesylate) prescribing information. January 2022. http://pi.shirecontent.com/PI/PDFs/Vyvanse_USA_ENG.pdf. Accessed 11 Apr 2022.
Laugesen K, Ludvigsson JF, Schmidt M, et al. Nordic Health Registry-based research: a review of health care systems and key registries. Clin Epidemiol. 2021;13:533–54.
Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–91.
Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–9.
Statistics Denmark. https://www.dst.dk/en/. Accessed 27 Aug 2021.
Nguyen TL, Collins GS, Spence J, et al. Double-adjustment in propensity score matching analysis: choosing a threshold for considering residual imbalance. BMC Med Res Methodol. 2017;17(1):78.
McCaffrey DF, Griffin BA, Almirall D, Slaughter ME, Ramchand R, Burgette LF. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat Med. 2013;32(19):3388–414.
Viechtbauer W. Bias and efficiency of meta-analytic variance estimators in the random-effects model. J Educ Behav Stat. 2005;30(3):261–93.
Kittel-Schneider S, Arteaga-Henriquez G, Vasquez AA, et al. Non-mental diseases associated with ADHD across the lifespan: Fidgety Philipp and Pippi Longstocking at risk of multimorbidity? Neurosci Biobehav Rev. 2022;132:1157–80.
Jeong HE, Lee H, Lai EC, et al. Association between methylphenidate and risk of myocardial infarction: a multinational self-controlled case series study. Pharmacoepidemiol Drug Saf. 2021;30(10):1458–67.
Acknowledgements
Funding
This study and the Rapid Service Fee associated with this article were funded by Shire Pharmaceuticals, now part of the Takeda group of companies.
Medical Writing, Editorial, and Other Assistance
Kate Lothman of RTI Health Solutions provided medical writing services, John Forbes of RTI Health Solutions provided editorial services, and Ryan Miller of RTI Health Solutions provided graphic design services in the preparation of this article. These services were funded by Takeda Pharmaceuticals.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Prior Presentation
A portion of this work was presented as a poster by Forns J, Dudukina E, Hagg D, Szentkúti EP, Gembert K, Plana E, Gilsenan A, Horváth-Puhó E, Reutfors J, Rebordosa C. Cohort study of the incidence of major cardiovascular events in new adult users of lisdexamfetamine and remote adult users of other attention-deficit/hyperactivity disorder treatments. Presented at the 2021 8th World Congress on ADHD Virtual Event; May 6, 2021.
Disclosures
This study was conducted under a research contract between Shire Pharmaceuticals, now part of the Takeda group of companies, and RTI Health Solutions and was funded by Shire Pharmaceuticals. Joan Forns, Estel Plana, Alicia Gilsenan, and Cristina Rebordosa are employees of RTI Health Solutions. Elena Dudukina, Péter Szentkúti, Erzsébet Horváth-Puhó and Vera Ehrenstein are employees of Aarhus University and participated in this study under an institutional research agreement between RTI Health Solutions and Aarhus University. David Hägg, Karin Gembert, and Johan Reutfors are employees at the Centre for Pharmacoepidemiology at the Karolinska Institutet, which receives grants from several entities (pharmaceutical companies, regulatory authorities, contract research organisations) for performance of drug safety and drug utilisation studies.
Compliance With Ethics Guidelines
The study complied with the ethical requirements of all relevant authorities for the participating organizations. The data sources were used with the permission of the responsible data holders. This study was reviewed on ethical grounds and approved by the Swedish Ethical Committee (approval no. 2018/1935-31). The study was deemed exempt from review by the Danish Data Protection Agency, consistent with the standards for studies based exclusively on routinely collected data, and was registered in the Aarhus University roster of studies. The study was reviewed by the RTI International Institutional Review Board, was determined not to constitute research with human subjects, and was deemed exempt (study no. 03000020450). Because the study involved only de-identified and aggregated patient data, informed consent requirements were waived.
Data Availability
The datasets generated and analysed during the current study are not publicly available to comply with data-use agreements.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Forns, J., Dudukina, E., Hägg, D. et al. Risk of Major Cardiovascular and Cerebrovascular Events in Users of Lisdexamfetamine and Other Medications for Attention-Deficit/Hyperactivity Disorder in Denmark and Sweden: A Population-Based Cohort Study. Neurol Ther 11, 1659–1676 (2022). https://doi.org/10.1007/s40120-022-00396-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-022-00396-y