
Abstract
Objectives
To evaluate the incidence of long-term de novo acid reflux–related complications following sleeve gastrectomy (SG) to determine whether routine postoperative surveillance endoscopy is necessary.
Methods
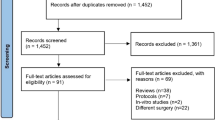
A systematic search of Medline, Embase, CINAHL, CENTRAL, the Web of Science, and bibliographic reference lists was conducted. A proportion meta-analysis model was constructed to quantify the risk of the de novo gastro-oesophageal reflux disease (GORD), oesophagitis, and Barrett’s oesophagus (BE) at least 4 years after SG. Random-effects modelling was applied to calculate pooled outcome data.
Results
Thirty-two observational studies were included reporting a total of 7904 patients who underwent primary SG and were followed up for at least 4 years. The median follow-up period was 60 months (48–132). Preoperative acid-reflux symptoms existed in 19.1% ± 15.1% of the patients. The risk of development of de novo GORD, oesophagitis, and BE after SG was 24.8% (95% CI 18.6–31.0%), 27.9% (95% CI 17.7–38.1%), and 6.7% (95% CI 3.7–9.7%), respectively. The between-study heterogeneity was significant in all outcome syntheses. It was suspected that several of the included studies have not reported BE and oesophagitis because such events might not have happened in their cohorts.
Conclusions
Long-term risk of de novo GORD after SG seems to be comparable with those of the general population which questions the merit of surveillance endoscopy after SG in asymptomatic patients. De novo BE and oesophagitis after SG have not been reported by most of the available studies which may lead to overestimation of the rates of both outcomes in any evidence synthesis. We recommend endoscopic surveillance for symptomatic patients only.



Similar content being viewed by others


References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of outstanding importance
Angrisani L, Santonicola A, Iovino P, Ramos A, Shikora S, Kow L. Bariatric surgery survey 2018: similarities and disparities among the 5 IFSO chapters. Obes Surg. 2021;31(5):1937–48.
Felsenreich DM, Bichler C, Langer FB, Gachabayov M, Prager G. Sleeve gastrectomy: surgical technique, outcomes, and complications. Surg Technol Int. 2020;36:63–9.
Quero G, Fiorillo C, Dallemagne B, Mascagni P, Curcic J, Fox M, et al. The causes of gastroesophageal reflux after laparoscopic sleeve gastrectomy: quantitative assessment of the structure and function of the esophagogastric junction by magnetic resonance imaging and high-resolution manometry. Obes Surg. 2020;30(6):2108–17.
Greilsamer T, de Montrichard M, Bruley des Varannes S, Jacobi D, Guillouche M, Regenet N, et al. Hypotonic low esophageal sphincter is not predictive of gastroesophageal reflux disease after sleeve gastrectomy. Obes Surg 2020;30(4):1468–72.
Salman MA, Mikhail HMS, Abdelsalam A, Abdallah A, Elshafey HE, Abouelregal TE, et al. Acceleration of gastric emptying and improvement of GERD outcome after laparoscopic sleeve gastrectomy in non-diabetic obese patients. Obes Surg. 2020;30(7):2676–83.
Tolone S, Savarino E, De Bortoli N, Docimo L. Sleeve gastrectomy, GERD, and Barrett’s esophagus: it is time for objective testing. Obes Surg. 2019;29(7):2312–3. https://doi.org/10.1007/s11695-019-03902-8.
Soricelli E, Casella G, Baglio G, et al. Lack of correlation between gastroesophageal reflux disease symptoms and esophageal lesions after sleeve gastrectomy. Surg Obes Relat Dis. 2018;14(6):751–6. https://doi.org/10.1016/j.soard.2018.02.008.
Sebastianelli L, Benois M, Vanbiervliet G, Bailly L, Robert M, Turrin N, Gizard E, Foletto M, Bisello M, Albanese A, Santonicola A, Iovino P, Piche T, Angrisani L, Turchi L, Schiavo L, Iannelli A. Systematic endoscopy 5 years after sleeve gastrectomy results in a high rate of Barrett’s esophagus: results of a multicenter study. Obes Surg. 2019;29(5):1462–9.
Felsenreich DM, Ladinig LM, Beckerhinn P, Sperker C, Schwameis K, Krebs M, Jedamzik J, Eilenberg M, Bichler C, Prager G, Langer FB. Update: 10 years of sleeve gastrectomy-the first 103 patients. Obes Surg. 2018;28(11):3586–94. https://doi.org/10.1007/s11695-018-3399-1.
Fisher OM, Chan DL, Talbot ML, Ramos A, Bashir A, Herrera MF, Himpens J, Shikora S, Higa KD, Kow L, Brown WA. Barrett’s oesophagus and bariatric/metabolic surgery-IFSO 2020 position statement. Obes Surg. 2021;31(3):915–34. https://doi.org/10.1007/s11695-020-05143-6.
Mahawar KK, Omar I, Singhal R, Aggarwal S, Allouch MI, Alsabah SK, et al. The first modified Delphi consensus statement on sleeve gastrectomy. Surg Endosc. 2021;35(12):7027–33. https://doi.org/10.1007/s00464-020-08216-w.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;21(339): b2700.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. April 2, 2020
Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Chapter 8: assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane handbook for systematic reviews of interventions version 6.1 (updated September 2020). Cochrane, 2020. Available from https://training.cochrane.org/handbook. (last accessed 20 February 2023).
•• Alvarez R, Youssef J, Zadeh J, et al. Sleeve gastrectomy morphology and long-term weight-loss and gastroesophageal reflux disease outcomes. Surg Endosc. 2023. https://doi.org/10.1007/s00464-022-09555-6. This is the first study assessing the impact of SG morphology on long-term weight loss and GORD. Our data suggest an association between SG morphology and long-term weight loss but not with GORD outcomes.
• Ferrer JV, Acosta A, García-Alementa EM, et al. High rate of de novo esophagitis 5 years after sleeve gastrectomy: a prospective multicenter study in Spain. Surg Obes Relat Dis. 2022;18(4):546–54. Weight regain and a striking increase in gastric capacity are risk factors indicative of esophagitis, even when patients are asymptomatic.
•• Matar R, Maselli D, Vargas E, et al. Esophagitis after bariatric surgery: large cross-sectional assessment of an endoscopic database. Obes Surg. 2020;30(1):161–8. Erosive oesophagitis is more prevalent after SG compared with RYGB in a pre-bariatric surgery cohort with GORD. SG is associated with significant esophageal physiologic changes conducive to GERD and its clinical consequences.
Migaczewski M, Czerwińska A, Rubinkiewicz M, et al. The prevalence of, and risk factors for, Barrett’s oesophagus after sleeve gastrectomy. Wideochir Inne Tech Maloinwazyjne. 2021;16(4):710–4.
Elkassem S. Gastroesophageal reflux disease, esophagitis, and Barrett’s esophagus 3 to 4 years post sleeve gastrectomy. Obes Surg. 2021;31(12):5148–55.
Braghetto I, Korn O. Late esophagogastric anatomic and functional changes after sleeve gastrectomy and its clinical consequences with regards to gastroesophageal reflux disease. Dis Esophagus. 2019;32(6):doz020.
Soricelli E, Casella G, Baglio G, et al. Lack of correlation between gastroesophageal reflux disease symptoms and esophageal lesions after sleeve gastrectomy. Surg Obes Relat Dis. 2018;14:751–6.
Castagneto Gissey L, Casella Mariolo JR, Genco A, et al. 10-year follow-up after laparoscopic sleeve gastrectomy: outcomes in a monocentric series. Surg Obes Relat Dis. 2018;14:1480–7.
Kowalewski PK, Olszewski R, Waledziak MS, et al. Long-term outcomes of laparoscopic sleeve gastrectomy—a single-center, retrospective study. Obes Surg. 2018;28:130–4.
Singla V, Aggarwal S, Garg H, et al. Outcomes in super obese patients undergoing laparoscopic sleeve gastrectomy. J Laparoendosc Adv Surg Tech A. 2018;28:256–62.
Chang DM, Lee WJ, Chen JC, et al. Thirteen-year experience of laparoscopic sleeve gastrectomy: surgical risk, weight loss, and revision procedures. Obes Surg. 2018;28:2991–7.
Chuffart E, Sodji M, Dalmay F, et al. Long-term results after sleeve gastrectomy for gastroesophageal reflux disease: a single-center French study. Obes Surg. 2017;27:2890–7.
Gadiot RP, Biter LU, van Mil S, et al. Long-term results of laparoscopic sleeve gastrectomy for morbid obesity: 5 to 8-year results. Obes Surg. 2017;27:59–63.
Nocca D, Loureiro M, Skalli EM, et al. Five-year results of laparoscopic sleeve gastrectomy for the treatment of severe obesity. Surg Endosc. 2017;31:3251–7.
Flolo TN, Andersen JR, Kolotkin RL, et al. Five-year outcomes after vertical sleeve gastrectomy for severe obesity: a prospective cohort study. Obes Surg. 2017;27:1944–51.
Garg H, Aggarwal S, Misra MC, et al. Mid to long term outcomes of laparoscopic sleeve gastrectomy in Indian population: 3–7 year results—a retrospective cohort study. Int J Surg. 2017;48:201–9.
Barry RG, Amiri FA, Gress TW, et al. Laparoscopic vertical sleeve gastrectomy: a 5-year veterans affairs review. Medicine. 2017;96: e7508.
Arman GA, Himpens J, Dhaenens J, et al. Long-term (11þyears) outcomes in weight, patient satisfaction, comorbidities, and gastroesophageal reflux treatment after laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2016;12:1778–86.
Braghetto I, Csendes A. Prevalence of Barrett’s esophagus in bariatric patients undergoing sleeve gastrectomy. Obes Surg. 2016;26:710–4.
Pok EH, LeeWJ, Ser KH, et al. Laparoscopic sleeve gastrectomy in Asia: long term outcome and revisional surgery. Asian J Surg. 2016;39:21–28.
Angrisani L, Santonicola A, Hasani A, et al. Five-year results of laparoscopic sleeve gastrectomy: effects on gastroesophageal reflux disease symptoms and co-morbidities. Surg Obes Relat Dis. 2016;12:960–8.
Hirth DA, Jones EL, Rothchild KB, et al. Laparoscopic sleeve gastrectomy: long-term weight loss outcomes. Surg Obes Relat Dis. 2015;11:1004–7.
Alexandrou A, Athanasiou A, Michalinos A, et al. Laparoscopic sleeve gastrectomy for morbid obesity: 5-year results. Am J Surg. 2015;209:230–4.
Abd Ellatif ME, Abdallah E, Askar W, et al. Long term predictors of success after laparoscopic sleeve gastrectomy. Int J Surg. 2014;12:504–8.
Rebecchi F, Allaix ME, Giaccone C, et al. Gastroesophageal reflux disease and laparoscopic sleeve gastrectomy: a physiopathologic evaluation. Ann Surg. 2014;260:909–14.
Boza C, Daroch D, Barros D, et al. Long-term outcomes of laparoscopic sleeve gastrectomy as a primary bariatric procedure. Surg Obes Relat Dis. 2014;10:1129–33.
Catheline JM, Fysekidis M, Bachner I, et al. Five-year results of sleeve gastrectomy. J Visc Surg. 2013;150:307–12.
Rawlins L, Rawlins MP, Brown CC, et al. Sleeve gastrectomy: 5-year outcomes of a single institution. Surg Obes Relat Dis. 2013;9:21–5.
Bohdjalian A, Langer FB, Shakeri-Leidenmuhler S, et al. Sleeve gastrectomy as sole and definitive bariatric procedure: 5-year results for weight loss and ghrelin. Obes Surg. 2010;20:535–40.
Himpens J, Dobbeleir J, Peeters G. Long-term results of laparoscopic sleeve gastrectomy for obesity. Ann Surg. 2010;252:319–24.
BMJ Best Practice (2022) Gastro-oesophageal reflux disease. BMJ Publishing Group. https://bestpractice.bmj.com/info/.
Braghetto I, Korn O, Csendes A, Gutiérrez L, Valladares H, et al. Laparoscopic treatment of obese patients with gastroesophageal reflux disease and Barrett’s esophagus: a prospective study. Obes Surg. 2012;22:764–72.
Prachand VN, Alverdy JC. Gastroesophageal reflux disease and severe obesity: fundoplication or bariatric surgery? World J Gastroenterol. 2010;16:3757–61.
Macmillan Cancer Support - https://macmillan.org.uk/cancer-information-and-support/worried-about-cancer/pre-cancerous-and-genetic-conditions/barretts-oesophagus. Accessed Feb 2023.
Yeung KTD, Penney N, Ashrafian L, Darzi A, Ashrafian H. Does sleeve gastrectomy expose the distal esophagus to severe refluX?: a systematic review and meta-analysis. Ann Surg. 2020;271(2):257–65. https://doi.org/10.1097/SLA.0000000000003275.
Kuipers EJ. Barrett esophagus and life expectancy: implications for screening? Gastroenterol Hepatol (N Y). 2011;7(10):689–91.
Kanat BH, Doğan S. Is gastroscopy necessary before bariatric surgery? World J Gastrointest Endosc. 2022;14(1):29–34. https://doi.org/10.4253/wjge.v14.i1.29.
Genco A, Castagneto-Gissey L, Lorenzo M, Ernesti I, Soricelli E, Casella G. Esophageal adenocarcinoma after sleeve gastrectomy: actual or potential threat? Italian series and literature review. Surg Obes Relat Dis. 2021;17(5):848–54.
Wright FG, Duro A, Medici JR, Lenzi S, Beskow AF, Cavadas D. Esophageal adenocarcinoma five years after laparoscopic sleeve gastrectomy. A case report. Int J Surg Case Rep. 2017;32:47–50.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
Considering the design of our study, ethical approval and consent were not required.
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Shahin Hajibandeh and Shahab Hajibandeh equally contributed to this paper, and joint first authorship is proposed
Appendix 1: Included study data and characteristics of the included populations
Appendix 1: Included study data and characteristics of the included populations
Search no | Search strategy* |
|---|---|
#1 | MeSH descriptor: [Barrett’s esophagus] explode all trees |
#2 | Barrett’s oesophagus: TI,AB,KW |
#3 | MeSH descriptor: [Barrett’s oesophagus] explode all trees |
#4 | Barrett’s oesophagus: TI,AB,KW |
#5 | MeSH descriptor: [gastroesophageal reflux disease] explode all trees |
#6 | Gastroesophageal reflux disease: TI,AB,KW |
#7 | MeSH descriptor: [GERD] explode all trees |
#8 | GERD: TI,AB,KW |
#9 | MeSH descriptor: [gastro-oesophageal reflux disease] explode all trees |
#10 | Gastro-oesophageal reflux disease: TI,AB,KW |
#11 | MeSH descriptor: [GORD] explode all trees |
#12 | GORD: TI,AB,KW |
#13 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 |
#14 | MeSH descriptor: [sleeve gastrectomy] explode all trees |
#15 | Sleeve gastrectomy: TI,AB,KW |
#16 | #14 OR #15 |
#17 | #13 AND #16 |
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hajibandeh, S., Hajibandeh, S., Ghassemi, N. et al. Meta-analysis of Long-term De Novo Acid Reflux–Related Outcomes Following Sleeve Gastrectomy: Evidence Against the Need for Routine Postoperative Endoscopic Surveillance. Curr Obes Rep 12, 395–405 (2023). https://doi.org/10.1007/s13679-023-00521-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13679-023-00521-4