
Abstract
Multiple sclerosis (MS) is a chronic inflammatory, autoimmune, and neurodegenerative disease of the central nervous system (CNS), characterized by demyelination and axonal loss. It is induced by attack of autoreactive lymphocytes on the myelin sheath and endogenous remyelination failure, eventually leading to accumulation of neurological disability. Disease-modifying agents can successfully address inflammatory relapses, but have low efficacy in progressive forms of MS, and cannot stop the progressive neurodegenerative process. Thus, the stem cell replacement therapy approach, which aims to overcome CNS cell loss and remyelination failure, is considered a promising alternative treatment. Although the mechanisms behind the beneficial effects of stem cell transplantation are not yet fully understood, neurotrophic support, immunomodulation, and cell replacement appear to play an important role, leading to a multifaceted fight against the pathology of the disease. The present systematic review is focusing on the efficacy of stem cells to migrate at the lesion sites of the CNS and develop functional oligodendrocytes remyelinating axons. While most studies confirm the improvement of neurological deficits after the administration of different stem cell types, many critical issues need to be clarified before they can be efficiently introduced into clinical practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is a chronic autoimmune inflammatory disease of the central nervous system (CNS) primarily associated with demyelination of the neural axons but also leading to axonal degradation and neurodegeneration. As a consequence, neuronal impulses are not adequately transmitted and patients develop neurological symptoms. It is one of the main causes of disability in young adults and its incidence is increasing [1]. The pathogenesis of the disease is complex and has not yet been fully unraveled [2]. It is considered that the onset of the disease long precedes the first clinical symptoms. Existing immunomodulatory agents, despite being very efficient in reducing the rate of relapses, do not prevent progressive neurodegenerative processes, nor do they have any regenerative effect, while they may cause significant adverse effects [3].
A stem cell is an undifferentiated cell that can self-renew and differentiate into tissue-specific cell types. During the lifetime of an organism stem cells are able to act as repair cells, regenerating cells of organs. The behavior and properties of stem cells are regulated by their immediate environment, the niche [4]. Depending on their properties, stem cells can be divided into three main categories: pluripotent stem cells, totipotent stem cells, and multipotent stem cells. Pluripotent stem cells can differentiate into all tissue types except extra-embryonic tissues [5]. This category includes embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs). ESCs are derived from the cells of the inner mass of the blastocyst during early embryogenesis and their differentiation in vitro is an important chapter in regenerative medicine [6]. iPSCs are generated in vitro from a patient’s own fully differentiated somatic cells by the process of cellular reprogramming [5], [7]. Totipotent stem cells include zygotes and blastomeres up to the eight-cell stage and have the ability to differentiate into all cell types needed to create a complete organism [8]. Finally, multipotent stem cells include stem cells of embryonic (fetal stem cells, FSCs) and adult tissues (adult stem cells, ASCs), and can differentiate into limited cell types of the tissue or the organ where they are found [5]. FSCs are mesenchymal-type cells that originate in the tissues of the fetus, can be found in the circulation during the first trimester of pregnancy and differentiate into bone, cartilage, haematopoietic cells, and oligodendrocytes [9]. ASCs are located in the niche of all body tissues, and their main function is to produce specialized cells for repair in case of damage, injury or disease. They include mesenchymal stromal cells (MSCs), hematopoietic stem cells (HSCs), stem cells from muscle tissue, and neural stem cells (NSCs) [10].
Due to their ability to self-renew and differentiate, stem cells have recently been proposed as a promising treatment for various degenerative and autoimmune disorders, including MS [11], [12]. The underlying mechanisms for the beneficial effects of administered stem cells include immunomodulation, transforming the central nervous system microenvironment from hostile to supportive and neurotrophic action, promoting the differentiation and regeneration of endogenous oligodendrocytes [13]. Despite all, their most interesting function is cell replacement, meaning their use as an exogenous source for the production of new oligodendrocytes that could possibly restore the damaged myelin sheaths. This review aims to present and clarify the role of stem cell replacement therapy in MS, to reveal the types of stem cells that perform cell replacement and their optimal route of administration.
Materials and methods
A systematic literature search was conducted to identify eligible primary studies on stem cell replacement therapy in multiple sclerosis. Three medical and scientific databases (Medline, Embase, and Scopus) were searched, using the following search terms: “stem cell”, “cell replacement” and “multiple sclerosis”. No language or other restrictions were applied. The search spanned from inception of each electronic database to January 25th, 2022. Furthermore, the reference lists of published articles were searched manually, to ensure the comprehensiveness of the bibliography.
This effort resulted in 263 citations, from which relevant studies were selected for the review. Their potential relevance was examined and 129 studies were excluded as irrelevant. The full texts of the remaining 134 citations were assessed to select those primary studies that directly related to stem cell replacement therapy in multiple sclerosis. These criteria excluded 54 studies and left 80 in the review.
Hematopoietic stem cells (HSCs)
HSCs constitute approximately 0.01% of the proliferating cells in the bone marrow and they can generate all hematopoietic cell lines, including erythrocytes, megakaryocytes and cells of the immune system [14]. Transplantation of HSCs was the first cell therapy to emerge for the treatment of MS and is currently the only clinically validated approach, having been introduced in the field of hematology, where it is mainly used for the treatment of malignancies [15]. In experiments performed in vivo in rodents, it was found that early treatment has substantial results in improving the clinical picture and prevention of relapses, while in contrast, in chronic stages of experimental allergic encephalomyelitis (EAE) the effect is negligible [16], [17]. The only comprehensive randomized clinical trial is the international autologous trial stem cell transplantation in MS, which compared mitoxantrone versus autologous HSC transplantation and included patients with aggressive relapsing–remitting MS (RRMS) and with secondary progressive MS (SPMS). Although a difference in EDSS scores was not observed, the results showed that autologous HSC was superior in terms of reducing MRI activity and recurrence rate [18]. The neurological disability observed in SPMS is mainly caused by neurodegenerative processes, due to axonal atrophy rather than inflammatory processes. As a result, the progressive phase may be curable by neither immunomodulatory agents nor autologous HSC [19], so there is a need to emphasize cell replacement with HSCs.
Cell replacement with HSCs
Only two study was found to have encouraging results about the cell replacement that HSCs can accomplish in oligodendrocytes (Table 1). In the study of Goolsby et al., 2013, after autologous HSC and injection into the striatum and hippocampus, structural cell replacement was observed. CD34+ stem cells (HSCs) migrated long distances after injection into the shiverer brain, in many cases up to the contralateral hemisphere to the injection site. In some cases, the transplanted CD34+ cells selectively manifested oligodendrocyte MBP, in some cases, neuronal neurofilament H and NeuN, and in others astroglial GFAP. Finally, CD34+ cells from adult mouse bone marrow express classic MBP, extend oligodendroglial-like cell processes and ensheath axons in the brain and optic nerve [20]. Furthermore, in the clinical trial of Harris et al., 2020, HSCs were administered intravenously (IV) resulting in replacement of T cells. More than 90% of the pre-existing cerebrospinal fluid (CSF) repertoire in participants with active RRMS was removed following autologous HSC transplantation and replaced with clonotypes predominantly generated from engrafted autologous stem cells. The result was extensive removal of pre-existing T cell clonotypes in both CSF and CD4 T cells in peripheral blood. In addition, autologous HSCs replaced > 90% of the pre-existing T cell repertoire in CSF with new clones at month 24 after transplant [21].
Mesenchymal stromal cells (MSCs)
Mesenchymal stromal cells (MSCs) are self-renewing cells with a role in supporting HSCs within the bone marrow vault and maintaining vascular and immune homeostasis, through their ability to selectively migrate to sites of tissue damage or inflammation (‘homing’). They have been extensively studied in multiple disease models as they are an easily accessible source of autologous or allogeneic somatic stem cells with the ability to differentiate in multiple directions [22, 23]. Moreover, they escape immunological surveillance and can be transplanted from an autologous, allogeneic source, even as a xenograft. It is noteworthy that their immunomodulatory, immunosuppressive, neurotrophic and repair functions may contribute to the treatment of MS [24].
The properties of MSCs that have been shown to be of potential therapeutic value for MS are as follows:
-
Myelin repair: differentiation into cells of neuroendothelial origin and replacement in the injured CNS, stimulation of proliferation of endogenous CNS neural stem cells [25, 26], and guidance of their differentiation towards oligodendrocyte lineages [27].
-
Suppression of inflammation and immunomodulation
-
Neuroprotection through neuroprotective, antioxidant agents, promotion of CNS neurite outgrowth and remodeling.
-
Reduced formation of gliotic scar: through their paracrine action, they can modify brain’s cellular microenvironment leading to a significant reduction of the lesion area [26]
-
Promotion of angiogenesis, enhances tissue repair [28]
-
Cell fusion: a mechanism of neuroprotection, whereby healthy nuclei or functional genes are introduced into damaged cells and help rescue them and restore function [29]
-
Direct transfer of mitochondria to vulnerable cells via membrane fusion with subsequent phagocytosis [30]
Cell replacement with MSCs
Several preclinical studies have been performed with administration of MSCs from various sources in animal models of MS, in which an improvement of the clinical picture and repair of the injured tissue has been observed [31], without clarifying whether the phenomenon is due to cellular replacement or paracrine and other actions of MSCs. There are on the other hand a number of studies that have proven cellular replacement with MSCs (Table 2).
EAE model
Nine of the experimental MSCs transplantation studies in the Table 2 were performed in rodent models with EAE and resulted in improved neurological function. Five of the studies used rodent MSCs [32,33,34,35,36], derived from bone marrow and placenta, while the other four used human MSCs isolated from bone marrow [36,37,38,39]. In two of the studies using rodent MSCs, cell replacement of various degrees was observed [35, 36], whereas no cell replacement was observed after administration of human MSCs. The therapeutic effect of intracerebroventricularly (ICV) and intrathecally (ITH) administered rat MSCs was partially attributed to cell replacement, as they trans-differentiated into cells expressing markers of neuronal and neuroglial phenotype, such as NF-200, Olig1, MBP, and GFAP [35]. The anti-inflammatory activity of MSCs also played an important role, as they attenuated perivascular and parenchymal infiltration, suppressed proinflammatory factors and increased the expression of anti-inflammatory cytokines. Similarly, in the study by Kassis et al. [36], both IV and ICV administered murine MSCs derived from bone marrow, have exhibited cell replacement, with MSCs being attracted to sites of CNS inflammation and displaying morphological and immunohistological characteristics of neuronal-directed cells, expressing beta-tubulin type III, GFAP, and galactosebroside. In addition, a reduction in CNS inflammation and significant protection of axons was observed, particularly after ICV injection, suggesting a possible local in situ immunomodulatory effect of MSCs. During IV administration, systemic immunomodulatory effects also played an important role through a reduction in lymphocyte proliferation.
In contrast, in the study by Grigoriadis et al. [33], where autologous MSCs from bone marrow were administered ICV to mice with EAE, cells displayed GFAP and NG2 phenotypes, but without sufficient morphological integration within the tissue. In the mild EAE model, MSCs exerted anti-inflammatory activity in the spinal cord and reduced axonopathy. However, in the severe form of EAE, significant adverse effects were observed, with the formation of cell masses in the brain parenchyma, focal inflammation, demyelination, axonal loss and increased collagen and fibronectin deposition. In the experiment of Gerdoni et al. [32], IV administered mouse MSCs derived from bone marrow entered the CNS but did not trans-differentiated into cells of neural origin. However, they led to a reduction in demyelination and inflammation by interfering with the pathogenic autoimmune response, inhibiting the pathogenic T and B cell response and the proliferation and production of inflammatory cytokines of brain-derived T cells. In the experiments of Zhang et al. [37, 39] and Bai et al. [27], human bone marrow derived MSCs were injected IV into mice with EAE and entered the demyelination areas of the CNS. However, either no colocalization was observed, or only a small number of MSCs colocalized with neuroglial cell markers. Even if the colocalization of these markers is due to actual trans-differentiation of a small proportion of MSCs into oligodendrocyte progenitor cells, their therapeutic effect cannot be attributed to this. Instead, enhancement of endogenous repair by stimulation of oligodendrogenesis was found, as well as anti-inflammatory activity of MSCs, with a decrease in inflammatory TH1 and TH17 cells, an increase in anti-inflammatory TH2, and expression of neurotrophic factors, such as brain-derived neurotrophic factor (BDNF) and neural growth factor (NGF). Nor in the study by Gordon et al. [38], where human MSCs were administered intraperitoneally to EAE mice, did cell replacement take place, as very little infiltration by MSCs was observed in the CNS and the demyelinated lesions. It is, thus, speculated that the beneficial effect is due to a peripheral or systemic immune effect.
In the experiment of Harris et al. [40], bone marrow-derived mouse MSCs were in vitro differentiated into neural progenitor cells, in order to have a greater neurogenic potential. After intracranial injection in mice with EAE, a reduction in demyelination and a detection of the stem cells in inflammatory foci was observed. However, despite the in vitro neural differentiation potential of these cells, no evidence of in vivo trans-differentiation was detected. The transplanted cells led to reduced T cell infiltration, indicating an anti-inflammatory mechanism of action and enhanced endogenous repair, with the detection of increased numbers of endogenous NPCs. Clinically, improvement in neurological function was found with multiple intradural injections, while a single injection did not affect disease scores.
In experiments involving the transplantation of MSCs into EAE models, diverse outcomes were observed. This variability reflects the differences in the studies’ design mainly regarding the source of the MSCs and the site of transplantation. It could also stem from other factors, including the microenvironment encountered by MSCs during homing. This environment may either enable them to eventually replace cells or hinder their functionality. The causes of this variability could be an area of further research and may reveal new roles for MSCs. Undoubtedly, this phenomenon underscores the challenges associated with cell therapy using MSCs.
Chemical demyelination
Three studies used rats with focal demyelination in the spinal cord after ethidium bromide injections followed by irradiation (EB-X model), to exclude the possibility of endogenous remyelination by oligodendrocytes or Schwann cells for at least 6–8 weeks [41,42,43]. MSCs from rodent bone marrow were administered by direct injection into the lesion or IV. In the experiment of Akiyama et al. [42], GFP-labeled mouse MSCs were administered by direct microinjection into the EB-X model. Upon electron microscopy of the lesion at 3 weeks, relatively extensive remyelination was observed, which was almost complete near the center of the lesion and partial at the lateral borders. In the absence of endogenous repair and in the presence of intense GFP fluorescence, it was concluded that the injected MSCs differentiated mainly into myelinating cells, thus cell replacement occurred. Furthermore, the remyelinated axons were also shown to be functional, as they showed improved conduction velocity. Similarly, in another study by Akiyama et al. [41], rat MSCs, contaminated with the LacZ gene, were administered, this time IV, to rats with EB-X focal demyelination, leading to remyelination. Approximately, 9% of the cells that formed myelin in the lesion showed β-galactosidase reaction products, but the majority of myelinating cells did not. From this, it is concluded that cell replacement occurs to a small extent, but that some endogenous repair mechanism, probably enhanced by MSCs, is responsible for most of the induced remyelination. However, given issues related to the low efficacy of LacZ contamination and the possibility of gene inactivation as cells progress to a myelinating phenotype, we cannot discern whether the remyelination was caused by the injected cells or whether the injection procedure facilitated an endogenous repair mechanism. Interestingly, in the latter two studies, remyelinated axons showed, on electron microscopy, morphological features similar to either central myelination from oligodendrocytes or peripheral myelination from Schwann cells, with large nuclei and an enveloping basement membrane. In addition, colocalization of both MPB, a myelin-specific protein for both central and peripheral myelin, and P0, specific for peripheral myelin, was observed with transplanted stromal cells. Functionally, partial recovery of electrophysiological function was found, with improved axon conduction velocity.
Contrary, in a study conducted by Hunt et al. [43], the administration of MSCs not only did not lead to remyelination and cell replacement, but instead had deleterious consequences, as they migrated to areas of normal tissue where they deposited collagen and caused axonal damage. The study by El-Akabawy and Rashed [44], used mice with cuprizone-induced non-immune demyelination as an experimental model, which were injected IV with MSCs from mouse bone marrow. Cuprizone induces oligodendrocyte apoptosis and subsequent demyelination. MSCs migrated, integrated and led to both a reduction in demyelination and an enhancement of remyelination. However, the authors postulated that remyelination was not induced by the administered cells, as no differentiation of MSCs towards the oligodendroglial phenotype was detected (absence of CNPase expression). The putative mechanisms of action identified were the direct enhancement of endogenous repair and the induction of oligo/neuroprotection, via reduction of the neuroglial response (astroglia and microglia) to cuprizone and reduction of oligodendrocyte apoptosis.
Myelin twitcher mutant
In the experiment of Croitoru-Lamoury et al. [45], human bone marrow MSCs were administered via intracerebral injections into twitcher mice. In 28 of 40 animals, MSCs were successfully integrated and maintained rounded or flattened cellular morphologies with few dendritic appendages, but did not migrate extensively into the CNS until day 14 post-transplant. Differentiation of MSCs into CNS cells was observed, as they were found by immunostaining to express the neuron-specific protein MAP2, the astrocytic protein GFAP, and oligodendrocyte proteins, MBP and CNPase. However, functionally, no change in clinical progression was found.
Neural stem cells (NSCs)
During the last decade, increasing interest has been focused on the use of neural stem cells (NSCs) to promote remyelination. In the adult CNS, tissue-specific stem sheaths, such as the subventricular zone (SVZ) of the lateral ventricles and the subgranular zone (SGZ) of the dentate gyrus of the hippocampus, contain the majority of endogenous NSCs with the ability to self-renew and differentiate into functional neurons and glia [46].
Pluripotent NSCs have also been isolated from the subcortical white matter of the adult human brain [47]. MS has been shown to significantly affect the proliferation of the endogenous NSCs and this effect has been correlated with clinical and histopathological findings in animal models of the disease [48]. NSCs in the adult mammalian brain produce rapidly dividing neural progenitor cells (NPCs) to generate neurons, astrocytes, and oligodendrocytes and contribute functionally to post-injury recovery processes [49]. For example, SVZ neuroblasts of adult mice can be directed mainly toward oligodendrocyte differentiation during lysolecithin-induced demyelination of the corpus callosum [50].
Apart from endogenous NSCs, transplanted NSCs and NPCs, which possess a high myelinogenic potential, provide encouraging results in animal models of MS. Exogenously administered NSCs and NPCs exert a beneficial effect on demyelination through cell replacement and immunomodulation, or by providing nutritional support, neuroprotection, and stimulating endogenous remyelination. For NSCs therapy in MS to be successful, the cells must possess sufficient plasticity to integrate and survive in the unfavorable inflammatory environment of the CNS, excellent migratory capacity to reach multiple lesion sites, and the ability to contribute to remyelination [13].
Several studies report that transplanted NSCs reduce the clinical and inflammatory signs of EAE, although they remain in the perivascular region without migrating to the site of injury [51,52,53] and suggest that NSCs exert beneficial effects not through cell replacement but through other mechanisms, such as immune regulation. In particular, transplantation of NSCs within brain ventricles reduces perivascular infiltrates, CD3+ T cells, and ICAM-1 and LFA-1 expression and increases T-regulatory cells in the brain and spinal cord [52, 53]. Adult NSCs overexpressing IL-10 significantly suppress CD45+ cells, CD4+ T cells, CD68+ macrophages/microglia, and CD8+ T cells in the spinal cord. They also inhibit the production of the inflammatory cytokines IFNγ and IL-17 and induce apoptosis of cerebellar T cells [54]. IV administration of NSCs reduces the number of CD3+ T cells and Mac3+ macrophages infiltrating the spinal cord [55], whereas subcutaneous injection of human NSCs inhibits T executive cell generation, dendritic cell differentiation and maturation, and cytokine production [56].
The nutritional and neuroprotective effects of NSCs are exerted through the delivery of neurotrophins, growth factors, stem cell developmental regulators and immunomodulatory molecules, all of which serve to regulate the microenvironment [57]. NSCs IV injected in an animal model of EAE secrete PDGF-α and FGF2, causing stimulation of proliferation and differentiation of oligodendrocyte progenitor cells (OPCs), and consequently, enhancing remyelination [58]. In EAE mice that were subcutaneously injected with NPCs before disease onset, NPCs accumulated in lymph nodes and inhibited myeloid dendritic cells [56]. Moreover, in chronic Alzheimer’s disease (AD), SVZ-derived congenic NSCs promote neuroprotection through the secretion of immunomodulatory molecules and neurotrophic factors [59].
Transplanted NPCs can stimulate endogenous remyelination by inducing the proliferation and terminal differentiation of endogenous OPCs. NPCs transplanted into the lateral ventricles of mice with cuprizone-induced demyelination exerted a trophic effect on endogenous OPCs, and the achieved remyelination in the corpus callosum was attributed exclusively to endogenous OPCs [58]. In another study, intradural injection of MSC-NPCs at the onset of the chronic phase of EAE in mice increased the number of endogenous OPCs and accelerated remyelination [34].
Cell replacement with NSCs
The intrinsic ability of NSCs to differentiate into oligodendroglial lineage cells has fostered hope for their application as clinical therapies in MS. Many preclinical studies have been conducted in a variety of both rodents and non-human primates to investigate the therapeutic potential of transplanting NSCs or OPCs in MS. The current perspective on the predominant mechanisms underlying the beneficial effect of transplanted NSCs involves diverse graft-host interactions, not focusing on the replacement of damaged tissue [57, 60]. However, there is a number of preclinical studies in animal models of MS that have used NSCs or OPCs investigating their potential for cell replacement (Tables 3 and 4). These cells are generated in specific stem cell-containing regions of the CNS, from where they migrate extensively into axonal pathways that myelinate. They persist into adulthood and are the cells responsible for remyelination [61].
EAE model
Eight experimental NPCs transplantation studies were performed in the EAE model. All were implemented in rodents, except for the study by Pluchino Gritti et al. [62], which was performed in non-human primates and used human-derived NSCs. McIntyre et al. in their study used both human and mouse NSCs in discrete experiments, while the remaining studies used rodent-derived NSCs[51, 59, 63,64,65,66]. Of the 7 studies using rodent NSCs, in 5 studies, cell replacement was observed, whereas no cell replacement was observed after administration of human NSCs [62, 67].
In the experiment by McIntyre et al. (2020), remyelination was observed after transplantation of both human and mouse NSCs intraspinal, but without significant clinical improvement. The beneficial structural effect in the case of mouse NSCs was attributed to cell replacement, whereas in the case of human NSCs to immunomodulation and promotion of endogenous repair. Similarly, in the study by Pluchino Gritti et al. (2009), immune regulation, rather than neural differentiation, is proposed as the main mechanism by which human NPCs improve EAE in vivo when the cells were injected IV and ITH. Immune functions, rather than cell replacement, were also attributed to the reduction of demyelination upon transplantation of congenic NPCs into mice with EAE in the experiment of Pluchino et al. (2005). IV administered NPCs selectively reached inflamed perivascular regions of the CNS (via activated integrins and chemokine receptors), where they survived as undifferentiated cells and exerted neuroprotective effects, inducing apoptosis of cerebellar T cells and thus protecting against chronic loss of neural tissue. Similarly, in the study by Merzaban et al. (2015), after IV injection of NPCs, despite the mitigation of the clinical process, no evidence of long-term stem cell integration was observed and neural repair was attributed to endogenous repair rather than direct cell replacement. Cell replacement was observed in the rest of the studies performed on the EAE model. In the experiment of Ben-Hur et al. (2003) injection of rat NPCs ICV or ITH resulted in extensive cell migration exclusively to the infiltrating white matter and expression of astrocytic (GFAP) and oligodendrocyte (NG2, GalC) markers. Another study found that neurospheres administered IV or intra-abdominally reduce demyelination and axonal loss in EAE with a dual mechanism of action, leading to both cell replacement and stimulation of endogenous remyelination [65]. Besides, Giannakopoulou et al. (2011) proposed that the stage of the disease has an important role, as the administration of mouse NPCs with bilateral ICV injection, had a different effect in the acute and chronic phase of EAE, with cell replacement occurring only in the chronic phase. The study by Sher et al. (2012) used unmodified mouse NSCs, but also NSCs with transient overexpression of the transcription factor Olig2, which is crucial for OPC maturation in myelinating oligodendrocytes [68]. Both cell types injected ICV migrated directly to active lesions, however, only Olig2-NSCs differentiated into OPCs (NG2+), while NSCs remained undifferentiated, expressing nestin [66].
Viral demyelination
When NPCs were administered with intracerebral or intraspinal injections to mice with virally induced demyelination after JHMV infection, cell replacement was observed as the transplanted cells migrated to the lesion sites and differentiated into myelinating cells that remyelinated the axons [69, 70]. Furthermore, it was shown that the Olig1 function is essential for the ability to remyelinate direct transplanted NPCs [71]. The Olig1 gene encodes the homonymous transcription factor, which is particularly involved in the development as well as the maturation of oligodendrocytes [72]. Olig1+/+NPCs differentiated mainly into NG2+ OPCs and formed MBP-expressing appendages surrounding the axons, whereas Olig1-/- NPCs differentiated into GFAP+ cells of the astrocytic lineage [71]. Migration into the lesion, differentiation into oligodendrocytes, and extensive remyelination after OPCs administration was also observed in another study with viral demyelination from JHMV [73], in which transplanted-retransplanted animals with OPCs injected at T8 spinal cord, contained approximately twice as many axons as non-transplanted animals, suggesting that remyelination is associated with axonal rescue.
Chemical demyelination
Three studies were found using rats with EB-X model. The study by Akiyama et al. (2001) used human NPCs, while the other two studies used rat NPCs [74, 75]. The myelinating cells displayed morphological and phenotypic characteristics of Schwann cells [76]. In the study of Keirstead et al. (1999), in which NPCs were directly injected into the lesion, the majority of axons were remyelinated from oligodendrocytes and only 19% were remyelinated from Schwann cells. In the study of Mothe & Tator (2008), transplanted NPCs in the spinal cord differentiated predominantly in an oligodendrocyte direction. However, only some of the oligodendrocyte progeny expressed MBP and remyelinated host axons, while most differentiated into non-myelinating oligodendrocytes. It is, therefore, concluded that NPCs have the intrinsic plasticity to differentiate into oligodendrocytes or Schwann-type cells depending on the host environment, with both cell types capable of myelinating axons [75]. In the experiments of Copray et al. (2006) performed with stereotactic implantation of mouse NPCs in the striatum, just below the demyelinated corpus callosum, mice with cuprizone-induced demyelination of the corpus callosum were used as experimental models, which were injected with mouse NPCs, as Olig2-NSCs, in contrast to unmodified NSCs, developed into active myelinating oligodendrocytes that contributed to remyelination [77]. In the study by Einstein et al. (2009), after intraventricular injection of NPCs, the observed corpus callosum remyelination was not due to cell replacement, as the transplanted cells did not migrate to the corpus callosum, but remained mostly in the periventricular region in an undifferentiated state. Remyelination was exclusively carried out by the endogenous OPCs of the recipient. Cell replacement was performed in two studies using lysolecithin demyelination rodents as experimental models, which were injected with human NPCs [78, 79]. In the study by Windrem et al. (2002), progenitor cells from adult human subcortical white matter were injected into the lesion of dysmyelination, migrated extensively through the demyelination sites and differentiated into myelinating MBP+ oligodendrocytes.
In the experiments of Franklin et al. (1995, 1996) and Groves et al. (1993), OPCs were administered to adult rats and cell replacement was observed, with OPCs differentiating into myelin-forming oligodendrocytes that remyelinate the stripped axons[80,81,82]. In the study by Franklin et al. (1995), differentiation of OPCs was performed not only in oligodendrocytes but also in GFAP(+) astrocytes within the lesion. Franklin et al. (1996) found that administered OPCs do not survive in normal tissue, but survive in tissue irradiated with X-rays or damaged by gliotoxin injection. Transplanted OPCs cannot migrate through normal tissue separating areas of demyelination, leading to the conclusion that transplantation of OPCs is only likely to be successful if cells are injected either directly into or near a lesion [80]. Migration into the lesion, differentiation into oligodendrocytes, and extensive remyelination after OPCs administration was also observed in zymosan demyelination [83].
Shiverer model of congenital dysmyelination
Cell replacement occurred in all five studies in which NPCs were transplanted into shiverer mice. In two of them, human NPCs were used [78, 84] while in the others mouse NPCs were used [75, 85, 86]. In all studies, the administered neural progenitor cells migrated extensively, integrated, and differentiated into oligodendrocytes that produced compact functional myelin.
Many of the above studies demonstrate the ability of transplanted human ΟPCs to myelinate the hypomyelinated brain of shiverer animals and improve both their neurological phenotype and lifespan [87,88,89,90]. All studies used OPCs of embryonic origin, except for the study by Windrem et al. (2004) where adult cells were also used. Both embryonic and adult OPCs were extensively incorporated and differentiated into oligodendrocytes that induced extensive myelination [87,88,89,90]. The myelination was so extensive that virtually complete chimerism of the recipient CNS was observed, with mouse gray matter and human-derived white matter glia [89]. However, some differences were observed between cells of embryonic and adult origin. Embryonic OPCs had a high migratory potential, whereas adult OPCs migrated shorter distances. Adult OPCs, however, produced oligodendrocytes in much higher proportions and, unlike embryonic OPCs, produced no astrocytes, indicating that adult OPCs behave in a more restricted manner, while embryonic OPCs act as glial progenitors. Furthermore, adult OPCs myelinated the shiverer mouse brain much faster (6 weeks) than their fetal counterparts (12–16 weeks) and covered more axons per cell [88].
For more efficient isolation of myelinogenic OPCs, Sim et al. (2011) selected embryonic human forebrain cells with the marker CD140a, an epitope of platelet-derived growth factor receptor that is specifically expressed by OPCs. Embryonic CD140a+ cells showed in vivo faster and more efficient remyelination, generating both oligodendrocytes and astrocytes (at a much lower fraction) in the recipient’s brains. Furthermore, they were observed to myelinate with an efficiency and time course analogous to adult OPCs, yet migrated widely, extending throughout the brain and stem, like embryonic OPCs. Thus, given their relative homogeneity, ability to migrate widely, and rapid myelinogenesis, CD140a+ cells have a potential advantage as cellular vectors for the treatment of myelin disorders [87, 88].
Myelin proteolipid protein (PLP) mutants
Administration of congenic OPCs to myelin-deficient rats with a mutation in the PLP1 gene resulted in cell migration and formation of normal PLP-positive graft-derived myelin [91,92,93]. In the study by Learish et al. (1999), long-term survival of ICV transplanted cells and retention of the capacity for astrocyte differentiation was observed, with a small percentage of astrocytes (< 5%) being donor-derived, although many of the transplanted cells seen in the gray matter remained undifferentiated.
Taiep rats (rats with inherited disorder of myelination)
In the experiment of Foote and Blakemore (2005), rat OPCs were administered to the Taiep model via injection into the spinal cord. This study showed that transfected OPCs, as in normal tissue [80] do not enter tissue containing endogenous OPCs, but only in areas where OPCs are depleted. However, even achieving extensive repopulation by OPCs, remyelination was limited to the cell injection site. This study also shows a clear correlation between the induction of acute inflammation and successful remyelination. This adds to the growing body of evidence that acute inflammation provides the stimulus for initiation of remyelination [94] and is evidence for the 'time mismatch’ hypothesis, an explanation for remyelination failure in MS. The absence of an acute inflammatory environment to provide the signals required to promote remyelination will fail the remyelination process [95].
Cells derived from embryonic stem cells (ESCs)
Embryonic stem cells (ESCs) are pluripotent cells derived from the internal cell mass of the blastocyst and are of interest as candidate cells for the treatment of MS, as they can differentiate into NSCs or OPCs [96]. The ability to form myelin from ESCs has been tested in vivo in a variety of animal models (Table 5). Although NSCs/OPCs derived from ESCs have shown promising preclinical results, their use is constricted due to ethical concerns regarding the source of the cells, as the collection of ESCs destroys the blastocyst. Furthermore, any residual pluripotency from the persistence of some undifferentiated ESCs remains an important safety issue. Thus, alternative sources of stem cells other than internal cell mass are favored for future clinical applications [22].
Cell replacement with ESCs
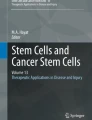
When administering mouse ESC-OPCs, via ICV or intraspinal infusion, to myelin-deficient rats with dysmyelination due to PLP mutation, they differentiated into oligodendrocytes that myelinated their host axons [97, 98]. Similarly, transplantation of ESCs of both humans [99, 100] and mice [101] in a shiverer model of dysmyelination led to migration and differentiation of cells into mature oligodendrocytes producing MBP+ myelin (Fig. 1).

(Reproduced with permission from Nistor Gi et al. 2005 [100])
Human embryonic stem cell (hESC)-derived oligodendrocytes integrate, differentiate and display a functional myelinating phenotype following transplantation into the shiverer mutant mouse. A BrdU immunostaining illustrating the presence of transplanted BrdU pre-labeled cells within the spinal cord white matter. BrdU pre-labeled cells were found almost exclusively within spinal cord white matter. B CC-1 immunostaining on the same section as (A) illustrating oligodendrocytes. C Composite of BrdU and CC-1 double immunostaining, illustrating that transplanted BrdU+ cells adopted the oligodendroglial marker CC-1. Arrows point to double labeled cells, arrowheads point to BrdU-CC-1+ cells (endogenous shiverer oligodendrocytes). These panels indicate that transplanted BrdU pre-labeled cells survived and integrated within the spinal cord white matter, and became oligodendrocytes. D Electron micrograph illustrating that axons of shiverer mice are devoid of myelin or are surrounded by one or two uncompacted wraps of myelin. E Electron micrograph of the dorsal column white matter of a shiverer mouse 6 weeks after transplantation of hESC-derived oligodendrocyte progenitors, illustrating multilayered compact myelin. F High-magnification image of compact myelin 6 weeks after transplantation of hESC-derived oligodendrocyte progenitors, illustrating multilayered compact myelin. Shiverer mice do not contain multilayered compact myelin. E, F Myelination by transplanted cells. G, H MBP immunopositive myelin patches within the dorsal column white matter of shiverer mice 6 weeks after transplantation of hESC-derived oligodendrocyte progenitors. I MBP immunopositive myelin patches within the ventral column white matter of shiverer mice 6 weeks after transplantation of hESC-derived oligodendrocyte progenitors; nuclei are in blue. As shiverer mice do not produce MBP, G–I demonstrate myelination by transplanted cells. A, B, C, G, H, × 400; D, E, × 20,500; F, × 40,000; I, × 2,000.
When administering ESC-derived NSCs to mice with EAE, a significant improvement in the clinical picture was observed with a reduction in the severity of the disease. However, this beneficial effect was not due to cell replacement, but to the immunomodulatory and neuroprotective properties of ESCs [102,103,104]. In the study of Aharonowiz et al. (2008), human ESC-NPCs transplanted within the lateral ventricles of mice with EAE reduced the number of T cells which cause encephalitis, axonal damage, and demyelination. Although NPCs survived and migrated extensively into the brain parenchyma, no differentiation into mature oligodendrocytes occurred, and the extent of remyelination was negligible [102]. In the experiment of Cao et al. (2011), mouse ESC-NPCs administered IV in mice with EAE led to a reduction in inflammation and demyelination, but NPCs were rarely detected in the CNS [103]. Furthermore, intra-abdominal administration of human ESC-OPCs in mice with EAE led to a reduction in inflammation and an increase in the number of regulatory T cells within the CNS, while the transplanted cells themselves remained within the ventricular system and did not survive for more than 10 days [104].
Similarly, in the model with demyelination by murine hepatitis virus, human ESC-NPCs that were administered intraductal survived in the parenchyma of the spinal cord for only 1 week, but through immunomodulatory and paracrine effects improved functional effects, reduced demyelination, increased remyelination, and limited neuroinflammation. As the transplanted human NPCs did not differentiate into oligodendroglia, the remyelination appeared in response to the activation of endogenous OPCs via specific factors secreted by human NPCs [105].
Cells derived from induced pluripotent stem cells (iPSCs)
Reprogrammed cells, having similar characteristics to ESCs, can be differentiated into all cell types, such as NSCs or OPCs (iPSC-NSCs and iPSC-OPCs, respectively). Reprogramming somatic cells of patients into pluripotent cells permit their differentiation in vitro towards desired cell lines or tissues for pathophysiological research or in vivo cell therapy. For the treatment of MS, the differentiation of iPSCs towards oligodendrocyte direction plays a predominant role [106].
However, iPSCs-derived cells cannot yet be used in clinical practice. There is growing evidence that the epigenetic signature of cells can be maintained after induction into iPSCs, leading to issues of immune rejection of grafts [107], or unexpected functions of iPSCs. In one example, iPSC-NSCs grown from patients with PPMS, when transplanted into models of cuprizone-demyelinated mice, exhibited inherent defects, as they lack the neuroprotective phenotype observed in control iPSC-NSCs [108]. Furthermore, the induction process required for the generation of nervous system cells from iPSCs and the expansion to produce enough cells for transplantation is very time-consuming, increasing the likelihood of genetic instability leading to oncogenesis upon transplantation [91].
Cell replacement with iPSCs
iPSC-NSCs
iPSC-NSCs have similar results in animal models of MS, with NSCs from the subventricular zone (Table 6). NSCs from mouse iPSCs, administered intracranially to mice with EAE, provided clinical improvement and reduction of demyelinating areas, axonal damage, and infiltrating inflammatory cells, while no toxicity or tumorigenesis was observed [109]. In addition, they were attracted to damaged areas such as somatic NSCs [65] and were found either in demyelinating lesions or at sites of increased inflammatory cell infiltration. However, most transplanted NSCs did not differentiate in vivo in an oligodendrocyte direction, demonstrating that remyelination is not due to cell replacement. In contrast, iPSC-NSCs, through secretion of a neurotrophin leukemia inhibitory factor (LIF), promoted the survival and differentiation of endogenous OPCs and mature oligodendrocytes [109]. Similarly, a subsequent study observed an improvement in symptoms and reduced T cells via ICV transplantation of iPSC-NSCs at the peak of EAE (18 days after induction) [110].
iPSC-OPCs
Another common source of cells for transplantation are OPCs derived from iPSCs. Their in vivo administration in different animal models of MS examined myelin formation from iPSC-OPCs. After their infusion into the cuprizone-induced demyelinated mouse mesenchyme, they differentiated into mature MBP+ oligodendrocytes contributing to the remyelination of neurons [111, 112]. They were also transplanted into, demyelinated from lysolecithin, rat optic chiasm, leading to apparent remyelination. In addition, they were incorporated into the chiasm and differentiated into mature PLP+ and/or MBP+ oligodendrocytes, which remyelinated the axons and contributed to the functional recovery. Some of the transplanted cells also differentiated into GFAP+ astrocytes or MAP2+ neurons [113]. In a genetic model of congenital hypomyelination, administering OPCs derived from human iPSCs to mouse shiverer observed potent derived donor myelination and electron microscopy revealed the production of structurally mature solid myelin, with alternating major dense and intraperipheral lines [114, 115].
Mice transplanted with human iPSC-OPCs improved survival and reduced mortality over a 9-month observation period. In addition, they migrated widely, and differentiated into myelinogenic oligodendrocytes throughout the subcortical white matter and into astrocytes, especially in the central white matter. The speed and efficiency of myelination of human iPSC-OPCs were higher than that of OPCs derived from embryonic tissue [115]. Human iPSC-OPCs generated from MS patients were also injected into shiverer mice and after 16 weeks, human MBP+ oligodendrocytes were detected diffusely throughout the mesocolonium and approximately 30% of the mouse axons were myelinated by them; however, very few differentiated into human GFAP+ astrocytes, localized in the SVZ and periventricular, suggesting that the local environment may induce astrocyte differentiation in these areas [114].
OPCs derived from human iPSCs were also tested in EAE models, where they were transplanted ICV in mice or marmosets with EAE, reducing inflammatory cell infiltration and demyelination, and improving functionality, but without detecting exogenous cells in the lesions. Thus, their beneficial effect did not appear to be due to cell replacement, but most likely to secreted protective or anti-inflammatory factors. However, when transplanted directly into the parenchyma of primates (marmosets) with EAE, the majority of iPSC-OPCs differentiated into mature oligodendrocytes that myelinated the stripped axons, while the remainder retained characteristics of OPCs or differentiated into astrocytes [112].
Direct transformation of body cells in NSCs and OPCs (iNSCs, iOPCs)
CNS regeneration could also be based on stem cells related to iNSCs and iOPCs that differentiated from somatic cells such as fibroblasts. In this way, they circumvent the problem of multipotency and immunogenicity, and are able to be used in autologous transplantation.
Cell replacement with iNSCs and iOPCs
iNSCs
According to Kim et al. (2011) [116], fibroblasts were transformed into iNSCs cells under appropriate culture conditions based on the four Yamanaka reprogramming factors (Table 6). In vitro iNSCs cells grow stably and secrete pro-regenerative molecules such as neurotrophic factors from glial cells (GDNF) and the brain (BDNF). On the other hand, in vivo, they can be integrated long-term and functionally into the CNS offering various regenerative applications.
iNSCs cells were transplanted into the cerebellum of 1-day-old shiverer mice, according to dysmyelination models, and differentiated in 10 weeks into functional oligodendrocytes, producing MBP+ myelin [117]. Besides, in demyelinated mouse mesenchyme via cuprizone, transplanted iNSCs differentiated into either oligodendrocytes or astrocytes or remained undifferentiated. Although this transplantation did not reduce demyelination, it succeeded in increasing oligodendrocytes and endogenous OPCs, improving motor deficits. Chronic neuroinflammation and behavioral deficits were ameliorated by transplanted iNSCs cells, which are equivalent to their somatic NSC counterparts and migrate to the meningeal regions of mice, producing proinflammatory MPs. However, few cells proliferated and expressed neuronal, astroglial or oligodendroglial markers [118]. Thus, the therapeutic effect of transplanted iNSCs cells relies not only on cell replacement but also on stimulation of endogenous repair and immunomodulation.
iOPCs
According to Najm et al. [119], regarding iOPCs cells, fibroblasts through specific transcription factors are directly reprogrammed into myeloid iOPCs without the mediation of iPSCs cells. These surround host neurons, producing structurally compact MBP+ myelin when transplanted into hypomyelinated shiverer mice [119]. Similarly, Yang et al. used shiverer mouse brains that were injected with iOPCs cells derived from mouse and rat fibroblasts. These, formed tubular structures around axons at all injection sites expressing myelin, which is present in the CNS, because all MBP+ cells expressed PLP. But they did not produce protein zero, which is the main protein of peripheral myelin. This finding supports the myelinogenicity of iOPCs [120].
Conclusion
While the treatment of MS continues to evolve, treatment options appear to remain limited in the improvement or prevention of relapses and episodes of acute inflammation in recurrent or active MS. There are no approved interventions capable of effectively promoting the recovery of damaged CNS and stopping the gradual accumulation of disability. Stem cell transplantation is a promising treatment in terms of its regenerative potential, however, most of the preclinical and clinical research has shown that immunomodulatory and trophic properties of stem cells, and not the cell replacement, are the main mechanism of their beneficial effects, making them candidates for the treatment of relapsing or progressive forms of MS. The major hopes for cell replacement and impact on progressive forms of the disease rest on NSCs, somatic or trans-differentiated, for which there is strong preclinical evidence for improving chronic neuroinflammation, but which have not yet been clinically studied to a significant extent in the context of MS [22].
Overall, cell therapies in MS have been experimentally tested for at least 4 decades [121] and significant progress has been made in recent years (Table 7). Hematopoietic and mesenchymal stem cell-based approaches are already in clinical trials. Regarding HSCs, it has strong efficacy in recurrent MS, with markedly better outcomes in patients with active inflammatory disease, short duration of disease, and lower EDSS scores. This is consistent with a therapy that aims to control peripheral immunopathology without directly affecting pathological processes within the CNS. Unfortunately, only one of the studies has shown direct cell replacement when it was injected directly into the striatum and hippocampus and remyelination was performed with different pathways. Transplantation of other types of stem cells, such as MSCs or NSCs/OPCs, may be more useful in patients with progressive forms of MS, where degenerative mechanisms dominate, but this hypothesis has not yet been confirmed [122]. Recent clinical trials are exploiting the immunomodulatory, neuroprotective, and reparative properties of MSCs. Most of the experiments did not show cell replacement despite the positive effect in the reverse of clinical picture and symptomatology which was mainly attributed to the beneficial paracrine action of transplanted MSCs. MSCs administration showed cell replacement only, in one experiment when they were transplanted in the demyelination area and showed no effect in ICV nor IV administration. The use of MSCs has several practical advantages, including relative ease of isolation, mainly when it comes to MSCs of dental pulp or adipose tissue origin, safe administration, and avoidance of the need for immunosuppressive therapy to prevent rejection since autologous transplantation is possible [123]. To date, published clinical trials have been limited to small safety and efficacy studies, and while they have shown a favorable adverse event profile, the efficacy of MSCs transplantation is modest [31].
NSCs/OPCs transplantation showed a significant positive effect in cell replacement in multiple demyelination models with high percentages of successful outcomes. Only when the injection was IV there was no cell replacement but other ways of remyelination, immunomodulation, and neuroprotection.
While HSCs, MSCs, and NSCs have long been used in preclinical and/or clinical studies for the treatment of demyelination, the successful generation of iPSCs from somatic cells opens a new era in stem cell therapy. The advantages of easy obtaining from the patient’s tissues and good tolerance make stem cells derived from iPSCs or direct trans-differentiation of somatic cells, such as iNSCs and iOPCs, the most suitable candidates for personalized cell replacement therapy. Following trials in EAE and other demyelinating models, stem cell-derived iPSCs have shown significant potential in the treatment of MS when transplanted in the demyelination area. Cell replacement and differentiation into mature oligodendrocytes were observed in most of the experiments when the cell was transplanted directly into the parenchyma. Although there are still many issues to be resolved before clinical application, it is expected that, with the rapid progress in the field of iPSCs, these challenges can be addressed, making iPSC-derived cell transplantation an autologous, safe, and highly effective treatment for MS [22, 106].
While the safety and feasibility of stem cell transplantation have been demonstrated for various cell types and routes of delivery, there is still a need for larger and/or more rigorous studies to quantify the benefits of stem cell therapy and demonstrate superiority over current best treatment models [22]. Thus, all forms of cell therapy for MS should be considered experimental at this time. Rarely, there may be patients with aggressive recurrent MS, with no response to available therapies, for whom autologous HSC transplantation may be warranted. Except for these, cell therapy in MS should only be applied in the context of rigorous clinical trials. In all the cases, comprehensive safety and efficacy data should be collected and reported to existing databases [122].
Data availability
All data related to this paper are available upon reasonable request to the first author.
Code availability
Not applicable.
References
Dobson R, Giovannoni G. Multiple sclerosis–a review. Eur J Neurol. 2019;26:27–40.
Ghasemi N, Razavi S, Nikzad E. Multiple sclerosis: pathogenesis, symptoms, diagnoses and cell-based therapy. Cell J. 2017;19:1–10.
Hauser SL, Cree BAC. Treatment of multiple sclerosis: a review. Am J Med. 2020;133:1380-90.e2.
Hicks MR, Pyle AD. The emergence of the stem cell niche. Trends Cell Biol. 2022. https://doi.org/10.1016/j.tcb.2022.07.003.
Biehl JK, Russell B. Introduction to stem cell therapy. J Cardiovasc Nurs. 2009;24:98–103.
Mahla RS. Stem cells applications in regenerative medicine and disease therapeutics. Int J Cell Biol. 2016;2016:1–24.
Chang C-Y, Ting H-C, Liu C-A, et al. Induced pluripotent stem cell (iPSC)-based neurodegenerative disease models for phenotype recapitulation and drug screening. Molecules. 2020;25:2000.
Baker CL, Pera MF. Capturing totipotent stem cells. Cell Stem Cell. 2018;22:25–34.
O’Connell AE, Guseh S, Lapteva L, et al. Gene and stem cell therapies for fetal care. JAMA Pediatr. 2020;174:985.
Gonzalez MA, Bernad A. Characteristics of adult stem cells. Adv Exp Med Biol. 2012;741:103–20. https://doi.org/10.1007/978-1-4614-2098-9_8.
Dulak J, Szade K, Szade A, et al. Adult stem cells: hopes and hypes of regenerative medicine. Acta Biochim Pol. 2015;62:329–37.
Sivandzade F, Cucullo L. Regenerative stem cell therapy for neurodegenerative diseases: an overview. Int JMol Sci. 2021;22(4):2153. https://doi.org/10.3390/ijms22042153.
Xiao J, Yang R, Biswas S, et al. Neural stem cell-based regenerative approaches for the treatment of multiple sclerosis. Mol Neurobiol. 2018;55:3152–71.
Ng AP, Alexander WS. Haematopoietic stem cells: past, present and future. Cell Death Discov. 2017;3:17002.
Muraro PA, Martin R, Mancardi GL, et al. Autologous haematopoietic stem cell transplantation for treatment of multiple sclerosis. Nat Rev Neurol. 2017;13:391–405.
Burt RK, Padilla J, Begolka WS, et al. Effect of disease stage on clinical outcome after syngeneic bone marrow transplantation for relapsing experimental autoimmune encephalomyelitis. Blood. 1998;91:2609–16.
Karussis DM, Vourka-Karussis U, Lehmann D, et al. Prevention and reversal of adoptively transferred, chronic relapsing experimental autoimmune encephalomyelitis with a single high dose cytoreductive treatment followed by syngeneic bone marrow transplantation. J Clin Investig. 1993;92:765–72.
Mancardi GL, Sormani MP, Gualandi F, et al. Autologous hematopoietic stem cell transplantation in multiple sclerosis: a phase II trial. Neurology. 2015;84:981–8.
Genc B, Bozan HR, Genc S, Genc K. Stem Cell Therapy for Multiple Sclerosis. Adv Exp Med Biol. 2019;1084:145–74. https://doi.org/10.1007/5584_2018_247.
Goolsby J, Makar T, Dhib-Jalbut S, et al. Hematopoietic progenitors express myelin basic protein and ensheath axons in Shiverer brain. J Neuroimmunol. 2013;257:13–20.
Harris KM, Lim N, Lindau P, et al. Extensive intrathecal T cell renewal following hematopoietic transplantation for multiple sclerosis. JCI Insight. 2020. https://doi.org/10.1172/jci.insight.127655.
Smith JA, Nicaise AM, Ionescu R-B, et al. Stem cell therapies for progressive multiple sclerosis. Front Cell Dev Biol. 2021. https://doi.org/10.3389/fcell.2021.696434.
Siatskas C, Payne NL, Short MA, et al. A Consensus Statement Addressing Mesenchymal Stem Cell Transplantation for Multiple Sclerosis: It’s Time! Stem Cell Rev Rep [Internet]. 2010;6:500–06. Available from: http://link.springer.com/https://doi.org/10.1007/s12015-010-9173-y.
Rice CM, Scolding NJ. Adult human mesenchymal cells proliferate and migrate in response to chemokines expressed in demyelination. Cell Adh Migr. 2010;4:235–40.
Munoz JR, Stoutenger BR, Robinson AP, et al. Human stem/progenitor cells from bone marrow promote neurogenesis of endogenous neural stem cells in the hippocampus of mice. Proc Natl Acad Sci. 2005;102:18171–6.
Dori I, Petrakis S, Giannakopoulou A, et al. Seven days post-injury fate and effects of genetically labelled adipose-derived mesenchymal cells on a rat traumatic brain injury experimental model. Histol Histopathol. 2017;32:1041–55.
Bai L, Lennon DP, Eaton V, et al. Human bone marrow-derived mesenchymal stem cells induce Th2-polarized immune response and promote endogenous repair in animal models of multiple sclerosis. Glia. 2009;57:1192–203.
Branscome H, Paul S, Yin D, et al. Use of stem cell extracellular vesicles as a “Holistic” approach to CNS repair. Front Cell Dev Biol. 2020. https://doi.org/10.3389/fcell.2020.00455.
Kemp K, Gray E, Wilkins A, et al. Purkinje cell fusion and binucleate heterokaryon formation in multiple sclerosis cerebellum. Brain. 2012;135:2962–72.
Li C, Cheung MKH, Han S, et al. Mesenchymal stem cells and their mitochondrial transfer: a double-edged sword. 2019. Biosci Rep. https://doi.org/10.1042/BSR20182417.
Sarkar P, Rice CM, Scolding NJ. Cell therapy for multiple sclerosis. CNS Drugs. 2017;31:453–69.
Gerdoni E, Gallo B, Casazza S, et al. Mesenchymal stem cells effectively modulate pathogenic immune response in experimental autoimmune encephalomyelitis. Ann Neurol. 2007;61:219–27.
Grigoriadis N, Lourbopoulos A, Lagoudaki R, et al. Variable behavior and complications of autologous bone marrow mesenchymal stem cells transplanted in experimental autoimmune encephalomyelitis. Exp Neurol. 2011;230:78–89.
Harris VK, Yan QJ, Vyshkina T, et al. Clinical and pathological effects of intrathecal injection of mesenchymal stem cell-derived neural progenitors in an experimental model of multiple sclerosis. J Neurol Sci. 2012;313:167–77.
Jiang H, Zhang Y, Tian K, et al. Amelioration of experimental autoimmune encephalomyelitis through transplantation of placental derived mesenchymal stem cells. Sci Rep. 2017;7:41837.
Kassis I, Grigoriadis N, Gowda-Kurkalli B, et al. Neuroprotection and immunomodulation with mesenchymal stem cells in chronic experimental autoimmune encephalomyelitis. Arch Neurol. 2008. https://doi.org/10.1001/archneur.65.6.753.
Zhang J, Li Y, Chen J, et al. Human bone marrow stromal cell treatment improves neurological functional recovery in EAE mice. Exp Neurol. 2005;195:16–26.
Gordon D, Pavlovska G, Glover CP, et al. Human mesenchymal stem cells abrogate experimental allergic encephalomyelitis after intraperitoneal injection, and with sparse CNS infiltration. Neurosci Lett. 2008;448:71–3.
Zhang J, Li Y, Lu M, et al. Bone marrow stromal cells reduce axonal loss in experimental autoimmune encephalomyelitis mice. J Neurosci Res. 2006;84:587–95.
Harris VK, Vyshkina T, Sadiq SA. Clinical safety of intrathecal administration of mesenchymal stromal cell–derived neural progenitors in multiple sclerosis. Cytotherapy. 2016;18:1476–82.
Akiyama Y, Radtke C, Honmou O, et al. Remyelination of the spinal cord following intravenous delivery of bone marrow cells. Glia. 2002;39:229–36.
Akiyama Y, Radtke C, Kocsis JD. Remyelination of the rat spinal cord by transplantation of identified bone marrow stromal cells. J Neurosci. 2002;22:6623–30.
Hunt DPJ, Irvine KA, Webber DJ, et al. Effects of direct transplantation of multipotent mesenchymal stromal/stem cells into the demyelinated spinal cord. Cell Transpl. 2008;17:865–73.
El-Akabawy G, Rashed LA. Beneficial effects of bone marrow-derived mesenchymal stem cell transplantation in a non-immune model of demyelination. Ann Anat Anat Anz. 2015;198:11–20.
Croitoru-Lamoury J, Williams KR, Lamoury FMJ, et al. Neural transplantation of human MSC and NT2 cells in the twitcher mouse model. Cytotherapy. 2006;8:445–58.
Jin K, Galvan V. Endogenous Neural Stem Cells in the Adult Brain. Journal of Neuroimmune Pharmacology [Internet]. 2007;2:236–42. Available from: http://link.springer.com/https://doi.org/10.1007/s11481-007-9076-0.
Nunes MC, Roy NS, Keyoung HM, et al. Identification and isolation of multipotential neural progenitor cells from the subcortical white matter of the adult human brain. Nat Med. 2003;9:439–47.
Giannakopoulou A, Grigoriadis N, Bekiari C, et al. Acute inflammation alters adult hippocampal neurogenesis in a multiple sclerosis mouse model. J Neurosci Res. 2013;91:890–900.
Ming G, Song H. Adult neurogenesis in the Mammalian brain: significant answers and significant questions. Neuron. 2011;70:687–702.
Nait-Oumesmar B, Decker L, Lachapelle F, et al. Progenitor cells of the adult mouse subventricular zone proliferate, migrate and differentiate into oligodendrocytes after demyelination. Eur J Neurosci. 1999;11:4357–66.
Ben-Hur T, Einstein O, Mizrachi-Kol R, et al. Transplanted multipotential neural precursor cells migrate into the inflamed white matter in response to experimental autoimmune encephalomyelitis. Glia. 2003;41:73–80.
Einstein O, Grigoriadis N, Mizrachi-Kol R, et al. Transplanted neural precursor cells reduce brain inflammation to attenuate chronic experimental autoimmune encephalomyelitis. Exp Neurol. 2006;198:275–84.
Einstein O, Karussis D, Grigoriadis N, et al. Intraventricular transplantation of neural precursor cell spheres attenuates acute experimental allergic encephalomyelitis. Mol Cell Neurosci. 2003;24:1074–82.
Yang J, Jiang Z, Fitzgerald DC, et al. Adult neural stem cells expressing IL-10 confer potent immunomodulation and remyelination in experimental autoimmune encephalitis. J Clin Investig. 2009;119:3678–91.
Einstein O, Fainstein N, Vaknin I, et al. Neural precursors attenuate autoimmune encephalomyelitis by peripheral immunosuppression. Ann Neurol. 2007;61:209–18.
Pluchino S, Zanotti L, Brambilla E, et al. Immune regulatory neural stem/precursor cells protect from central nervous system autoimmunity by restraining dendritic cell function. PLoS ONE. 2009;4:e5959.
Cossetti C, Alfaro-Cervello C, Donegà M, et al. New perspectives of tissue remodelling with neural stem and progenitor cell-based therapies. Cell Tissue Res. 2012;349:321–9.
Einstein O, Friedman-Levi Y, Grigoriadis N, et al. Transplanted neural precursors enhance host brain-derived myelin regeneration. J Neurosci. 2009;29:15694–702.
Pluchino S, Zanotti L, Rossi B, et al. Neurosphere-derived multipotent precursors promote neuroprotection by an immunomodulatory mechanism. Nature. 2005;436:266–71.
Ben-Hur T, Goldman SA. Prospects of cell therapy for disorders of myelin. Ann N Y Acad Sci. 2008;1142:218–49.
Franklin RJM, Ffrench-Constant C. Remyelination in the CNS: from biology to therapy. Nat Rev Neurosci. 2008;9:839–55.
Pluchino S, Gritti A, Blezer E, et al. Human neural stem cells ameliorate autoimmune encephalomyelitis in non-human primates. Ann Neurol. 2009;66:343–54.
Giannakopoulou A, Grigoriadis N, Polyzoidou E, et al. Time-dependent fate of transplanted neural precursor cells in experimental autoimmune encephalomyelitis mice. Exp Neurol. 2011;230:16–26.
Merzaban JS, Imitola J, Starossom SC, et al. Cell surface glycan engineering of neural stem cells augments neurotropism and improves recovery in a murine model of multiple sclerosis. Glycobiology. 2015;25:1392–409.
Pluchino S, Quattrini A, Brambilla E, et al. Injection of adult neurospheres induces recovery in a chronic model of multiple sclerosis. Nature. 2003;422:688–94.
Sher F, Amor S, Gerritsen W, et al. Intraventricularly injected Olig2-NSCs attenuate established relapsing-remitting EAE in mice. Cell Transplant. 2012;21:1883–97.
McIntyre LL, Greilach SA, Othy S, et al. Regulatory T cells promote remyelination in the murine experimental autoimmune encephalomyelitis model of multiple sclerosis following human neural stem cell transplant. Neurobiol Dis. 2020;140:104868.
Zhou Q, Wang S, Anderson DJ. Identification of a novel family of oligodendrocyte lineage-specific basic helix–loop–helix transcription factors. Neuron. 2000;25:331–43.
Carbajal KS, Schaumburg C, Strieter R, et al. Migration of engrafted neural stem cells is mediated by CXCL12 signaling through CXCR4 in a viral model of multiple sclerosis. Proc Natl Acad Sci. 2010;107:11068–73.
Greenberg ML, Weinger JG, Matheu MP, et al. Two-photon imaging of remyelination of spinal cord axons by engrafted neural precursor cells in a viral model of multiple sclerosis. Proc Natl Acad Sci. 2014. https://doi.org/10.1073/pnas.1406658111.
Whitman LM, Blanc CA, Schaumburg CS, et al. Olig1 function is required for remyelination potential of transplanted neural progenitor cells in a model of viral-induced demyelination. Exp Neurol. 2012;235:380–7.
Lu QR, Sun T, Zhu Z, et al. Common developmental requirement for olig function indicates a motor neuron/oligodendrocyte connection. Cell. 2002;109:75–86.
Totoiu M. Remyelination, axonal sparing, and locomotor recovery following transplantation of glial-committed progenitor cells into the MHV model of multiple sclerosis. Exp Neurol. 2004;187:254–65.
Keirstead HS, Ben-Hur T, Rogister B, et al. Polysialylated neural cell adhesion molecule-positive CNS precursors generate both oligodendrocytes and schwann cells to remyelinate the CNS after transplantation. J Neurosci. 1999;19:7529–36.
Mothe AJ, Tator CH. Transplanted neural stem/progenitor cells generate myelinating oligodendrocytes and Schwann cells in spinal cord demyelination and dysmyelination. Exp Neurol. 2008;213:176–90.
Akiyama Y, Honmou O, Kato T, et al. Transplantation of clonal neural precursor cells derived from adult human brain establishes functional peripheral myelin in the rat spinal cord. Exp Neurol. 2001;167:27–39.
Copray S, Balasubramaniyan V, Levenga J, et al. Olig2 overexpression induces the in vitro differentiation of neural stem cells into mature oligodendrocytes. Stem Cells. 2006;24:1001–10.
Buchet D, Garcia C, Deboux C, et al. Human neural progenitors from different foetal forebrain regions remyelinate the adult mouse spinal cord. Brain. 2011;134:1168–83.
Windrem MS, Roy NS, Wang J, et al. Progenitor cells derived from the adult human subcortical white matter disperse and differentiate as oligodendrocytes within demyelinated lesions of the rat brain. J Neurosci Res. 2002;69:966–75.
Franklin RJM, Bayley SA, Blakemore WF. Transplanted CG4 cells (an oligodendrocyte progenitor cell line) survive, migrate, and contribute to repair of areas of demyelination in x-irradiated and damaged spinal cord but not in normal spinal cord. Exp Neurol. 1996;137:263–76.
Franklin RJM, Bayley SA, Milner R, et al. Differentiation of the O-2A progenitor cell line CG-4 into oligodendrocytes and astrocytes following transplantation into glia-deficient areas of CNS white matter. Glia. 1995;13:39–44.
Groves AK, Barnett SC, Franklin RJM, et al. Repair of demyelinated lesions by transplantation of purified 0–2A progenitor cells. Nature. 1993;362:453–5.
Wang Y, Piao J-H, Larsen EC, et al. Migration and remyelination by oligodendrocyte progenitor cells transplanted adjacent to focal areas of spinal cord inflammation. J Neurosci Res. 2011;89:1737–46.
Uchida N, Chen K, Dohse M, et al. Human neural stem cells induce functional myelination in mice with severe dysmyelination. Sci Transl Med. 2012. https://doi.org/10.1126/scitranslmed.3004371.
Vitry S, Avellana-Adalid V, Lachapelle F, et al. Migration and multipotentiality of PSA-NCAM+ neural precursors transplanted in the developing brain. Mol Cell Neurosci. 2001;17:983–1000.
Yandava BD, Billinghurst LL, Snyder EY. “Global” cell replacement is feasible via neural stem cell transplantation: evidence from the dysmyelinated shiverer mouse brain. Proc Natl Acad Sci. 1999;96:7029–34.
Sim FJ, McClain CR, Schanz SJ, et al. CD140a identifies a population of highly myelinogenic, migration-competent and efficiently engrafting human oligodendrocyte progenitor cells. Nat Biotechnol. 2011;29:934–41.
Windrem MS, Nunes MC, Rashbaum WK, et al. Fetal and adult human oligodendrocyte progenitor cell isolates myelinate the congenitally dysmyelinated brain. Nat Med. 2004;10:93–7.
Windrem MS, Schanz SJ, Guo M, et al. Neonatal chimerization with human glial progenitor cells can both remyelinate and rescue the otherwise lethally hypomyelinated shiverer mouse. Cell Stem Cell. 2008;2:553–65.
Windrem MS, Schanz SJ, Zou L, et al. Human glial progenitor cells effectively remyelinate the demyelinated adult brain. Cell Rep. 2020;31:107658.
Lee AS, Tang C, Rao MS, et al. Tumorigenicity as a clinical hurdle for pluripotent stem cell therapies. Nat Med. 2013;19:998–1004.
Tontsch U, Archer DR, Dubois-Dalcq M, et al. Transplantation of an oligodendrocyte cell line leading to extensive myelination. Proc Natl Acad Sci. 1994;91:11616–20.
Zhang S-C, Ge B, Duncan ID. Adult brain retains the potential to generate oligodendroglial progenitors with extensive myelination capacity. Proc Natl Acad Sci. 1999;96:4089–94.
Franklin RJM. Why does remyelination fail in multiple sclerosis? Nat Rev Neurosci. 2002;3:705–14.
Chari D, Blakemore W. New insights into remyelination failure in multiple sclerosis: implications for glial cell transplantation. Mult Scler. 2002;8:271–7.
Chanoumidou K, Mozafari S, Baron-Van Evercooren A, et al. Stem cell derived oligodendrocytes to study myelin diseases. Glia. 2020;68:705–20.
Brüstle O, Jones KN, Learish RD, et al. embryonic stem cell-derived glial precursors: a source of myelinating transplants. Science. 1979;1999(285):754–6.
Glaser T, Perez-Bouza A, Klein K, et al. Generation of purified oligodendrocyte progenitors from embryonic stem cells. FASEB J. 2005;19:112–4.
Izrael M, Zhang P, Kaufman R, et al. Human oligodendrocytes derived from embryonic stem cells: effect of noggin on phenotypic differentiation in vitro and on myelination in vivo. Mol Cell Neurosci. 2007;34:310–23.
Nistor GI, Totoiu MO, Haque N, et al. Human embryonic stem cells differentiate into oligodendrocytes in high purity and myelinate after spinal cord transplantation. Glia. 2005;49:385–96.
Zhang P-L, Izrael M, Ainbinder E, et al. Increased myelinating capacity of embryonic stem cell derived oligodendrocyte precursors after treatment by interleukin-6/soluble interleukin-6 receptor fusion protein. Mol Cell Neurosci. 2006;31:387–98.
Aharonowiz M, Einstein O, Fainstein N, et al. Neuroprotective effect of transplanted human embryonic stem cell-derived neural precursors in an animal model of multiple sclerosis. PLoS ONE. 2008;3:e3145.
Cao W, Yang Y, Wang Z, et al. Leukemia inhibitory factor inhibits T helper 17 cell differentiation and confers treatment effects of neural progenitor cell therapy in autoimmune disease. Immunity. 2011;35:273–84.
Kim H, Walczak P, Kerr C, et al. Immunomodulation by transplanted human embryonic stem cell-derived oligodendroglial progenitors in experimental autoimmune encephalomyelitis. Stem Cells. 2012;30:2820–9.
Chen L, Coleman R, Leang R, et al. Human neural precursor cells promote neurologic recovery in a viral model of multiple sclerosis. Stem Cell Reports. 2014;2:825–37.
Xie C, Liu Y-Q, Guan Y-T, et al. Induced stem cells as a novel multiple sclerosis therapy. Curr Stem Cell Res Ther. 2016;11:313–20.
Zhao T, Zhang Z-N, Rong Z, et al. Immunogenicity of induced pluripotent stem cells. Nature. 2011;474:212–5.
Nicaise AM, Banda E, Guzzo RM, et al. iPS-derived neural progenitor cells from PPMS patients reveal defect in myelin injury response. Exp Neurol. 2017;288:114–21.
Laterza C, Merlini A, De Feo D, et al. iPSC-derived neural precursors exert a neuroprotective role in immune-mediated demyelination via the secretion of LIF. Nat Commun. 2013;4:2597.
Zhang C, Cao J, Li X, et al. Treatment of multiple sclerosis by transplantation of neural stem cells derived from induced pluripotent stem cells. Sci China Life Sci. 2016;59:950–7.
Czepiel M, Balasubramaniyan V, Schaafsma W, et al. Differentiation of induced pluripotent stem cells into functional oligodendrocytes. Glia. 2011;59:882–92.
Thiruvalluvan A, Czepiel M, Kap YA, et al. Survival and functionality of human induced pluripotent stem cell-derived oligodendrocytes in a nonhuman primate model for multiple sclerosis. Stem Cells Transl Med. 2016;5:1550–61.
Pouya A, Satarian L, Kiani S, et al. Human induced pluripotent stem cells differentiation into oligodendrocyte progenitors and transplantation in a rat model of optic chiasm demyelination. PLoS ONE. 2011;6:e27925.
Douvaras P, Wang J, Zimmer M, et al. Efficient generation of myelinating oligodendrocytes from primary progressive multiple sclerosis patients by induced pluripotent stem cells. Stem Cell Reports. 2014;3:250–9.
Wang S, Bates J, Li X, et al. Human iPSC-derived oligodendrocyte progenitor cells can myelinate and rescue a mouse model of congenital hypomyelination. Cell Stem Cell. 2013;12:252–64.
Kim J, Efe JA, Zhu S, et al. Direct reprogramming of mouse fibroblasts to neural progenitors. Proc Natl Acad Sci. 2011;108:7838–43.
Lujan E, Chanda S, Ahlenius H, et al. Direct conversion of mouse fibroblasts to self-renewing, tripotent neural precursor cells. Proc Natl Acad Sci. 2012;109:2527–32.
Peruzzotti-Jametti L, Bernstock JD, Vicario N, et al. Macrophage-derived extracellular succinate licenses neural stem cells to suppress chronic neuroinflammation. Cell Stem Cell. 2018;22:355-68.e13.
Najm FJ, Lager AM, Zaremba A, et al. Transcription factor–mediated reprogramming of fibroblasts to expandable, myelinogenic oligodendrocyte progenitor cells. Nat Biotechnol. 2013;31:426–33.
Yang N, Zuchero JB, Ahlenius H, et al. Generation of oligodendroglial cells by direct lineage conversion. Nat Biotechnol. 2013;31:434–9.
Blakemore WF. Remyelination of CNS axons by Schwann cells transplanted from the sciatic nerve. Nature. 1977;266:68–9.
Scolding NJ, Pasquini M, Reingold SC, et al. Cell-based therapeutic strategies for multiple sclerosis. Brain. 2017;140:2776–96.
Karussis D, Karageorgiou C, Vaknin-Dembinsky A, et al. Safety and immunological effects of mesenchymal stem cell transplantation in patients with multiple sclerosis and amyotrophic lateral sclerosis. Arch Neurol. 2010. https://doi.org/10.1001/archneurol.2010.248.
Funding
Open access funding provided by HEAL-Link Greece. No external funding was used for this publication.
Author information
Authors and Affiliations
Contributions
All the authors contributed to the literature search and analysis, writing, and reviewing the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests related to this manuscript.
Ethics approval
Not applicable, since this is a review manuscript.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Christodoulou, M.V., Petkou, E., Atzemoglou, N. et al. Cell replacement therapy with stem cells in multiple sclerosis, a systematic review. Human Cell 37, 9–53 (2024). https://doi.org/10.1007/s13577-023-01006-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13577-023-01006-1