
Abstract
Introduction
Vitiligo is an autoimmune disease, causing skin depigmentation. Individuals with vitiligo incur substantial psychosocial burden and have expressed frustration with their treatments. Here, we describe the burden of vitiligo and opinions on what constitutes meaningful change among participants of two qualitative interview studies.
Methods
Qualitative interviews were conducted with a subgroup of adolescent and adult participants with vitiligo from two pivotal phase 3 clinical trials of ruxolitinib cream (Study 1) and a real-world panel (Study 2). Participants were asked about their disease burden, treatment goals, importance of facial/body improvement (treatment satisfaction: scale range 0–10), and meaningfulness of change (yes/no).
Results
A total of 36 participants from Study 1 and 23 from Study 2 were interviewed. In Study 1, the highest degree of impact was on reduced self-esteem (facial lesions, 62.5%; body lesions, 55.6%), social inhibition (facial lesions, 65.6%; body lesions, 61.1%), and sun sensitivity (facial lesions, 31.3%; body lesions, 55.6%). Most participants (83.3%) reported that facial improvement was equally (36.1%) or more important (47.2%) than body improvement, with mean treatment satisfaction of 8.1 and 6.9, respectively. Meaningful change was reported by 83.3% and 92.9% of participants with 50–74% and ≥ 75% improvement per the facial Vitiligo Area Scoring Index, respectively, and by 82.6% of participants with ≥ 25% improvement per the total Vitiligo Area Scoring Index per Study 1 outcomes at Week 24. In Study 2, most (82.6%) participants felt that the noticeability of their vitiligo affected their behavior. Nearly all (87.0%) said that an ideal treatment would repigment or return natural color to their facial skin; 56.5% considered ≥ 50% facial repigmentation to be the smallest meaningful improvement.
Conclusions
Participants from both qualitative interviews expressed substantial psychosocial burden. Repigmentation in both facial and body vitiligo were important, with meaningful change determined to be ≥ 50% facial repigmentation and ≥ 25% body repigmentation.
Plain Language Summary
Vitiligo is an autoimmune disease that causes white patches to appear on the skin, affecting about 2% of people worldwide. People with vitiligo often have poor quality of life due to their disease and frequently do not believe that treatments work. We explored how people with vitiligo felt about their disease, and asked what hopes they had for treatment. Individual telephone interviews were conducted with 36 adolescents and adults with vitiligo from two clinical studies (Study 1) and 23 adolescents and adults with vitiligo from a real-world panel (Study 2) in the USA and Canada. Those from Study 1 said that their vitiligo caused them to have low self-esteem and to feel lonely. Most said that it was as important or more important to restore color to white patches on their face (i.e., repigmentation) than the body. Most achieving repigmentation of more than 50% on the face or more than 25% on the body were pleased with their treatment. In Study 2, most people said that their disease affected their behavior, and nearly all said that completely restoring color to their facial skin (i.e., 100% repigmentation) was important. Over half said that the smallest change they thought was important was more than 50% facial repigmentation. In short, people with vitiligo in two interview studies said that their vitiligo affected their quality of life. Most people with vitiligo in these studies reported that it was important to repigment more than 50% on the face and more than 25% on the body.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Patients with vitiligo, an autoimmune disease in which patches of skin are progressively depigmented, have reduced quality of life and are largely dissatisfied with their treatments. |
In two phase 3 studies (TRuE-V1/TRuE-V2), ruxolitinib cream, a selective Janus kinase (JAK) 1/JAK2 inhibitor, was statistically superior versus vehicle cream in repigmenting lesions after 24 weeks of treatment, with continued improvement in outcomes through Week 52. |
In this study, interviews were conducted with a subgroup of patients from TRuE-V1/TRuE-V2 (Study 1) and a real-world panel (Study 2) regarding their experiences with vitiligo and what constitutes meaningful improvement. |
What was learned from this study? |
Study participants expressed that living with vitiligo is associated with substantial psychosocial burden. |
Repigmentation of facial and body vitiligo were important to study participants, with ≥ 50% facial repigmentation and ≥ 25% body repigmentation considered to be meaningful. |
Nearly all study participants indicated that an ideal treatment would repigment or the return of natural color to their facial skin. |
Introduction
Vitiligo is a chronic autoimmune disease in which depigmented patches appear on the skin due to destruction of melanocytes [1]. Vitiligo affects 0.5–2.0% of the global population, varying by geographic region [2, 3]. Patients with vitiligo often have psychological distress, diminished quality of life (QoL), and increased risk of psychosocial morbidity, with certain clinical variables (e.g., disease duration, lesion location, extent of disease, and skin type) predicting reduced QoL [4, 5]. Notably, patients with vitiligo are more likely to have depression or anxiety compared with healthy individuals [6,7,8]. Many patients have expressed that their treatment regimens have not been helpful and hoped for novel and improved treatments [9, 10]. Thus, there is a need to further understand vitiligo disease burden, as well as treatment experiences and expectations from the patient perspective.
A cream formulation of ruxolitinib, a selective Janus kinase (JAK) 1/JAK2 inhibitor [11], is approved for the treatment of nonsegmental vitiligo in adults and adolescents ≥ 12 years old in the USA (2022), Europe, and the UK (2023) [12,13,14]. In two randomized phase 3 trials [TRuE-V1 (NCT04052425) and TRuE-V2 (NCT04057573), collectively referred to as Study 1 hereafter], ruxolitinib cream was statistically superior to vehicle cream in repigmenting lesions after 24 weeks of treatment, including facial lesions [the primary endpoint of an improvement in facial Vitiligo Area Scoring Index (F-VASI) of ≥ 75% from baseline (F-VASI75) was met by approximately 30% of patients], with a higher percentage of patients achieving repigmentation endpoints at Week 52 [15].
These trials, alongside real-world practice, present an opportunity to query patients about their experiences with vitiligo and their treatment expectations. Qualitative interviews were conducted with a subgroup of adolescent and adult patients with vitiligo in Study 1 (i.e., TRuE-V phase 3 trials) and with a real-world panel of adolescents and adults with vitiligo (Study 2) to evaluate the burden of facial and body vitiligo and to better understand what treatment goals are important to people with vitiligo.
Methods
Study 1 Exit Interviews
Participants ≥ 12 years old with nonsegmental vitiligo with depigmented areas ≤ 10% body surface area (BSA) including ≥ 0.5% BSA on the face and ≥ 3% BSA on nonfacial areas, with scores ≥ 0.5 on the F-VASI (range 0–3, with higher scores representing a greater area of facial lesions, e.g., 1.5 equals half of the face) and scores ≥ 3 on total VASI (T-VASI; range 0–100, with higher scores indicating a greater area of total body lesions), were eligible for enrollment in the Study 1 trials. Trial design was described previously [15].
Adolescent and adult participants in the USA and Canada who completed the 24-week double-blind treatment period of the Study 1 trials were eligible for interviews if they were available to be interviewed within approximately 10–15 weeks of reaching Week 24 endpoints of the preceding TRuE-V phase 3 studies, consented to and were able to participate in a telephone interview, and did not have a history of any neurologic or mental health condition that may have rendered them unable to fully understand the nature and scope of the study. During the 60-min telephone exit interview (see Interview Guide in Appendix S1 in the electronic supplementary materials), participants were asked open-ended questions with probes to explore their experiences with vitiligo in relation to vitiligo lesions on the face and body before and after 24 weeks of treatment with ruxolitinib cream. Participants were also asked about the types of impacts or effects of vitiligo (emotional, social, and physical) on their lives before trial enrollment and observed changes on the face and body after 24 weeks of ruxolitinib cream treatment. Participants were asked to rate their treatment satisfaction [11-point scale; scale range 0–10 (higher scores indicating more satisfaction or importance)] and the meaningfulness of change (yes or no) as a function of F-VASI, T-VASI, and the Vitiligo Noticeability Scale (VNS; 5-point scale: 1, more noticeable; 2, as noticeable; 3, slightly less noticeable; 4, a lot less noticeable; 5, no longer noticeable). Both treatment satisfaction and reported meaningfulness of change were segmented by the participant’s measured reduction in F-VASI and T-VASI (i.e., improvement in repigmentation) from baseline at Week 24 in the preceding TRuE-V studies. Observed differences among subgroups were used to define a threshold for meaningful improvements from baseline in VASI [quantitatively segmented: 0–24% (smallest improvement), 25%–49%, 50%–74%, and 75%–100% (largest improvement) for F-VASI and T-VASI] and VNS (scores 3–5, slightly less to no longer noticeable).
De-identified transcripts were generated from all recorded interviews using the ATLAS.ti v8 software (Berlin, Germany). From the coded interviews, participant-level data were entered into a macro-enabled Excel (Microsoft, Redmond, WA) spreadsheet for further analysis and to enable the tracking of impacts for each participant and the quantitative data (e.g., participant treatment satisfaction, identified meaningfulness of change). Data were summarized using descriptive statistics. Immediate and general impacts were grouped into three categories for analysis: emotional, social, and physical. Treatment satisfaction, VNS rating, and participant-expressed meaningfulness of change were segmented on the basis of measured F-VASI and T-VASI improvements from baseline at Week 24.
The study protocols were approved by the Western Institutional Review Board and an institutional review board or ethics committee at participating centers. Trials conducted under Study 1 were conducted in accordance with the Declaration of Helsinki and adhered to study protocols, Good Clinical Practice, and applicable country-specific laws and regulations. Written informed consent or assent was provided by all patients. The Incyte Corporation sponsored the trial (including provision of study drug), participated in study design development, and collaborated with authors in analyzing and interpreting the data and writing and approving the manuscript. Authors prepared the manuscript, with medical writing assistance funded by the sponsor. All authors confirm the accuracy and completeness of the data and analyses and adherence to the trial protocol. Agreements requiring study investigators to maintain data confidentiality were in place between the sponsor and authors.
Study 2 Interviews
Participants from the USA were from a convenience sample identified by a recruiting firm via their proprietary database, support groups, and social media advertising. Adolescents (aged ≥ 12 years) and adults who self-reported a clinician diagnosis of either vitiligo, “loss of pigment”, or “depigmentation” on the face were eligible for inclusion. During the 45-min telephone interview (Interview Concept Overview in Appendix S2 in the electronic supplementary materials), participants were asked general questions intended to elicit information on their experience with facial vitiligo. These included time since diagnosis, how participants characterize their facial vitiligo [i.e., affected surface area, location of lesions, color and texture of lesions, how active (spreading) or stable lesions have been, and self-reported severity: not severe, less severe, moderately severe, or severe], what is most bothersome to them about their condition, and the treatment outcomes they consider most important (e.g., affected surface area, lesion location on the face, repigmentation, and ability to cover facial vitiligo). Targeted questions were asked to ensure that all concepts of interest were addressed if not mentioned spontaneously. Participants were also asked to indicate the smallest improvement in facial repigmentation they would consider meaningful.
Data were systematically collected from study participants in the form of Excel-based field notes and audio files, with the latter being transcribed and prepared for qualitative analysis. Standard qualitative analysis methods were applied to evaluate the data collected during the individual interviews [16]. Using both the transcripts and field notes, dominant trends in each interview were identified and compared across interviews to describe the themes and relative importance of concepts described by participants. This process was used to generate themes or patterns in the way participants described their observations and experiences. Data were summarized using descriptive statistics.
Study 2 was performed in accordance with the Declaration of Helsinki and in adherence to the study protocol and local regulatory requirements. All survey participants provided informed consent at screening and could withdraw consent at any time. The study protocol was approved by the RTI Institutional Review Board.
Results
Demographics and Baseline Clinical Characteristics
A total of 36 participants completed the Study 1 exit interviews and had a mean (range) age of 38.2 (12–80) years; 50.0% were female, and the most common Fitzpatrick skin types were skin types II (36.1%) and III (33.3%; Table 1). All participants had vitiligo on the face and body. In Study 2, 23 participants with facial vitiligo were interviewed and had a mean (range) age of 42.4 (15–66) years; 91.3% were female, and the majority had Fitzpatrick skin types II (21.7%), III (26.1%), and IV (21.7%). Lesions below the face and neck were present in 60.9% of participants.
Study 1 Exit Interviews
Disease Burden and Treatment Satisfaction
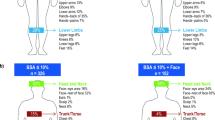
Study 1 participants described vitiligo as having emotional, social, and physical impacts, with the highest degree of impact for these categories being reduced self-esteem (facial and body lesions, 62.5%, 55.6%, respectively), social inhibition (65.6% and 61.1%), and sun sensitivity (31.3% and 55.6%; Fig. 1). The majority (69.4%) reported prior treatment for their vitiligo, with the most commonly used therapies being topical corticosteroids (30.6%) and topical calcineurin inhibitors (25.0%; Figure S1 in the electronic supplementary materials).

Percentage of interviewees from Study 1 who reported an impact for facial and body vitiligo. aResponses available for 32 of 36 participants with facial vitiligo
Most participants (83.3%) indicated that facial improvement (i.e., repigmentation) was equally (36.1%) or more (47.2%) important than body improvement, primarily due to the visibility and difficulty of covering up the face. Mean importance of facial and body vitiligo improvement (i.e., treatment satisfaction) were 8.1 and 6.9, respectively. For F-VASI, participants who achieved F-VASI75 at Week 24 reported the highest mean treatment satisfaction rating (8.1) compared with those who had < 75% reduction from baseline (range, 4.7–6.8; Fig. 2). For T-VASI, the highest mean satisfaction rating was identified among those who had a reduction of 50–74% (T-VASI50–74; 7.5; Fig. 2).

Treatment satisfaction by F-VASI and T-VASI among interviewees from Study 1. F-VASI facial VASI; T-VASI total VASI; VASI Vitiligo Area Scoring Index. aResponses available for 33 of 36 participants; 3 participants were not asked this exact question. bResponses available for 34 of 36 participants; 2 participants were not asked about their treatment satisfaction of body vitiligo at Week 24
Meaningful Change in Facial and Total Body Vitiligo
Among participants who achieved ≥ 50% reduction from baseline in F-VASI (F-VASI50) at Week 24, 18/20 (90.0%) reported their improvement as clinically meaningful compared with 8/15 (53.3%) of participants who achieved < 50% reduction from baseline (Fig. 3). Notably, 5/6 (83.3%) participants with 50–74% reduction from baseline (F-VASI50–74) and 13/14 (92.9%) participants with F-VASI75 reported clinically meaningful change. Clinically meaningful change in T-VASI was reported by 19/23 (82.6%) participants with ≥ 25% reduction from baseline (T-VASI25) compared with 6/10 (60.0%) participants who achieved < 25% reduction from baseline. No increase in meaningful change was observed between T-VASI reductions of 25–49% [10/12 (83.3%)], 50–74% [5/6 (83.3%)], and ≥ 75% [4/5 (80.0%)]. All participants who reported a facial VNS of 3 (n = 10), 4 (n = 14), or 5 (n = 1) indicated that they had clinically meaningful change. Among participants with F-VASI75, 13/14 (92.9%) reported a facial VNS score ≥ 3 and clinically meaningful change; the 1 participant who reported the change as not meaningful also reported a facial VNS of 2 (as noticeable).

Percentage of interviewees from Study 1 reporting meaningful change in facial and body vitiligo based on F-VASI and T-VASI reduction at Week 24. F-VASI facial VASI; T-VASI total VASI; VASI Vitiligo Area Scoring Index. aResponses available for 35 of 36 participants; 1 participant was either not asked about meaningful change of F-VASI reduction or did not answer the question. bResponses available for 33 of 36 participants; 3 participants were either not asked about meaningful change of T-VASI reduction or did not answer the question
Study 2 Interviews
Disease Burden and Treatment History
Mean (range) facial vitiligo coverage reported by Study 2 participants was 44.3% (5–100%). Of 23 participants, nearly half [11 (47.8%)] described their vitiligo as “very severe,” “pretty severe,” or “extremely severe,” and most [19 (82.6%)] reported that the noticeability of their facial vitiligo affected their behavior. Across Fitzpatrick skin types, 10 (43.5%) participants reported that vitiligo affects them emotionally (e.g., feeling self-conscious or uncomfortable) and mentally (e.g., feeling anxious or depressed). Social life (e.g., avoiding or limiting social activities) was impacted in 9 (39.1%) participants, and 5 (21.7%) participants reported that they wear skin protection to conceal affected areas. Aspects of vitiligo reported as most bothersome were loss of pigmentation [6 (26.1%)], appearance [6 (26.1%)], location of lesions [6 (26.1%)], and ability or inability to cover affected areas [3 (13.0%)]. A total of 20 (87.0%) participants had prior treatment, with the most commonly used therapies being topical prescription medication [12 (52.2%)] and light therapy [11 (47.8%); Fig. S2 in the electronic supplementary materials]. At the time of the interview, 17 (73.9%) participants were not receiving any prescription medications or medical procedures. Participants generally reported either no results or no lasting results from previous treatment, or they discontinued treatments due to side effects (e.g., sunburn, blisters, and nausea), expense, or inconvenience.
Meaningful Change in Facial Vitiligo
A total of 20 (87.0%) participants indicated that an ideal facial vitiligo treatment would repigment their face or return natural color to their skin. Therapy aspects considered “extremely important” or “very important” by a majority of participants were complete elimination of their facial vitiligo [i.e., complete repigmentation, 16 (69.6%)], reduction in noticeability [15 (65.2%)], reduction in the affected area of facial vitiligo [15 (65.2%)], and change in the appearance of the affected area on the face (12 [52.2%]; Fig. 4). In all, 21 (91.3%) participants were interested in repigmentation. Overall, 13 (56.5%) participants reported that ≥ 50% facial repigmentation would be the smallest meaningful improvement to them, and 1 participant indicated that ≥ 75% would be the smallest meaningful improvement (Fig. 5).

Importance of aspects of an ideal facial vitiligo treatment reported by Study 2 participants. Participants rated the importance of each treatment goal

Percentage of facial repigmentation considered meaningful among Study 2 participants (N = 23). F-VASI facial Vitiligo Area Scoring Index
Discussion
Participants with vitiligo from qualitative studies in populations from a clinical trial (Study 1) and a real-world panel of adolescents and adults (Study 2) demonstrated profound disease burden that affected their QoL. Both facial and body vitiligo conferred emotional, social, and physical impacts that caused participants to alter their behavior. They especially felt that their vitiligo made them self-conscious about their appearance and inhibited their social lives. The participants in both studies emphasized their priority for improvements in facial vitiligo, with ≥ 50% facial repigmentation considered clinically meaningful among a majority of participants in either study. Furthermore, participants in Study 1 also considered ≥ 25% body repigmentation and a facial VNS score ≥ 3 to indicate a meaningful improvement.
A systematic literature review of clinical and observational studies in patients with vitiligo demonstrated an association between vitiligo and low self-esteem, social avoidance behavior, and psychiatric conditions such as depression and anxiety [5]. Patient stories have shown the negative real-world impact of vitiligo on self-consciousness, careers, and daily interactions, regardless of age or race [17]. These impacts were also observed in a recent qualitative study of adolescents and adults with vitiligo, who felt self-conscious and impaired in their social interactions and needed to protect their skin from the sun [18]. The results of the two qualitative studies presented here support these findings, with a majority of participants in Study 1 reporting low self-esteem, feeling socially inhibited, and experiencing sun sensitivity; in Study 2, nearly all participants reported alterations in behavior due to their vitiligo.
In surveys of individuals from Germany and the Netherlands, many people with vitiligo reported not experiencing benefit from their treatment and expressed demand for novel treatments [9, 10]. Most participants in Studies 1 and 2 reported having used ≥ 1 previous treatment for their vitiligo. Although not solicited in Study 1, most participants in Study 2 reported not receiving any treatment at the time of the interview, citing lack of or nondurable results or discontinuation due to side effects, expense, or inconvenience.
The International Initiative for Outcomes workshops and a recent qualitative study found that individuals with vitiligo view ≥ 80% repigmentation on a target lesion as successful repigmentation, with F-VASI75 and T-VASI50 considered measures of overall treatment success [19, 20]. Notably, patients in previous studies felt that improvement in facial vitiligo was critical due to the visibility of disfiguring lesions on the face, and facial involvement was found to be the main driver of patient-perceived vitiligo severity [19, 21, 22]. Participants in both studies presented here indicated that facial improvement was an important goal for an ideal treatment, including among nearly 70% of participants in Study 2, who noted that complete facial repigmentation was very or extremely important. Most participants in Study 1 felt that improvement in facial vitiligo was as important or more important than improvement in body vitiligo. In both studies presented here, the threshold improvement in facial vitiligo considered clinically meaningful was achievement of ≥ F-VASI50; in Study 1, ≥ T-VASI25 was determined to indicate clinically meaningful improvement in body vitiligo. It should be noted that participants in Study 1 reflected on whether the level of repigmentation they actually experienced following 24 weeks of treatment was clinically meaningful, whereas previous studies asked participants to anticipate what they might find clinically meaningful in an abstract ideal, similar to the population in Study 2 [19, 20]. Additionally, participants in Study 1 were motivated to enroll in a clinical trial to alleviate their lesions, so they may have had a higher level of bother before enrollment and potentially could have had greater satisfaction with a lower threshold of clinically meaningful improvement. The view of such improvements among individuals with vitiligo may be consistent with a VNS score of 3 (“slightly less noticeable”), which was found to be clinically meaningful among participants in Study 1 and also recently validated in another clinical trial [23].
Studies 1 and 2 were based on qualitative patient interviews, although the interview responses were summarized using a descriptive, quantitative approach. This merger of qualitative research with quantitative reporting may help identify areas that warrant further investigation. Additionally, this approach was considered as an objective way to overcome the bias and high variability of purely qualitative data outputs.
Interpretation of the presented analyses are limited by potential bias based on nonsystematic participant selection that may result in participants not being reflective of broader vitiligo populations; therefore, caution should be used when generalizing these findings. Of note, the population of Study 1 consisted of participants who were enrolled in a clinical trial and had ≤ 10% affected BSA, including ≥ 0.5% facial BSA and ≥ 3% nonfacial BSA at baseline, and participants in Study 2 had self-reported facial vitiligo with no inclusion criteria for body lesions. Study 2 also had the limitation of over 90% of participants being female (versus 50% in Study 1). Additionally, the sample sizes in both studies were small, although they fell within generally acceptable ranges for qualitative studies [24], and subgroup analysis by baseline characteristics including Fitzpatrick skin type could not be undertaken. In Study 2, questions regarding cessation of spread or maintenance of repigmentation as treatment goals were not asked. Other limitations include potential errors in data due to reliance on the accuracy of participants’ responses.
Conclusion
In summary, results from both qualitative interview studies indicate that facial and body vitiligo affects participants emotionally, socially, and physically, causing them to alter their behavior in several ways. Participants indicated that improvement in both facial and body vitiligo were important, with ≥ 50% facial repigmentation (F-VASI50), ≥ 25% body repigmentation (T-VASI25), and less noticeable lesions (VNS score ≥ 3) identified as being meaningful. Taken together, these findings highlight the burden of vitiligo in daily life and ideal milestones for new treatments. Larger surveys of patients in clinical trials and real-world studies of individuals with vitiligo are necessary to support these findings.
Data Availability
Incyte Corporation (Wilmington, DE, USA) is committed to data sharing that advances science and medicine while protecting patient privacy. Qualified external scientific researchers may request anonymized datasets owned by Incyte for the purpose of conducting legitimate scientific research. Researchers may request anonymized datasets from any interventional study (except phase 1 studies) for which the product and indication have been approved on or after 1 January 2020 in at least one major market (eg. USA, EU, Japan). Data will be available for request after the primary publication or 2 years after the study has ended. Information on Incyte’s clinical trial data sharing policy and instructions for submitting clinical trial data requests are available at: https://www.incyte.com/Portals/0/Assets/Compliance%20and%20Transparency/clinical-trial-data-sharing.pdf?ver=2020-05-21-132838-960.
References
Rodrigues M, Ezzedine K, Hamzavi I, Pandya AG, Harris JE. New discoveries in the pathogenesis and classification of vitiligo. J Am Acad Dermatol. 2017;77(1):1–13.
Kruger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51(10):1206–12.
Bibeau K, Pandya AG, Ezzedine K, et al. Vitiligo prevalence and quality of life among adults in Europe, Japan, and the USA. J Eur Acad Dermatol Venereol. 2022;36(10):1831–44.
Alikhan A, Felsten LM, Daly M, Petronic-Rosic V. Vitiligo: a comprehensive overview. Part I. Introduction, epidemiology, quality of life, diagnosis, differential diagnosis, associations, histopathology, etiology, and work-up. J Am Acad Dermatol. 2011;65(3):473–91.
Ezzedine K, Eleftheriadou V, Jones H, et al. Psychosocial effects of vitiligo: a systematic literature review. Am J Clin Dermatol. 2021;22(6):757–74.
Lai YC, Yew YW, Kennedy C, Schwartz RA. Vitiligo and depression: a systematic review and meta-analysis of observational studies. Br J Dermatol. 2017;177(3):708–18.
Wang G, Qiu D, Yang H, Liu W. The prevalence and odds of depression in patients with vitiligo: a meta-analysis. J Eur Acad Dermatol Venereol. 2018;32(8):1343–51.
Liu J, Tang R, Xiao Y, et al. Meta-analytic review of high anxiety comorbidity among patients with vitiligo. BioMed Res Int. 2021. https://doi.org/10.1155/2021/6663646.
Narayan VS, Uitentuis SE, Luiten RM, Bekkenk MW, Wolkerstorfer A. Patients’ perspective on current treatments and demand for novel treatments in vitiligo. J Eur Acad Dermatol Venereol. 2021;35(3):744–8.
Radtke MA, Schafer I, Gajur AI, Augustin M. Clinical features and treatment outcomes of vitiligo from the patients’ perspective: results of a national survey in Germany. Dermatology (Basel, Switzerland). 2010;220(3):194–200.
Quintás-Cardama A, Vaddi K, Liu P, et al. Preclinical characterization of the selective JAK1/2 inhibitor INCB018424: therapeutic implications for the treatment of myeloproliferative neoplasms. Blood. 2010;115(15):3109–17.
Opzelura™ (ruxolitinib cream). Full prescribing information, Incyte Corporation, Wilmington, DE, 2023.
Opzelura™ (ruxolitinib cream). Summary of product characteristics, Incyte Biosciences Distribution B.V., Amsterdam, Netherlands, 2023.
OpzeluraTM. (ruxolitinib cream). Summary of product characteristics, Incyte Biosciences UK Ltd, Leatherhead, UK, 2023.
Rosmarin D, Passeron T, Pandya AG, et al. Two phase 3, randomized, controlled trials of ruxolitinib cream for vitiligo. N Engl J Med. 2022;387:1445–55.
Patrick DL, Burke LB, Gwaltney CJ, et al. Content validity–establishing and reporting the evidence in newly developed patient-reported outcomes (PRO) instruments for medical product evaluation: ISPOR PRO good research practices task force report: part 1—eliciting concepts for a new PRO instrument. Value Health. 2011;14(8):967–77.
Grimes PE, Miller MM. Vitiligo: patient stories, self-esteem, and the psychological burden of disease. Int J Womens Dermatol. 2018;4(1):32–7.
Kitchen H, Gandhi K, Carmichael C, et al. A qualitative study to develop and evaluate the content validity of the vitiligo patient priority outcome (ViPPO) measures. Dermatol Ther (Heidelb). 2022;12(8):1907–24.
Kitchen H, Wyrwich KW, Carmichael C, et al. Meaningful changes in what matters to individuals with vitiligo: content validity and meaningful change thresholds of the Vitiligo Area Scoring Index (VASI). Dermatol Ther (Heidelb). 2022;12(7):1623–37.
Eleftheriadou V, Hamzavi I, Pandya AG, et al. International initiative for outcomes (INFO) for vitiligo: workshops with patients with vitiligo on repigmentation. Br J Dermatol. 2019;180(3):574–9.
Talsania N, Lamb B, Bewley A. Vitiligo is more than skin deep: a survey of members of the Vitiligo Society. Clin Exp Dermatol. 2010;35(7):736–9.
Merhi S, Salameh P, Abboud M, et al. Face involvement is reflective of global perception of extent in vitiligo patients. Br J Dermatol. 2023;189(2):188–94.
Batchelor JM, Gran S, Leighton P, et al. Using the Vitiligo Noticeability Scale in clinical trials: construct validity, interpretability, reliability and acceptability. Br J Dermatol. 2022;187(4):548–56.
Rothman M, Burke L, Erickson P, Leidy NK, Patrick DL, Petrie CD. Use of existing patient-reported outcome (PRO) instruments and their modification: the ISPOR good research practices for evaluating and documenting content validity for the use of existing instruments and their modification PRO task force report. Value Health. 2009;12(8):1075–83.
Medical Writing and Editorial Assistance
Writing assistance was provided by Joshua Solomon, Ph.D., an employee of ICON (Blue Bell, PA, USA), and was funded by Incyte Corporation (Wilmington, DE, USA), in accordance with Good Publication Practice (GPP) guidelines.
Funding
Funding for this research and the Rapid Service Fee was provided by Incyte Corporation (Wilmington, DE, USA).
Author information
Authors and Affiliations
Contributions
Amit G. Pandya, Theresa Amoloja, Kristen Bibeau, Dana DiBenedetti, Katherine Kosa, Kathleen Butler, Deanna Kornacki, and Khaled Ezzedine were involved in (1) conception or design, or analysis and interpretation of data; (2) collecting the data; (3) drafting and revising the article; (4) providing intellectual content of critical importance to the work described; and/or (5) final approval of the version to be published, and therefore meet the criteria for authorship in accordance with the International Committee of Medical Journal Editors (ICMJE) guidelines. In addition, all named authors take responsibility for the integrity of the work as a whole and have given their approval for this version to be published.
Corresponding author
Ethics declarations
Conflict of interest
Amit G. Pandya has served as an investigator for Aclaris Therapeutics, Immune Tolerance Network, Incyte Corporation, and Pfizer and a consultant for AbbVie, Arcutis, Avita Medical, Immune Tolerance Network, Incyte Corporation, Pfizer, Thalocan, TWi, Viela Bio, Vimela, Villaris, Vyne and WCG/Trifecta, and holds stock options for Tara Medical and Zerigo Health. Theresa Amoloja and Deanna Kornacki are employees and shareholders of Incyte Corporation. Kristen Bibeau (currently an employee at Moderna) and Kathleen Butler (currently an employee at Astria Therapeutics) were employees of Incyte Corporation at the time of the study and are shareholders of Incyte Corporation. Dana DiBenedetti and Katherine Kosa are employees of RTI Health Solutions, which was contracted by Incyte Corporation to conduct interviews with participants identified by a recruiting firm (Study 2). Khaled Ezzedine is a consultant for AbbVie, Incyte Corporation, La Roche-Posay, Pfizer, Pierre Fabre, Sanofi, and Viela Bio.
Ethical Approval
The TRuE-V1/TRuE-V2 study protocols (Study 1) were approved by the Western Institutional Review Board and an institutional review board or ethics committee at participating centers. Trials were conducted in accordance with the Declaration of Helsinki and adhered to study protocols, Good Clinical Practice, and applicable country-specific laws and regulations. Written informed consent or assent was provided by all patients. Study 2 was performed in accordance with the Declaration of Helsinki and in adherence to the study protocol and local regulatory requirements. Prior to the start of each interview, participants provided verbal informed consent (for adult interviewees) or assent with parental permission (for adolescent participants) and could withdraw consent at any time. The study protocol was approved by the RTI Institutional Review Board.
Consent to Participants
The authors thank the patients and their families for their participation in the TRuE-V1 and TRuE-V2 studies, including those who agreed to be interviewed for Study 1, and the individuals who participated in the interviews in Study 2.
Additional information
Prior Presentations: Data included in this manuscript have previously been presented at: Maui Derm for Dermatologists, Grand Wailea, Maui, HI, USA, 24–28 January 2022, with encores at the Global Vitiligo Foundation Annual Scientific Symposium, Boston, MA, USA, 24 March 2022, and the Innovations in Dermatology Spring Conference, Scottsdale, AZ, USA, 27–30 April 2022.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Pandya, A.G., Amoloja, T., Bibeau, K. et al. Assessing Participants’ Experiences with Vitiligo from Patient Interviews. Dermatol Ther (Heidelb) (2024). https://doi.org/10.1007/s13555-024-01241-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13555-024-01241-w