
Abstract
Introduction
The increased prevalence of depression is a global phenomenon, with an estimated 320 million cases worldwide. In Brazil, the World Health Organization (WHO) estimated that there are about 12 million cases or more, mainly among adult women with lower socioeconomic status, leading to a high consumption of health resources. Studies suggest a positive association of measures related to appearance care on depressive symptoms, but usually with no objective methodology. This study aimed to estimate the prevalence of depressive symptoms in adult Brazilian women with lower purchasing power and to verify the association between the intensity of symptoms and the use of makeup.
Methods
A national sample of 2400 cases from all regions of the country, drawn randomly from an online panel representative of the Brazilian population, was studied using an online questionnaire accessible via computer or smartphone, from which the frequency of use of makeup was surveyed, and the Zung Depressive Self-Rating Scale was applied for the inventory of symptoms.
Results
A prevalence of 61.4% (0.59–0.63) of depressive symptoms was identified. The association between frequent use of makeup and a lower prevalence of cases with a Zung index suggestive of mild depression was confirmed. Association between frequent use of makeup and lower intensity of depressive symptoms was also identified among cases with a Zung index suggestive of absence of depression. Additionally, an association was identified between the habit of frequent use of makeup and higher economic class as well as the younger age group.
Conclusion
The results suggest the hypothesis that use of makeup may contribute both to a lower prevalence of mild depression and less expressive symptoms when index of absence of depression is observed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In Brazil, the WHO estimates that there are around 12 million cases of depression, with studies suggesting an even higher prevalence | |
Several studies suggest a positive association between makeup use and improvement in depressive symptoms, but generally without measuring it objectively | |
This study aimed to identify the prevalence of depressive symptoms among adult women with medium-low purchasing power as well as the association between the measures obtained by applying the Zung Self-Assessment Depression Scale and the use of makeup | |
The results indicated a prevalence of > 60% of cases with a Zung index suggestive of some degree of depression | |
Associations were also found between frequent use of makeup and: (1) lower prevalence of cases with a Zung index suggestive of mild depression; (2) less expressive symptoms when observing the Zung index suggestive of absence of depression | |
The results suggest the hypothesis that the frequent use of makeup can contribute to the improvement of depressive symptoms. To evaluate this hypothetical causal relationship, our research group is conducting a study on the effect of introducing frequent use of makeup on depressive symptoms |
Introduction
According to the World Health Organization (WHO) [1], the prevalence of depression increased by 18% between 2005 and 2015, reaching 322 million people worldwide, with most cases being women. The study also indicates that the prevalence in Brazil is 5.8% of the population, 5.9% in the USA, ranging from 4.1% (Iceland) to 6.3% (Ukraine) in European countries, 5.9% in Australia and 4.2% in Japan and China. Based on the population projected for 2021 by the Brazilian Institute of Geography and Statistics (IBGE) [2] and considering the prevalence estimated by the WHO, there are about 12 million people currently diagnosed with this disorder in the country. Additionally, it is common for people of different age groups to present depressive symptoms even without a formal diagnosis of this disorder, with rates that far exceed that of the general prevalence. Considering the pandemic period of Corona virus disease (COVID-19), a systematic review of 2020 [3] indicated a prevalence of 35.5% in Asia and 32.4% in Europe, that is, far above the aforementioned estimates.
However, despite the effect of the pandemic, which varied by country, but was high in all of them [4], studies conducted before this period already indicated a prevalence higher than the estimates, such as 20.6% in the USA [5]. Studies from Brazil showed the presence of depressive symptoms in 79% (29% with mild symptoms) of medical students [6] and identified the presence of symptoms in 14.2% of elderly people [7]. A Brazilian study [8] involving 1285 men and 1722 women over 14 years of age indicated a prevalence of 28.3% of depressive symptoms (13% with mild to moderate symptoms and 15.3% with severe symptoms) with higher rates among women, people > 45 years of age and those from less favored socioeconomic classes of the population. This established a relationship between the presence of these symptoms and psychosocial aspects and, additionally, by the magnitude of the numbers, suggests a strong potential of economic impact. Depression is one of the most disabling diseases in the world, both physically and psychologically. Therefore, it is not only challenging because of its diagnosis and treatment, but also due to its considerable socioeconomic impact [9]. Programs such as “Look Good, Fell Better” [10], a private initiative that involves stimulating and guiding the use of makeup as a way to improve well-being and thereby positively impacting the quality of life of adult women with cancer, has been recognized as effective in this purpose. The profile of patients who seek help from dermatologists and cosmetic beauticians involves psychopathological issues, such as charismaphobia and others [11], perhaps as a reflection of social pressures and established aesthetic standards, but which seem to justify the growing role of an emerging area of knowledge, which is psychodermatology. However, little has been produced scientifically to measure the real impact of these procedures, especially with people from the general population. A study carried out with aesthetic professionals [11] added other evidence that care for the appearance (a clear psychosocial factor), in the perception of the professionals surveyed, improved their clients’ quality of life, which suggests but does not measure this effect. The objective of this study was to estimate the prevalence of depressive symptoms (measured by the Zung Self-Rating Depression Scale) in adult women with lower purchasing power and higher age groups residing in Brazil and to verify the association of this condition with the frequency of makeup use.
Methodology
An observational and cross-sectional study was carried out based on a nationally representative sample of the population of women aged > 30 years from socioeconomic classes B2 and C. This population was established as the object of study based on the findings of Coelho [8], indicating greater prevalence of depressive symptoms in this profile.
The socioeconomic classification was defined based on a traditional instrument, named the “Brazil Criterion” of the Brazilian Association of Research Companies (ABEP), which considers purchasing power. It is not perfect, but suitable for most situations aiming at the segmentation of the population [12]. Figure 1 presents details of the surveyed classes and their representativeness.

Representativeness of the population studied. Scheme created by the author, based on data from the Brazilian Institute of Geography and Statistics (2) and a technical document on the Brazil Criterion [12]
The sample size was calculated according to Agranonik et al. [13] by using the following precision parameters: safety of 95% and margin of error of 2%. Considering estimated proportions of 50%, which guarantees a larger sample [14], the sample size of 2400 cases was obtained using the formula presented in Fig. 2.

Formula used and sample size calculation: n = sample size; Z = critical value for the desired security level; p = expected proportion in the population; e = maximum expected error
The sampling method adopted was semi-probabilistic by quotas, with sizes that led to a distribution of elements close to the population distribution (Table 1). Electronic invitations were randomly sent to people of the targeted profile, belonging to an online panel representative of the Brazilian population and accessible to different strata of the population. The first responses received were accepted up to the limit of each quota.
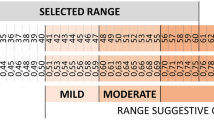
Data were collected through an online questionnaire containing the following questions: (1) frequency of makeup use (any kind) with options for a single answer presented in Table 2, where codes 4 or 5 were considered "frequent users of makeup;" (2) self-reported diagnosis of depression and others, with dichotomous answer, yes or no, considering the following diagnoses from a physician: depression, anxiety, bipolar disorder, obsessive-compulsive disorder (OCD), panic disorder, mood disorder and social phobia; (3) use of drugs that act on the central nervous system, prescribed or not by a doctor, considered by the volunteers as “soothing,” to “facilitate sleep” or any other for “some emotional problem, with dichotomous answer, yes or no, and the name of the medicines in positive cases, which were coded and grouped according to the active ingredient; (4) inventory of depressive symptoms using the Zung Self-Rating Depression Scale (ZSDS)Footnote 1 [15–22], translated and validated for Brazilian Portuguese in 2010 [23], providing an index that suggests the absence or existence of mild, moderate or severe depression. It is a public domain instrument for screening for depression in adults [16]; it was more sensitive than theDepression Anxiety Stress Scale (DASS) [25]. The answers are based on a Likert scale (a little of the time/some of the time/a good part of the time/most of the time) of 20 feelings and emotions, 10 negative (points from 1 to 4) and 10 positive (points from 4 to 1). In the end, it totals a raw score that can vary between 20 and 80. The Raw Score is then divided by 80, generating an index that varies between 0.25 to 1 (or 25 to 100 as a percentage). We used the decimal form of the index, aiming to minimize the risk of confusing its percentage form with the raw score. Table 3 illustrates the conversion of the raw score into an index and provides the interpretation of the results.
For analysis, the data were weighted to be adjusted to the distribution of the population according to the sociodemographic groups considered (age, socioeconomic class and region of the country combined), according to Bussab [26]. Details are presented in Table 4.
Data analysis was performed using SPSS v.21 software. Hypothesis tests were conducted with a significance level of 5%. The dataset generated during the current study is available at: https://1drv.ms/u/s!Ao2FRgWr7T6YgpBriwtSd-93EHYHoA?e=GvL3SI
The study was carried out exclusively by the Federal University of São Paulo (UNIFESP) and in accordance with the Declaration of Helsinki of 1964 and its subsequent amendments, having been approved by the Research Ethics Committee of the Federal University of São Paulo (UNIFESP)—Opinion No. 3,912,288. Prior to any study activity, all participants agreed to participate and authorized the dissemination of their results, signing the informed consent form.
Results and Discussion
Figure 3 shows a prevalence of 61.4% (0.56–0.63) of cases with indexes suggestive of depression in the surveyed population.

Distribution of participants according to the Zung index. IC95 = 95% confidence interval
Based on the Zung indices, and even considering that data collection was carried out during the COVID-19 pandemic, whose impact on Brazil was estimated at 20% [4], the results suggest a higher prevalence than previously estimated [1]. The prevalence of severe cases is close to that estimated by Coelho [8], but not the sum of mild and moderate cases (9% in class B2 and 11% in class C) compared to about 47% in the current study.
According to age groups, significant difference was observed as indexes suggestive of depression among participants aged 30 to 44 years was greater than for subgroup aged 45 years and over, as illustrated in Fig. 4.

Distribution of participants by the ranges of the Zung index, according to age group. IC95 = 95% confidence interval
Lira Correia [18] discussed depression in women from the perspective of behavior analysis, socio-environmental aspects and pregnancy based on the prevalence of 10%–15% for postpartum depression, reported in several countries, involving in this discussion the influence of hormonal changes, weight gain, changes in routine, etc. Our data allow us to consider that the greater proportion of cases with index suggestive of depression in the age group of 30 to 44 years may be related to higher comparative fertility rate [19]. Another possibility comes from the impact of the COVID-19 pandemic on the prevalence of depression: lower in older age groups than in younger ones [4].
Regarding the socioeconomic classes, the proportion of cases with indexes suggestive of moderate depression was significantly higher in class B2, with high purchasing power (Fig. 5).

Distribution of participants by the ranges of the Zung index, according to the socioeconomic classes. IC95 = 95% confidence interval
Contrarily, Coelho's survey [8] suggested a slightly higher prevalence in the lower socioeconomic class (9.2% in class B2 and 11.3% in class C). However, the data were not segmented by gender or age group, not allowing a comparison with our results. Likewise, the impact of the COVID-19 pandemic might have been responsible for this different result.
An association was identified (contingency coefficient: 0.99; P < 0.05; Spearrman correlation coefficient: 0.435; P < 0.01) between the index suggestive of depression and self-reported diagnosis of depression, as shown in Fig. 6. Notably, the proportion of participants who self-reported the diagnosis of depression increased in parallel with higher Zung index suggestive of severe depression.

Self-reported depression according to the Zung index ranges. IC95 = confidence interval (95%) in relation to the percentage of cases WITH self-reported depression
Considering the cases with index of mild depression, only 26% (0.23–0.30) reported that diagnosis. Even considering the 70.2% (0.66–0.73) of cases that mentioned at least one diagnosis, about 30% remain without any self-report. These numbers provide the dimension of the potential proportion of cases with index suggestive of mild depression, but not diagnosed. Table 5 shows that when analyzing cases with moderate index of depression, the percentage of participants potentially without a diagnosis varies from 16.9% (at least one diagnosis) to an expressive 61.2% (only self-report). In addition, even in cases with index of severe depression, the non-diagnosed cases vary from 5.8% (any diagnoses) to 29.2% (specific mention of depression).
In a review of the Brazilian Medical Association's (AMB) guidelines on depression treatment [20], the authors state that "in primary care services and other general medical services, 30% to 50% of cases of depression are not diagnosed." Based only on self-reports of depression, our data are aligned with the reported by Fleck and colleagues [20] when considering cases with indexes suggestive of moderate to severe depressive disorder. Nevertheless, for mild depression this alignment does not seem to occur as there is greater potential for non-diagnosis.
When asked about the current or past use (90 days) of medication (prescribed or not by a doctor), 26.5% (0.25–0.28) of participants responded positively. Table 6 shows that passionflower was the most frequently identified active ingredient, except among participants with rates suggestive of severe depression, in which clonazepam and fluoxetine stood out.
An association was identified (contingency coefficient: 0.98; P < 0.05) between the proportion of medication users and the Zung index ranges and, as shown in Fig. 7, more frequent use of medicines in the subgroups with higher Zung index.

Percentage of participants who reported current or previous use (90 days) of medication, according to the Zung index ranges. IC95 = confidence interval (95%) in relation to the percentage of cases WITH use of medications
A study on the use of psychotropics (not including herbal medicines) in primary health care [21] indicated a prevalence of 25.8% of use, identifying fluoxetine and amitriptyline as the most prescribed antidepressants and clonazepam and diazepam as the most prescribed drugs among the benzodiazepines. The authors did not include herbal medicines and a comparable sample of participants, so it is not possible to say that their results were in line with ours, although they are comparable when antidepressants and benzodiazepines are considered. Research on the consumption of passionflower and valerian [22] reported growth in their consumption in the period of the COVID-19 pandemic, which may contribute to explain the prominence of passionflower in the list of active ingredients we have identified.
Considering the frequent use of makeup according to socioeconomic classes, an association was identified (contingency coefficient: 0.66; P < 0.05) between “frequent use” and “socioeconomic class,” as shown in Fig. 8. A higher proportion of “frequent use” was detected among participants in class B2, with high purchasing power, compared to class C.

Distribution of participants with and without frequent use of makeup, according to the socioeconomic classes. IC95 = 95% confidence interval in relation to the percentage of cases WITH frequent use of makeup
A study on the factors that lead low-income women to consume beauty products [23] revealed that it is one of the ways to “raise self-esteem, constantly shaken by financial constraints, which puts them at a permanent disadvantage" and that they also "seek, through beauty, to obtain respect from hierarchically superior social classes, since appearance seems to be an effective way to reduce their perception of discrimination because they are poor." Our results established a relationship between purchasing power and frequency of makeup use, which confirms the hypothesis raised by Strehlau and colleagues [24]. As stated by Livramento and colleagues [23], these findings reflect another inequality that imposes additional difficulties to the less favored classes, restricting access to a resource with potential to contribute to well-being. The hypothesis of less frequent use of makeup due to depressive symptoms was not addressed in this study, thus leaving the opportunity for future studies on the subject.
When analyzing the proportion of cases with or without frequent use of makeup according to the Zung index ranges, an association was identified between the variables (contingency coefficient: 0.23; P < 0.05). Figure 9 shows a significant lower prevalence of participants with an index suggestive of mild depression among frequent users 23.2% (0.21–0.26) vs. 29.4% (0.27–0.32), relative risk = 0.79 (0.69–0.90).Footnote 2

Distribution of participants with and without frequent use of makeup, according to Zung index ranges. IC95 = 95% confidence interval
Multinomial logistic regression indicated a 25% chance (0.08–0.39) of lower index (P < 0.05) suggestive of mild depression compared to cases with an index suggestive of absence of depression. The analysis of cases with indexes suggestive of moderate or severe depression did not result in statistically significant indicators.
The finding of the lack of association between frequent use of makeup and indices suggestive of moderate or severe depression, in addition to not diminishing the importance of the association with the prevalence of cases with indices suggestive of mild depression, is in line with the fact that moderate and severe cases typically are treated with medication [25]; therefore, an association with frequent use of makeup was not expected.
By regrouping the total number of participants according to the self-report of diagnoses and/or use of medications, the same difference was identified, as illustrated in Fig. 10.

Redistribution of participants with or without frequent makeup use according to the Zung index ranges and specified subgroups. IC95 = confidence interval (95%) for the percentage of cases with suggestive index of mild depression
The analysis by Pais Ribeiro [26] stated that higher values on the Zung index were indicative of greater symptoms. Considering the participants with index of absence of depression, no self-report of diagnosis and/or use of medication, a statistically significant difference was identified when comparing the means of the Zung index between frequent users and non-users of makeup, as shown in Fig. 11.

Comparison between the means of the Zung index according to the frequency of makeup use, obtained from the specified profile of participants. IC95 = confidence interval (95%) of the means obtained. S = standard deviation
Limitations
The study involved a significant population, but equivalent to about 25% of the female population in Brazil, thus leaving open the opportunity to expand this investigation to other profiles involving, for example, other segments of the general population or even specific profiles with potential to benefit from the effects described by this research. No cases of "body image disorders" were identified in the surveyed sample, despite having an open question about diagnoses received from a physician. However, the self-report of these diagnoses may contain distortions, and therefore this possibility cannot be ruled out.
Conclusion
A prevalence of 61.4% (0.59–0.63) of depressive symptoms was identified in women according to the level of severity as follows: mild depression: 26.2% (0.24 to – 0.28); moderate: 20.9% (0.19–0.23); severe: 14.3% (0.13–0.16). An association was found between frequent use of makeup and a lower prevalence of cases with index suggestive of mild depression, with or without medication use and self-report of this diagnosis. Additionally, in cases without self-report of depression, use of medication and an index suggestive of absence of depression, a significantly lower mean of Zung indexes was detected among frequent makeup users. The results suggest the hypothesis that use of makeup may contribute to both a lower prevalence of mild depression and less expressive symptoms when index of absence of depression is observed. To assess this hypothetical causal relationship, our research group is conducting a study on the effect of introducing regular makeup use on depressive symptoms.
Notes
The ZSDS scale was also chosen because it is widely used (it is the second most cited self-assessment scale in the literature [27]—behind only "Beck Depression Inventory" (BDI), applied by self-assessment (this is not the case for the Hamilton-D, for example), and it is a public domain instrument (this is not the case for the BDI).
A relative risk < 1 indicates a protective factor or a lower risk of event development in the exposed group [28].
References
OPS. Depresión y otros trastornos mentales comunes. Organ Panam la Salud Organ Mund la Salud [Internet]. 2017;1–24. Available from: http://iris.paho.org/xmlui/bitstream/handle/123456789/34006/PAHONMH17005-spa.pdf
Brasil. IBGE. Estimativa da População [Internet]. Agência IBGE. 2021. p. 1. Available from: https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/31461-ibge-divulga-estimativa-da-populacao-dos-municipios-para-2021
Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Global Health. 2020;16(1).
Santomauro DF, Mantilla Herrera AM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–12.
Hasin DS, Sarvet AL, Meyers JL, Saha TD, June Ruan W, Stohl M, et al. Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States Supplemental content. JAMA Psychiatry [Internet]. 2018;75(4):336–46. Available from: https://jamanetwork.com/
Rezende CHA de, Abrão CB, Coelho EP, Passos LB da S. Prevalência de sintomas depressivos entre estudantes de medicina da Universidade Federal de Uberlândia. Rev Bras Educ Med [Internet]. 2008;3(32):315–23. Available from: https://www.scielo.br/j/rbem/a/svDydRQM5hwj6J9dBN9PKBG/?lang=pt
Mendes-Chiloff CL, Lima MCP, Torres AR, Santos JLF, Duarte YO, Lebrão ML, et al. Depressive symptoms among the elderly in são paulo city, brazil: Prevalence and associated factors (SABE study). Rev Bras Epidemiol. 2018. https://doi.org/10.1590/1980-549720180014.supl.2.
Coelho CLS, Alexandre JSC, Santos JLF, Pinsky I, Zaleski M, Caetano R, et al. Higher prevalence of major depressive symptoms in Brazilians aged 14 and older. Rev Bras Psiquiatr. 2013;35(2):142–9.
Kessler RC. The costs of depression. Psychiatr Clin North Am [Internet]. 2012;35(1):1–14. https://doi.org/10.1016/j.psc.2011.11.005.
Taggart LR, Ozolins L, Hardie H, Nyhof-Young J. Look good feel better workshops: A big lift for women with cancer. J Cancer Educ. 2009;24(2):94–9.
Black USP. Beauty therapy as emotional labour. Sociology [Internet]. 2001;35(4):913–31. Available from: https://journals.sagepub.com/doi/https://doi.org/10.1177/0038038501035004007
ABEP AB de empresas de P. Alterações na aplicação do Critério Brasil, válidas a partir de 01/06/2021 [Internet]. Critério Brasil. 2021 [cited 2021 Aug 10]. p. 1–7. Available from: https://www.abep.org/criterio-brasil
Agranonik M, Hirakata VN. Sample size calculation: proportions. Rev HCPA [Internet]. 2011;31(1):382–8. Available from: https://www.lume.ufrgs.br/handle/10183/159229
Raggio Luiz R, Magnanini MMF. A Lógica Da Determinação Do Tamanho Da Amostra Em Investigações. Cad Saúde Coletiva [Internet]. 2000;8:9–28. Available from: https://edisciplinas.usp.br/pluginfile.php/4116370/mod_resource/content/1/DeterminaçãoamostraRonir2000_2.pdf
Zung WWK. Self-Rating Depression. Arch Gen Psychiatry. 1965;
Lakkis NA, Mahmassani DM. Screening instruments for depression in primary care: A concise review for clinicians. Postgrad Med. 2015;127(1):99–106.
Dunstan DA, Scott N. Assigning clinical significance and symptom severity using the zung scales: levels of misclassification arising from confusion between index and raw scores. Depress res treat [Internet]. 2018;2018:13. Available from: https://doi.org/10.1155/2018/9250972
Lira Correia K, Borloti E. Mulher e depressao: uma análise comportamental-contextual. Acta Comport Rev Lat Análisis Comport. 2011;19(3):359–73.
UNFPA Brasil. Fecundidade e dinâmica da população brasileira. 2018. 8 p.
Fleck M, Berlim M, Lafer B. Revisão das diretrizes da Associação Médica Brasileira para o tratamento da depressão. Rev Bras [Internet]. 2009;31(Supl I):7–17. Available from: http://www.scielo.br/pdf/rbp/v31s1/a03v31s1.pdf
Borges TL, Miasso AI, Vedana KGG, Telles Filho PCP, Hegadoren KM. Prevalência do uso de psicotrópicos e fatores associados na atenção primária à saúde. Acta Paul Enferm. 2015;28(4):344–9.
Pessolato JP, Rodrigues S de P, Souza DA, Boiati RF. Avaliação do consumo de Valeriana e Passiflora durante pandemia COVID-19/ Assessment of Valerian and Passiflora consumption during a pandemic COVID-19. Brazilian J Heal Rev. 2021;4(2):5589–609.
Livramento MN, Hor-Meyll LF, Pessôa LAG de P. Valores que motivam mulheres de baixa renda a comprar produtos de beleza. Gestão Humana e Soc [Internet]. 2013;14(1). Available from: http://web.a.ebscohost.com.recursosbiblioteca.eia.edu.co/ehost/detail/detail?vid=2&sid=15e476f4-5a89-4595-9bac-477ccf453a68%40sessionmgr4003&hid=4204&bdata=Jmxhbmc9ZXMmc2l0ZT1laG9zdC1saXZl#db=fua&AN=88930164
Strehlau VI, Claro DP, Laban Neto SA. A vaidade impulsiona o consumo de cosméticos e de procedimentos estéticos cirúrgicos nas mulheres? Uma investigação exploratória Rev Adm. 2015;50(1):73–88.
Cuijpers P, Quero S, Dowrick C, Arroll B. Psychological treatment of depression in primary care: recent developments. Curr Psychiatry Rep. 2019. https://doi.org/10.1007/s11920-019-1117-x.
Pais Ribeiro JL. Avaliação em Psicologia da Saúde: Instrumentos Publicados em Português. Coimbra: Quarteto; 2007. 350 p.
Aros MS, Yoshida EMP. Estudos da depressão: instrumentos de avaliação e gênero. Bol Psicol. 2009;59(130):61–76.
Tramujas L. Qual é a diferença entre medida relativa e absoluta em estudos médicos?. [Internet]. Portal PEBMED. 2018 [cited 2022 May 29]. Available from: https://pebmed.com.br/qual-e-a-diferenca-entre-medida-relativa-e-absoluta-em-estudos-medicos/#:~:text=Um risco relativo menor que,aumentado de desenvolver determinado evento.
Acknowledgements
We are grateful to the study participants who, with their best efforts, made it possible to obtain the results reported here.
Funding
This study was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo—FAPESP, Process 2020/01563–2. No funding or sponsorship was received for this study or publication of this article.
Medical Writing or Editorial Assistance
No medical writing or editorial assistance was received during the writing of this article.
Author Contributions
Marcos C.Veçoso: Conceptualization, Methodology, Formal analysis, Project administration, Writing—original draft. Edileia Bagatin: Writing—review, editing and validation. Fernando L.A. Fonseca: Conceptualization, Funding acquisition. Newton Andreo-Filho: Conceptualization, Writing—review and editing. Patrícia S. Lopes: conceptualization, writing—review and editing. Vânia R. Leite-Silva: Conceptualization, Methodology, Validation, Writing—review and editing, Supervision, Funding acquisition.
Prior Publication
This study has not been previously published.
Disclosures
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Compliance with Ethics Guidelines
The study was carried out exclusively by the Federal University of São Paulo (UNIFESP) and carried out in accordance with the Declaration of Helsinki of 1964 and its subsequent amendments, having been approved by the Research Ethics Committee of the Federal University of São Paulo (UNIFESP)—Opinion No. 3,912,288. Prior to any study activity, all participants agreed to participate and authorized the dissemination of their results, signing the informed consent form.
Data Availability
The dataset generated during the current study is available at: https://1drv.ms/u/s!Ao2FRgWr7T6YgpBriwtSd-93EHYHoA?e=GvL3SI.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Veçoso, M.C., Bagatin, E., Fonseca, F.L.A. et al. Association Between Frequent Use of Makeup and Presence of Depressive Symptoms—Population-Based Observational Study, Including 2400 Participants. Dermatol Ther (Heidelb) 13, 1083–1097 (2023). https://doi.org/10.1007/s13555-023-00911-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-023-00911-5