
Abstract
Background and Objective
Omeprazole is a proton pump inhibitor that is used in acid suppression therapy in infants. Infants cannot swallow the oral tablets or capsules. Since, infants require a non-standard dose of omeprazole, the granules or tablets are often crushed or suspended in water or sodium bicarbonate, which may destroy the enteric coating. In this study we explore the efficacy and pharmacokinetics of rectally administered omeprazole in infants with gastroesophageal reflux disease (GERD) due to esophageal atresia (EA) or congenital diaphragmatic hernia (CDH) and compare these with orally administered omeprazole.
Methods
Infants (6–12 weeks postnatal and bodyweight > 3 kg) with EA or CDH and GERD were randomized to receive a single dose of 1 mg/kg omeprazole rectally or orally. The primary outcome was the percentage of infants for whom omeprazole was effective according to predefined criteria for 24-h intraesophageal pH. Secondary outcomes were the percentages of time that gastric pH was < 3 or < 4, as well as the pharmacokinetic parameters.
Results
Seventeen infants, 4 with EA and 13 with CDH, were included. The proportion of infants for whom omeprazole was effective was 56% (5 of 9 infants) after rectal administration and 50% (4 of 8 infants) after oral administration. The total reflux time in minutes and percentages and the number of reflux episodes of pH < 4 decreased statistically significantly after both rectal and oral omeprazole administration. Rectal and oral administration of omeprazole resulted in similar serum exposure.
Conclusions
A single rectal omeprazole dose (1 mg/kg) results in consistent increases in intraesophageal and gastric pH in infants with EA- or CDH-related GERD, similar to an oral dose. Considering the challenges with existing oral formulations, rectal omeprazole presents as an innovative, promising alternative for infants with pathological GERD.
Clinical Trial Register
ClinicalTrials.gov Identifier: NCT00226044.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
A single rectal omeprazole dose results in consistent increases in intraesophageal and gastric pH in infants with gastroesophageal reflux disease due to congenital malformations. |
A dose of 1 mg/kg rectal omeprazole in infants results in rapid exposure in the therapeutic range. |
Rectal omeprazole presents as an innovative, promising alternative for infants with gastroesophageal reflux disease. |
1 Introduction
Gastroesophageal reflux (GER) is a very common and self-limiting condition in infancy. If GER is accompanied with ‘troublesome’ symptoms or complications, such as esophagitis, poor weight gain, or respiratory complications, it is defined as gastroesophageal reflux disease (GERD) [1]. The incidence of GERD is estimated to be around 10% in healthy infants, whereas it increases to 50–90% in infants with birth defects, such as esophageal atresia (EA) or congenital diaphragmatic hernia (CDH) [2,3,4]. In the latter, life-threatening complications, such as aspiration or pneumonia, may occur. For infants with GERD who do not improve with conservative treatment, an empiric trial using acid suppression therapy with proton pump inhibitors (PPIs) can be considered [5, 6]. Omeprazole, a frequently used PPI, is commercially available in gelatin capsules or tablets containing enteric-coated granules to prevent inactivation of omeprazole by exposure to gastric acid [7,8,9].
The currently available omeprazole formulations do not enable exact dosing in neonates and infants, as the average starting dose of 3 mg in a neonate (based on a recommended dose of 1 mg/kg/day) will be much lower than the lowest available solid formulation (10 mg/dose). Since infants cannot take solid oral formulations, these formulations are either crushed which damages the enteric-coated granules or suspended in water or sodium bicarbonate. In addition, infants can chew on the granules and this will also damage the coating [10, 11]. Moreover, many infants with GERD and an underlying disease like EA or CDH need enteral feeds by a gastric tube. The suspended granules are notorious for causing a gastric tube blockage [9]. Finally, the commercially available omeprazole suspensions are, in our opinion, not a good alternative for infants because it is unclear if the amount of sodium bicarbonate, added to buffer the acid stomach content, is effective and safe in this population. Consequently, the oral bioavailability of currently available oral omeprazole formulations may be unpredictable and result in variable degrees of systemic drug exposure, which may explain the low effectiveness reported [5, 6]. In addition, the practical issues related to oral omeprazole use, e.g., crushing or suspending and gastric tube blockage present an additional burden to parents and children who are already overwhelmed due to the (underlying) disease.
To overcome the limitations associated with the current oral omeprazole formulations, alternative formulations are needed. Based on studies in healthy adult volunteers [12, 13] we developed age-appropriate omeprazole suppositories of good quality and stability [12,13,14]. In the current pilot study, we aimed to explore the efficacy and pharmacokinetics of rectally administered omeprazole in infants with GERD due to EA or CDH and compare these with orally administered omeprazole.
2 Methods
2.1 Study design
This study was an open-label randomized pilot trial to study the efficacy of a single orally or rectally administered 1 mg/kg dose of omeprazole in infants with GERD due to EA or CDH. The study was performed at the Departments of Pediatric Surgery at the Erasmus MC Sophia, Rotterdam, The Netherlands. The protocol was approved by the institutional review board of the Erasmus Medical Centre Rotterdam (ClinicalTrials.gov Identifier: NCT00226044). All parents gave written informed consent for their infant to be involved in the study.
2.2 Standard of care
The standard of clinical care protocol for GERD prescribed omeprazole 1 mg/kg with or without Gaviscon® or domperidone in all infants after neonatal surgical repair for EA or CDH, as soon as enteral feeding was started. Between the age of 6 and 12 weeks postnatally, 48-h pH monitoring was performed to assess the severity of acid reflux and the impact of a single dose of omeprazole. The first 24-h pH monitoring was performed after the omeprazole was stopped for 4 days and the domperidone and Gaviscon® (where relevant) for 2 days. This wash-out period is a standard procedure before pH monitoring is performed. The omeprazole medication was administered as standard of care after the wash-out before a second 24-h pH monitoring was performed.
2.3 pH Monitoring
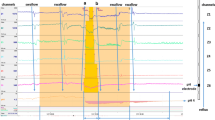
A portable pH meter (Orion, Medical Measurement Systems) with a two-tip measuring probe was used. The measuring tips were calibrated before and after the measurement. The upper probe measured the pH in the esophagus and the lower probe measured the pH in the stomach. A chest X-ray confirmed the position of the two probes. The pH analysis was based on automated pH analysis and the measured values were compared with the Vandenplas criteria [16]. Evaluation of the pH measurements was performed by trained gastroenterologists.
2.4 Inclusion and Exclusion Criteria
Infants were eligible for the study if they were 6–12 weeks postnatal, weighed > 3 kg, had undergone surgical repair for EA or CDH, showed clinical GERD, and were to undergo 48-h pH measurements. Initially, all infants were randomized to study medication after the first 24-h pH measurement. After inclusion of the first 8 infants, however, only 2 fulfilled the criteria of GERD during the first 24-h pH measurement, so the protocol was changed. Only infants whose first 24-h pH measurement showed GERD were eligible to receive the study medication. Infants were excluded if they were allergic to omeprazole, had participated in other interventional trials, or had used medications known to interact with omeprazole.
2.5 Sample Size and Randomization
We planned to include 20 infants in this pilot study, with 10 receiving omeprazole rectally and 10 orally. The pediatric gastroenterologist decided if a patient was eligible for inclusion. After inclusion, allocation was by means of the sealed envelope method.
2.6 Omeprazole Dose
At the start of the second day (t 24–48 h) of pH measurements, the infants received a single dose of study medication—1 mg/kg of orally or rectally administered omeprazole. The suppositories (3–10 mg, rounded to whole milligrams) were prepared as described previously [12]. Uniformity of mass was checked and the content of uniformity as well as the stability were determined with a validated quantitative high-performance liquid chromatography–ultraviolet (HPLC–UV) method. The oral suspension was also custom-made. Briefly, commercially available 40 mg omeprazole capsules were opened, and the precise amount of omeprazole granules was measured (3–10 mg) and deposited in new capsules. On the day of administration, the capsule was opened and the granules were dissolved in 5 ml of water. After pH measurements, the patients continued with the rectally or orally administered study omeprazole at 1 mg/kg for approximately 6 weeks.
2.7 Blood Sampling for Pharmacokinetics
During the second 24-h pH monitoring, IV access was obtained to draw up to 10 blood samples of 1 ml (2 × 0.5 ml) for pharmacokinetic analysis, at the following time points—pre-administration, and at 30, 60, 90, 120, 150 min, and 3, 4, 6 and 8 h after omeprazole administration. The blood samples were centrifuged and stored in a freezer (− 80 °C) until the serum samples were analyzed for concentrations of the active drug omeprazole (OME) and the non-active metabolites hydroxy-omeprazole (OH-OME) and omeprazole-sulphone (OME-S) in the laboratory of the pharmacy of the Hague hospitals, using a validated HPLC with diode array detection method [15].
2.8 Outcomes
The primary outcome was the percentage of infants for whom omeprazole was effective. Efficacy was based on 24-h intraesophageal pH in 509 healthy infants and defined as the following parameters being within normal values for age (Supplemental Table 1)—number of episodes of pH < 4, percentage of time with pH < 4, number of episodes of pH < 4 and longer than 5 min, and longest reflux episode [16]. The secondary outcomes were the percentage of time with intragastric pH > 3, the percentage of time with intragastric pH > 4, and analysis of the pharmacokinetic parameters.
2.9 Pharmacokinetic Analysis
The maximal concentrations of OME, OH-OME, and OME-S in serum (Cmax) and the time to reach Cmax (Tmax) were visually extracted from the serum concentration versus time curves. The area under the curve (AUC) from time zero to the last sampling time point (AUC0–t) was calculated using the log-linear trapezoidal method. The apparent volume of distribution (Vd/F) and apparent serum clearance (CL/F) were calculated for OME only by using standard non-compartmental techniques. All pharmacokinetic parameters derived from individual patients were estimated using Excel PKsolver add-in software [17].
The criterion for excluding study patients from all pharmacokinetic analyses was fewer than four blood samples. If CL/F, Vd/F, or half-life (t1/2) were not predicted because of non-negative estimated λz, they were excluded for the CL/F, Vd/F, or t1/2 analyses, respectively. If the part of AUC0–∞ that was extrapolated beyond the last observation was > 20% of the actual AUC0–t, the AUC0–∞ was excluded from the analyses, as it would introduce unreliable overestimation of the AUC0–∞.
2.10 Statistical Analysis
All data were analyzed using SPSS 25. Standard descriptive statistics were used to describe demographic and clinical characteristics. Due to the small numbers and non-normal distributions, all continuous variables were summarized in medians with ranges. Differences between groups were analyzed using Mann–Whitney U tests, while differences in parameter values before and after omeprazole administration were analyzed using Wilcoxon Signed Ranks tests. The level of significance was set at p < 0.05.
3 Results
3.1 Demographics
We screened 99 infants for inclusion, of whom 65 were excluded for various reasons (Fig. 1). Of the 34 infants who underwent pH monitoring, 17 received study medication. The trial was terminated early for logistic and financial reasons in April 2016. In total, 9 infants received omeprazole rectally and 8 orally. The rectal omeprazole group consisted of 7 boys (78%) and 2 girls (22%), whereas the gender distribution was 50%:50% in the oral omeprazole group. Birth weight, postnatal age at surgery, and age at pH measurement did not differ between the two groups (Table 1).

Flow chart of screening and randomization of infants
3.2 Primary Outcome
3.2.1 Esophageal pH
The proportion of patients for whom omeprazole was effective, as defined above, was 56% (5 out of 9 patients) after rectal and 50% (4 out of 8 patients) after oral omeprazole (Table 2). In both groups and when dosing before and after were compared, the total reflux time in minutes and percentages and the number of reflux episodes of pH < 4 showed a statistically significant decrease (p ≤ 0.015) after administration of omeprazole (Table 2). The number of reflux episodes of pH < 4 longer than 5 min (p = 0.345) and the longest reflux period (p = 0.097) did not seem to decrease as much in the rectal omeprazole group as they did in the oral group (p ≤ 0.012). The patients in the rectal omeprazole group had better baseline values for these parameters compared to the oral group before omeprazole administration (e.g., longest median reflux periods of 4.9 vs 14.2 min, respectively). Supplemental Figures 1A and 1B show the number of reflux episodes and the total reflux time (%) per 24 h per individual infant.
3.3 Secondary Outcomes
3.3.1 Gastric pH
The percentage of time with pH > 4 showed a statistically significant increase after both oral and rectal omeprazole administration (Table 2). Furthermore, the percentage of time with pH > 3 also showed a statistically significant increase (p = 0.018) after oral administration, but less so after rectal administration, p = 0.069 (Table 2). The patients in the rectal omeprazole group already had better baseline values for these parameters than the patients in the oral group.
3.4 Pharmacokinetics
From 5 infants (4 rectally and 1 orally administered omeprazole), blood was collected to estimate the pharmacokinetic parameters of omeprazole and its metabolites (Table 3). We were not able to collect pharmacokinetic data from all included infants as not all parents provided consent for the pharmacokinetic sub-study and in the remaining infants the small-bore peripheral intravenous line did not allow sampling on all occasions or was not maintained throughout the full sampling time. The concentration time curves of OME and its metabolites are shown in Fig. 2a, b. The median (range) AUC0–∞ was 57.7 (13.3–64.8) and 50.5 mg/L·min after rectal and oral dosing, respectively. The median (range) half-life was 65 (19–137) min after rectal and 38 min after oral dose administration. For rectal omeprazole, the median (range) Cmax was 0.3 (0.3–0.4) mg/L which was reached at 96.5 (60–167) min. The oral Cmax was 1.0 mg/L which was reached at 123 min.

Serum concentration profiles of omeprazole (OME), hydroxy-omeprazole (OH-OME) and omeprazole sulphone (OME-S) after administration of rectal omeprazole 1 mg/kg in 4 patients (a) and oral omeprazole 1 mg/kg in 1 patient (b)
3.5 Safety
No study-specific adverse events were reported during the study period.
4 Discussion
Our data show that a single rectal omeprazole dose results in a consistent increase in intraesophageal and intragastric pH in infants with congenital malformation-related GERD. Considering the challenges with existing oral PPI formulations, rectal omeprazole presents as an innovative, promising alternative for infants with GERD.
Our data are in line with adult studies showing adequate systemic exposure and gastric acid suppression after a single 1 mg/kg dose of rectal omeprazole [12, 13]. Our current data suggest that rectal omeprazole is as efficacious as oral omeprazole. It may be even more efficacious in regular clinical care settings, as in our study the oral omeprazole could be more precisely dosed at approximately 1 mg/kg than in regular clinical care, as customized capsules were prepared. For regular clinical care, the smallest commercially available formulation is 10 mg, which needs to be manipulated by parents or care-givers to enable administration to infants, resulting in imprecise dosing. Hence, the efficacy of oral omeprazole in real-life clinical care may be more variable than in the current study, providing an additional rationale for rectal administration. Moreover, the reduction in burden to parents and children by reducing the logistic challenges of dosage form manipulations and gastric tube replacement often needed for tube blockage by the granules is a major benefit of the suppository.
Although only approximately half of the patients reached the primary endpoint (no GER, based on combined intraesophageal pH indices), we observed that total reflux time, the number of reflux episodes of pH < 4, and the longest reflux period decreased considerably in both the oral and rectal omeprazol groups. Only the latter did not show a statistically significant decrease in the rectal group, which was most likely due to the already short reflux periods before omeprazole administration in this group. In addition, it is known that the maximum omeprazole effect is only reached after several days of administration (in adults) [18]. As we measured pH after a single dose only, this may explain why we observed large improvements in pH indices but not all patients reaching the primary endpoint. We would have preferred a multi-dose study, but the current study was ethically only feasible in the context of existing clinical care, namely two 24-h pH measurements on consecutive days, with and without omeprazole. An additional hospital visit (for ambulatory patients) and a second insertion of the pH probe (for all patients) would have been ethically unacceptable, as the additional burden to infants would not outweigh the potential benefit of the study. Nevertheless, we think that the data on a single dose of omeprazole are very informative as we observed a large reduction in esophageal and gastric pH. In a previous study in older critically ill infants (5–27 months), receiving approximately 0.5 mg/kg omeprazole orally, gastric pH was > 4 for approximately 45% of the time, and in those receiving 1 mg/kg for approximately 90% of the time [18]. Our data are also in line with a recent dose-finding study in neonates, where 24-h pH monitoring starting 48–96 h after omeprazole initiation, supported optimal acid reduction at 1 mg/kg daily oral administration [19].
We were able to estimate pharmacokinetics in a sub-set of patients. In the four patients receiving rectal omeprazole, the median (range) Tmax of 97 (60–167) min was in line with the adults study by Choi et al. (mean ± SE Tmax 129 ± 20 min) [12]. In addition, the Tmax of oral omeprazole (123 min) from the one patient with pharmacokinetic data was also in the range as reported for adults and children aged 1–18 years (Tmax 60–360 h) [18, 20]. Elimination half-life was similar in our patients after rectal and oral administration compared to the study by Andersson et al. in a cohort of children aged 1–6 years [20]. Interestingly, Choi et al. showed similar pharmacokinetics for rectal and oral omeprazole in adults, with less inter-individual variation after rectal administration [12]. To the best of our knowledge, oral pharmacokinetic data from the infant population (term infants, 1–12 months of age) are lacking so far. Individual pharmacokinetics are also of great importance. For example, one of the infants in this study no longer had an active omeprazole level after 100 min. In this infant, omeprazole was not effective at all. Moreover, another patient showed very high metabolite levels. The interplay of age and genotype on CYP2C19 activity, the main drug metabolizing enzyme involved in omeprazole disposition, may have contributed to these observations [21].
Our study had some limitations. First, this was only a small pilot study, with 17 patients and 5 patients with pH and pharmacokinetic data, respectively. The small sample size of this pilot study did not allow testing the superiority of rectal over oral omeprazole in infants and likely also explains the difference in baseline values between the groups. Although we planned to study the clinical GERD symptoms in addition to the effect of omeprazole in pH measurements of reflux, we were not able to collect these data reliably from the parents.
Therefore, although our data suggest that rectal omeprazole could provide an innovative and feasible option to reduce gastric pH in infants with GERD, further studies are needed to show the benefits on clinical outcomes.
To show the superiority of rectal versus oral omeprazole with our pH measurement-based endpoint in a randomized controlled trial, 521 patients per arm are needed, assuming 56% versus 40% success percentages in the rectal versus oral groups, 90% power and 5% significance level. However, such a large study appears unfeasible. Studies focusing on patient-reported outcomes, which should include not only symptom reduction but also reduction of experienced burden and benefit of administration-related issues of the oral and rectal formulations, might be more feasible and clinically relevant. Finally, our study ran into several logistic challenges, leading to prolonged inclusion with financial hurdles and changing clinical care.
Although this was a single-center pilot study, we believe our results can be useful for other settings, as the manufacturing of the omeprazole suppositories does not require specialized equipment or expertise and can be carried out in any GMP-certified laboratory [12]. Moreover, the pH measurements were performed according to international standards. In the current guidelines for GERD in the general pediatric population and in infants with EA and CDH, a place in the treatment with PPIs certainly remains for selected patients [22, 23]. A potential roadblock could be the acceptability of rectal drug administration, which varies across countries and appears culturally and socially determined. In countries where rectal paracetamol is widely used, omeprazole suppositories will likely be easily accepted, especially to overcome the challenges with oral administration of omeprazole and other oral PPI formulations.
5 Conclusions
The incidence of GERD is between 50 and 90% in infants with birth defects, such as EA and CDH. As infants require a non-standard dose of omeprazole, the oral bioavailability may be unpredictable and result in variable degrees of drug exposure. A single rectal omeprazole dose of 1 mg/kg results in rapid exposure in the therapeutic range and a consistent increase in intraesophageal and gastric pH in infants with EA or CDH. We consider rectal omeprazole to be an innovative, promising alternative for infants with pathological GERD since the results of our pilot study showed its effectiveness. Further clinical studies are needed to confirm our results.
References
Vandenplas Y, Rudolph CD, DiLorenzo C, et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr. 2009;49:498–547.
Peetsold MG, Kneepkens CM, Heij HA, et al. Congenital diaphragmatic hernia: long-term risk of gastroesophageal reflux disease. J Pediatr Gastroenterol Nutr. 2010;51:448–53.
Tovar JA, Fragoso AC. Gastroesophageal reflux after repair of esophageal atresia. Eur J Pediatr Surg. 2013;23:175–81.
Marseglia L, Manti S, D’Angelo G, et al. Gastroesophageal reflux and congenital gastrointestinal malformations. World J Gastroenterol. 2015;21:8508–15.
Tighe M, Afzal NA, Bevan A, et al. Pharmacological treatment of children with gastro-oesophageal reflux. Cochrane Database Syst Rev. 2014;11:CD008550.
El-Mahdy MA, Mansoor FA, Jadcherla SR. Pharmacological management of gastroesophageal reflux disease in infants: current opinions. Curr Opin Pharmacol. 2017;37:112–7.
Cuthrell C, Rubino C, Ransom JL, et al. GERD in neonates and pediatrics: use of omeprazole. J Pharm Pract. 1999;12:492–3.
Bishop J, Furman M, Thomson M. Omeprazole for gastroesophageal reflux disease in the first 2 years of life: a dose-finding study with dual-channel pH monitoring. J Pediatr Gastroenterol Nutr. 2007;45:50–5.
Ponrouch MP, Sautou-Miranda V, Boyer A, et al. Proton pump inhibitor administration via nasogastric tube in pediatric practice: comparative analysis with protocol optimization. Int J Pharm. 2010;390:160–4.
Gibbons TE, Gold BD. The use of proton pump inhibitors in children: a comprehensive review. Paediatr Drugs. 2003;5:25–40.
Zimmermann AE, Walters JK, Katona BG, Souney PE, Levine D. A review of omeprazole use in the treatment of acid-related disorders in children. Clin Ther. 2001;23:660–79.
Choi M, Chung S, Shim C. Rectal absorption of omeprazole from suppository in humans. J Pharm Sci. 1996;85:893–4.
Zylicz Z, van Sorge AA, Yska JP. Rectal omeprazole in the treatment of reflux pain in esophageal cancer. J Pain Symptom Manage. 1998;15:144–5.
Bestebreurtje P, Roeleveld N, Knibbe CAJ, et al. Development and stability study of an omeprazole suppository for infants. Eur J Drug Metab Pharmacokinet. 2020. https://doi.org/10.1007/s13318-020-00629-1.
Lagerstrom P-O, Persson B-A. Determination of omeprazole and metabolites in plasma and urine by liquid chromatography. J Chrom. 1984;309:347–56.
Vandenplas Y, Goyvaerts H, Helven R, et al. Gastroesophageal reflux as assessed by 24-hour pH monitoring; in 509 healthy infants screened for SIDS-risk. Pediatrics. 1991;88:834–40.
Zhang Y, Huo M, Zhou J, et al. PKSolver: an add-in program for pharmacokinetic and pharmacodynamic data analysis in Microsoft Excel. Comput Methods Progr Biomed. 2010;99:306–14.
Marier JF, Dubuc MC, Drouin E, et al. Pharmacokinetics of omeprazole in healthy adults and in children with gastroesophageal reflux disease. Ther Drug Monit. 2004;26:3–8.
Kaguelidou F, Alberti C, Biran V, et al. Dose-finding study of omeprazole on gastric pH in neonates with gastroesophageal acid reflux using a Bayesian sequential approach. PLoS One. 2016;11:e0166207.
Andersson T, Hassall E, Lundborg P, et al. Pharmacokinetics of orally administered omeprazole in children. International Pediatric Omeprazole Pharmacokinetic Group. Am J Gastroenterol. 2000;95:3101–6.
Ward R, Kearns G. Proton pump inhibitors in peadiatrics: mechanism of action, pharmacokinetics, pharmacogenetics, and pharmacodynamics. Paediatr Drugs. 2013;15(2):119–31.
Krishnan U, Mousa H, Dall’Oglio L, et al. ESPGHAN-NASPGHAN Guidelines for the evaluation and treatment of gastrointestinal and nutritional complications in children with esophageal atresia-tracheoesophageal fistula. J Pediatr Gastroenterol Nutr. 2016;63:550–70.
Rosen R, Vandenplas Y, Singendonk M, et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2018;66:516–54.
Acknowledgements
We thank Dr. Adriaan van Sorge for initiating this study. We also want to thank Mrs. Joke Dunk, research coordinator, and Mrs. Tjitske van der Zanden, research project manager for their extra-ordinary support of the study REB submission and the study execution.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported by Fonds Nuts Ohra Grant number 1103-049.
Conflict of Interest
The authors have no conflicts of interest to declare.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Review board of the Erasmus Medical Centre Rotterdam) and with the Declaration of Helsinki. The protocol was approved by the institutional review board of the Erasmus Medical Centre Rotterdam.
Informed Consent
All parents gave written informed consent for their infant to be involved in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Bestebreurtje, P., de Koning, B.A.E., Roeleveld, N. et al. Rectal Omeprazole in Infants With Gastroesophageal Reflux Disease: A Randomized Pilot Trial. Eur J Drug Metab Pharmacokinet 45, 635–643 (2020). https://doi.org/10.1007/s13318-020-00630-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13318-020-00630-8