
Abstract
Introduction
Efficacy and safety of the fixed ratio combination of insulin degludec and liraglutide (IDegLira) has been largely documented. However, long-term data are limited. This study aimed at describing persistence in therapy and the effectiveness at 48 months of IDegLira.
Methods
We conducted an observational study based on retrospective chart review. All patients treated with IDegLira during 2018–2022 were included. Data on treatment approaches and clinical outcomes were collected at the first prescription of IDegLira (T0) and after 6, 12, 24, 36, and 48 months.
Results
Overall, 156 patients (mean age 68 years, 64.1% men) started IDegLira, of whom 88 (56.4%) were previously treated with basal-oral therapy (BOT) and 68 (43.6%) with basal-bolus schemes (BB). Before starting IDegLira, 23.8% were treated with ≥ 2 oral antihyperglycemic agents in association with insulin; at T0, the proportion decreased to 3.2%. Short-acting insulin was discontinued after the first week. After 48 months, levels of HbA1c were significantly reduced by 1.34% in the BOT group and 1.07% in the BB group (p < 0.0001 in both groups). In the BOT group, FBG levels decreased by about 50 mg/dl and body weight was unchanged. In the BB group, FBG levels decreased by about 40 mg/dl and body weight was significantly reduced by an average of 7.7 kg. Five patients (3.2%) interrupted therapy with IDegLira during 48 months, and no severe hypoglycemia occurred.
Conclusions
Our study emphasizes the important role of IDegLira in maintaining a good metabolic control while minimizing the risk of major hypoglycemia and weight gain in the long term. The substantial simplification of treatment schemes can increase adherence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Efficacy and safety of the fixed ratio combination of insulin degludec and liraglutide (IDegLira) has been largely documented, although long-term data are still limited. |
This observational study aimed at describing persistence in therapy and effectiveness of IDegLira over 48 months. |
What was learned from the study? |
Patients previously treated with either basal-oral therapy or basal-bolus schemes (these latter discontinuing short-acting insulin after the first week) were considered. |
In both groups, good metabolic control while minimizing the risk of hypoglycemia and weight gain was documented in the long term. |
Introduction
Type 2 diabetes (T2D) is a chronic condition that requires progressive therapy intensification [1]. However, inertia in intensifying anti-hyperglycemic therapy, especially when insulin needs to be started, is a common barrier [2].
Both glucagon-like peptide 1 receptor agonists (GLP-1RA) and basal insulin are now recommended treatment options for intensification at many stages of T2D, with the potential of overcoming clinical inertia [3]. These agents have complementary mechanisms of action and, when used together, can offer several benefits to people with T2D [4]. In fact, basal insulin is effective in lowering fasting plasma glucose (FPG), and its dose can be titrated to the individual patient’s needs. However, a caveat of an increased risk of hypoglycemia and weight gain exists. As compared to first-generation basal insulin analogues, second-generation analogues are associated with longer duration of action and low risk of hypoglycemia [5, 6]. In parallel, GLP-1 RA increases glucose-dependent insulin secretion, decreases glucose-dependent secretion of glucagon, and slows gastric emptying and increases satiety, targeting both FPG and postprandial glycemia (PPG) [7]. GLP-1 RAs are attractive add-on options to basal insulin because they improve glycemic control, decrease weight, and have a low risk of hypoglycemia; however, they do cause gastrointestinal (GI) adverse effects (AEs) [7]. In several studies, GLP1-RA reduced the risk of chronic kidney disease development and progression, with benefits mainly driven by a reduction in new onset macroalbuminuria [8]. GLP1-RA are now considered as a second-line, or even arguably first-line, glucose-lowering therapy in patients at high cardiovascular risk, or with established cardiovascular (CV) disease, irrespective of glycemic control [3].
Formulations of fixed ratio combinations (FRC) of basal insulin with GLP-1 RA in pre-filled pens suitable for once-daily injection are available, and their use has been demonstrated to result in greater glycemic-lowering efficacy than the monocomponents, less weight gain, lower rates of hypoglycemia than intensified insulin regimens, and better gastrointestinal tolerability than GLP-1 RA alone [9]. FRC composed by the second-generation basal insulin analogue degludec and liraglutide (IDegLira) has been adopted in Italy since January 2018. Approval by health authorities followed evidence from the comprehensive DUAL clinical trial program [10], which documented efficacy and safety of IDegLira in patients with uncontrolled T2D on oral antidiabetic drugs (DUAL I, IV, and VI) [11,12,13], GLP-1RAs (DUAL III) [14], basal insulin (DUAL II and V) [15, 16], and basal-bolus insulin (DUAL VII) [17].
Subsequently, real-world data documented the effectiveness and safety of IDegLira when used under routine clinical practice conditions, consistently confirming the benefits documented in randomized clinical trials [18,19,20,21,22,23]. Furthermore, since IDegLira allows once-daily injection and simple dose adjustment, it is judged a more attractive option for patients reluctant to start multiple daily insulin therapy [24].
However, most of the evidence on IDegLira was derived from studies having a duration of follow-up of 6 or 12 months. Data on long-term effectiveness and durability of IDegLira are limited. The 12-month extension of the DUAL I trial [25] confirmed the initial 26-week main phase results and the sustainability of the benefits of IDegLira compared with its components in glycemic efficacy, safety, and tolerability [26]. Longer durability of the treatment effect with IDegLira vs. insulin glargine was documented in the DUAL VIII trial during a 104-week follow-up. Among observational studies, in only one the follow-up reached 18 months [27].
Furthermore, a standard, widely accepted protocol for discontinuing short-acting insulin in patients on basal-bolus regimen (BB) who switch to other treatment schemes is not available in clinical practice. As a consequence, the discontinuation of short-acting insulin might require a long time, due for example to the physician’s fear of suspending insulin and worsening metabolic control, especially in patients treated with large doses of insulin.
In Italy, the Diabetes Service of the Umbria local heath authority (USL Umbria 1) in Perugia conducted a retrospective observational study of all patients treated with IDegLira since February 2018. The results of a first evaluation of the effectiveness were previously published [28] and documented that in patients deriving from basal-oral therapy (BOT) starting IDegLira represented a good option for improving metabolic control, while in those treated with BB, the switch to IDegLira allowed a reduction of insulin doses. The extension phase of this study was approved by the local Ethics Committee and now 4-year follow-up has been reached.
The aim of the present paper is to report data on persistence in therapy and effectiveness of IDegLira in all BOT or BB patients cared for by the center and starting IDegLira under routine clinical practice conditions. In addition, a strategy for early short-acting insulin deprescription is proposed, based on clinical practice of our center.
Methods
This was a longitudinal, observational study based on the retrospective patient chart review, performed in the Diabetes Service of the Umbria local health authority (USL Umbria 1) in Perugia.
As reported by the Summary of Product Characteristics (https://www.ema.europa.eu/en/documents/product-information/xultophy-epar-product-information_en.pdf), in Italy IDegLira is indicated for the treatment of adults with insufficiently controlled T2D to improve glycaemic control as an adjunct to diet and exercise in addition to other oral medicinal products for the treatment of diabetes. All patients already treated with basal insulin receiving a prescription of IDegLira according to the physician judgment under routine clinical conditions were included in the study; exclusion criteria were represented by contraindication to the use of IDegLira. The drug is reimbursed by the public national healthcare system.
At baseline (i.e., the date of the first prescription of IDegLira, T0), the following information was collected: gender, age, diabetes duration, presence of diabetes micro- and macrovascular complications, last prescribed diabetes treatment before starting IDegLira, and clinical parameters [glycated hemoglobin (HbA1c), fasting blood glucose (FBG), body mass index (BMI), waist circumference, estimated glomerular filtration rate (eGFR), and albuminuria].
Follow-up data collected included: HbA1c, FBG, BMI, waist circumference, blood pressure, and renal function. Information on changes in IDegLira dose and concomitant treatments, discontinuation rate, and incidence of severe episodes of hypoglycemia (i.e., episodes requiring intervention of third parties) was also collected. According to Italian standards of care [29], patients were seen approximately every 6 months and data at 6, 12, 24, 36, and 48 months from the first prescription of IDegLira were collected.
FBG tests were recommended and administration of IDegLira was often suggested in the morning to avoid possible titration errors derived from self-monitoring of blood glucose at bedtime. In fact, patients usually consider these tests for the administration of basal insulin.
IDegLira was titrated according to a routine scheme adopted by the diabetes clinic. IDegLira was started at the same dose of the previous basal insulin (no more than 20 dose steps). Dose adjustment was managed by titrating basal insulin based on FBG values. Phone contacts were performed at 1 and 3 months and the titration was managed by the physician. After 3 months, patients were adequately trained to self-titrate the dose. Patients were instructed to familiarize themselves with the concept that each dose-step consisted of 1 U of degludec, with insulin being the primary driver to consider in the titration. Patients were also informed about the benefits deriving from combining basal insulin with liraglutide. Patients not reaching the personalized target were asked to send every 3 months by e-mail the results of their blood glucose measurements and received advice from the diabetologist. At each follow-up visit, clinicians checked whether the patient understood the instructions and whether the dose was correct.
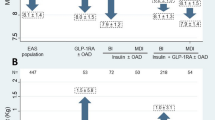
In patients previously treated with short-acting insulin, a deintensification algorithm was applied (Fig. 1), implying the discontinuation of short-acting insulin after the first week of therapy with IDegLira, in order to simplify the therapeutic scheme and allow the optimal up-titration of IDegLira.

Algorithm of BB therapy deintensification at IDegLira initiation
Informed consent was obtained from all patients for being included in the study.
Statistical Methods
Considering the descriptive nature of this study, a formal sample size calculation was not performed. However, a minimum sample size of 47 patients allowed to detect, with a statistical power of 90% and a significance level (alpha) of 0.05, a decrease in HbA1c levels of at least 0.5% after 48 months, assuming an estimated standard deviation of differences of 1.0.
Statistical analyses were performed overall and by stratifying the study population by treatment scheme: patients initiating IDegLira within a basal-oral therapy scheme (BOT) or patients initiating IDegLira to simplify a previous basal-bolus treatment scheme (BB).
Descriptive data were summarized as mean and standard deviation for continuous variables and frequency and proportion for categorical variables. Baseline patient characteristics according to the study cohort were compared using the unpaired t test or the Mann–Whitney U test in case of continuous variables and the chi-square test or the Fisher’s exact test for categorical variables, as appropriate. Statistical significance was declared if the p value was < 0.05.
Changes in continuous study endpoints (HbA1c, FBG, body weight, BMI, albuminuria, and eGFR) were assessed. Mixed models for repeated measurements were adopted for their ability to handle missing data by means of maximum likelihood estimation, thus allowing the estimates at each follow-up visit to be based on all initial cases. Results were expressed as estimated mean or estimated mean difference from T0 with their 95% confidence interval (95% CI). Paired t test derived from linear mixed models for repeated measurements was applied for within-group comparisons in the study cohorts. Comparative effectiveness analysis between BOT and BB groups was avoided due to the high risk of bias in between group comparisons. In fact, the study had a non-randomized design and systematic differences in baseline characteristics (i.e., phenotypes) of the two study cohorts were documented (Table 1).
Results
Overall, 156 patients (mean age, 68 years, 64.1% men) started IDegLira treatment (T0) from February 2018 to April 2022, of whom 88 (56.4%) derived from BOT schemes and 68 (43.6%) derived from BB schemes.
Baseline Characteristics of the Cohort
The two groups differed in terms of diabetes duration (BOT: 11.4 years; BB: 17.3 years; p = 0.0001) and insulin therapy duration (BOT: 3.3 years; BB: 8.4 years; p < 0.0001). Overall, 17.8% of patients had renal impairment, 36% micro/macroalbuminuria, 28.9% retinopathy, 4.2% lower limb complications. Furthermore, 19.9% had experienced one cardiovascular (CV) event, and 8.2% had two CV events. No statistically significant differences emerged between the two groups in the prevalence of CV complications. The switch to IDegLira occurred in both groups at levels of HbA1c above 8.0%, FBG levels close to 160 mg/dl, and BMI levels of 31 kg/m2 (Table 1).
Treatment Approaches Adopted with IDegLira
In the BOT group, 31.1% of patients were already treated with insulin degludec and 12.5% of patients were already treated with a GLP1-RA in free combination (liraglutide 1.2 or 1.8 mg). In the BB group, insulin degludec was prescribed in 14.7% of patients and no patient was already treated with GLP1-RA (Table 1).
Further details on changes in therapy concomitant to the start of IDegLira are reported in Table 2. In BOT group, before starting IDegLira, 60.2% of patients were treated with 1 oral hypoglycemic agent (OHA), 33% with 2 OHAs, and 4.5% with 3 or more OHAs. At T0, IDegLira was used in association with 1 OHA in 98.9% of the cases, and with 2 OHA in 1.1% of cases. The IDegLira starting dose was 17.3 ± 5.7 U, whereas the mean dose of the previous basal insulin was 19.8 ± 9.6 U.
In the BB group, before starting IDegLira, 45.6% of patients were treated with one OHA and 5.9% with two OHAs. At T0, IDegLira was used alone in 8.8% of cases, with one OHA in 85.3% of the cases, and with two OHA in 5.9% of cases. All patients interrupted short-acting insulin. The IDegLira starting dose step was of 17.9 ± 5.3, whereas the mean dose steps of the previous basal and short-acting insulins were 21.1 ± 10.8 and 23.6 ± 18.0, respectively. Based on the deintensification protocol, short-acting insulin was discontinued in all patients after the first week of therapy with IDegLira.
At T48, 80.8% of patients were treated with metformin and 4.5% with a sodium-glucose cotransporter-2 inhibitor (SGLT2i) in association with IDegLira (combination of SGLT2i and IDegLira was not reimbursed by the national health system at the time of observation). Other OHA classes were is continued. Mean dose of metformin was reduced as compared to baseline (Table 3).
IDegLira was taken in the morning by 90% of the patients and self-titrated from the 3rd to the 48th months.
Effectiveness Analysis and IDegLira Titration During 48 Months
Longitudinal changes, overall and by group, in estimated mean levels of continuous endpoints and within-group comparisons are shown in Table 4 and Fig. 2.

Main effectiveness results by previous insulin scheme
In the BOT group, levels of HbA1c were significantly reduced by 1.31% (14.35 mmol/mol) (p < 0.0001) after 6 months from IDegLira initiation, and the reduction was sustained after 48 months (p < 0.0001). In addition, FBG levels decreased by 37 mg/dl (2.06 mmol/l) after 6 months by about 50 mg/dl (2.88 mmol/l) after 48 months. Body weight/BMI and waist circumference were unchanged. eGFR slightly decreased, while no significant changes were observed in albuminuria. On average, dose of IDegLira was titrated during 48 months from 17 to 27 dose steps (Table 4).
In the BB group, levels of HbA1c were significantly reduced by 0.83% (9.02 mmol/mol) after 6 months, by 0.54% (5.88 mmol/mol) after 12 months, and by about 1% (10 mmol/mol) at the subsequent follow-up visits. In addition, FBG levels decreased by about 40 mg/dl (3 mmol/l) during 48 months. Body weight/BMI was significantly reduced by about 5 kg after 6 months and 7 kg after 48 months (corresponding to about − 2.5 kg/m2 BMI points and associated to about − 3.5 cm of waist circumference). eGFR levels slightly decreased, while albuminuria levels did not significantly change. IDegLira was titrated during 48 months from 18 to 26 dose steps during 48 months (Table 4).
Overall, the proportion of patients with HbA1c < 7.0% (53 mmol/mol) was 15.0% at T0, 52.3% after 6 months, and 58.2% after 48 months.
Safety and Persistence in Therapy
No serious adverse events occurred, including severe hypoglycemia. Five patients (3.2%) interrupted IDegLira during 48 months, of whom four due to the need of further therapy intensification and one for intolerance.
Discussion
Many randomized and observational studies have provided evidence of the effectiveness and safety of IDegLira. What this study adds is the evidence of the long-term durability up to 48 months in terms of HbA1c, FBG, and weight. Mean levels of HbA1c reached 7.0% (53 mmol/mol) and were substantially maintained during the follow-up.
A slight reduction in eGFR levels was documented. In particular, the decline in eGFR during 4 years was similar in the BOT and BB groups (− 7.6 ml/min/1.73 m2). This translates into an annual reduction of less than 2 ml/min/1.73 m2. It is estimated that in healthy people, starting from the age of 40, an annual reduction in eGFR of approximately 0.8–1 ml/min/1.73 m2/year occurs, with a rate that usually accelerates after 50–60 years. This process is amplified in subjects with T2D, in whom eGFR decreases almost twice as rapidly as in subjects without diabetes, with a rate ranging from − 1.5 to − 4.0 ml/min/1.73 m2/year [30, 31]. Therefore, our findings are coherent with existing knowledge regarding the decline of eGFR in people with T2D.
As for albuminuria, levels did not significantly change during 48 months. However, the limited availability of information on albuminuria precluded the possibility of drawing solid conclusions regarding the longitudinal changes in this outcome.
IDegLira was titrated during the follow-up by nine dose steps on average, reaching a mean dose of 27 dose steps. The number of concomitant drugs was reduced after 48 months, with the only exceptions of metformin, albeit at a lower dose than baseline, or SGLT2-i. In patients previously treated with BB, short-acting insulin was discontinued after the first week of therapy with IDegLira. Only a small proportion of patients (3.2%) discontinued IDegLira during 48 months.
In real-world studies, IDegLira treatment in poorly controlled patients with T2D was shown to be safe, maintained adequate glycemic control, and was associated with weight loss [18,19,20,21,22,23]. In the EXTRA study, a European multicenter retrospective chart review initiative [18], IDegLira resulted in substantial reductions in HbA1c and body weight, even if it was commonly used at moderate dose, with a reduced risk of hypoglycemia. The REX study [19] documented that IDegLira was used in patients previously treated with BOT and BB regimens, but for different reasons: it was used after BOT in patients with high baseline HbA1c mainly to improve glycemic control and in patients on a BB insulin regimen mainly to simplify the therapeutic regimen.
Furthermore, ADA and EASD recommendations suggest a holistic person-centered care to improve health behaviors and acceptance of, adherence to, and persistence with medical interventions prescribed to support cardiorenal health, attainment of glycemic and weight goals, and adequate quality of life [3]. In this respect, our educational approach to insulin self-titration has been demonstrated to increase patient acceptability and adherence to therapy [28]. Furthermore, among older patients with T2D, deprescribing using a single dose of IDegLira resulted in a greater likelihood of improving health and quality of life [32].
Study results have important clinical implications. First, the study shows that in patients treated with BOT and inadequate metabolic control, the initiation of IDegLira allowed a reduction in the number of classes of drugs to be daily administered and improvements in metabolic control. Second, results confirm the possibility of simplifying therapy and avoiding BB, with long-term beneficial effects on metabolic control, hypoglycemia and body weight. Existing literature does not provide clear indications on how to discontinue short-acting insulin in patients starting IDegLira. However, discontinuation of short-acting insulin is relevant for several reasons: first, the discontinuation of short-acting insulin may contribute to the weight loss documented; second, reimbursement issues related to the concomitant use of other insulins can be avoided; third, it offers the opportunity of not missing the therapeutic simplification that IDegLira offers. Furthermore, early interruption of short-acting insulin also allows a timely and appropriate (self-)titration of IDegLira, minimizing the risk of inertia. Fourth, while free combination of basal insulin and GLP-1 RA allows a more flexible dose titration, the study shows that adequate metabolic control can be obtained with a FRC, facilitating treatment self-management. Finally, we documented the long-term persistence in therapy and its benefits over a period of 4 years.
The study has strengths and limitations. Among the strengths, the study allowed to assess the effectiveness of IDegLira over 4 years and its impact on treatment simplification. Among the limitations, the monocentric nature of the study limits the generalizability of the results. Furthermore, the retrospective design limited the possibility to collect safety data other than severe hypoglycemia during the follow-up. On the other hand, information on the incidence of severe episodes of hypoglycemia before starting the treatment with IDegLira was not available and pre-post comparisons in the rate of hypoglycemic episodes could not be performed. Finally, the study did not include a control group; however, the aim of the study was to assess the long-term outcomes in patients treated with IDegLira and evaluate whether results obtained in RCTs were reproduced in clinical practice.
Conclusions
In conclusion, real-world evidence provides important insights regarding new available therapeutic options. Our study emphasizes the relevant role of IDegLira in pursuing the double aim of improving metabolic control while minimizing the risk of major hypoglycemia and weight gain. These results can be obtained through a simplification of treatment schemes, likely facilitating a better long-term adherence. In the near future, possible additional cardiorenal benefits deriving from the association of IDegLira and SGLT2i (recently made reimbursable in Italy) in a real-world setting will deserve our interest.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Kahn SE. The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of type 2 diabetes. Diabetologia. 2003;46:3–19.
Khunti K, Gomes MB, Pocock S, et al. Therapeutic inertia in the treatment of hyperglycaemia in patients with type 2 diabetes: a systematic review. Diabetes Obes Metab. 2018;20:427–37.
Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, Rosas SE, Del Prato S, Mathieu C, Mingrone G, Rossing P, Tankova T, Tsapas A, Buse JB, Management of Hyperglycemia in Type 2 Diabetes. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;2022(45):2753–86.
Nuffer W, Guesnier A, Trujillo JM. A review of the new GLP-1 receptor agonist/basal insulin fixed-ratio combination products. Ther Adv Endocrinol Metab. 2018;3:69–79.
Kalra S, Shaikh S, Priya G, Baruah MP, Verma A, Das AK, Shah M, Das S, Khandelwal D, Sanyal D, Ghosh S, Saboo B, Bantwal G, Ayyagari U, Gardner D, Jimeno C, Barbary NE, Hafidh KA, Bhattarai J, Minulj TT, Zufry H, Bulugahapitiya U, Murad M, Tan A, Shahjada S, Bello MB, Katulanda P, Podgorski G, AbuHelaiqa WI, Tan R, Latheef A, Govender S, Assaad-Khalil SH, Kootin-Sanwu C, Joshi A, Pathan F, Nkansah DA. Individualizing time-in-range goals in management of diabetes mellitus and role of insulin: clinical insights from a multinational panel. Diabetes Ther. 2021;12:465–85.
Vargas-Uricoechea H. Current state and principles of basal insulin therapy in type 2 diabetes. J Clin Med Res. 2022;14:8–21.
Ussher JR, Drucker DJ. Glucagon-like peptide 1 receptor agonists: cardiovascular benefits and mechanisms of action. Nat Rev Cardiol. 2023;20:463–74.
Brown E, Heerspink HJL, Cuthbertson DJ, Wilding JPH. SGLT2 inhibitors and GLP-1 receptor agonists: established and emerging indications. Lancet. 2021;398:262–76.
Maiorino MI, Chiodini P, Bellastella G, Scappaticcio L, Longo M, Esposito K, Giugliano D. Free and fixed-ratio combinations of basal insulin and GLP-1 receptor agonists versus basal insulin intensification in type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2018;20:2309–13.
Harris S, Abrahamson MJ, Ceriello A, Charpentier G, Evans M, Lehmann R, Liebl A, Linjawi S, Holt RIG, Hosszúfalusi N, Rutten G, Vilsbøll T. Clinical considerations when initiating and titrating insulin degludec/liraglutide (ideglira) in people with type 2 diabetes. Drugs. 2020;80:147–65.
Gough SC, Bode B, Woo V, et al. Efficacy and safety of a fixed-ratio combination of insulin degludec and liraglutide (IDegLira) compared with its components given alone: results of a phase 3, open-label, randomised, 26-week, treat-to-target trial in insulin-naive patients with type 2 diabetes. Lancet Diabetes Endocrinol. 2014;2:885–93.
Rodbard HW, Bode BW, Harris SB, et al. Safety and efficacy of insulin degludec/liraglutide (IDegLira) added to sulphonylurea alone or to sulphonylurea and metformin in insulin-naive people with type 2 diabetes: the DUAL IV trial. Diabet Med. 2017;34:189–96.
Harris SB, Kocsis G, Prager R, et al. Safety and efficacy of IDegLira titrated once weekly versus twice weekly in patients with type 2 diabetes uncontrolled on oral antidiabetic drugs: DUAL VI randomized clinical trial. Diabet Obes Metab. 2017;19:858–65.
Linjawi S, Bode BW, Chaykin LB, et al. The efficacy of IDegLira (insulin degludec/liraglutide combination) in adults with type 2 diabetes inadequately controlled with a GLP-1 receptor agonist and oral therapy: DUAL III randomized clinical trial. Diabet Ther. 2017;8:101–14.
Buse JB, Vilsbøll T, Thurman J, et al. Contribution of liraglutide in the fixed-ratio combination of insulin degludec and liraglutide (IDegLira). Diabet Care. 2014;37:2926–33.
Lingvay I, Perez Manghi F, Garcıa-Hernandez P, DUAL V Investigators, et al. Effect of insulin glargine up-titration vs insulin degludec/liraglutide on glycated hemoglobin levels in patients with uncontrolled type 2 diabetes: the DUAL V randomized clinical trial. JAMA. 2016;315:2125.
Billings LK, Doshi A, Gouet D, et al. Efficacy and safety of IDegLira versus basal-bolus insulin therapy in patients with type 2 diabetes uncontrolled on metformin and basal insulin: the DUAL VII randomized clinical trial. Diabetes Care. 2018;41:1009–16.
Price H, Blüher M, Prager R, Phan TM, Thorsted BL, Schultes B, EXTRA study group. Use and effectiveness of a fixed-ratio combination of insulin degludec/liraglutide (IDegLira) in a real-world population with type 2 diabetes: Results from a European, multicentre, retrospective chart review study. Diabetes Obes Metab. 2018;20:954–62.
Fadini GP, Buzzetti R, Fittipaldi MR, D’Incau F, Da Porto A, Girelli A, Simoni L, Lastoria G, Consoli A, REX study group. IDegLira for the Real-World Treatment of Type 2 Diabetes in Italy: protocol and Interim Results from the REX Observational Study. Diabetes Ther. 2022;13:1483–97.
Drummond R, Baru A, Dutkiewicz M, Basse A, Tengmark BO. Physicians’ real-world experience with IDegLira: results of a European survey. BMJ Open Diabet Res Care. 2018;6: e000531.
Melzer-Cohen C, Chodick G, Naftelberg S, Shehadeh N, Karasik A. Metabolic control and adherence to therapy in type 2 diabetes mellitus patients using IDegLira in a real-world setting. Diabet Ther. 2020;11:185–96.
Egede LE, Bogdanov A, Fischer L, et al. Glycemic control among patients newly prescribed IDegLira across prior therapy group in us real-world practice. Diabetes Ther. 2020;11:1579–89.
Taybani ZJ, Bótyik B, Gyimesi A, Katkó M, Várkonyi T. One-year safety and efficacy results of insulin treatment simplification with IDegLira in type 2 diabetes. Endocrinol Diabetes Metab. 2023;6: e390.
Warren M, Steel D. Clinical use of IDegLira: initiation to titration after basal insulin. Clin Diabetes. 2020;38:62–70.
Gough SC, Bode BW, Woo VC, Rodbard HW, Linjawi S, Zacho M, Reiter PD, Buse JB. One-year efficacy and safety of a fixed combination of insulin degludec and liraglutide in patients with type 2 diabetes: results of a 26-week extension to a 26-week main trial. Diabetes Obes Metab. 2015;17:965–73.
Aroda VR, González-Galvez G, Grøn R, Halladin N, Haluzík M, Jermendy G, Kok A, Őrsy P, Sabbah M, Sesti G, Silver R. Durability of insulin degludec plus liraglutide versus insulin glargine U100 as initial injectable therapy in type 2 diabetes (DUAL VIII): a multicentre, open-label, phase 3b, randomised controlled trial. Lancet Diabetes Endocrinol. 2019;7:596–605.
Szépkúti S, Bandur S, Kovács G, Ferenci T, Svébis MM, Turbucz P, Tabák ÁG. Real-world effectiveness of IDegLira compared with intensified conventional insulin therapy in adults with type 2 diabetes: a retrospective cohort study. BMC Endocr Disord. 2022;22:229.
Di Loreto C, Celleno R, Piastrella L, Del Sindaco P. IDegLira fixed-ratio combination in the real world: a retrospective observational single-center Italian experience. Eur Rev Med Pharmacol Sci. 2020;24:10671–9.
Mannucci E, Candido R, Monache LD, Gallo M, Giaccari A, Masini ML, Mazzone A, Medea G, Pintaudi B, Targher G, Trento M, Turchetti G, Lorenzoni V, Monami M, for Società Italiana di Diabetologia (SID) and Associazione Medici Diabetologi (AMD). Italian guidelines for the treatment of type 2 diabetes. Acta Diabetol. 2022;59:579–622.
Doshi SM, Friedman AN. Diagnosis and management of type 2 diabetic kidney disease. Clin J Am Soc Nephrol. 2017;12:1366–73.
Fiazzi F, Russo GT, Ceriello A, Fioretto P, Giorda C, De Cosmo S, Pontremoli R. Natural history and risk factors for diabetic kidney disease in patients with T2D: lessons from the AMD-annals. J Nephrol. 2019;32:517–25.
Rizza S, Piciucchi G, Mavilio M, Longo S, Montagna M, Tatonetti R, Nucera A, Federici M. Effect of deprescribing in elderly patients with type 2 diabetes: IDegLira might improve quality of life. Biomed Pharmacother. 2021;144: 112341.
Acknowledgements
The authors thank the whole staff of participating center and all the collaborators.
Medical Writing and/or Editorial Assistance
Editorial assistance provided by CORESEARCH SRL (Maria Chiara Rossi, Giusi Graziano). The authors of the publication are fully responsible for the contents and conclusions. Novo Nordisk S.p.A. did not influence and has not been involved in the data interpretation presented in the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. The Rapid Service Fee was funded through a Novo Nordisk S.p.A. unconditional grant.
Author information
Authors and Affiliations
Contributions
Authors adhere to the ICMJE guidelines for authorship. Chiara Di Loreto contributed to study concept and design of data, Debora Pezzuto, Franca Ambrosi, Silvia Bellavita, Marinella Biagini, and Monica Passeri contributed to acquisition of data, Paola Del Sindaco, and Roberta Celleno revised statistical analysis, Chiara Di Loreto, PDS, RC contributed to interpretation of data, Chiara Di Loreto drafted of the manuscript, Chiara Di Loreto contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. Chiara Di Loreto is the guarantor of this work and, as such, has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Conflict of Interest
Chiara Di Loreto, Roberta Celleno, Debora Pezzuto, Franca Ambrosi, Silvia Bellavita, Marinella Biagini, Monica Passeri, and Paola Del Sindaco have no interests to declare.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. The study protocol was approved by the Umbria Regional Committee, Italy (Prot. No. 17550/19/ON—date October 22nd, 2019). Informed consent was obtained from all patients for being included in the study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Di Loreto, C., Celleno, R., Pezzuto, D. et al. Effectiveness, Simplification and Persistence of IDegLira in Poorly Controlled People with Type 2 Diabetes: A 4-Year Follow-Up Real-World Study. Diabetes Ther 15, 1313–1331 (2024). https://doi.org/10.1007/s13300-024-01564-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-024-01564-z