
Abstract
Introduction
Insulin degludec/liraglutide (IDegLira) is a fixed-ratio combination (FRC) of basal insulin and glucagon-like protein-1 receptor agonist (GLP-1 RA) that has demonstrated glycemic and metabolic benefits in patients with type 2 diabetes mellitus (T2DM) in both randomized controlled trials and real-world studies. The impact of adherence to this medication and its effect on patients with T2DM who switch from loose-dose combination therapy to a FRC of insulin and GLP-1RA have not yet been reported. We have examined the metabolic effects and adherence to this medication in a real-life setting, in T2DM patients who initiated IDegLira therapy after being treated with other glucose-lowering drugs.
Methods
This is a retrospective observational study of adult T2DM patients managed by the Maccabi Healthcare Services (Israel) who initiated IDegLira and persisted with therapy for 180 days between July 2017 and August 2018. Mean glycated hemoglobin (HbA1c), body weight change, metabolic parameters, dose and proportion of days covered (PDC) by IDegLira were recorded from initiation to after 180 days of therapy.
Results
A total of 413 patients who persisted with IDegLira therapy for at least 180 days were evaluated as a per protocol group. A significant mean reduction in HbA1c of 0.65% (95% confidence limits [CL] − 0.78, − 0.52; P < 0.001) was observed at 180 days compared with baseline. IDegLira therapy led to a significant reduction in HbA1c in patients previously treated with different background combinations of glucose-lowering drugs before being started on IDegLira. The largest group (n = 247) comprised those who switched from a loose-dose combination therapy of insulin and GLP-1 RA as injectable components given alone to the IDegLira FRC. In this group, HbA1c was reduced by 0.42% (95% CL − 0.57, − 0.27; P < 0.001) and in parallel the PDC of insulin and GLP-1 RA increased from a median of 60% (interquartile range [IQR] 34.4–79.4) in the 180 days prior to IDegLira initiation to 77.8% (IQR 65.6–90.0) in the 180 days after initiation.
Conclusion
In a real-world setting, the use of IDegLira was associated with improved glycemic control and adherence to therapy.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Why Carry Out This Study? |
Fixed-ratio combinations (FRC) of glucagon-like protein-1 receptor agonist (GLP-1 RA) and insulin are designed to provide better glycemic control by targeting both fasting and postprandial glucose levels with one therapy and therefore reduce and simplify the treatment regimen to improve adherence. The efficacy and safety of the FRC IDegLira (insulin degludec/liraglutide) have been proven in several clinical trials, but real-world studies are needed to evaluate the effectiveness of IDegLira therapy as well as improved adherence in clinical practice. |
This study aimed to evaluate this co-occurrence of improved adherence and reduction in glycated hemoglobin (HbA1c) in patients who initiated IDegLira therapy in a real-world setting. |
What Was Learned from the Study? |
Persistence to IDegLira for > 180 days was associated with a significant mean reduction of 0.65% in HbA1c compared with baseline. |
The switch to the FRC IDegLira was associated with a significant reduction in HbA1c in patients with different background therapies of oral and parenteral glucose-lowering drugs at baseline, including the largest group (n = 247) who switched from a loose-dose combination therapy of insulin and GLP-1 RA to FRC of IDegLira. |
Those who switched from loose-dose combination therapy to FRC showed improved adherence, with proportion of days covered with insulin and GLP-1 RA increasing from median of 60% (interquartile range [IQR]) 34.4–79.4) in the 180 days prior to the drug initiation to 77.8% (IQR 65.6–90.0) in the 180 days after initiation. |
Introduction
Co-administration of a glucagon-like protein-1 receptor agonist (GLP-1 RA) and long-acting basal insulin as a treatment of type 2 diabetes mellitus (T2DM) to achieve improved glycemic control in patients with T2DM is based on a solid understanding of the complementary physiological mechanisms of the actions of both agents [1]. Ample clinical data support combining these agents for the treatment of T2DM, an approach which is endorsed as a third-line treatment in the consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) on the management of hyperglycemia in T2DM [2]. Fixed-ratio combinations (FRC) of GLP-1 RA and insulin have been introduced and approved for use in adults with T2DM by regulatory agencies, with the aim to reduce the number of injections and treatment burden by targeting both fasting and postprandial glucose levels by one parenteral therapy and, thereby, simplify the treatment regimen. IDegLira (marketed under the trade name Xultophy® 100/3.6; Novo Nordisk, Bagsværd, Denmark) is a FRC of a long-acting new generation of basal insulin (degludec) and a long-acting GLP-1 RA analogue (liraglutide) to be used as a once-daily subcutaneous injection for the treatment of T2DM. The safety and efficacy of IDegLira were examined in the DUAL I–IX set of randomized clinical trials (RCTs) that compared IDegLira use to that of long-acting new generation and modern basal insulin (degludec and glargine U100) and long-acting GLP-1 RA analogue (liraglutide) as components given alone [3,4,5,6,7,8,9,10,11]. The results showed that IDegLira was superior to the other drugs given alone at reducing glycated hemoglobin (HbA1c), with weight neutrality or weight loss rather than weight gain, as well as at significantly reducing hypoglycemia rates and insulin-dose requirement, with a high proportion of subjects achieving a < 7% HbA1c target [3,4,5,6,7,8,9,10,11]. These advantages, as documented in the various DUAL RCTs, highlight the great potential of the IDegLira FRC to increase adherence to therapy.
Studies that evaluate the real-world use of IDegLira allow the advantages of IDegLira to be assessed in practice and their effect on patients’ adherence to be determined. In the study reported here, we examined the clinical effectiveness of IDegLira in Israeli patients who completed at least 180 days of IDegLira therapy. Our results add to the accumulating real-world data on IDegLira use.
Methods
Study Design and Patients
This retrospective analysis of computerized clinical databases was carried out at Maccabi Healthcare Services (MHS), a healthcare provider. MHS provides healthcare services to a quarter of the population of Israel, covering approximately 2.2 million members, 180,000 (8.2%) of whom have documented diabetes. The central computerized database stores data on members’ medical information, including medication, and all patients with diabetes are included in a diabetes registry with specific inclusion criteria detailed elsewhere [12, 13].
This study was approved by the local institutional review board of Assuta Hospital, Israel and was performed in accordance with the Declaration of Helsinki of 1964, as revised in 2013. Individual patient-informed consent was not required because of the anonymized nature of the patient records.
All patient data from those who initiated IDegLira treatment between 1 July 2017 and 17 August 2018 and for whom at least two prescriptions for the drug were dispensed were included in the study. The index date was defined for each patient as the first date of purchase of IDegLira. To be included, patients had to be members of MHS for at least 12 months prior to treatment initiation (index date) and until 180 days after treatment initiation; be > 18 years old at index date; and to be included in the diabetes registry prior to index date. Patients were required to have an HbA1c measurement at baseline (defined as 180 days prior to the index date) and after 180 days (± 90 days) from the index date. Patients who were defined in the diabetes registry as having type 1 diabetes were excluded from the study.
Two approaches were used to evaluate outcomes: an intention-to-treat (ITT)-like approach population, which included all patients with at least two dispensed prescriptions for IDegLira during the first 180 days, and a per protocol-like approach population that persisted with IDegLira treatment for ≥ 180 days, based on the continuous despensing of prescriptions for IDegLira.
Variable Definitions
For all laboratory measurements, baseline values were measured ≤ 180 days before the index date (most recent measurement used); post -therapy values (HbA1c) were measured 90–270 days after baseline (the measurement closest to 180 days was used). The difference in change in body weight and body mass index (BMI) from baseline to 180 days was calculated. Total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol and triglyceride levels were measured at baseline and after 180 days of therapy. Values of > 300 mg/dL were recorded as 300 mg/dL for the analyses.
Anti-hyperglycemic medications at baseline were defined based on the dispensing of medications in the 180 days prior the index date. Patients on oral anti-diabetic medications only were defined as the oral antidiabetic drugs (OADs) group. Among patients prescribed injectable medication(s) (with or without OADs), the following categories were defined: those on GLP-1 RA; those on basal insulin, those on GLP-1 RA + basal insulin (loose-dose combination therapy); and those on multi-daily injections (MDIs) of insulin.
Duration of diabetes was defined as the number of years in the MHS diabetes registry [12], which was based on diagnosis, medication dispensed and laboratory measurements. Comorbidities reported within 12 months prior to the index date were defined according to the relevant disease registries (cardiovascular disease [14], cerebrovascular disease, chronic kidney disease and hypertension [15]) or according to the International Classification of Diseases, Ninth Revision (ICD-9) codes (dyslipidemia: 272.X; liver disease: 570.X–573.X; pancreatitis: 577.X; gallbladder disease: 575.X–576.X; https://www.cdc.gov/nchs/icd/icd9cm.htm).
Primary evaluation was performed on the group that completed at least 180 days of therapy (defined as the per protocol cohort). An additional sensitivity analysis was performed as an ITT-like approach including the full cohort. The pre-treatment period was defined as the 180 days prior to the index date. The follow-up period was defined as 180 days after the index date (measurements made 180 ± 90 days after the index date). Change in HbA1c was evaluated in the full cohort as well as in specific subgroups (by baseline regimen, sex, age, baseline HbA1c, BMI and by history of cardiovascular disease). In addition, longitudinal mean change in HbA1c during the follow-up period was presented at the following time points: 0 time point (closest measurement within 180 days prior to the index date); 3 months (90 [± 45] days); 6 months (180 [± 45] days); and 9 months (270 [± 45] days).
Persistence was used to describe patients who used IDegLira for at least 180 days. Adherence was reported as the proportion of days covered (PDC) based on days covered by filled (dispensed) prescriptions (based on duration parameter from dispensed medication, calculated as days covered by both GLP-1 RA and insulin) during the 180 days prior to the index date as well as the first 180 days of treatment, which included the titration period (maximum coverage days was defined as 100%). GLP-1 RA dosage was converted to defined daily doses (DDD) units defined in the World Health Organization’s collaboration center for Drug Statistics Methodology (https://www.whocc.no/).
Statistical Methods
Patient’s characteristics were presented as the mean ± standard deviation (with the median as appropriate) for continuous variables and as the number and percentages for categorical variables. Changes in laboratory measurements, medication dosage and PDC were evaluated using the paired t test or the Wilcoxon-signed rank test, as appropriate. The same procedure was used to compute the change in the various subgroups of patients as defined previously.
In all statistical analyses, a two-sided P value of < 0.05 was considered to be statistically significant. All analyses were performed using SAS version 9.4 or higher (SAS Institute, Cary, NC, USA) and SPSS statistical software (IBM Corp., Armonk, NY, USA).
Results
Patient Demographics and Baseline Characteristics
A total of 484 patients initiated IDegLira from July 2017 up to 17 August 2018 and fulfilled all inclusion and exclusion criteria. Of these, 413 (> 85%) persisted with IDegLira therapy for at least 180 days and were included in the per protocol-like analysis. The baseline characteristics, co-morbidities, laboratory measurements and medications of these 413 patients included in the primary analysis are presented in Table 1. Briefly, the mean age of this group at index date was 63.8 ± 8.9 years, 45.0% were women and 79.2% were included in the diabetes registry for > 10 years; 93% were on injectable glucose-lowering agents before being switched to IDegLira. Insulin was included in the baseline treatment regimen in 85.5% of the patients, and GLP-1 RA was included in the baseline treatment regimen in 67.3% of patients. The largest group (n = 247, 59.8%) was treated with a loose-dose combination therapy of a GLP-1 RA and insulin prior to switching to the IDegLira FRC. The mean HbA1c and mean BMI at baseline was 8.6 ± 1.4% and 32 ± 4.8 kg/m2, respectively.
IDegLira Persistence and HbA1c Levels
Among patients who persisted on IDegLira therapy for 180 days, the mean measured reduction in HbA1c from baseline to 180 days was − 0.65% (95% confidence limits [CL] − 0.78, − 0.52; P < 0.001) (Fig. 1). The most pronounced decrease in HbA1c (− 1.87%; 95% CL − 2.50, − 1.23; P < 0.001) was observed in the 29 patients who were on OADs only at baseline. Significant reductions in HbA1c were observed after 180 days in patients treated with basal insulin (− 0.94%; 95% CL − 1.30, − 0.57; n = 74), MDI (− 0.39%; 95% CL − 0.84, 0.06; n = 32) and GLP-1 RA (− 0.93%; 95% CL − 1.24, − 0.62; n = 31). In the largest group (n = 247) who switched from a loose combination of insulin and GLP-1 RA to FRC therapy of IDegLira, a reduction of − 0.42% (95% CL − 0.57, − 0.27; P < 0.001) from a baseline HbA1c of 8.43% ± 1.38 was measured after 180 days of therapy. Most of those who switched (n = 146, 60%) from loose-dose combinations to the FRC of IDegLira improved their glycemic control; after 180 days, HbA1c was reduced by > 1% in 65 patients (45%) and by 0.1–1% in 81 (55%) patients.

Box plot of glycated hemoglobin (HbA1c) at baseline and after 180 ± 90 days of insulin degludec/liraglutide (IDegLira) therapy by hypoglycemic therapy prior to index date. Dark-gray shadowing represents values at the baseline period; light-gray shadowing represents values at the follow-up period. GLP-1RA glucagon-like protein-1 receptor agonist, MDI multi-daily injections of insulin, N Number of patients, OADs oral antidiabetic drugs
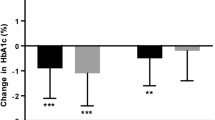
The significant reduction in HbA1c after 180 days of IDegLira therapy was consistent in the subgroups according to age, gender, BMI and baseline HbA1c and in patients with and without cardiovascular disease. HbA1c baseline level was the most influencing parameter, with the exception of baseline glycemic regimen, which significantly influenced the degree of HbA1c change (Fig. 2). Measurements of HbA1c at the different time points showed that maximal reduction was achieved around the 180 day time point and that this level was stable in the following measurements taken at 270 days after the index date (Fig. 3).

Change in HbA1c after 180 days of IDegLira therapy by baseline characteristics. P value represents P value for heterogeneity, and Total represents P value for change in HbA1c. BMI Body mass index, N number of patients in each subgroup, CL confidence limits

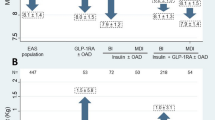
Change in HbA1c after 180 + 90 days of IDegLira therapy (and during treatment). Patients may have more than one measurement. Measurements closer to the time points were collects. GLP-1 RA glucagon-like protein receptor agonist, N number of patients in each subgroup
Insulin and GLP-1 RA Doses and Proportion of Days Covered
Mean doses of IDegLira over the 180 days were 38.48 ± 11.50 units and decreased from 40.44 ± 13.57 in the first 90 days to 36.52 ± 13.67 units between 90 and 180 days (P < 0.001). Only 64 patients (15.5%) reached the maximal dose of 50 units given in one injection; this percentage was similar (12.2%) among the 113 patients with a previous cardiovascular disease history. For those patients who switched from loose-dose combinations of insulin and GLP-1 RA to FRC, insulin doses did not change (− 0.29 units/day; 95% CL − 3.67, 3.09; P = 0.584) while GLP-1 RA doses increased (0.22 DDD units; 95% CL 0.16, 0.28; P < 0.001]. In the whole group, 43.8% of patients had > 75% PDC and 36.3% had PDC of 50–75% (based on treatment duration records on actual dispensing of medication). Among those who switched from a loose-dose combination therapy to a FRC, 54.7% of patients had PDC of > 75%, and an additional 34.0% had > 50% of days covered. The median PDC of the group which switched was significantly improved (P < 0.01) from 60% (interquartile ratio [IQR] 34.4–79.4) in the 180 days prior to the index day to 77.8% (IQR 65.6–90.0) in the 180 days after the index date. In the subgroup of switchers who reduced their HbA1c by > 1%, PDC for insulin and GLP-1 RA increased from a median of 51.7 (IQR 33.3–73.3) to 72.8 (IQR 63.9–83.3) (P < 0.01).
IDegLira Therapy and Other Metabolic Parameters
Improvements in other metabolic parameters were also noted after switching to IDegLira (Table 2). These included a reduction in fasting blood glucose from a mean of 169.27 ± 62.06 to 143.01 ± 51.17 mg/dL, which is an average change of − 25.61 mg/dL (95% CL − 32.53, − 18.70; P < 0/001). This reduction was consistent in all baseline treatment subgroups. The largest reduction in fasting blood glucose was in the group of patients on OADs at baseline (− 98.77 mg/dL; 95% CL − 130.35, − 67.19; P < 0.001) and in the group which switched from loose-dose combinations (data not shown). Significant improvements were noted in triglyceride and LDL levels ((− 15.61 mg/dL; 95% CL − 24.68, − 6.53; P < 0.001) and (− 15.74 mg/dL; 95% CL − 22.55, − 8.92; P < 0.001), respectively) , but there were no significant changes in total cholesterol and HDL cholesterol. These improvements in glucose control were observed with no significant weight change in the whole group or in the different subgroups (Table 2).
IDegLira Therapy in the ITT Group
Evaluation of the glycemic effect was repeated in the whole group of patients who initiated the treatment, including those who did not complete the 180 days of therapy, to resemble an ITT approach. This group of 484 patients, which included an additional 71 patients, was analyzed in a similar fashion. HbA1c reduction was very similar to that seen in those who completed the 180 days of therapy (− 0.67%; 95% CL − 0.79, − 0.55; P < 0.001); among the 281 patients who switched from loose-dose combinations to FRC, the reduction of HbA1c was identical at − 0.42 (95% CL − 0.56, − 0.28; P < 0.001) as only three patients did not complete the treatment.
Discussion
In this observational study we found that patients with T2DM who were started on a treatment regimen with IDegLira, a FRC of basal insulin and GLP-1 RA, after being treated with different glucose-lowering therapies improved their glycemic control. A total of 413 patients who were treated with IDegLira for at least 6 months and routinely followed up at a large health maintenance organization in Israel showed a statistically significant decrease in HbA1c. The decrease was most pronounced in patients previously treated with OADs alone, but it was still significant in those previously treated with insulin and/or GLP-1 RA and was not accompanied by either weight gain or an increase in insulin dosage. In this study, IDegLira-treated patients were not compared to a control group, and it is possible that the effect is simply due to the initiation of a new mode of treatment. However, these results are very much in line with the findings in the DUAL set of RCTs in which IDegLira resulted in greater HbA1c reductions compared with the insulin and GLP-1 RA components given alone. They are also supported by the findings of several previous studies that have examined the effect of the IDegLira FRC in real-world setting. In all of these studies, a substantial and significant improvement in HbA1c was observed [16,17,18,19]. The largest of these studies is the European multicenter retrospective real-world EXTRA study, which included 611 patients from five countries on different baseline treatment regimens [16]. In the EXTRA study, IDegLira use resulted in improved glycemic control across all baseline therapy groups, with a substantial − 0.9% overall reduction in HbA1c (P < 0.001) after 6 months from the initiation of therapy. The greatest reduction in the EXTRA study was observed for the non-injectable therapy group (− 1.6%) and lower moderate additional patients who switched from loose-dose combinations to IDegLira (− 0.6%). The analysis in the EXTRA study included all patients who bought even one pack of IDegLira, which resembles an ITT approach.
In our study, we initially analyzed the effect of IDegLira in patients who completed at least 180 days of therapy. This analysis, which resembles a per protocol analysis, provides insight into the effectiveness of those patients who persist with treatment in real-world settings. We performed an additional ITT-like analysis which demonstrated similar trends and reductions in HbA1c among patients from all of the different background therapies. The similarity is not surprising as a high degree of persistence (> 85%) was seen among the initiators of IDegLira therapy. This high persistence is in line with the finding of a physicians’ survey study [19] that reported high patient satisfaction with the switch to IDegLira and with the DUAL results that indicated a significant improvement of several patient-reported outcomes measures (TRIM-D) [9, 10]. IDegLira has also been observed to demonstrate a higher durability effect of treatment when compared to insulin glargine U100, with a significantly longer time until need for intensification (median of > 2 years, compared to only 1 year with glargine U100) [11]. This high durability may contribute to the persistence found in real-world evidence (RWE). Indeed, a recent RWE study demonstrated that 94% of patients initiating IDegLira persisted with treatment for > 6 months and 84% persisted for 1 year. This higher persistence was accompanied by improved glycemic control [20].
A unique observation in our study stems from the large group of patients who were treated with a loose-dose combination of basal insulin and GLP-1 RA and switched to a FRC of the same pharmacologic agents: 60% (N = 247) of the cohort were on a loose-dose combination of insulin and GLP-1 RA before being switched to the FRC. The change to the FRC was associated with a significant reduction in HbA1c. The reduction was also clinically significant with more than a quarter of patients improving their HbA1c level by > 1%. The PDC was significantly improved in all patients in the group who switched to the FRC, with those who improved most having a lower PDC in the baseline period. Adherence to antihyperglycemic medications is often suboptimal in patients with T2DM, a behavior which contributes to poor glycemic control, increased hospitalization and the development of diabetic complications. It is important to measure and assess medication adherence when using medications in the real-world setting. Adherence is evaluated using PDC, a tool developed, validated and approved by the Pharmacy Quality Alliance as a high-quality measure of medication adherence (https://www.cdc.gov/dhdsp/docs/med-adherence-evaluation-tool.pdf). Reported adherence rates to antihyperglycemics varies widely among studies and is reported to be < 50% for injectable medications. More convenient drug administration regimens and advances in formulations and delivery devices are among the strategies shown to improve adherence to antihyperglycemic therapy, especially in those on injectable therapy. IDegLira provides a tool that reduces the regimen complexity by combining FDC into one pen-injector device, thus minimizing the quantity of injections per day. Our study shows that, in a real-life setting, adherence improved in patients who were previously treated with a loose-dose combination of basal insulin and GLP-1 RA and then switched to an FRC and that this improved adherence translated to improved glycemic control. Further insights into the explanatory effects of PDC on HbA1c reduction will be addressed in a longer follow-up study.
In accordance with the findings in the DUAL RCT program and previously published as real-world data on IDegLira, in our study the improved glycemic control achieved using the FDC therapy did not significantly influence body weight and led to a minor but statistically significant improvement in the measurements of most lipid profiles (LDL and triglycerides). A post hoc meta-analysis conducted by Vilsbol et al. also indicated consistently lower levels of LDL with IDegLira compared with comparators across subgroups in all trials, with statistical significance achieved in men, participants aged < 65 years and both diabetes duration subgroups in DUAL II and in all subgroups, with the exception of participants with diabetes duration ≥ 10 years, in DUAL V [21].
The major limitation of this study is its observational nature and lack of a control group to verify that the improvement in glycemic control is not related to the initiation of any new treatment and not IDegLira specifically. Future studies could be planned similar to the RCTs with IDegLira on one arm and other therapies on the other arm to achieve a direct head-to-head comparison, which would improve our understanding of the benefits and superiority of this drug. Nevertheless, the data from the present study support the notion that ease of use in an FRC given once daily leads to increased persistence and adherence to treatment that translates to improved glycemic control in the real-world setting.
Conclusions
In a real-world setting IDegLira led to an improved glycemic and metabolic profile in patients previously treated with different glucose-lowering agents. The largest group was treated with a loose-dose combination of insulin and GLP-1 RA. When these patients were switched to the FRC IDegLira, adherence improved, which led to a statistical and clinically significant improvement in glycemic control.
References
Berlie H, Hurren KM, Pinelli NR. Glucagon-like peptide-1 receptor agonists as add-on therapy to basal insulin in patients with type 2 diabetes: a systematic review. Diabetes Metab Syndr Obes. 2012;5:165–74.
Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;2018(41):2669–701.
Gough SC, Bode B, Woo V, et al. Efficacy and safety of a fixed-ratio combination of insulin degludec and liraglutide (IDegLira) compared with its components given alone: results of a phase 3, open-label, randomised, 26-week, treat-to-target trial in insulin-naive patients with type 2 diabetes. Lancet Diabetes Endocrinol. 2014;2:885–93.
Buse JB, Vilsboll T, Thurman J, et al. Contribution of liraglutide in the fixed-ratio combination of insulin degludec and liraglutide (IDegLira). Diabetes Care. 2014;37:2926–33.
Linjawi S, Bode BW, Chaykin LB, et al. The efficacy of IDegLira (insulin degludec/liraglutide combination) in adults with type 2 diabetes inadequately controlled with a GLP-1 receptor agonist and oral therapy: DUAL III randomized clinical trial. Diabetes Ther. 2017;8:101–14.
Rodbard HW, Bode BW, Harris SB, et al. Safety and efficacy of insulin degludec/liraglutide (IDegLira) added to sulphonylurea alone or to sulphonylurea and metformin in insulin-naive people with type 2 diabetes: the DUAL IV trial. Diabet Med. 2017;34:189–96.
Lingvay I, Perez Manghi F, Garcia-Hernandez P, et al. Effect of insulin glargine up-titration vs insulin degludec/liraglutide on glycated hemoglobin levels in patients with uncontrolled type 2 diabetes: the DUAL V randomized clinical trial. JAMA. 2016;315:898–907.
Harris SB, Kocsis G, Prager R, et al. Safety and efficacy of IDegLira titrated once weekly versus twice weekly in patients with type 2 diabetes uncontrolled on oral antidiabetic drugs: DUAL VI randomized clinical trial. Diabetes Obes Metab. 2017;19:858–65.
Billings LK, Doshi A, Gouet D, et al. Efficacy and safety of IDegLira versus basal-bolus insulin therapy in patients with type 2 diabetes uncontrolled on metformin and basal insulin: the DUAL VII randomized clinical trial. Diabetes Care. 2018;41:1009–16.
Philis-Tsimikas A, Billings LK, Busch R, et al. Superior efficacy of insulin degludec/liraglutide versus insulin glargine U100 as add-on to sodium-glucose co-transporter-2 inhibitor therapy: a randomized clinical trial in people with uncontrolled type 2 diabetes. Diabetes Obes Metab. 2019;21:1399–408.
Aroda VR, Gonzalez-Galvez G, Gron R, et al. Durability of insulin degludec plus liraglutide versus insulin glargine U100 as initial injectable therapy in type 2 diabetes (DUAL VIII): a multicentre, open-label, phase 3b, randomised controlled trial. Lancet Diabetes Endocrinol. 2019;7(8):596–605.
Chodick G, Heymann AD, Shalev V, Kookia E. The epidemiology of diabetes in a large Israeli HMO. Eur J Epidemiol. 2003;18:1143–6.
Heymann A, Maor Y, Goldstein I, et al. Efficacy of liraglutide in a real-life cohort. Diabetes Ther. 2014;5:193–206.
Shalev V, Chodick G, Goren I, et al. The use of an automated patient registry to manage and monitor cardiovascular conditions and related outcomes in a large health organization. Int J Cardiol. 2011;152:345–9.
Weitzman D, Chodick G, Shalev V, et al. Prevalence and factors associated with resistant hypertension in a large health maintenance organization in Israel. Hypertension. 2014;64:501–7.
Price H, Bluher M, Prager R, et al. Use and effectiveness of a fixed-ratio combination of insulin degludec/liraglutide (IDegLira) in a real-world population with type 2 diabetes: results from a European, multicentre, retrospective chart review study. Diabetes Obes Metab. 2018;20:954–62.
Sofra D. Glycemic control in a real-life setting in patients with type 2 diabetes treated with IDegLira at a single Swiss center. Diabetes Ther. 2017;8:377–84.
Williams DM, Shrikrishnapalasuriyar N, Syed W, et al. Real-world clinical experience of Xultophy in the management of patients with type 2 diabetes in a secondary care clinic. Diabetes Metab Syndr. 2018;12:1079–82.
Drummond R, Baru A, Dutkiewicz M, et al. Physicians’ real-world experience with IDegLira: results of a European survey. BMJ Open Diabetes Res Care. 2018;6:e000531.
Eliasson B, Ekelund T, Sveneson AM et al. Use of IDegLira is associated with high persistency rates up to 12 months and improved HbA1c after 6 months in Swedish clinical practice. Diabetes. 2019;68[Suppl 1]:1110-P.
Vilsboll T, Blevins TC, Jodar E, et al. Fixed-ratio combination of insulin degludec and liraglutide (IDegLira) improves cardiovascular risk markers in patients with type 2 diabetes uncontrolled on basal insulin. Diabetes Obes Metab. 2019;21:1506–12.
Acknowledgements
Funding
This study and the Rapid Service Fee were funded by Novo Nordisk A/S.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published.
Authorship Contributions
Cheli Melzer-Cohen performed the statistical analyses, with input from Gabriel Chodick. Avraham Karasik, Shiran Naftelberg and Naim Shehade were involved in the study design and conduct. All authors interpreted the results, were involved with the writing of the manuscript and approved the final draft.
Disclosures
Shiran Naftelberg is an employee of Novo Nordisk. Avraham Karasik has received research grants and consulting fees from Novo Nordisk. Cheli Melzer-Cohen, Gabriel Chodick and Naim Shehadeh have nothing to disclose.
Compliance with Ethics Guidelines
This study was approved by the local institutional review board of Assuta Hospital, Israel and was performed in accordance with the Declaration of Helsinki of 1964, as revised in 2013. Individual patient-informed consent was not required because of the anonymized nature of the patient records.
Data Availability
The datasets analyzed during the current study are not publicly available due Institutional Review Board limitation but are available from the corresponding author on reasonable request.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.10082762.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Melzer-Cohen, C., Chodick, G., Naftelberg, S. et al. Metabolic Control and Adherence to Therapy in Type 2 Diabetes Mellitus Patients Using IDegLira in a Real-World Setting. Diabetes Ther 11, 185–196 (2020). https://doi.org/10.1007/s13300-019-00725-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-019-00725-9