
Abstract
Introduction
Glucagon-like peptide-1 receptor agonists are well-established type 2 diabetes (T2D) treatments. As variations among populations and culture might influence treatment effects, this post hoc analysis evaluates the efficacy and safety of once-weekly (OW) semaglutide in a Korean population.
Methods
Korean adults with T2D inadequately controlled on metformin included in a 30-week, phase 3a, international, multicentre trial (NCT03061214) compared OW subcutaneous semaglutide (0.5 mg and 1.0 mg) with once-daily sitagliptin (100 mg). Key endpoints included change in glycated haemoglobin (HbA1c) and body weight; additional endpoints assessed proportions of participants reaching targets of HbA1c < 7.0% and ≤ 6.5%, ≥ 5% weight loss, and a composite endpoint of HbA1c < 7.0% without severe/blood glucose-confirmed symptomatic hypoglycaemia and no weight gain.
Results
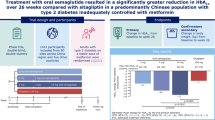
Korean participants (n = 110) showed a greater reduction in HbA1c and body weight with semaglutide 0.5 mg (–1.6%, –2.7 kg) and 1.0 mg (–1.8%, –4.8 kg) versus sitagliptin (–0.9%, 0.5 kg). HbA1c targets of < 7.0% and ≤ 6.5% were achieved by more participants treated with semaglutide 0.5 mg (80.0% and 60.0%, respectively) and 1.0 mg (87.5% and 67.5%, respectively) versus sitagliptin (54.3% and 25.7%, respectively); ≥ 5% weight loss was observed in 42.9% and 65.0% of participants treated with semaglutide 0.5 mg and 1.0 mg versus 0.0% with sitagliptin. The composite endpoint was achieved by 71.4%, 77.5%, and 31.4% of the population in the semaglutide 0.5 mg, 1.0 mg, and sitagliptin group, respectively. No new safety concerns were observed.
Conclusion
This analysis confirms efficacy and safety of OW semaglutide (0.5 and 1.0 mg) in a Korean population with T2D.
Clinical Trial Registration Number
NCT03061214.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Semaglutide is a glucagon-like peptide-1 receptor agonist approved for the treatment of type 2 diabetes (T2D), and its efficacy and safety have been evaluated across various global regions. |
As variations among populations might impact treatment effects, the current analysis assessed the efficacy of semaglutide treatment versus sitagliptin specifically in a Korean population. |
What was learned from the study? |
Once-weekly (OW) subcutaneous semaglutide therapy (0.5 and 1.0 mg) significantly improves glycaemic control and reduces body weight in Korean adults with T2D versus sitagliptin, with a similar safety profile as previously observed for semaglutide versus placebo. |
OW semaglutide therefore offers a clinically relevant treatment option for T2D in a Korean population. |
Introduction
The global prevalence of type 2 diabetes (T2D) more than doubled between 1990 and 2019, reaching approximately 437.9 million people. In addition, type 1 diabetes and T2D are directly responsible for approximately 1.5 million deaths worldwide per year [1,2,3]. In Korea, it is estimated that 6.05 million (16.7%) adults ≥ 30 years lived with diabetes in 2020 [4]. As a result, T2D represents a significant socioeconomic burden in Korea, with associated direct medical costs accounting for approximately 10.6% of all healthcare expenditure [5].
T2D is a complex disease, with guidelines for management of diabetes promoting a personalised, multifactorial treatment based on individual clinical characteristics and, besides optimising glycaemic control, also targeting obesity and other comorbidities [6,7,8]. The close association between obesity and T2D is well known, and overweight or obesity is recognised as a primary risk factor amenable to change in T2D [6]. In Korea, approximately half of adults with diabetes are obese, as defined by a body mass index (BMI) ≥ 25.0 kg/m2 [4, 5, 8], and the Committee of Clinical Practice Guidelines of the Korean Diabetes Association (KDA) now recommends diabetes screening of all people aged ≥ 35 years, and selected people aged ≥ 19 years with identified risk factors, one of which is abdominal obesity [9].
Glucagon-1 peptide receptors are shown to potentiate glucose-dependent insulin secretion while minimising hypoglycaemia, which supported the development of multiple, structurally distinct, glucagon-like peptide-1 receptor agonists (GLP-1RAs) for glycaemic control in people with T2D [10, 11]. In addition, GLP-1RA treatment is associated with weight loss, beneficial effects on kidney outcomes, and significant cardiovascular (CV) benefits [12,13,14,15].
Once-weekly (OW) subcutaneous (s.c.) semaglutide, an approved GLP-1RA for the treatment of T2D, has been evaluated through the comprehensive SUSTAIN clinical trial programme. Not only did OW s.c. semaglutide demonstrate consistent superior glycaemic control and weight loss versus comparators [16,17,18,19,20,21,22,23,24,25], the occurrence of major CV events was significantly decreased compared with placebo and standard of care in participants with T2D at high risk of CV disease [23].
NN9535-4114 (SUSTAIN China) was a 30-week, phase 3a, international, multicentre trial comparing OW s.c. semaglutide with once-daily (OD) oral sitagliptin in adults with T2D inadequately controlled on metformin. A total of 868 participants were recruited from Brazil, the China region (consisting of mainland China, Taiwan, and Hong Kong), the Republic of Korea, South Africa, and Ukraine [26]. Results showed that semaglutide was superior to sitagliptin in improving glycaemic control and reducing body weight [26]. However, given the variations in culture across the regions included in this study, such as diet and lifestyle factors, diabetes management practice, and standard of care, evaluation of the Korean population from the NN9535-4114 trial will provide additional insight in the efficacy and safety of semaglutide. Therefore, the aim of this post hoc analysis was to evaluate the efficacy and safety of semaglutide versus sitagliptin in a Korean subpopulation with T2D inadequately controlled on metformin.
Methods
Study Design and Participants
This was a post hoc analysis of participants from the Republic of Korea enrolled in the NN9535-4114 trial (NCT03061214) [26], who were randomised to receive OW s.c. semaglutide 0.5 mg, OW s.c. semaglutide 1.0 mg, or OD oral sitagliptin 100 mg. Full details of the trial design are reported elsewhere [26].
Key participant inclusion criteria included adults with a diagnosis of T2D with glycated haemoglobin (HbA1c) 7.0–10.5% (53–91 mmol/mol; both inclusive), and treated with metformin monotherapy, at a stable dose ≥ 1500 mg, or a maximum tolerated dose ≥ 1000 mg for 60 days prior to screening [26]. Individuals were excluded from the study if they had treatment with glucose-lowering agent(s) other than metformin for 60 days before screening, a screening calcitonin value ≥ 50 ng/l, history of acute or chronic pancreatitis, a cancer diagnosis in the previous 5 years, history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2, impaired kidney function (as defined by an estimated glomerular filtration rate [eGFR] < 60 ml/min/1.73 m2 per the 4-variable version of Modification of Diet in Renal Disease [MDRD] formula), heart failure (New York Heart Association [NYHA] class IV), or an acute coronary or cerebrovascular event within 90 days before randomisation [26].
Study Outcomes
The primary outcome was change in HbA1c from baseline to week 30 and the confirmatory secondary endpoint was change in body weight from baseline to week 30.
Supportive secondary endpoints included the evaluation of proportions of participants at week 30 who achieved a target HbA1c of < 7.0%, HbA1c of ≤ 6.5%, weight loss of ≥ 5%, and a composite endpoint of HbA1c < 7.0% without severe or blood glucose-confirmed symptomatic hypoglycaemia and no weight gain.
Supportive secondary efficacy endpoints included change from baseline to week 30 in fasting plasma glucose, self-measured plasma glucose (SMPG), blood pressure (BP), fasting insulin, fasting C-peptide, fasting glucagon, fasting proinsulin, fasting proinsulin to insulin ratio, homeostatic model assessment of β-cell function (fasting HOMA-Β) and insulin resistance (fasting HOMA-IR), BMI, waist circumference, fasting lipids (total cholesterol, low-density lipoprotein [LDL] cholesterol, very low-density lipoprotein [VLDL] cholesterol, high-density lipoprotein [HDL] cholesterol, triglycerides, and free fatty acids), and high-sensitivity C-reactive protein. Weight parameters and blood samples for these efficacy assessments were standardly collected during the six study visits under the treatment period and after 30 weeks, apart from SMPG, which was performed twice throughout the study by the participants. SMPG measurements were performed with capillary blood test strips, which automatically calibrated blood to plasma equivalent glucose values. Patient-reported outcomes questionnaires, including the Short Form‐36v2 (SF‐36v2) health survey and Diabetes Treatment Satisfaction Questionnaire status (DTSQs), were completed at baseline and after 30 weeks.
All adverse events (AEs) were collected throughout the study, including events starting from the first trial-related activity after signing the informed consent until the end of the 5-week post-treatment follow-up period and recorded at prespecified study visits. Severe or blood glucose (BG)-confirmed symptomatic hypoglycaemic episodes were recorded throughout the study.
Statistical Analysis
Post hoc analyses were based on the full analysis set (FAS), including all randomised participants who received a treatment dose and had any post-randomisation data. The statistical evaluation of the FAS followed the intention-to-treat principle.
Efficacy subgroup analyses for endpoints assessing change from baseline were performed using a mixed model for repeated measures with all post-baseline measurements obtained at planned visits up to and including week 30 data, before discontinuation from randomised treatment or initiation of rescue treatment as the dependent variables. Visit and treatment were included as fixed factors and the associated baseline values as covariates. For measurements within the same participants, an unstructured covariance matrix was used. Estimated treatment differences (ETDs) were shown comparing OW semaglutide with OD sitagliptin at week 30 by both dose levels, with p < 0.05 indicating a statistically significant difference.
Variables related to fixed responses in HbA1c or weight loss (yes/no) at week 30 were evaluated with logistic regression and treatment as a fixed effect adjusted for relevant baseline response(s).
It was assumed that any missing data were missing at random. Sensitivity analyses including pattern mixture models were used to address the impact of any missing values. Efficacy results are described by odds ratios (OR) and the associated 95% confidence interval (CI). Data are shown as mean (standard deviation [SD]) unless otherwise specified.
Safety endpoints were summarised and evaluated by descriptive statistics using the safety analysis set (SAS), which included all participants exposed to at least one dose of randomised semaglutide or sitagliptin.
Ethical Approval
The trial was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practice and was approved by an Institutional Review Board (Seoul National University Bundang Hospital [B-1705/395-002], The Catholic University of Korea, St. Vincent’s Hospital [VIRB-[sin]20170518-036], Seoul National University Hospital [H-1706-022-857], Severance Hospital [4-2017-0212], Korea University Anam Hospital [ED17090], Hallym University Kangnam Sacred Heart Hospital [HKS 2018-01-002]). Informed consent was obtained from all participants prior to enrolment in the study.
Results
Of the 868 participants with T2D originally enrolled in the NN9535-4114 trial, 110 from the Republic of Korea were included at study initiation. Study participants were treated with semaglutide 0.5 mg (n = 35), semaglutide 1.0 mg (n = 40), or sitagliptin 100 mg (n = 35). The trial was completed by 93 (84.5%) of the study participants and 87 (79.1%) participants completed randomised treatment throughout the trial period (Table S1). Overall, 23 patients (20.9%) discontinued treatment prematurely, with 14 (12.7%) participants discontinuing because of AEs.
Demographics and Clinical Characteristics
The mean (SD) age of the study population was 55.4 (11.4) years, with 58 male participants (52.7%), having mean (SD) diabetes duration of 7.8 (6.3) years and mean (SD) BMI of 27.0 (4.8) kg/m2 (Table 1). Baseline characteristics were generally balanced across treatment arms. A slight variation was observed in mean (SD) body weight across the treatment groups, with 75.6 kg (19.9) and 73.4 kg (15.9) in the semaglutide 0.5 mg and 1.0 mg groups, respectively, versus 68.6 kg (11.5) for sitagliptin 100 mg (Table 1). The percentage of participants with a history of dyslipidaemia was higher in the semaglutide 0.5 mg group (42.9%) compared with semaglutide 1.0 mg (25.0%) and sitagliptin 100 mg (25.7%), although the imbalance in the proportion of participants receiving statins as a concomitant medication was less pronounced across the groups treated with semaglutide 0.5 mg (57.1%), semaglutide 1.0 mg (45.0%), and sitagliptin 100 mg (48.6%).
Efficacy
Assessment of the primary endpoint of change in HbA1c from baseline to week 30 showed a reduction of 1.6% with semaglutide 0.5 mg and 1.8% with semaglutide 1.0 mg versus 0.9% with sitagliptin 100 mg in Korean participants (ETD –0.64 [95% CI –1.03; –0.26], p = 0.0015 and –0.88 [95% CI: –1.27; –0.50], p < 0.0001, respectively; Table 2; Fig. 1).

Primary and secondary efficacy endpoints (HbA1c and body weight) from baseline to week 30. a Estimated change in mean HbA1c by week and estimated change in mean HbA1c after 30 weeks. b Estimated change in mean body weight by week and estimated change in mean body weight after 30 weeks. Error bars indicate standard errors of the means. *p < 0.05, indicating a statistically significant difference. CI confidence interval, ETD estimated treatment difference. Reproduced from Ji et al. [26]. This work is licensed under the Creative Commons Attribution-NonCommercial 4.0 International License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc/4.0/ or send a letter to Creative Commons, PO Box 1866, Mountain View, CA 94042, USA
Body weight in the Korean population decreased by 2.7 kg with semaglutide 0.5 mg and by 4.8 kg with semaglutide 1.0 mg, corresponding with a reduction in body weight percentage of 3.9% and 7.3%, respectively, from baseline to week 30. In contrast, in participants receiving sitagliptin 100 mg, both absolute body weight (0.5 kg [ETD –3.15 [95% CI: –4.79; –1.51], p = 0.0002 vs semaglutide 0.5 mg, and –5.26 [95% CI: –6.89; –3.63], p < 0.0001 vs semaglutide 1.0 mg) and body weight percentage (0.9% [ETD –4.80 [95% CI: –7.31; –2.30], p = 0.0003 vs semaglutide 0.5 mg, and –8.23 [95% CI: –10.72; –5.75], p < 0.0001 vs semaglutide 1.0 mg) increased (Table 2; Fig. 1).
Differences in HbA1c and body weight across treatment groups were observed within the first 8 weeks and increased over time (Fig. 1).
A greater proportion of participants achieved the target of HbA1c < 7.0% with semaglutide 0.5 mg (80.0%) and semaglutide 1.0 mg (87.5%) compared with sitagliptin 100 mg (54.3%; Fig. 2A). These results were in line with the proportion of participants achieving the HbA1c target of ≤ 6.5%, where more participants treated with semaglutide 0.5 mg (60.0%) and semaglutide 1.0 mg (67.5%) achieved this target compared with the study population treated with sitagliptin 100 mg (25.7%; Fig. 2B).

Proportion of participants achieving a HbA1c target < 7.0%, b HbA1c target ≤ 6.5%, c WL ≥ 5%, and d composite endpoint of HbA1c target < 7.0% without severe or BG-confirmed symptomatic hypoglycaemia and weight gain. aHbA1c < 7.0% without severe or BG-confirmed symptomatic hypoglycaemia and without weight gain on treatment without rescue medication. BG blood glucose, BW body weight, CI confidence interval, OR odds ratio, WL weight loss
A statistically significant proportion of participants in the semaglutide 0.5 mg (42.9%) and semaglutide 1.0 mg (65.0%) groups achieved ≥ 5% weight loss compared with none of the participants in the sitagliptin 100 mg group after 30 weeks (0.0%; Fig. 2C). In addition, a statistically significant reduction in BMI and waist circumference was observed for both doses of semaglutide compared with sitagliptin 100 mg (Table 2).
More participants receiving semaglutide 0.5 mg (71.4%) and 1.0 mg (77.5%) achieved the composite endpoint (HbA1c < 7.0% without severe or BG-confirmed symptomatic hypoglycaemia and without weight gain) after 30 weeks compared with participants receiving sitagliptin 100 mg (31.4%; p = 0.0005 and p < 0.0001, respectively; Fig. 2D).
The reductions in mean fasting plasma glucose, mean seven-point SMPG, and incremental SMPG were also greater with both doses of semaglutide than with sitagliptin after 30 weeks (Table 2). Regarding the β-cell function, HOMA-B, proinsulin, and proinsulin/insulin ratio consistently showed favourable effects with semaglutide 0.5 mg and 1.0 mg over sitagliptin 100 mg after 30 weeks compared with baseline (Fig. S1).
A numerical reduction in systolic blood pressure was reported for both doses of semaglutide compared with sitagliptin; however, this was only statistically significant for semaglutide 1.0 mg versus sitagliptin (Table S2). No difference between change from baseline in lipid parameters was observed across the treatment groups (Fig. S2).
For patient-reported outcomes, the change from baseline to week 30 in DTSQ score was greater for semaglutide 0.5 mg versus sitagliptin 100 mg, reflecting a greater semaglutide treatment satisfaction for this dosing compared with sitagliptin 100 mg (Fig. S3). No significant differences were observed for the change in the overall DTSQ score when comparing semaglutide 1.0 mg with sitagliptin 100 mg, or for change in the SF-36v2 score from baseline to week 30 between semaglutide and sitagliptin treatment (Fig. S3).
Adverse Events
The proportion of participants experiencing AEs was lower for semaglutide 0.5 mg (45.7%) compared with sitagliptin 100 mg (57.1%). A higher proportion of participants (70.0%) in the semaglutide 1.0 mg group vs sitagliptin 100 mg experienced AEs, with the majority of these being mild and moderate (Table 3). There was one death during the study in the semaglutide 1.0 mg group, categorised as sudden death and unlikely related to treatment. The five serious AEs reported for semaglutide 1.0 mg and one for sitagliptin 100 mg were classified under gastrointestinal (GI) disorders, blood and lymphatic system disorders, hepatobiliary disorders, and injury, poisoning and procedural complications and were possibly or unlikely treatment related. Regarding AEs leading to premature discontinuation, a higher proportion was seen for semaglutide 0.5 mg and 1.0 mg doses (8.6% and 27.5%, respectively) compared with none for the sitagliptin 100 mg group. GI AEs were generally mild and more common in the participants receiving semaglutide, with nausea, diarrhoea, vomiting, and dyspepsia the most frequently reported (Table S3). No episodes of severe or BG-confirmed hypoglycaemia were reported (Table 3).
Discussion
This was the first analysis to our knowledge on the efficacy of OW semaglutide administered in a Korean population with T2D inadequately controlled on metformin in a randomised clinical trial setting. The current observations demonstrated that OW semaglutide therapy was efficacious in improving glycaemic control and reducing body weight in Korean adults with T2D. These results are aligned with previous observations investigating treatment of T2D with OW semaglutide in Japanese adults and across the global SUSTAIN clinical trial programme [16,17,18,19,20,21,22, 24, 25, 27, 28]. After 30 weeks of OW semaglutide treatment, the current results from the Korean subpopulation displayed a slightly greater numerical difference in HbA1c, body weight, and composite target endpoints compared with the full NN9535-4114 trial where approximately 85% of the population was Asian [26]. However, the difference was minimal.
In addition to glycaemic control, body weight management is increasingly acknowledged to be an important factor in T2D treatment programmes for Asian populations [8]. From an epidemiological standpoint, evidence suggests that Asian populations tend to develop T2D at a lower BMI and at a younger age than Western populations, which might have implications for diabetes management [29]. In the SUSTAIN 1, 2, 5, and 9 clinical trials, for example, a post hoc analysis showed that the treatment effect with OW semaglutide on HbA1c was greater in the Japanese cohort across the four studies compared with the total population covering global populations (–1.69 to –2.49% vs –1.32 to –1.85%), and a similar trend was noted in relative body weight reduction [27]. The authors suggested that these observations may be due to differences in the genetic variants, as genetic variants associated with T2D have been identified in people of East Asian descent that have not previously been detected in people of European descent [30, 31] as well as T2D pathophysiology. In particular, some genetic variants (e.g., NKX6-3, or NK6 homeobox 3, and ANK1) display multiple influences on the development of T2D, including affecting both insulin production and insulin resistance [32]. Additionally, lower fasting C-peptide levels consistent with impaired β-cell function were also observed in Asian populations without a history of diabetes [31, 33].
Observations of a potential increased efficacy of semaglutide in the Japanese population were confirmed in a real-world study that demonstrated a significant reduction in HbA1c from baseline to 6 months with semaglutide, with most study participants receiving lower OW semaglutide dosing of 0.25 mg and 0.50 mg [34]. Determination of the optimal OW semaglutide dose for Korean adults with T2D will be warranted in future real-world studies.
OW semaglutide therapy previously demonstrated a statistically significant reduction in the rate of CV death, non-fatal myocardial infarction, and non-fatal stroke in people with T2D and a high CV risk [21]. The beneficial effects of semaglutide on HbA1c, body weight, and BP observed here may therefore contribute to improvements in cardiometabolic risk factors.
In addition, the safety profile of semaglutide in Korean adult participants was consistent with previous observations when using GLP-1RAs, and included mainly mild and transient GI effects, with most participants recovering from GI AEs over time [35]. The rate of AEs and serious AEs was lower for semaglutide 0.5 mg in the Korean subpopulation (45.7% and 0.0%, respectively) compared with the overall NN9535-4114 study population (72.8% and 6.3%, respectively), while being similar for semaglutide 1.0 mg and sitagliptin 100 mg across both populations [26]. This variation might be due to the relatively small study population. In addition, no episodes of severe or BG-confirmed hypoglycaemia were reported among the current treatment groups, which is consistent with the low number of such events observed in the total NN9535-4114 population [26]. An increase in AEs and proportion of premature discontinuation with increasing semaglutide dosing was observed compared with sitagliptin, albeit to a lesser extent than observed in the NN9535-4114 study.
The rate of GI AEs for semaglutide was similar, and increased with increasing dose, in the Korean subpopulation compared with the total NN9535-4114 study population and was in accordance with the SUSTAIN programme [16,17,18,19,20,21,22,23,24,25,26,27]. An individualised treatment approach, including appropriate dose up-titration, to manage GI AEs might be considered for Korean adults with T2D requiring OW semaglutide [36].
The 2021 Clinical Practice Guidelines for Diabetes Mellitus of the KDA recommend a clinical target to prevent and delay vascular complications of HbA1c < 6.5%, a body weight reduction of ≥ 5%, BP < 140/85 mmHg, and LDL cholesterol < 100 mg/dl [8]. If the patient has not achieved HbA1c targets, has severe hyperglycaemia, or has atherosclerotic CV disease or chronic kidney disease (eGFR < 60 ml/min/1.73 m2 or urine albumin:creatinine ratio ≥ 30 mg/g), GLP-1RAs are recommended as an option for combination therapy with metformin, insulin, sulfonylurea, thiazolidinedione, or sodium-glucose cotransporter-2 inhibitor [7]. A study performed in Korea during 2019–2020 showed that among adults diagnosed with diabetes, 61.4% were receiving oral glucose-lowering medications or insulin, and 24.5% of this population achieved an HbA1c target of < 6.5% [4]. Only 9.7% of adults diagnosed and treated for T2D achieved all three goals of HbA1c < 6.5%, BP < 140/85 mmHg, and LDL cholesterol < 100 mg/dl as defined by the KDA [4]. However, in the current study, > 60% of Korean participants with T2D reached HbA1c levels ≤ 6.5%, and about half of the population reached a body weight loss target of ≥ 5% after 30 weeks of treatment with OW semaglutide.
The strength of this study is that it is the first evaluation of OW semaglutide in a Korean population with T2D. Limitations of the current study, which should also be considered for future studies, include the post hoc nature of the analysis, meaning that assessed outcomes were not prespecified in the original study protocol. In addition, a small number of participants were included in this study, which was insufficient to evaluate the effect of OW semaglutide, for example, in relevant subgroups based on body weight or obesity categories in a Korean population. The relatively short study duration of 30 weeks also warrants longer-term future studies to confirm the current findings.
Conclusions
These data confirm the efficacy and safety profile of OW semaglutide (0.5 and 1.0 mg) versus OD sitagliptin by improving both glycaemic control and reducing body weight in a Korean population with T2D. The current results support the use of OW semaglutide in the management of Korean adults with T2D and offers a relevant treatment option for T2D in a Korean population.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.
References
Nanda M, Sharma R, Mubarik S, et al. Type-2 Diabetes mellitus (T2DM): spatial-temporal patterns of incidence, mortality and attributable risk factors from 1990 to 2019 among 21 world regions. Endocrine. 2022;77:444–54.
World Health Organization. Diabetes [Internet]. 2023 [cited 20 April 2023]. Available from https://www.who.int/news-room/fact-sheets/detail/diabetes.
Kim JH, Lim JS. Trends of diabetes and prediabetes prevalence among Korean adolescents from 2007 to 2018. J Korean Med Sci. 2021;36:e112.
Bae JH, Han KD, Ko SH, et al. Diabetes fact sheet in Korea 2021. Diabetes Metab J. 2022;46:417–26.
Oh SH, Ku H, Park KS. Prevalence and socioeconomic burden of diabetes mellitus in South Korean adults: a population-based study using administrative data. BMC Public Health. 2021;21:548.
Leitner DR, Frühbeck G, Yumuk V, et al. Obesity and type 2 diabetes: two diseases with a need for combined treatment strategies—EASO can lead the way. Obes Facts. 2017;10:483–92.
Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41:2669–701.
Hur KY, Moon MK, Park JS, et al. 2021 Clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J. 2021;45:461–81.
Lee KA, Kim DJ, Han K, et al. Screening for prediabetes and diabetes in Korean nonpregnant adults: a position statement of the Korean Diabetes Association, 2022. Diabetes Metab J. 2022;46:819–26.
Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27:740–56.
Ahrén B. Glucagon-like peptide-1 receptor agonists for type 2 diabetes: a rational drug development. J Diabetes Investig. 2019;10:196–201.
Sheahan KH, Wahlberg EA, Gilbert MP. An overview of GLP-1 agonists and recent cardiovascular outcomes trials. Postgrad Med J. 2020;96:156–61.
Granata A, Maccarrone R, Anzaldi M, et al. GLP-1 receptor agonists and renal outcomes in patients with diabetes mellitus type 2 and diabetic kidney disease: state of the art. Clin Kidney J. 2022;15:1657–65.
Ard J, Fitch A, Fruh S, et al. Weight loss and maintenance related to the mechanism of action of glucagon-like peptide 1 receptor agonists. Adv Ther. 2021;38:2821–39.
Baggio LL, Drucker DJ. Glucagon-like peptide-1 receptors in the brain: controlling food intake and body weight. J Clin Invest. 2014;124:4223–6.
Sorli C, Harashima S-I, Tsoukas GM, et al. Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol. 2017;5:251–60.
Ahrén B, Masmiquel L, Kumar H, et al. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): a 56-week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol. 2017;5:341–54.
Ahmann AJ, Capehorn M, Charpentier G, et al. Efficacy and safety of once-weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): a 56-week, open-label, randomized clinical trial. Diabetes Care. 2017;41:258–66.
Aroda VR, Bain SC, Cariou B, et al. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): a randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol. 2017;5:355–66.
Rodbard HW, Lingvay I, Reed J, et al. Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): a randomized, controlled trial. J Clin Endocrinol Metab. 2018;103:2291–301.
Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375:1834–44.
Pratley RE, Aroda VR, Lingvay I, et al. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018;6:275–86.
Aroda VR, Ahmann A, Cariou B, et al. Comparative efficacy, safety, and cardiovascular outcomes with once-weekly subcutaneous semaglutide in the treatment of type 2 diabetes: Insights from the SUSTAIN 1–7 trials. Diabetes Metab. 2019;45:409–18.
Zinman B, Bhosekar V, Busch R, et al. Semaglutide once weekly as add-on to SGLT-2 inhibitor therapy in type 2 diabetes (SUSTAIN 9): a randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2019;7:356–67.
Capehorn MS, Catarig AM, Furberg JK, et al. Efficacy and safety of once-weekly semaglutide 1.0 mg vs once-daily liraglutide 1.2 mg as add-on to 1–3 oral antidiabetic drugs in subjects with type 2 diabetes (SUSTAIN 10). Diabetes Metab. 2020;46:100–9.
Ji L, Dong X, Li Y, et al. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as add-on to metformin in patients with type 2 diabetes in SUSTAIN China: a 30-week, double-blind, phase 3a, randomized trial. Diabetes Obes Metab. 2021;23:404–14.
Araki E, Harashima S, Nishida T, et al. Efficacy and safety of once-weekly semaglutide in Japanese individuals with type 2 diabetes in the SUSTAIN 1, 2, 5 and 9 trials: post-hoc analysis. J Diabetes Investig. 2022;13:1971–80.
Lingvay I, Catarig A-M, Frias JP, et al. Efficacy and safety of once-weekly semaglutide versus daily canagliflozin as add-on to metformin in patients with type 2 diabetes (SUSTAIN 8): a double-blind, phase 3b, randomised controlled trial. Lancet Diabetes Endocrinol. 2019;7:834–44.
Ma RC, Chan JC. Type 2 diabetes in East Asians: similarities and differences with populations in Europe and the United States. Ann NY Acad Sci. 2013;1281:64–91.
Hu C, Jia W. Diabetes in China: epidemiology and genetic risk factors and their clinical utility in personalized medication. Diabetes. 2018;67:3–11.
Kwak SH, Chae J, Lee S, et al. Nonsynonymous variants in PAX4 and GLP1R are associated with type 2 diabetes in an East Asian population. Diabetes. 2018;67:1892–902.
Spracklen CN, Horikoshi M, Kim YJ, et al. Identification of type 2 diabetes loci in 433,540 East Asian individuals. Nature. 2020;582:240–5.
Ohn JH, Kwak SH, Cho YM, et al. 10-year trajectory of β-cell function and insulin sensitivity in the development of type 2 diabetes: a community-based prospective cohort study. Lancet Diabetes Endocrinol. 2016;4:27–34.
Yamada H, Yoshida M, Suzuki D, et al. Effectiveness and safety of once-weekly semaglutide in Japanese patients with type 2 diabetes in treatment intensification: a retrospective observational single-center study. Diabetes Ther. 2022;13:1779–88.
Smits MM, Van Raalte DH. Safety of semaglutide. Front Endocrinol (Lausanne). 2021;12:645563.
Wharton S, Davies M, Dicker D, et al. Managing the gastrointestinal side effects of GLP-1 receptor agonists in obesity: recommendations for clinical practice. Postgrad Med. 2022;134:14–9.
Acknowledgements
The authors thank the investigators, study staff, and patients for their participation.
Medical writing and editorial support
The authors also thank Boram Bae (Novo Nordisk) for manuscript review, supervision, and support and Leni Vandekerckhove (AXON Communications) for writing assistance funded by Novo Nordisk.
Funding
The current analysis, medical writing assistance, and the Rapid Service Fee were funded by Novo Nordisk.
Author information
Authors and Affiliations
Contributions
Byung-Wan Lee, Young Min Cho, Sin Gon Kim, Seung-Hyun Ko, Soo Lim, Amine Dahaoui, Jin Sook Jeong, Hyo Jin Lim, and Jae Myung Yu contributed to the interpretation of data, the writing and critical revisions of the manuscript at all stages of development. Byung-Wan Lee, Young Min Cho, Sin Gon Kim, Seung-Hyun Ko, Soo Lim, Amine Dahaoui, Jin Sook Jeong, Hyo Jin Lim, and Jae Myung Yu approved the final submitted manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Byung-Wan Lee, Sin Gon Kim, Seung-Hyun Ko, Soo Lim, and Jae Myung Yu declare that there is no conflict of interest. Young Min Cho has received grants from Daewoong Pharmaceutical, Sanofi Korea and LG Chemical and has received consulting fees from LG Chemical. Amine Dahaoui, Jin Sook Jeong, and Hyo Jin Lim are employees of Novo Nordisk.
Ethical Approval
The trial was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practice and was approved by an Institutional Review Board (Seoul National University Bundang Hospital [B-1705/395-002], The Catholic University of Korea, St. Vincent’s Hospital [VIRB-[sin]20170518-036], Seoul National University Hospital [H-1706-022-857], Severance Hospital [4-2017-0212], Korea University Anam Hospital [ED17090], Hallym University Kangnam Sacred Heart Hospital [HKS 2018-01-002]). Informed consent was obtained from all participants prior to enrolment in the study.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Lee, BW., Cho, Y.M., Kim, S.G. et al. Efficacy and Safety of Once-Weekly Semaglutide Versus Once-Daily Sitagliptin as Metformin Add-on in a Korean Population with Type 2 Diabetes. Diabetes Ther 15, 547–563 (2024). https://doi.org/10.1007/s13300-023-01515-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-023-01515-0