
Abstract
This commentary analyzes the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial, which has reported the cardiovascular benefits of liraglutide. It places the results of this seminal trial in the context of the evolution of diabetes care, compares them with other recently published cardiovascular outcome trials, and suggests novel mechanisms to explain the benefits and properties of liraglutide. The editorial discusses the potential impact that LEADER will have on the prevention and management of diabetes and its vascular complications.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Secular Trends in Diabetology
Modern diabetology, which traces its beginning to the discovery of insulin, has witnessed various landmark events, and experienced significant changes in its approach since then. Screening tests, diagnostic cutoffs, investigative modalities, parameters for follow-up, treatment strategies and management goals, all have evolved over the past century.
In general, we have moved from an autocratic, empirical, physician-oriented, gluco-centric biomedical model to a pantisocratic, evidence-based, patient-centered, comprehensive metabolic control approach based upon a biopsychosocial framework [1–3]. Instead of focusing solely on glycemic indicators, we now rely on comprehensive parameters, including weight, blood pressure and lipids, to assess quality of care. We have also begun measuring meaningful outcomes, such as disease-free life span, survival rates, and time to important events such as stroke, myocardial infarction and heart failure, instead of relying on surrogate markers.
These developments have been made possible by multiple advances in science. Greater knowledge of etiology, pathogenesis, and natural history of diabetes, coupled with a multi-dimensional, holistic understanding of diabetic complications has led to changes in our approach to diabetes. These changes have been facilitated by technological improvements in diagnostic and treatment interventions, which have allowed the achievement of hitherto difficult to achieve targets and goals.
Cardiovascular Outcome Trials
Modern diabetes care expects not only symptomatic and biochemical control from glucose-lowering drugs, but also requires long-term improvement in micro-vascular health, macrovascular health, and overall survival. While the impact of such drugs on glucose control can be assessed by short-term trials, their effect on cardiovascular outcomes (CVO) needs studies of longer duration. Such trials, termed CVO trials, are mandatory for all newly registered drugs, as cardiovascular (CV) disease is the main contributor to mortality in persons with diabetes [4]. Newer molecules such as saxagliptin, sitagliptin, empagliflozin and lixisenatide have reported CVO in the past few years, adding to our knowledge and understanding [5–8].
The LEADER Trial
The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial (NCT01179048) is one such landmark trial [9]. The results of LEADER have been discussed on various platforms. In this commentary, we summarize the findings of LEADER (Table 1), suggest novel hypotheses to explain the benefits of liraglutide, and discuss how this trial will influence the future of diabetes care.
Results
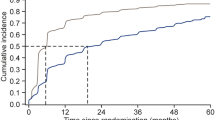
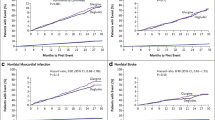
In LEADER, the primary outcome was a composite of three major adverse cardiovascular (CV) events (three-point MACE), defined as first occurrence of death from CV causes, non-fatal myocardial infarction (MI), or non-fatal stroke. Table 1 summarizes the findings of this study, which revealed a significant 13% reduction in the primary outcome, a significant 22% fall in CV death, and a numerical, but statistically non-significant lowering of risk of non-fatal MI and non-fatal stroke [9].
Death from CV causes was reduced in participants taking liraglutide in LEADER (hazard ratio (HR) 0.8). A similar lowering of all-cause mortality was noticed in this group (HR 0.8 5). As 219 out of 381 deaths in the liraglutide arm (57.5%) and 278 out of 447 deaths in the placebo arm (62.2%) occurred due to CV causes, the major driver of improvement in all-cause death seemed to be the CV benefit of liraglutide [9].
All types of vascular disease were attenuated with liraglutide, including MI, stroke and heart failure, even though statistical significance could not be demonstrated for individual endpoints. It is certain, however, that the benefits of the drug extended to all vascular beds and to the myocardium as well.
Comparison with Other Trials
It is self-evident that various CVO trial results be compared with each other (Table 2). However, it must be noted that CVO trials are not head-to-head trials of two molecules [barring a few exceptions such as DEVOTE (NCT01959529), CAROLINA (NCT01243424) and TOSCA. IT (NCT00700856)] [10–12]. The results of these trials are influenced by various factors in study design such as inclusion criteria, baseline medication use, quality of ‘standard of care’, duration of follow-up, and statistical plan. This implies that while LEADER and EMPA-REG OUTCOME (NCT01131676) can be discussed together, their results cannot be compared numerically. While EMPA-REG OUTCOME has been able to demonstrate CV benefits of empagliflozin, there are subtle differences in its results, as compared to those of liraglutide. Liraglutide has a gradually developing positive effect on all aspects of CV disease and mortality, while empagliflozin has a relatively faster effect on CV mortality and heart failure, but a numerically negative effect on stroke [7]. The number needed to treat (NNT) to prevent coronary events or deaths is much lower with empagliflozin than with liraglutide (Table 2). This raises questions about the economic viability of extrapolating the results of these trials to routine clinical practice. ELIXA (NCT01147250), which studied lixisenatide, a shorter acting glucagon-like peptide-1 receptor agonist (GLP-1 RA), has demonstrated CV safety of the molecule, but could not find significant CV benefit of its use [8].
Calorie Restriction Mimicry
The authors of LEADER suggest that liraglutide modifies progression of atherosclerotic disease [9]. We highlight another facet of this drug which can be used to explain its beneficial action. Calorie restriction has long been known to improve longevity in both animal and human species [13]. Calorie restriction mimicry, using drugs designed to act on the adenosine monophosphate kinase (AMPK) pathway, in a manner similar to that of calorie restriction, has also been tried to achieve similar benefits. Perhaps, the most well-known calorie restriction mimetic is metformin, which has also shown improved outcomes in the UKPDS (United Kingdom Prospective Diabetes Study) trial (ISRCTN 75451837) [14].
Liraglutide acts as a direct calorie restrictor by reducing appetite, and also as a calorie restriction mimetic by modifying AMPK action. Its actions on the hypothalamus, gastrointestinal tract and pancreas are designed to mimic a state of calorie restriction [13, 15, 16]. This facet of liraglutide’s mechanism of action needs detailed study.
Cholelithiasis
Another facet of the LEADER study that deserves close attention is the incidence of cholelithiasis. LEADER reports exceptional safety and tolerance with liraglutide, finding no increase in the risk of pancreatitis or neoplasms. There is, however, a higher risk of cholelithiasis in persons treated with liraglutide [9]. Risk factors for cholelithiasis that operate in the general population also tend to occur in participants of CVO trials. These include older age, female gender, heavy body weight and hypertriglyceridemia [17]. A higher incidence of gallstones has also been reported with exenatide [18].
While GLP-1-specific mechanisms have been postulated for this, such as reduced cholecystokinin, slower biliary tract motility and increased stasis of bile, it must be noted that cholelithiasis is a risk inherent to every weight-lowering therapy, including very low-calorie diet [19]. Gallstones may develop as soon as 4 weeks after initiation of weight-reducing diet. Hypotheses that have been suggested include an increase in cholesterol output, due to increased mobilization of tissue cholesterol to bile; increased gall bladder secretion of mucin and calcium; increased presence of prostaglandin E2 and arachidonic acid in bile; super-saturation of cholesterol in bile, due to reduced bile salt secretions; gall bladder stasis due to reduced stimulation by low-fat diet [20].
Primary and Secondary Prevention
Liraglutide provides comprehensive metabolic modulation, including weight, systolic blood pressure and lipid control. Similar results are seen with empagliflozin as well. Once again, subtle differences are visible to the discerning eye. Empagliflozin has a diuretic effect, and reduces both systolic and diastolic blood pressure, without causing reflex tachycardia. However, its effects on lipid profile are not significant. Direct hemodynamic effects on the heart and vasculature are also suggested, as it has a more marked benefit on heart failure than on coronary events [21]. Liraglutide has a greater effect on body weight, systolic blood pressure and lipids, and seems to modify the progression of the basic atherosclerotic process in diabetes.
It may be that liraglutide prevents the actual CV event (primary prevention) while empagliflozin reduces mortality after the event (secondary prevention) [22]. However, though the numerical data from LEADER are in favor of this statement, more research is needed to support this claim.
Richard the Lionheart and Robin Hood
The ‘Robin Hood effect’ has been suggested as a moniker for the metabolic effects of sodium glucose cotransporter-2 (SGLT2) inhibitors, which shift energy production from carbohydrate metabolism to lipid metabolism [23]. In a similar (Anglo-centric) vein, the term Lion Heart effect may be used to describe liraglutide. Richard the Lionheart was an iconic twelfth century English king who was famous for his military prowess. Richard the Lionheart and Robin Hood are shown as contemporaries in various quasi-historical accounts. The results of LEADER suggest a Ricardian property of liraglutide, which provides vascular safety and benefit, and modifies the natural history of diabetes in a favorable manner.
Influence and Impact: Follow the LEADER
The LEADER trial, which studied the effect of liraglutide on CVO has changed much more than the clinical usage of liraglutide. Reported recently, its results place LEADER in the same league as the DCCT (Diabetes Control and Complications Trial) (NCT00360815) and UKPDS trials [24, 25]. These studies have contributed immeasurably to modern diabetes care, and their impact cannot be understated. The results of ongoing trials such as EXSCEL (exenatide once weekly) and REWIND (dulaglutide) will also modify the way in which we view LEADER [25, 26]. The EXenatide Study of Cardiovascular Event Lowering (EXSCEL) study (NCT01144338) will assess the impact of exenatide once weekly on major CV outcomes. EXSCEL is a double-blind, pragmatic placebo-controlled trial being conducted in 35 countries on 14,000 participants with type 2 diabetes mellitus (T2DM) and a broad range of CV risk over approximately 5 years. The Researching Cardiovascular Events With a Weekly Incretin in Diabetes (REWIND) trial (NCT01394952), being carried out in 9600 participants over nearly 7 years, evaluates whether dulaglutide, administered by a once-weekly injection, can prevent the appearance of CV complications in people with type 2 diabetes. Both EXSCEL and REWIND results will be eagerly awaited, to see if the benefits obtained in LEADER are liraglutide specific or are a class effect of long-acting and intermediate-acting GLP1-RA.
Liraglutide has shown robust benefits, which extend beyond its glucose-lowering effect. Currently, it is the only glucose-lowering drug which is approved for use as an anti-obesity treatment in euglycemic persons as well. LEADER adds to this spectrum of use by encouraging its use in persons with diabetes at high risk of CV disease, and high risk of renal disease. The drug has been shown to have both macro- and micro-vascular benefits, and this allows its use as a pan-vascular preventive molecule apart from being a glucose-lowering treatment. LEADER data suggest that liraglutide can be used for secondary prevention (prevention of MI and stroke), and strongly supports its use for tertiary prevention (prevention of fatality after occurrence of MI or stroke). Long-term studies are still required to assess its utility in primary prevention, i.e., prevention of CV events and death in persons without diabetes or other lower risk populations.
Conclusion
The LEADER trial contributes to the evolution of diabetes care in a significant manner, and will certainly find a place as a milepost in the history of diabetes. Its results provide evidence that a single drug can be used to provide not only comprehensive glycemic and metabolic control but also achieve beneficial CV outcomes. These benefits occur at all vascular bed sites, viz., coronary and cerebrovascular, and do not impair myocardial function (as shown by lack of increase in heart failure). Viewed from this vantage point, LEADER should immensely help improve the way in which we care for people with diabetes.
References
Baruah MP, Kalra B, Kalra S. Patient centred approach in endocrinology: from introspection to action. Indian J Endocrinol Metab. 2012;16(5):679.
Chinenye S, Ogbera AO, Kalra S. Patient-centered care in diabetology: Sub-Saharan African perspectives. Afr J Diabetes Med. 2014;22(1):5–8.
Kalra S, Megallaa MH, Jawad F. Patient-centered care in diabetology: from eminence-based, to evidence-based, to end user-based medicine. Indian J Endocrinol Metab. 2012;16(6):871.
John M, Unnikrishnan AG, Kalra S, Nair T. Cardiovascular outcome trials for anti-diabetes medication: A holy grail of drug development? Indian Heart J. 2016;68(4):564–71.
Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, Ohman P, Frederich R, Wiviott SD, Hoffman EB, Cavender MA. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369(14):1317–26.
Green JB, Bethel MA, Armstrong PW, Buse JB, Engel SS, Garg J, Josse R, Kaufman KD, Koglin J, Korn S, Lachin JM. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;373(3):232–42.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–28.
Pfeffer MA, Claggett B, Diaz R, Dickstein K, Gerstein HC, Køber LV, Lawson FC, Ping L, Wei X, Lewis EF, Maggioni AP. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med. 2015;373(23):2247–57.
Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, Nissen SE, Pocock S, Poulter NR, Ravn LS, Steinberg WM. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311–22.
Marso SP, McGuire DK, Zinman B, Poulter NR, Emerson SS, Pieber TR, Pratley RE, Haahr P-M, Lange M, Frandsen KB, Rabol R, Buse JB. Design of DEVOTE (trial comparing cardiovascular safety of insulin degludec vs insulin glargine in patients with type 2 diabetes at high risk of cardiovascular events)—DEVOTE 1. Am Heart J. 2016;17(179):175–83.
Rosenstock J, Marx N, Kahn SE, Zinman B, Kastelein JJ, Lachin JM, Bluhmki E, Patel S, Johansen OE, Woerle HJ. Cardiovascular outcome trials in type 2 diabetes and the sulphonylurea controversy: rationale for the active-comparator CAROLINA trial. Diabetes Vasc Dis Res. 2013;10(4):289–301.
Vaccaro O, Masulli M, Bonora E, Del Prato S, Nicolucci A, Rivellese AA, Riccardi G;, TOSCA.IT Study Group. The TOSCA.IT trial: a study designed to evaluate the effect of pioglitazone versus sulfonylureas on cardiovascular disease in type 2 diabetes. Diabetes Care. 2012;35(12):e82–e82.
Kalra S, Jacob JJ, Gupta Y. Newer antidiabetic drugs and calorie restriction mimicry. Indian J Endocr Metab. 2016;20:142–6.
UK Prospective Diabetes Study. UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33. Lancet. 1998;352(9131):837–53.
Beiroa D, Imbernon M, Gallego R, Senra A, Herranz D, Villarroya F, et al. GLP-1 agonism stimulates brown adipose tissue thermogenesis and browning through hypothalamic AMPK. Diabetes. 2014;63:3346–58.
Miao XY, Gu ZY, Liu P, Hu Y, Li L, Gong YP, et al. The human glucagon-like peptide-1 analogue liraglutide regulates pancreatic beta-cell proliferation and apoptosis via an AMPK/mTOR/P70S6K signaling pathway. Peptides. 2013;39:71–9.
Festi D, Villanova N, Colecchia A. Risk factors for gallstone formation during weight loss. Clin Gastroenterol Hepatol. 2015;13(3):613.
Keller J, Trautmann ME, Haber H, San Tham L, Hunt T, Mace K, Linnebjerg H. Effect of exenatide on cholecystokinin-induced gallbladder emptying in fasting healthy subjects. Regul Pept. 2012;179(1):77–83.
Johansson K, Sundström J, Marcus C, Hemmingsson E, Neovius M. Risk of symptomatic gallstones and cholecystectomy after a very-low-calorie diet or low-calorie diet in a commercial weight loss program: 1-year matched cohort study. Int J Obes. 2014;38(2):279–84.
McKenna LA, Drummond RS, Drummond S, Talwar D, Lean ME. Seeing double: the low-carb diet. Br Med J. 2013;2013(346):f2563.
Avogaro A, Fadine GP, Sesti G, Bonora E, Del Prato S. continued efforts to translate diabetes cardiovascular outcome trials into clinical practice. Cardiovasc Diabetol. 2016;15:111.
Kalra S. One small step for empagliflozin, one giant leap for diabetology. Diabetes Ther. 2015;6(4):405–9.
Kalra S, Jain A, Ved J, Unnikrishnan AG. Sodium-glucose cotransporter 2 inhibition and health benefits: The Robin Hood effect. Ind J Endocr Metab. [cited 2016 Aug 31]. http://www.ijem.in/preprintarticle.asp?id=183826. Accessed 31 Aug 2016 (Epub ahead of print).
Control TD, Group CT. Effect of intensive diabetes management on macrovascular events and risk factors in the diabetes control and complications trial. Am J Cardiol. 1995;75(14):894–903.
Holman RR, Bethel MA, George J, Sourij H, Doran Z, Keenan J, Khurmi NS, Mentz RJ, Oulhaj A, Buse JB, Chan JC. Rationale and design of the EXenatide Study of Cardiovascular Event Lowering (EXSCEL) trial. Am Heart J. 2016;30(174):103–10.
Eli Lilly and Company. Researching cardiovascular events with a weekly incretin in diabetes (REWIND). clinicaltrials.gov. Bethesda: National Library of Medicine; 2011–2013. NLM Identifier NCT01394952.
Acknowledgments
No funding or sponsorship was received for publication of this article. The named author meets the International Committee of Medical Journal Editors (ICMJE) criteria for authorship of this manuscript, takes responsibility for the integrity of the work as a whole, and has given final approval for the version to be published.
Disclosures
Sanjay Kalra has received honoraria/speaker’s fees from Novo Nordisk, sanofi-aventis, Boehringer Ingelheim, AstraZeneca, and Janssen and was a primary investigator for the LEADER trial.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by the author.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/0E76F0602BE61B31.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kalra, S. Follow the LEADER—Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results Trial. Diabetes Ther 7, 601–609 (2016). https://doi.org/10.1007/s13300-016-0197-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-016-0197-4