
Abstract
The purpose of this pictorial review is to illustrate chest imaging findings of cystic fibrosis (CF) using tomosynthesis (digital tomography), in comparison to radiography and computed tomography (CT). CF is a chronic systemic disease where imaging has long been used for monitoring chest status. CT exposes the patient to a substantially higher radiation dose than radiography, rendering it unsuitable for the often needed repeated examinations of these patients. Tomosynthesis has recently appeared as an interesting low dose alternative to CT, with an effective dose of approximately 0.08 mSv for children and 0.12 mSv for adults. Tomosynthesis is performed on the same X-ray system as radiography, adding only about 1 min to the normal examination time. Typical pulmonary changes in CF such as mucus plugging, bronchial wall thickening, and bronchiectases are shown in significantly better detail with tomosynthesis than with traditional radiography. In addition, the cost for a tomosynthesis examination is low compared to CT. To reduce the radiation burden of patients with CF it is important to consider low dose alternatives to CT, especially in the paediatric population. Tomosynthesis has a lower radiation dose than CT and gives a superior visualisation of pulmonary CF changes compared to radiography. It is important to further determine the role of tomosynthesis for monitoring disease progression in CF.
Similar content being viewed by others


Introduction
Cystic fibrosis (CF) is a chronic systemic disease where imaging has long been used for monitoring chest status, and for chest evaluation in exacerbation of the disease. Chest radiography has traditionally been used as the main imaging modality. Computed tomography (CT) is a superior imaging tool compared to radiography [1, 2], but despite its use for more than two decades has yet to show its true clinical value [3, 4]. CT exposes the patient to a substantially higher radiation dose than chest radiography, rendering it unsuitable for the often needed repeated examinations of these patients. Recently tomosynthesis (digital tomography) [5] has appeared as an interesting low dose alternative to chest CT, with significantly better delineation of CF changes than conventional radiography. The principle has been used in mammography for more than a decade. Technical developments have now led to the introduction of the technique also for chest [6–8], abdominal [9, 10] and musculoskeletal imaging [11, 12]. The aim of this pictorial essay is to give an overview of the tomosynthesis imaging findings in CF for different stages of the disease and to compare them to radiographic and CT findings in the same patients.
Tomosynthesis—technical considerations
Tomosynthesis images were acquired on a commercially available product (Definium 8000 and VolumeRAD; GE Healthcare, Chalfont St Giles, England). In chest tomosynthesis, tomographic images are generated from multiple low dose exposures directed towards a stationary digital amorphous silicon flat-panel detector, from tube angles of −17.5° to +17.5° of a moving X-ray tube. These exposures are used to reconstruct up to approximately 60 coronal sectional images with a nominal thickness of 3 mm for children and 4 mm for adults, without overlap. The structures included in each sectional image are sharply depicted, while structures located anteriorly or posteriorly to the section are blurred (Fig. 1) [13]. An antero-posterior (AP) chest radiograph is always automatically included in the tomosynthesis examination. Chest tomosynthesis is performed under breath hold in inspiration for a scan time of approximately 10 s. As small children unfortunately cannot cooperate adequately, tomosynthesis is currently used in children from about 8 years of age. Adults and teenagers are examined upright. Children between about 8 and 12 years are examined supine, which makes it easier for them to be still and concentrate on holding their breath, thus reducing motion artefacts.

A 13-year-old girl, examined with tomosynthesis to exclude lung metastases from sarcoma. The lungs are normal. a Normal antero-posterior (AP) radiograph. b Normal tomosynthesis section. The selected section shows anatomical structures in great detail while structures located anteriorly and posteriorly are increasingly blurred with increasing distance. The vascular branches can be seen as far peripherally as about 1 cm from the pleura
Compared to CT, tomosynthesis has a higher spatial resolution in the imaging (coronal) plane since the full resolution of the detector can be utilised (2,022 × 2,022 pixels), while a coronal CT MPR section has a matrix size of 512 × at most 512 pixels. However, the depth resolution is inferior to CT, since the tomosynthesis sections have non-precise thickness, with a sharper image at the centre and superimposed adjacent anatomical structures that become increasingly blurred with increasing distance from the section. Consequently objects such as intravenous lines, tubes or other devices generate artefacts in the adjacent sections, which may obscure the lung parenchyma. In addition, tomosynthesis does not have CT’s inherent ability of multiplanar imaging.
All images were selected, after informed consent, from a prospective study population on CF patients, which was approved by the local ethics committee. At the time of this pictorial essay, the population included 36 children from 8 to 18 years with a total of 92 tomosynthesis exams and 39 adults (19 to 59 years) with a total of 43 tomosynthesis exams. When the patients were examined with radiography as part of a clinical control, the examination was supplemented with tomosynthesis. In 125 cases the reason was a yearly check-up and 10 patients were examined due to an exacerbation of the disease. During the study period seven HRCTs and three contrast-enhanced CTs of the chest were performed in seven of the paediatric patients for clinical reasons. In the adult group one HRCT and one contrast-enhanced CT of the chest were performed in two patients. From the clinical files a number of cases of cystic fibrosis with typical findings were selected. In all cases corresponding radiographs are shown, and in a number of cases sections from chest CT close in time have been selected for comparison.
Pulmonary changes in cystic fibrosis
The lungs of newborn children with CF are almost normal, but they are prone to bacterial infection, which triggers an inflammatory response. The “vicious circle” of infection, impaired mucociliary clearance, inflammation, bronchial obstruction and tissue damage is well documented [14]. Inflammation and squamous metaplasia lead to thickening of the bronchial walls, which reduces the size of the small airways causing airway obstruction. The excessive mucus production and airway impaction together with the weakening of airway walls, secondary to infection and inflammation, lead to the development of bronchiectases [15].
Common radiologic pulmonary changes seen in CF are mucus plugging, bronchial wall thickening and peribronchial changes, bronchiectases, overinflation and air trapping, atelectases, and consolidation of lung parenchyma [16, 17]. In particular mucus plugging, bronchial wall thickening and bronchiectases are better delineated with tomosynthesis compared to radiography (see Fig. 2 above).
In mild disease, bronchial wall thickening, discrete cylindrical bronchiectases and small mucus plugs can be seen. With advancing disease the bronchiectases increase in number and gradually become more dilated, and large mucus plugs can be seen in the dilated bronchi. Pneumonia, small abscesses and atelectases can also develop.
Tomosynthesis findings
In the normal healthy lung, the bronchial walls are visible in the central lung with tomosynthesis but not in the periphery (Fig. 1). The vascular tree is depicted in more detail than with radiography, and vascular branches can be seen as far as approximately 1 cm from the pleura.
Small mucus plugs are usually not visible on radiographs but can be seen as a tree-in-bud pattern or as small clustered nodules in the periphery of the lobes with tomosynthesis (Figs. 2b and 3), with a similar appearance on coronal CT scans. Large mucus plugs can be seen as blurred nodular or cylindrical shadows on radiographs, but with tomosynthesis are sharply depicted inside the bronchi (Fig. 4). When the bronchi are thickened, they are clearly delineated with tomosynthesis, not only centrally, but also in the peripheral lung (Figs. 4 and 5). Bronchiectases may be clearly visualised with bronchography and CT, but are often difficult to assess with radiography. Radiographs depict suspicious bronchiectases as increased linear markings or blurred cystic lesions; with tomosynthesis it is possible to differentiate them in detail as cylindrical, varicose or cystic bronchiectases (Figs. 6, 7, 8 and 9). When the examination is performed upright air-fluid levels might be observed in the bronchiectases (Figs. 4c, 7b and 9b) or in abscesses, and small air-fluid levels seen on tomosynthesis are especially easy to miss on radiographs. In our patient group, no CF patient has yet presented with pneumothorax, but in other patients a small lateral or apical pneumothorax has been better visualised with tomosynthesis than with radiography. Localised air trapping and mosaic pattern, which often is well assessed with CT, cannot be adequately evaluated with tomosynthesis. These findings can be suspected with tomosynthesis when there is an absence of vascular markings or an area of hyperlucent lung. Bullae are more clearly delineated with tomosynthesis than with radiography, but can be seen in more detail with CT.

A 14-year-old girl with cystic fibrosis. a The right upper quadrant of the AP radiograph shows increased linear markings. b In the corresponding area, the tomosynthesis section clearly depicts bronchial wall thickening, small mucus plugs (arrowheads) and cylindrical bronchiectasis (arrows), not apparent on the simultaneously obtained radiograph

A 12-year-girl with cystic fibrosis. a The AP radiograph shows mild to moderate general changes of cystic fibrosis; with increased linear markings and discrete nodular opacities (arrowheads) in the periphery of both lungs. Bronchiectases are suspected in the upper parts of both hilar regions (white arrows). b A tomosynthesis section shows the CF changes in more detail. There is general bronchial wall thickening. Cylindrical bronchiectasis (white arrows) and small mucus plugs (arrowheads), in a tree-in-bud pattern on the right side, are also clearly depicted. Artefacts from a central venous access device can be seen in the right upper quadrant (black arrow)

A 35-year-old man with cystic fibrosis. a The AP radiograph shows moderate changes of cystic fibrosis. Large mucus plugs can be suspected in the perihilar regions bilaterally (arrowheads). b, c Two tomosynthesis sections show severely thickened bronchial walls, especially in the left upper quadrant (white arrows). Many of the bronchi are dilated and filled with large mucus plugs (arrowheads). A fluid level is seen in the left upper quadrant (black arrow)

A 17-year-old girl with cystic fibrosis. a In the right upper quadrant of the AP radiograph increased linear markings are seen, suggestive of bronchiectases. b On the tomosynthesis sections these changes are resolved in more detail as cylindrical bronchiectasis (arrows), bronchial wall thickening and minor areas of small mucus plugging (circles) are seen

A 21-year-old man with cystic fibrosis. a On the AP radiograph bronchiectases are suspected in the apical regions of both lungs. b On a tomosynthesis section multiple varicose bronchiectases are clearly seen (two on the right side and one on the left side are marked witharrows)

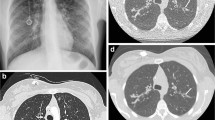
A 12-year-old girl with cystic fibrosis. a On the AP radiograph moderate cystic fibrosis changes are seen; the most severe are in the right lower quadrant. b, c Two tomosynthesis sections clearly show cystic bronchiectasis anteriorly in the right hilar region (circle) and varicose bronchiectasis in the perihilar regions bilaterally (white arrows). In addition a small fluid level is seen (black arrow) on the right side. Bronchial wall thickening, multiple cylindrical bronchiectases and small mucus plugs in the periphery are also seen in both lungs. d A section from HRCT of the lungs performed 1.5 months earlier shows bronchiectases anteriorly in the middle lobe and the lingula segment (arrows), and also in both lower lobes. In addition mucus plugging is seen in the right lower lobe (arrowheads)

A 32-year-old woman with cystic fibrosis. a An AP radiograph with suspected bronchiectases in the right lower lobe. b Tomosynthesis confirms the bronchiectases (arrows). Mucus plugs can be seen in some of the dilated bronchi (arrowheads). c A CT of the thorax with i.v. contrast was performed 5 months later, for other reasons. A coronal section shows large bronchiectases

A 13-year-old girl with cystic fibrosis. a An AP radiograph showing suspicious bronchiectases in the right upper quadrant. b The tomosynthesis section shows cystic bronchiectases (circle) with one small fluid level (black arrow). c A section from HRCT of the lungs performed 4 days earlier shows almost identical findings
As tomosynthesis depicts the lungs in the coronal plane with contiguous slices, it gives a better overview of the bronchial tree (Fig. 10a–c) compared to traditional axial high resolution CT (HRCT) images with 10 mm interspace (Fig. 10d). However, most centres now have multidetector CT scanners, and traditional HRCT examinations have been replaced by multiplanar reconstructions of thin contiguous slices. In our opinion sequential studies are easier to compare when the whole volume of the lungs is included in the tomosynthesis examination or in the volume CT of the lungs.

A 40-year-old man with cystic fibrosis. a In the right upper quadrant of the AP radiograph increased linear markings and blurred nodular lesions (arrowheads) are seen. b, c On the tomosynthesis sections, bronchial wall thickening, cylindrical bronchiectases (white arrows), large mucus plugs (black arrows), an area of mucus plugging in a tree-in-bud pattern (circles), and mucus plugs in a bronchus (arrowheads) are clearly depicted. d A section from HRCT of the lungs performed 2.5 months earlier also shows bronchial wall thickening, cylindrical bronchiectases and mucus plugging
Discussion
Since young patients with CF today may have a life expectancy of 40–50 years or more [18], dose considerations in radiologic examinations have become more important also for these patients. The effective adult dose from an AP and a lateral chest radiograph using a digital detector is approximately 0.04 to 0.05 mSv [13]. Chest CT may impart a 100-fold increase in effective dose, resulting in an adult effective dose of more than 4 mSv [19]. However, dose reduction algorithms and tube current modulations have now been introduced from several scanner manufacturers, which will reduce the dose for CT significantly [20–22]. With low dose chest CT protocols the effective dose may be reduced to 1.5 ± 0.5 mSv for 50 mAs, and 1.1 ± 0.3 mSv for 34 mAs [23], which is still almost 10 times higher than for tomosynthesis. Low dose CT protocols for CF have been designed [24], but have not been included in CF scoring systems so far. For children 8 to18 years old (median age 13) the effective dose at our department has been determined to be about 0.08 mSv from chest tomosynthesis and 0.04 mSv from chest radiography (AP and lateral view). The effective dose from chest tomosynthesis is 0.12 [6] to 0.13 [13] mSv for adults, which corresponds to the dose from a conventional film-intensifying screen system for radiography [25]. Thus chest tomosynthesis results approximately in a two- to three-fold increase in effective dose compared to chest radiography.
Tomosynthesis is performed on the same X-ray system as chest radiography adding only about 1 min to the normal examination time, which makes it a useful tool in the daily practice. The interpretation time for a tomosynthesis examination is normally shorter than for a CT scan with reconstructions in three planes, since there is only one series of images to evaluate.
In many countries the cost of an examination is an important issue, especially if patients are charged directly. In our department, the cost for a tomosynthesis examination, including the automatically generated AP radiograph and a supplemented lateral radiograph, is equivalent to 54€, which is about 10% more than for a chest radiograph (48€). The price for a chest CT (161€) is three times higher and an HRCT (214€) four times higher (all given prices include film reading and reporting).
Currently the scan time for tomosynthesis is 10 s, under breath hold in inspiration, which limits the use in small children without anaesthesia or sedation. Owing to its sectional imaging, tomosynthesis shows structures in more detail that cannot be sufficiently evaluated with radiography, such as a superior assessment of mucus plugging and bronchiectases, which according to some authors [16] are the most specific changes of CF lung disease. Since tomosynthesis exposes the patient to a comparatively low radiation dose it can be useful in the regular follow-up of CF patients as well as in everyday clinical practice, reducing the need to perform CT. When a more detailed assessment of the lungs may be required, CT still remains the method of choice.
Conclusion
A low dose diagnostic imaging strategy is important in the care of patients with CF, especially in the paediatric population. Tomosynthesis has a lower radiation dose than chest CT and gives a superior visualisation of pulmonary CF changes compared to radiography. In addition the cost for tomosynthesis is low compared to CT. It is performed on the same X-ray system as radiography, adding only about 1 min to the normal examination time, which makes it a useful tool in the daily practice. We believe that tomosynthesis can be of value in the monitoring of disease progression in CF, as a complement to radiography and CT. However, it is important to further define its role in the follow-up of CF patients and explore the strengths and weaknesses of the method.
References
De Jong P, Nakano Y, Lequin M et al (2004) Progressive damage on high resolution computed tomography despite stable lung function in cystic fibrosis. Eur Respir J 23:93–97
Robinson T (2007) Imaging of the chest in cystic fibrosis. Clin Chest Med 28:405–421
Saavedra M, Lynch D (2009) Emerging roles for CT imaging in cystic fibrosis. Radiology 252:327–329
Linnane B, Robinson P, Ranganathan S, Stick S, Murray C (2008) Role of high-resolution computed tomography in the detection of early cystic fibrosis lung disease. Paediatr Respir Rev 9:168–175
Dobbins J, Godfrey D (2003) Digital x-ray tomosynthesis: current state of the art and clinical potential. Phys Med Biol 48:R65–R106
Vikgren J, Zachrisson S, Svalkvist A et al (2008) Comparison of chest tomosynthesis and chest radiography for detection of pulmonary nodules: human observer study of clinical cases. Radiology 249:1034–1041
Kim E, Chung M, Lee H, Koh W, Jung H, Lee K (2010) Pulmonary mycobacterial disease: diagnostic performance of low-dose digital tomosynthesis as compared with chest radiography. Radiology 257:269–277
Zachrisson S, Vikgren J, Svalkvist A et al (2009) Effect of clinical experience of chest tomosynthesis on detection of pulmonary nodules. Acta Radiol 50:884–891
Wells I, Raju V, Rowberry B, Johns S, Freeman S, Wells I (2011) Digital tomosynthesis—a new lease of life for the intravenous urogram? Br J Radiol 84:464–468
Mermuys K, De Geeter F, Bacher K et al (2010) Digital tomosynthesis in the detection of urolithiasis: diagnostic performance and dosimetry compared with digital radiography with MDCT as the reference standard. AJR Am J Roentgenol 195:161–167
Mermuys K, Vanslambrouck K, Goubau J, Steyaert L, Casselman JW (2008) Use of digital tomosynthesis: case report of a suspected scaphoid fracture and technique. Skelet Radiol 37:569–572
Geijer M, Börjesson AM, Göthlin JH (2011) Clinical utility of tomosynthesis in suspected scaphoid fracture. A pilot study. Skelet Radiol 40:863–867
Båth M, Svalqvist A, von Wrangel A, Rismyhr-Olsson H, Cederblad Å (2010) Effective dose to patients from chest examinations with tomosynthesis. Radiat Prot Dosim 139:153–158
Cole P, Suppl. A (1997) The damaging role of bacteria in chronic lung infection. J Antimicrob Chemother 40:5–10
Barker A (2002) Bronchiectasis. N Engl J Med 346:1383–1393
de Jong P, Tiddens H (2007) Cystic fibrosis specific computed tomography scoring. Proc Am Thorac Soc 4:338–342
Koscik R, Kosorok M, Farrell P et al (2000) Wisconsin cystic fibrosis chest radiograph scoring system: validation and standardization for application to longitudinal studies. Pediatr Pulmonol 29:457–467
Swedish National Board of Health and Welfare (Socialstyrelsen) (2010) Ovanliga diagnoser, cystisk fibros. http://www.socialstyrelsen.se/ovanligadiagnoser/cystiskfibros. Accessed 15 June 2010
Donadieu J, Roudier C, Saguintaah M, Maccia C, Chiron R (2007) Estimation of the radiation dose from thoracic CT scans in a cystic fibrosis population. Chest 132:1233–1238
McCollough CH, Bruesewitz MR, Kofler JM (2006) CT dose reduction and dose management tools: overview of available options. Radiographics 26:503–512
Yu L, Bruesewitz MR, Thomas KB, Fletcher JG, Kofler JM, McCollough CH (2011) Optimal tube potential for radiation dose reduction in pediatric CT: principles, clinical implementations, and pitfalls. Radiographics 31:835–848
Allen BC, Baker ME, Einstein DM et al (2010) Effect of altering automatic exposure control settings and quality reference mAs on radiation dose, image quality, and diagnostic efficacy in MDCT enterography of active inflammatory Crohn’s disease. AJR Am J Roentgenol 195:89–100
Lucaya J, Piqueras J, Garcia-Pena P, Enriquez G, Garcia-Macias M, Sotil J (2000) Low-dose high-resolution CT of the chest in children and young adults: dose, cooperation, artifact incidence, and image quality. AJR Am J Roentgenol 175:985–992
Brody A, Tiddens H, Castile R et al (2005) Computed tomography in the evaluation of cystic fibrosis lung disease. Am J Resp Crit Care Med 172:1246–1252
Bacher K, Smeets P, Bonnarens K (2003) Dose reduction in patients undergoing chest imaging: digital amorphous silicon flat-panel detector radiography versus conventional film-screen radiography and phosphor-based computed radiography. AJR Am J Roentgenol 181:923–929
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Vult von Steyern, K., Björkman-Burtscher, I. & Geijer, M. Tomosynthesis in pulmonary cystic fibrosis with comparison to radiography and computed tomography: a pictorial review. Insights Imaging 3, 81–89 (2012). https://doi.org/10.1007/s13244-011-0137-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13244-011-0137-9