
Abstract
Objectives
The benefits of mindfulness meditation can only be achieved if it is practiced, but health behavior research tells us that initiating and maintaining long-term behavior change is difficult. We propose that mindfulness meditation can be usefully viewed as a health behavior and that this perspective generates insights into how individuals can be supported to develop a healthy habit of mindfulness practice.
Method
We synthesize health behavior models with research on mindfulness practice and with mindfulness curricula to develop the Sussex Mindfulness MEDitation (SuMMed) model. This new theoretical model of mindfulness meditation as a health behavior outlines the stages individuals progress through as they develop a sustained habit of meditation and the processes that facilitate transition between these stages. We contextualize these processes within existing curricula and outline how they could be further supported.
Results
Our model generates a roadmap for future research as well as practical suggestions tailored to individuals at different stages of behavior change. In particular, our model highlights the need to support individuals to continue practice beyond formal instruction, and suggests how maintenance of a meditation habit could be facilitated.
Conclusions
Mindfulness meditation can be viewed as a health behavior, and understanding mindfulness practice through this lens can help bridge the challenges associated with developing and sustaining mindfulness practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
There is a wealth of evidence from randomized controlled trials that mindfulness meditation practice is associated with a broad range of desirable health and well-being outcomes in clinical (Goldberg et al., 2018) and non-clinical (Galante et al., 2021) populations. Yet, evidence suggests people who are interested in practicing mindfulness often struggle to initiate meditation practice, sustain it over time, and establish it as an ongoing habit. Because of the strength of evidence for its effectiveness at improving a range of health outcomes, we propose that mindfulness meditation can be conceptualized as a “health behavior,” an “overt behavioral pattern, action or habit that relates to health maintenance, health restoration and to health improvement” (Gochman, 1997, p. 3). We draw upon well-established theories to present a health behavioral model of mindfulness practice (the Sussex Mindfulness MEDitation (SuMMed) model; Fig. 1), to help meet the need to support individuals to initiate and engage with mindfulness practice. We explain the insights our model offers into the process of behavior change and the practical recommendations it generates for supporting sustained mindfulness meditation practice.

The Sussex Mindfulness MEDitation (SuMMeD) model
Background and Rationale
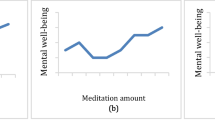
Mindfulness is defined as the awareness that arises through “paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally” (Kabat-Zinn, 1994, p. 4). This skill can be cultivated through mindfulness-based interventions (MBIs) such as the 8-week courses mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT). These interventions involve in- and between-session guided mindfulness meditation practices of up to 30–45 min where participants are invited to bring non-judgmental awareness to present-moment experiences followed by teacher-led discussion drawing out learning from practice. Developing this awareness requires practice (Kabat-Zinn, 2013). Exactly how much practice is still an open question. Evidence to support a direct dose-response relationship is mixed, there is scarce evidence available for the specific effects of long-term practice (Galante et al., 2023), and non-monotonic relationship has been hypothesized (Britton, 2019). While there is a clear need for further research on effects of continued mindfulness meditation practice (Galante et al., 2023), it is generally understood that more practice will lead to greater effects (Creswell, 2017; Parsons et al., 2017).
The curricula that support this practice, such as in MBSR and MBCT, are consistent in promoting regular and sustained engagement. While these curricula include teacher-led courses or sessions, they also increasingly include self-help resources such as books, internet programs, and smartphone applications (apps). Typically, these curricula will encourage and guide both formal practice (focused meditations) and informal practice (application of principles of mindfulness to daily activities), with these guided activities seen as “launching platforms” (Kabat-Zinn, 2013) for becoming more mindful. The frequency and length of recommended practice vary. Perhaps the most robust evidence base for mindfulness-based interventions comes from evaluation of MBCT and MBSR (Kabat-Zinn, 2013; Segal et al., 2013), but briefer practices of around 10–15 min are commonly included in self-guided and digital mindfulness curricula (Burch & Penman, 2013; Williams & Penman, 2011), and evidence is emerging that even brief practices can still promote greater mindfulness and better mental health outcomes (Howarth et al., 2019; Schumer et al., 2018).
However, recommendations do not always translate into actual behavior, and evidence suggests both engagement with curricula and amounts of practice are often less than recommended. Significant attrition and poor attendance may be observed in 8-week mindfulness courses (Lam et al., 2022; Tickell et al., 2020), and engagement with digital mindfulness courses may be even lower (Krusche et al., 2013; Sommers-Spijkerman et al., 2021). When individuals are asked about their engagement with practice outside the “classroom,” this also typically falls below recommended levels (Parsons et al., 2017; Taylor et al., 2021).
This problem is not unique to mindfulness meditation, but solving it may require a model specific to mindfulness meditation. While individuals often struggle to initiate and sustain new health behaviors, these behaviors differ in important ways. Behaviors such as physical exercise, smoking cessation, eating a healthy diet, or medication adherence all ultimately impact health, but vary in characteristics such as effort, frequency, immediacy of results, and whether results are easily visible (McEachan et al., 2010). Consequently, different interventions work to change different behaviors (Michie et al., 2013), and the processes driving successful behavior change also differ between behaviors (Rosen, 2000). Yet, health behavior theories provide limited guidance on which strategies should be used to modify which behaviors (Sheeran et al., 2017).
We argue that behavior-specific theory and guidance is especially necessary for mindfulness meditation because it presents a unique combination of characteristics compared to other health behaviors (i.e., high effort, long-term results, but results are not publicly visible and the behavior itself is often performed in private; McEachan et al., 2010). Thus, we aim to meet the need for a model describing processes and solutions tailored to the specific behavior of mindfulness meditation and its unique characteristics and challenges (Galante et al., 2023).
As a starting point for our model, we draw upon well-established psychosocial theories which aim to predict, explain, and change health behaviors. These can be divided into two types: social-cognition theories (e.g., the Health Belief Model and Theory of Planned Behavior), and stage theories (e.g., the Transtheoretical Model). These two types of theory should be viewed as complementary rather than competing, and our model recognizes that both approaches have unique insights to offer with respect to the challenges involved in initiating and developing a sustained practice of mindfulness meditation.
Social-cognition theories prioritize an understanding of the cognitive (e.g., attitudes, expectations, and beliefs) and affective constructs driving health behaviors, which are used to predict how likely individuals are to perform a behavior. The dominant social cognitive model of health-related behaviors is the Theory of Planned Behavior (TPB; Ajzen, 1991), which emphasizes intentions as the primary determinant of behavior; attitudes, perceived behavioral control, and social norms are seen as the primary determinants of intention. Other models foreground additional determinants including perceived benefits of and barriers to behavior change (Health Belief Model; Rosenstock, 2000) and perceived self-efficacy (Protection Motivation Theory; Rogers & Prentice-Dunn, 1997).
Stage theories, in contrast, prioritize the temporal and dynamic nature of engagement with health behavior, and see individuals in terms of how much progress they have made towards changing that behavior (Sutton, 2001). The dominant stage theory is the Transtheoretical Model (DiClemente & Prochaska, 1998), which divides behavior change into five key stages: pre-contemplation, contemplation, preparation, action, and maintenance. Other models such as the Health Action Process Approach (Schwarzer, 2016) and the Precaution Adoption Process Model (Weinstein, 1988) also view behavior change as progression through an ordered set of stages over time. These models share with social cognitive models the view that intentions are precursors to behavior, but also consider more explicitly how intentions progress to successful and sustained behavior change.
Our model incorporates aspects of both stage theories and social cognitive theories (as do some previous models, such as the Health Action Process Approach). In line with stage theories, we propose that individuals at different stages of engagement with mindfulness practice may experience qualitatively different problems and benefit from different solutions: In line with social cognitive theories, we propose that cognitive and affective processes can predict whether individuals transition between these stages. We have drawn upon research and practice in mindfulness to tailor these stages and transitional processes to the unique challenges involved in developing a mindfulness practice. The resulting model both describes the processes underlying the development of mindfulness practice and offers insights about how to support individuals in developing this practice.
Our model is broader in scope than previous applications of health behavior theories to mindfulness, which either have taken a solely social cognitive approach (Beattie et al., 2019), used the Reasoned Action Approach to predict engagement with an intervention, focused on understanding specific stages or transitions (i.e., the action stage; Masheder et al., 2020), the transition from the action to the maintenance stage (Langdon et al., 2011), or have focused on specific processes (i.e., how planning can best be used to facilitate initiation of short practices) (Mantzios & Giannou, 2018). The integration of both stages and processes in our model allows us to generate recommendations for tailoring interventions to individuals over time (e.g., planning should be particularly useful for individuals transitioning between preparation and action stages), highlight unexplored areas, and offer novel suggestions for applying insights from health psychology to mindfulness meditation practice.
The Sussex Mindfulness Meditation Model
Our model has a multi-stage structure in which individuals are classified into one of four stages according to their readiness to engage with mindfulness meditation and how much progress they have already made in initiating this behavior. As in other stage models such as the Transtheoretical Model and the Health Action Process Approach, our model broadly distinguishes between an intentional stage (first two stages) and a behavioral stage (final two stages), separated by the timepoint at which the individual takes action. Our model integrates also social cognitive approaches by mapping key predictors from previous models such as the Theory of Planned Behavior and Health Belief Model to the transitional processes between these stages. We next describe the four stages in our model and the transitions between these stages, highlighting the key theoretical insights that can be gained about mindfulness practice by viewing it through this lens.
From Pre-intention to Preparation
In the pre-intention stage, people do not intend to meditate in the foreseeable future. This includes individuals who are unaware of or uninterested in mindfulness meditation (the “pre-contemplation” stage in the Transtheoretical Model) as well as individuals who are interested and considering action but have not yet made any preparations (the “contemplation” stage in the Transtheoretical Model). Given the increasing popularity of mindfulness in mainstream medicine, education, psychology, and wider society (Crane, 2017; Williams & Kabat-Zinn, 2011), and the digitalization and increased accessibility of mindfulness-based therapy, a growing number of these individuals might become aware of its potential benefits.
Individuals transition to the preparation stage when they form an intention to embark on a mindfulness practice within the next month (Prochaska & DiClemente, 1986). This intention may simply be a spoken or unspoken decision to carry out a behavior (e.g., meditating every morning), or may be accompanied by an observable action (e.g., signing up for an 8-week course, buying a workbook, or downloading an app). Social cognitive theories are particularly relevant to this transition given their focus on the determinants of intentions, and there is reliable evidence to support the validity of key components of these models such as attitudes, perceived norms, self-efficacy, and perceived behavioral control in predicting intention formation across a variety of health behaviors (McEachan et al., 2010). However, their relative importance often varies according to the behavior. We focus on two components which are particularly relevant for understanding the initial stages of behavior change (Rothman et al., 2011) and which have been shown to predict engagement with mindfulness meditation. Outcome expectancies are the beliefs that individuals hold about whether a behavior will lead to positive outcomes; in the Theory of Reasoned Action, these beliefs determine whether an individual holds a positive attitude towards that behavior (and will thus form an intention to engage in that behavior). Self-efficacy is the belief that you can carry out a behavior successfully, and is broadly recognized in social cognitive models as an important determinant of intentions and behavior (along with the similar concept of perceived behavioral control).
Each of these beliefs has been shown to predict engagement with mindfulness meditation. Outcome expectancies have been found to predict the transition to intention formation in adolescents (Beattie et al., 2019), and have emerged as important predictors of engagement in formal training (Banerjee et al., 2017), and persistence of practice (Lam et al., 2022), suggesting the importance of beliefs about the benefits of mindfulness in understanding how and when individuals set intentions to meditate. Similarly, mindfulness self-efficacy, or individuals’ confidence in their ability to maintain mindful awareness during different situations, has been shown to increase from pre- to post-completion of 8-week programs (Chang et al., 2004) and is higher in individuals who regularly meditate (Cayoun et al., 2022), suggesting that low self-efficacy may be a problem in the initial stages of behavior change.
We recognize that other components of social cognitive theories are also likely to be important for understanding engagement with meditation. For example, perceived norms (i.e., the belief that people important to us approve of a behavior) have also been found to predict strength of practice intention and meditation practice time in undergraduates (Crandall et al., 2019). However, we propose that outcome expectancies and self-efficacy are likely to be particularly helpful for understanding and facilitating this specific stage transition.
From Preparation to Action
Evidence suggests no shortage of people in the preparation stage, who are intending to begin meditating in the near future. Demand for 8-week courses and the popularity of self-guided training resources as mindfulness meditation apps suggests a level of popularity which may be unprecedented for psychological interventions at large (Taylor et al., 2021). However, evidence also suggests many of these people will not act on those intentions. In a study of more than 100,000 people who had downloaded the Mindfulness Coach app, only just over half used the app at all after the first day it was installed (Kozlov et al., 2020). Transition to the action stage is marked by the initiation of mindfulness practice, which might be self-guided or guided by a mindfulness teacher. However, health behavior models recognize that intentions do not always lead to behavior, known as the “intention-behavior gap.” This gap has been demonstrated across a wide range of health behaviors, among a group of people who have strong intentions to exercise or quit smoking, for example, only half of them are likely to act (Sheeran, 2002). Thus, progression from the preparation stage to the action stage is not guaranteed.
In health behavior theories, intentions are not a binary variable that an individual either has or lacks, but a continuous variable that can vary in strength, similar to the concept of commitment. The strength of an individual’s intentions is considered the primary determinant of the transition to action (Ajzen, 1991). For this reason, factors such as outcome expectations and self-efficacy continue to be important predictors of the transition from preparation to action given their role in intention formation. Some individuals in the preparation stage may be more strongly committed to acting than others, it is likely that the stronger an individual’s intentions to practice mindfulness, the more likely they are to make the transition to action. However, as discussed in the previous paragraph, even people with strong intentions may fail to act for various reasons, including facing unanticipated barriers to practice, missing opportunities to practice, procrastinating, or simply forgetting to act (Sheeran & Webb, 2016). Planning in advance increases the chance individuals will act (Wiedemann et al., 2011), and planning is a key mediator between intention and behavior in previous health behavior frameworks (e.g., the Health Action Process Approach). Because planning is only effective for those who have already formed intentions, it is particularly well suited to helping individuals transition from preparation to action (Schüz et al., 2006) and is likely to work synergistically with interventions designed to boost commitment because planning is most successful when individuals have a strong commitment to their goal (Sheeran et al., 2005).
From Action to Maintenance
Individuals in the action stage have begun mindfulness practice and intend to keep doing so in the future. Some health behaviors only require a single action (e.g., vaccination), but mindfulness meditation is more comparable to health behaviors such as physical exercise, whose benefits require sustained action over time. Studies which track participants after completion of a training course (e.g., 8-week MBSR course) show variability in how successfully this action is sustained; for many individuals, longer-term mindfulness practice engagement is infrequent or non-existent (de Zoysa et al., 2014; Kabat-Zinn et al., 1985). The transition to the maintenance phase is defined not by a change in action but by the persistence of action. Individuals in the maintenance phase have sustained action for some time (e.g., 6 months or more; DiClemente & Prochaska, 1998) and intend to keep acting in the future. For mindfulness meditation, however, this transition may also involve some changes (e.g., after the conclusion of an 8-week training course, formal guided practice ceases and self-directed practice takes its place).
Unfortunately, long-term maintenance of any new health behavior is the exception, rather than the rule. New patterns of behavior often do not “stick,” leading to the “triangular relapse pattern,” whereby behavior changes initially but declines over time as old patterns of behavior re-emerge (Wood & Neal, 2016). The concept of habits is useful both for understanding when behaviors persist and how persistence can be facilitated. Habits are links between contexts and responses that develop through reward-based learning (Wood & Rünger, 2016). If behavior is performed repeatedly in the same context and is followed by a reward, eventually the context itself will trigger the behavior automatically, even if the reward is no longer present; our default response is to do what has worked for us in the past, which maximizes efficiency in the use of mental resources (Wood & Neal, 2016). Habits persist even when mental resources are scarce and are key to the successful maintenance of a behavior in the face of challenges (Neal et al., 2013).
Drawing on this work, we focus on reward and repetition as key features supporting the maintenance of behavior which are likely to be particularly challenging in the context of meditation. Mindfulness may not bring immediate rewards in the same way as other health behaviors (indeed, curricula may actively discourage participants from focusing on benefits), and the repetition of behavior in a stable context that underlies habit formation is often disrupted when training courses end and/or a transition is made from group-based to individual practice. Given the importance of reward and repetition in reinforcing initial behavior and supporting its maintenance (Sheeran et al., 2023), these factors are likely to be particularly relevant for understanding and supporting the transition between adopting mindfulness meditation in the short term and maintaining it in the longer term.
Sustaining Maintenance
For individuals in the maintenance stage, mindfulness meditation is an established habit. This is the goal of formal mindfulness curricula, which intend and encourage that participants continue to practice after instruction is over. Mindfulness programs encourage that this practice should be ongoing and daily, although for some people the maintenance stage may include attendance at group sessions or residential retreats to boost and sustain ongoing practice. Despite this view of mindfulness as a behavior like physical exercise where lifelong practice is the goal, there is very little evidence relating to how successful individuals are at maintaining mindfulness habits over time. A significant number of intervention studies do not incorporate a follow-up stage (Goldberg et al., 2017), thereby limiting our understanding of both the prevalence of longer-term practice and the benefits of longer-term practice. However, an observational survey in which 65% of participants reported having practiced mindfulness found that fewer than 1% had developed a habit for mindfulness practice (Mrazek et al., 2020). Health behavior theories view this maintenance stage, where a regular, self-directed behavioral habit has been established, as an ongoing process rather than a static end point. Even established behaviors can be disrupted, and individuals often relapse (defined as a regression to an earlier stage in the model; Prochaska et al., 1992). Thus, while maintenance is the final stage in our model, it is useful to consider the processes which promote continued maintenance and prevent relapse.
In health behavior research, it is acknowledged that the factors that promote maintenance are distinct from the factors that support initial behavior change, yet there is comparatively little evidence on how behaviors can be maintained as opposed to how they can be initiated (Sheeran et al., 2023). Even if an individual has formed a habit, this may not be maintained indefinitely over time, and making mindfulness practice a lifelong habit will involve continued negotiation of transitions that can derail even well-established practice. One such transition may occur if the stable link between context and behavior that forms the backbone of a habit is disrupted when the context changes (e.g., new job, moving house). The cues that were associated with the practice of meditation may no longer be present to trigger behavior. Such transitions are an especially good time to form new habits, or break undesired old habits, but can also be a challenging time for maintaining healthy habits (Wood et al., 2005). Another transition relates to how individuals value and perceive mindfulness itself. Once people have established a habit, their assessment of the costs and benefits of the behavior shifts as they now have access not only to information about the expected benefits of the behavior but also to the experienced benefits of the behavior (Rothman et al., 2011), which informs their consideration about whether the behavior is worth continuing. Maintenance of a health behavior is supported when people view the outcomes of a behavior as beneficial and consistent with their values (Sheeran et al., 2023). Thus, maintenance of a meditation habit may be threatened if mindfulness is no longer perceived as rewarding or consistent with the individual’s values.
Summary
The SuMMed model offers a framework for understanding how and when people progress towards developing and sustaining a healthy habit of mindfulness meditation. Above, we have outlined the model and presented some evidence supporting its potential value in predicting and promoting mindfulness meditation practice. In developing the model, we have drawn primarily on research into mindfulness meditation practices situated within the context of “first generation mindfulness-based interventions” (e.g., MBSR, MBCT; Van Gordon et al., 2022), where the cultivation of non-judgmental awareness is foregrounded and where evidence for effectiveness in improving health outcomes is arguably strongest, and therefore well suited to the application of a health behavior model. However, we believe our model may also be applicable to other related contemplative approaches that involve regular, sustained meditation practice as similar barriers to engagement may be evident.
We next turn to the practical applications of viewing meditation practice through this health behavior lens. In the following section, we use our model to contextualize how curricula already support individuals in transitioning through the four stages of practice and provide practical suggestions for how this support could be enhanced to support individuals in developing a mindfulness meditation habit.
Putting Theory into Practice
We begin our discussion of practical applications by noting that training programs already exist to help individuals progress through these stages. These curricula already acknowledge many of the challenges we have identified and offer some scaffolding to support individuals in initiating and sustaining practice. For example, they acknowledge that with the best of intentions, almost without exception, participants “come up against a range of stumbling blocks once they actually start to do it” (Segal et al., 2013, p. 129), and encourage participants to make plans, anticipate difficulties, and consider how these can be overcome (Segal et al., 2013). Our model offers a framework within which to understand the mechanisms and effectiveness of these existing practices through the contemporary principles of behavioral science and habit formation, and this health behavior framework can also systematically inform these curricula to improve their likelihood of developing a mindfulness meditation habit and its associated benefits.
In this section, we illustrate each of the key transitional processes in our model by first reviewing what existing practice already does to support that process, and then suggesting how that process could be supported more effectively. In making these suggestions, we draw upon a rich literature on behavior change techniques which has already identified many promising strategies to support the initiation and maintenance of health behaviors (Michie et al., 2011). The idea that different techniques may benefit individuals at different stages is a relatively untested one (Sheeran et al., 2023), although some evidence supports the idea that different strategies might facilitate different stage transitions (Schüz et al., 2006). We use the framework of our theoretical model and a grounded understanding of the challenges involved in mindfulness practice to recommend techniques likely to be effective for each transition.
Supporting the Transition to Intention Formation
Outcome Expectancies
Examples of Current Practice
Many people are likely to become aware of mindfulness practice through articles, adverts, campaigns, and pre-curricula, and these also frequently include articulation of potential benefits of mindfulness practice for outcomes such as well-being and mental health (“MBCT…is as effective as drugs for preventing depression”; Williams & Penman, 2011, back cover), physical health (“Your body becomes better at fighting diseases”; Alidina & Marshall, 2013), interpersonal relationships (“…improves couple communication, connection and cooperation”; Bardacke, 2012, cover page), or stress (“feel 14% less stressed in just 10 days”; www.headspace.com, 17.01.2023). These claims may be supported by reference to specific research evidence or clinical guidelines (“MBCT is recommended by the UK’s National Institute for Health and Clinical Excellence”; Williams & Penman, 2011, back cover), or by endorsements from peer practitioners, experts, or celebrities. Mindfulness courses also typically promise that the ultimate outcome of practice will be a reduction in mental health symptoms and an improvement in well-being (Segal et al., 2013). Traditional 8-week courses typically offer an orientation or taster session for those curious to find out more about mindfulness practice, which will usually highlight potential benefits (“increased awareness and concentration…learning to take better care of self…”; Santorelli et al., 2017; p. 11). However, this is tempered with discussion of the possible emotional and physical risks of practice, the limitations of practice (not a “quick fix”), and the need to have both the will and the way to make time and space for practice (“the level of commitment…and to the personal discipline it requires”; Santorelli et al., 2017, p. 15).
Enhancing Current Practice
Research indicates that intervention credibility and outcome expectancy can influence engagement with health behaviors including mindfulness practice (Strauss et al., 2021). Therefore, education about mindfulness practice that specifically targets credibility and outcome expectancy may support engagement. We recognize that mindfulness is thought to be less beneficial if participants pursue it simply because of the personal benefits they may experience (Segal et al., 2002), and that the promotion of positive outcome expectancies may seem at odds with the fact that mindfulness courses typically promote this non-striving attitude towards outcomes. Nevertheless, because individuals will only pursue behaviors which they expect to be worthwhile and beneficial, we argue that communicating about the positive outcomes of meditation is important to facilitate the initial stages of behavior change. Health psychology research adds the important context that realistic expectations are likely to be more effective in promoting behavior change than overly optimistic expectations (Jones et al., 2010).
How could practitioners promote positive, but realistic, outcome expectancies? We recommend addressing misconceptions people may hold about meditation that have been shown to impact engagement. In the context of meditation practice, misconceptions about mindfulness as “doing nothing,” or as exclusively a treatment for poor mental health, can inhibit practice (Remskar et al., 2022), or conversely that daily practice is unnecessary if they are already feeling positive, which can decrease engagement (Moore et al., 2020). The idea that mindfulness practice will be inherently calming or relaxing is also prevalent. Instructors could potentially optimize outcome expectancies by addressing such misconceptions about mindfulness, including guidance that the day-to-day experience of mindfulness practice may not be experienced as especially pleasant, but this is a normal part of the learning process.
Self-efficacy
Examples of Current Practice
Self-efficacy is likely to be facilitated by the broad array of options available to those considering mindfulness meditation. These include traditional in-person group-based 8-week curricula, online guidance for practices as short as 1 min (Kane, 2022), longer taster sessions in person (Santorelli et al., 2017), and online courses (Upcoming Courses – Courses – Oxford Mindfulness Centre; How to Meditate – Mindful). Resources frequently promote flexibility in where (“you can practice anywhere”; Mindfulness—NHS (www.nhs.uk), 18.01.2023), when (“any time”; www.headspace.com, 18.01.2023), how (Young, n.d.), and for how long individuals can practice (“as little as 15 min per day”; Wei, n.d.). This increase in the flexibility and accessibility of practice is likely to promote self-efficacy both by enhancing sense of ease and control and by addressing misconceptions that might otherwise have hindered self-efficacy (e.g., that mindfulness practice can only be accomplished in certain spaces, in complete silence, or with a lengthy time commitment). However, it is also notable that such an extensive menu of options to support practice may be overwhelming (Iyengar & Lepper, 2000). Promotional material for mindfulness training may also highlight the large numbers of students already engaged with their curricula: “join over 40 million users” or “over 1.5 million copies sold” (How Does Headspace Work?, 18.01.2023; Williams & Penman, 2011, cover). Presenting mindfulness as popular and accessible may boost intentions through changing perceptions of social norms (another key predictor in social cognitive theories), but is also likely to boost self-efficacy through enhancing the sense of practice as being personally achievable. Thus, while mindfulness resources often acknowledge that practice is “simple” but not necessarily “easy” (Kabat-Zinn, 2012), the promotion of meditation as accessible, popular, and flexible facilitates self-efficacy.
Enhancing Current Practice
The primary technique suggested to boost self-efficacy is gaining experience in successfully performing a behavior (Bandura, 1998). This is consistent with research showing that mindfulness self-efficacy increases with meditation experience (Chang et al., 2004). However, if low self-efficacy is a barrier to engaging with a behavior and gaining this experience, other strategies may be necessary to help people in the pre-intention stage feel more capable in setting intentions to meditate. Other ways of boosting self-efficacy include social persuasion (being persuaded that you are capable), and vicarious experiences (seeing people similar to yourself succeed; Bandura, 1998). These strategies could be modeled by instructors, but research shows they can also effectively be implemented by individuals, for example, by asking individuals to reflect upon past experiences of other goals they have already achieved (Koestner et al., 2006).
Self-efficacy is also lower in individuals who perceive more barriers to engaging with a health behavior (Olutende et al., 2017). In the context of meditation, not having time or space to meditate was reported as a barrier by novice meditators (Hunt et al., 2020), and length of practice may also be a barrier that hinders engagement (Banerjee et al., 2017); length of practice may be a particularly acute barrier for people experiencing severe and chronic mental health difficulties who may experience longer practices as overwhelming (Chadwick et al., 2016). Other reported barriers include not enjoying practice (Moore et al., 2020), perceiving mind wandering as a failure to be mindful (Remskar et al., 2022), or the fear of what might come into awareness during mindfulness (Gilbert et al., 2023). Instructors might boost self-efficacy by giving novice meditators strategies to overcome these barriers, such as recommending shorter meditations, validating and normalizing negative experiences, and reframing obstacles as learning experiences (e.g., reframing noticing mind wandering as part of the learning process, and therefore as success rather than failure).
Supporting the Transition to Action
Planning
Examples of Current Practice
Two key processes in planning are goal setting and action planning. Mindfulness curricula typically scaffold both processes by providing a clear schedule and program of formal practice, at least for an initial training period, and by specifying clear goals such as “plan on finding an hour a day to practice mindfulness” (Teasdale et al., 2014, p. 33), although the potential benefits of briefer practices are also acknowledged (e.g., Bardacke, 2012; Burch & Penman, 2013; Williams & Penman, 2011).
Curricula often offer additional support for planning through specific guidance about where and when to do formal practice (e.g., early morning (Bardacke, 2012); at the beginning and end of the day (Burch & Penman, 2013); on waking). Participants are also encouraged to plan ahead to pre-empt obstacles, for example, by letting others in their home know that they would like to remain undisturbed during practice, by setting up reminders to engage in practice as planned (e.g., by smartphone notification), and by considering what equipment they will need for practice (Burch & Penman, 2013, p. 43). Encouragement to monitor progress also facilitates effective planning (e.g., by keeping a record of daily practice), and planning activities are typically revisited in the transition out of the formal training period. Thus, planning for practice is integral to foundational mindfulness training, although sometimes with mixed messages about how best to plan.
Enhancing Current Practice
One way to optimize planning activities is to increase the specificity of the plans. An if-then format specifying both a specific behavior and the cue for behavior (e.g., “If I’ve just brushed my teeth, then I will sit on the cushion and meditate for 45 min”), known as implementation intentions (Gollwitzer, 1999), is a particularly effective planning technique. Encouraging individuals to make plans in this format could increase the likelihood of successfully acting on intentions to practice, as previously suggested by Mantzios and Giannou (2018), and initial evidence has shown that forming if-then plans can increase frequency of meditation following participation in a mindfulness program (Galla et al., 2016), although only among people with a strong commitment to meditation. One strategy to ensure low commitment does not undermine the effectiveness of planning is to combine planning interventions with a commitment boost. Mental contrasting with implementation intentions is a planning technique in which individuals envision their desired positive outcome, as well as the obstacles which may prevent this outcome, in advance of forming an if-then plan (Oettingen et al., 2013). This technique is particularly effective in facilitating health behavior (Cross & Sheffield, 2019), and we suggest it has potential to boost engagement with mindfulness practice.
Monitoring progress is also an important part of effectively executing plans and initiating new behaviors. Monitoring both keeps attention focused on the goal and allows individuals to notice deviations from their plan (Sheeran & Webb, 2016). Including monitoring as part of an intervention increases the likelihood of behavior change (Harkin et al., 2016). Thus, existing practices of self-monitoring in mindfulness curricula (e.g., diary keeping, progress run features in apps) are supported by evidence and could be particularly emphasized for individuals at early stages of action.
Commitment
Examples of Current Practice
Participants are invited to cultivate the “spirit of engaged commitment” for (at least) an initial 8-week training period (Segal et al., 2013)—to make time to practice, daily, whether or not they feel like it, or the conditions seem right. Recognizing that making this commitment is “no small matter” (Bardacke, 2012), pre-class interviews or orientation sessions advise that the commitment to spend time on home practice is an essential part of the class, and if participants feel unable “to make that commitment, it would be best not to start the classes” (Segal et al., 2013, p. 102). Similarly in MBSR, one of the main intentions of the orientation session is “eliciting a commitment from participants to engage in active participation with the program, which includes weekly class attendance and a minimum of 45 minutes to one hour of formal home practice [daily] as well as informal practice throughout the day” (Santorelli et al., 2017, p. 6). Participants are also encouraged to let friends and family know of their intention to complete the program (Teasdale et al., 2014, p. 32).
As in traditional curricula, digital mindfulness resources also include content designed to support commitment. For example, Headspace offers guided programs that begin with an invitation to “make a commitment to yourself” setting personalized “mindful reminders to stay consistent and committed to your goals,” as well as brief video guidance that further emphasizes the importance of commitment and persistence with practice, to “showing up every day” and that “with that commitment, dedication…you then start to see results” (Headspace, 2023). Thus, the importance of commitment is noted in mindfulness curricula, which already do much to support this transitional process.
Enhancing Current Practice
As discussed in the section on enhancing current practice for planning, increased commitment can be the outcome of effective planning; forming an implementation intention could be thought of as making a commitment to oneself to carry out a behavior (Gollwitzer, 1999). Simply asking people to make an explicit commitment to perform a behavior, such as signing a statement affirming that commitment, can in itself boost commitment and increase the likelihood of action (Ajzen et al., 2009). An alternative strategy originating from behavioral economics is the concept of commitment devices. These involve taking steps in advance to motivate the future self by changing the costs and benefits of future behavior. The commitment an individual makes in advance can be a practical commitment (e.g., charging electronic devices downstairs so that they are less likely to tempt you away from engaging in a morning meditation), financial commitment (e.g., paying in advance for a meditation course), or social commitment (e.g., arranging to meet someone else at the session, sharing your meditation goals with another person). There is emerging evidence that commitment devices can be useful strategies to help individuals successfully carry out health behaviors (Coupe et al., 2019), and therefore could be examined further within the context of mindfulness training curricula.
Supporting the Transition to Maintenance
Reward
Examples of Current Practice
Experiencing reward from a behavior is key to habit formation. In the context of developing a mindfulness meditation habit, the experience of reward could come from meditation itself, or from its benefits such as improved well-being; however, it could also come from other features of training such as the experience of setting and meeting practice goals, positive feedback from the mindfulness teacher, classmates or colleagues during reviews of weekly meditation practice, or gamification features of online programs (e.g., an app awarding “badges” on reaching practice landmarks). As noted under “Outcome Expectancies,” mindfulness curricula may also acknowledge reward in the sense of drawing attention to the fact that the rewards of mindfulness practice may not be instantly apparent (e.g., Segal et al., 2013). Because reward is a key part of the learning processes that underlie the formation of habits, we can see these practices as functioning to support habit formation. Social connections and experiences can also be rewarding experiences. Mindfulness courses are often delivered in a group context and curricula acknowledge the support that can be gained from practicing together with others—a partner (Bardacke, 2012), a buddy (Headspace), or a group (e.g., Teasdale et al., 2014). Online programs may invite the learner to link up with friends in an online social network, or connect with information reported about how many people worldwide are using the app at the same time (Headspace). These practices could also be seen through the lens of making meditation practice rewarding.
Enhancing Current Practice
Instructors could work with students to reframe the experience of mindfulness meditation itself as more rewarding. This could be achieved by emphasizing noticing feelings of joy and tranquility as inherent rewards (Brewer et al., 2013), or reframing aspects of practice that might be experienced negatively (e.g., the act of noticing that the mind has wandered) as positive experiences indicating success rather than a failure. However, mindfulness meditation may not inherently be rewarding for all learners, and this lack of reward may undermine the process of habit formation. Consistent with this, individuals who experienced meditation as boring or effortful were more likely to drop out before the end of an online course (Osin & Turilina, 2021).
If meditation itself is not rewarding, can external rewards be used to facilitate developing a meditation habit? External rewards risk undermining intrinsic motivation to engage in a behavior (Deci & Ryan, 2002), and if they are contingent on performance of the behavior, they can become the goal of practice, meaning people are unlikely to form a habit that will continue when the reward disappears (Lally & Gardner, 2013). However, the short-term behavior change prompted by external incentives can boost attitudes and self-efficacy towards the behavior (Gardiner & Bryan, 2017). Thus, scaffolding meditation using external rewards in the early stages of behavior change could facilitate the transition from action to maintenance. One implementation of this is “temptation bundling,” in which a desired activity that may not be inherently rewarding is performed alongside a rewarding activity (e.g., listening to an audiobook only while exercising at the gym; Milkman et al., 2013). Mindfully eating a desirable food, or mindfully practicing another enjoyable activity, could be examples of this strategy as applied to practice.
Over time, the continued practice of mindfulness may in itself change how the brain processes reward (Tang et al., 2015) and increase the experience of momentary positive emotions and enhanced responsiveness to pleasant daily life activities (Geschwind et al., 2011). Emphasizing the rewards of mindfulness practice as an initial strategy to support learners to form a meditation habit may thus cease to be necessary as meditation becomes an inherently more fulfilling and rewarding experience.
Repetition
Examples of Current Practice
Mindfulness curricula emphasize that “mindfulness gains its power through repetition” (Burch & Penman, 2013, p. 37), stressing that “this approach depends entirely on your willingness to do home practice between class meetings. This practice will take at least an hour a day, 6 days a week, for 8 weeks” (Segal et al., 2013, p. 102). The importance of regularity of practice is stressed (Burch & Penman, 2013)—its “everydayness” (Kabat-Zinn, 2013; Segal et al., 2013), and it is suggested that this “continuity builds and sustains motivation and momentum” (Segal et al., 2013, p. 375). As well as regularity of formal meditation practice, participants are encouraged to be mindful of routine activities (waking up, washing, getting dressed, etc.), and to touch base with mindfulness throughout the day (e.g., Kabat-Zinn, 2013; Segal et al., 2013). It is even suggested that repetition should be prioritized over reward. Kabat-Zinn (1990) states “you don’t have to like it, you just have to do it. When the eight weeks are over, then you can tell us whether it was any use or not. For now just keep practicing” (p. 41). This emphasis on repetition even if the behavior is not yet rewarding is likely to aid with establishing habits. Similarly, after an 8-week class, the practice of encouraging learners to choose a specific form of practice to focus on for the next few weeks (Segal et al., 2013) could be seen as encouraging the stable context needed for habit formation, as trying to do lots of different practices may be derailing at this stage of habit development.
Enhancing Current Practice
Because habits are learned associations between contexts and behaviors, they will be learned more quickly if the context of a behavior is similar across repetitions. Stable contextual features for meditation could be practicing at the same time, in the same place, with the same people, or after another action or event (Wood & Neal, 2016)—or even after experiencing a particular emotion, as suggested by formal practice of the brief 3-stage meditation in response to stress (Kabat-Zinn, 1994). Practitioners could help people to identify suitable cues or contexts for practice, and encourage prioritizing stability over variety when helping people to identify specific formal or informal practices. Another especially effective strategy could be to link mindfulness practice with another behavior that is already habitual, known as piggybacking (Wood & Neal, 2016), such as after brushing teeth or after changing out of work clothing, and there is some evidence that meditating after an existing routine may support sustained engagement with a mindfulness app (Sullivan et al., 2023).
It is also crucial that behaviors are repeated for long enough that habits can form. The length of time it takes to form a habit varies considerably between individuals. A study with new gym members found that 4 times per week for 6 weeks was the minimum time taken to form a new habit (Kaushal & Rhodes, 2015), but Lally et al. (2010) found that this varied between a few weeks and many months. Thus, while some mindfulness curricula suggest an 8-week course should be “sufficient time to bring your meditation practice to a point where it being to feel natural and like a way of life” (Kabat Zinn (1990), p. 424), this might not be long enough for some people to develop an established habit, and longer mindfulness training programs may be more effective in facilitating habit formation. Practitioners could share with students that forming a new habit is likely to take at least 10 weeks and will get progressively easier over time (Gardner et al., 2012). However, an important insight from the health behavior literature is that behaviors do not have to be performed with perfect consistency during this time in order to form a habit. A study which tracked 96 individuals as they tried to form new eating, drinking, or exercise habits found that while consistency of repetition was crucial, occasional lapses did not affect habit formation (Lally et al., 2010). Setting minimal goals to encourage repetition of practice (e.g., practice every day even if it is only for 5 min; Williams & Penman, 2011) could thus be an effective strategy to help form a meditation habit (as suggested by Mantzios & Giannou, 2018).
Consistency of repetition could also be supported by identifying and planning for difficulties that may cause lapses in behavior. These difficulties may be external, such as other activities competing for time, but might also be internal, such as feeling overwhelmed or disappointed by practice (Wyatt et al., 2013); novice meditators may feel like they are “doing it wrong” (Remskar et al., 2022), and people high in rumination or worry may also experience negative feelings as barriers (Banerjee et al., 2017). Langdon et al. (2011) found that these thoughts and feelings can act as obstacles to practice, so addressing these obstacles via reframing or planning could potentially support consistency of repetition. When lapses do occur, to prevent a vicious cycle where lapses can demotivate individuals and encourage further lapses (Herman & Polivy, 1984), a self-compassionate response recognizing that one lapse does not undo all one’s progress can be helpful (Homan & Sirois, 2017), as can using implementation intentions to plan for continuing action after a lapse despite negative emotions (e.g., Sheeran et al., 2007).
Supporting Continued Maintenance
Managing Transitions
Examples of Current Practice
The transition from an initial training schedule into self-guided practice is recognized as a new beginning with new challenges. These transitions may be experienced differently at the end of real-world mindfulness training group than in a digital environment, where the cues and context for ongoing digitally supported practice may change less dramatically. Mindfulness curricula offer various forms of scaffolding for this transition. In preparation, participants are encouraged to reread helpful material (Bardacke, 2012), and revisit planning activities for regular practice beyond the course. Reminders of the benefits of stable cues and context are given—“if at all possible, do the practice at the same time, in the same place, each day” (Teasdale et al., 2014, p. 205). Making a plan and sticking to it is encouraged, although “the important thing is that it should be realistic” (Segal et al., 2013, p. 375). Mindfulness curricula also encourage teachers to give participants a small object as a reminder of the class, their hard work, and the people who have share their journey (Segal et al., 2013, p. 380).
After the end of formal training, many mindfulness training centers offer further support for long-term practice such as reunions, follow-up classes, and day retreats (Segal et al., 2013). Such support may help to bridge the transition from the “launching platform” of guided activity towards a sustained, self-guided practice habit, and further research is needed to optimize engagement with and benefit from such resources. Beyond transitions in mindfulness training, changes in mood, thinking patterns and behavior, and life circumstances and events may disrupt even well-established practice, and mindfulness curricula encourage participants to reconnect with practice when possible. Participants are reminded that they can “always begin again” (Teasdale et al., 2014, p. 205) and that mindfulness is “only ever a breath away” (Williams & Penman, 2011, p. 66). The use of if–then plans to support practice is encouraged if a person notices early warning signs for the recurrence of depression (Segal et al., 2013, p. 354).
Enhancing Current Practice
As discussed in the section “Sustaining Maintenance,” physical or temporal transitions can disrupt the links between context and behavior that underlie habits. These might include the transition from formal training to informal practice, but also life transitions, such as changes in jobs, relationships, or location. Transitions can be disruptive and demotivating for people who have established habits (Wood et al., 2005). One way to minimize their negative effects could be to strive to maintain key contextual features of the behavior (e.g., where it is performed, whether it is performed with others), as some research has found that the more the performance context of a habit remained stable during a transition, the more that habit is protected (Wood et al., 2005). Identifying a constant physical practice context (e.g., sitting on a particular cushion) or transitional object (e.g., a pebble or shell) could be one useful cue to provide this stability.
Transitions can also be beneficial, however, because they will disrupt cues to old unhelpful patterns of behavior, and thus can be good times to renew or re-establish habits. Transitions such as the beginning of a new year or the passing of milestones such as birthdays can provide people with the sense that they are starting afresh and renew their motivation to pursue good habits (Dai et al., 2014), known as the “fresh start effect.” Thus, as well as managing the potentially disruptive effects of change, practitioners could help students to actively seek transitional opportunities for “fresh starts” when they are needed. Practitioners could help students identify a good opportunity or milestone to view as a transition (e.g., the beginning of a new month, a life event), or to actively make a change in their environment to create a transition (e.g., the place they meditate).
Finally, some people cope better with transitions than others, and practitioners could learn from those who cope well about how to better support those who struggle. People who are more confident in their ability to maintain a behavior, resume it after a break, and cope with barriers to performing the behavior are more likely to continue performing that behavior even if it is disrupted (e.g., Kwasnicka et al., 2016). Consistent with this, self-efficacy predicts who will relapse from the action stage (Schüz et al., 2008). While the best way to improve self-efficacy for mindfulness meditation remains to be tested, receiving positive feedback on performance has been demonstrated to improve self-efficacy for other behaviors (Ashford et al., 2010), so could be a strategy for supporting continued practice during transitions.
Reaffirming Values
Examples of Current Practice
Curricula emphasize the importance of values in motivating and sustaining practice. Mindfulness practice is maintained through the cultivation of personal vision “to help carry you through the inevitable periods of low motivation and give continuity to your practice” (Kabat-Zinn, 1990, p. 46). Participants are encouraged to “identify a heartfelt intention to sustain mindfulness practice” (Teasdale et al., 2014, p. 201), “to examine your deepest reasons and desires for maintaining your practice” (Burch & Penman, 2013, p. 226), that could include, for example, a desire for personal growth, improved relationships, or spiritual connection, and to identify and reaffirm values that are linked to everyday practice (Segal et al, 2013). Methods for making these connections include contemplative enquiry: “what is most important to me in my life (what do I most value) that this practice might help with?” (Segal et al., 2013, p. 376). Whatever emerges from this enquiry is noted on a card which is kept by the participant. As noted in our suggestions for managing transitions, teachers may also give participants a small object (e.g., shell or pebble) which could function as a reminder of these values (Segal et al., 2013, p. 380).
Enhancing Current Practice
Research on behavioral maintenance has found that individuals are more likely to maintain a healthy habit if they continue to see the behavior both as valuable and as consistent with their values (Rothman et al., 2011). A behavior may be valuable because it has brought positive change to our lives, and people who are more satisfied with the outcomes of a health behavior are more likely to maintain that behavior (Baldwin et al., 2006). These existing practices which encourage participants to reflect on the value they perceive in mindfulness and what it has brought to their lives could be particularly helpful even at the stage where this behavior is already established. Seeing mindfulness as an activity that is consistent with one’s personal values is also likely to support maintenance through its links with intrinsic motivation. Broadly speaking, when we pursue goals because they are consistent with our values and we are intrinsically motivated to do so, we are more successful, partly because acting on those goals feels easier (Werner et al., 2016).
Intrinsic motivation is thought to be a key determinant of behavioral maintenance (Kwasnicka et al., 2016) and is thus also a promising target for supporting maintenance of a mindfulness habit. An important determinant of intrinsic motivation is a sense of autonomy over one’s actions, so it is likely that individuals will be more motivated to maintain a healthy habit and more successful in doing so if they are encouraged to experience a sense of ownership over their practice and freedom of choice in how they practice. This sense of autonomy could be achieved through defining their own goals, connecting with their own motivations for meditating, and limiting external rewards or praise (in contrast to our recommendation that external rewards can be useful in the initial stages of behavior change). Reinforcing the link between mindfulness meditation and an individual’s values could also harness these motivational processes.
Models of self-regulation suggest that goals which are viewed as part of the self, i.e., that reflect who we truly are, will be valued more highly and thus pursued more successfully (Berkman, 2017). Individuals could be encouraged to frame mindfulness meditation as part of the self through using language that presents this practice as an enactment of participants’ identity, rather than as something they do: “being a meditator,” rather than “meditating.” In experimental studies, these linguistic cues have been shown to influence behavior (Bryan et al., 2011), because action becomes a valuable way to affirm our identity. Linking habits to an individual’s identity might help to maintain habits in the long term (Verplanken & Sui, 2019), but also, having multiple valued identities itself has benefits for well-being (Jetten et al., 2011). Thus, encouraging participants to identify as “meditators” or “mindfulness practitioners” could harness multiple beneficial psychological processes.
Discussion
We suggest mindfulness practice could be viewed as a health behavior, and that recognizing mindfulness practice through this lens could help us to understand and bridge the challenges associated with developing and sustaining mindfulness practice. We have considered in detail the journey of mindfulness practice over time and how different health behavioral principles and techniques from research on behavior change and habit formation may be useful in supporting engagement at different points in this process.
Our model has the potential to help optimize the potential real-world benefits of mindfulness practice for large numbers of people. The effectiveness of mindfulness-based interventions in improving a range of health outcomes has been established, but how to effectively scale up access to these interventions has not (Goldberg, 2022). Digital health interventions offer the potential for broad access to mindfulness, but engagement with these interventions is often extremely low (Lipschitz et al., 2023), with no clear evidence on which strategies work best to solve this problem (Winter et al., 2022). Our framework, and the practical suggestions that follow from it, could help to meet this need for effective strategies to support behavior change, and is also applicable across a broad range of individuals and situations, from novice meditators to experienced meditators, from self-guided interventions to formal programs.
An implication of our analysis is that the real-world benefits of mindfulness could also be optimized by focusing on people who are already engaging with mindfulness, and that this could be just as beneficial for population health and well-being as encouraging new people to take up mindfulness. Our review of the literature on stages of change as they apply to mindfulness practice demonstrates that a significant number of people progress to the preparation stage but fail either to act (e.g., Kozlov et al., 2020) or to maintain this action in the long term (e.g., de Zoysa et al., 2014). Thus, helping people who are already engaged with mindfulness to enact their intentions and develop desired habits could have a large impact on translating the potential benefits of mindfulness practice into real effects, and this applies both to novice and to experienced meditators, who may face different challenges but who both stand to benefit from interventions designed to help them to achieve their desired level of mindfulness practice. As an analogy to a biomedical context, researchers have suggested that improving adherence to existing treatments could have far larger effects on outcomes than developing new effective treatments (Nieuwlaat et al., 2014).
Our model generates a programmatic research agenda that will help to test and refine our approach. We suggest that such future research could usefully be informed by the experimental medicine approach to developing health behavior interventions (Sheeran et al., 2017), which advocates for first testing key theoretical assumptions (e.g., whether the processes we have proposed are valid, which interventions can most effectively target those processes) before testing whether targeting those processes successfully influences the desired behavior. The experimental medicine approach provides a framework for designing informative studies that can measure mechanistic processes and advance theoretical understanding at the same time as they change behavior, and we suggest using this approach to target the components identified in our model would be the most effective way to put our theory into practice.
Caveats and Considerations
Our analysis of mindfulness meditation behavior change focuses on quantity of practice, but quality of practice may also be important. It could be that “how” rather than “how often” one practices has the greatest impact on mindfulness training outcomes (Goldberg et al., 2014), and the primacy of duration and frequency of practice in training curricula may overshadow the potential importance of practice quality (Del Re et al., 2013). An individual’s reflection on learning from practice, and a focus on developing the attitudinal foundations of mindfulness practice, may be more important than simply “sitting on the cushion.” Further research is needed to develop knowledge of the relative importance of practice quantity and quality and how they may interact.
Similarly, our analysis has focused primarily on formal mindfulness practice—making a specific time to stop other activities and focus for some time on moment-to-moment awareness. This is not the only way to practice mindfulness. “Informal practice”—paying mindful attention to whatever you are doing in any aspect of daily life—may be at least as valuable (Kabat-Zinn, 1990). Formal and informal practices may complement each other, are both strongly recommended in mindfulness training curricula, and may contribute interactively to benefits of mindfulness (Goldberg, 2022). Informal practice could also be understood as a health behavior, and the principles outlined in this paper may be equally applied to this kind of practice. Similarly, we expect our core insights about how to support regular and sustained mindfulness meditation practice maybe applicable to other types of meditation practice.
Mindfulness itself can also be distinguished from the practices used to develop it, which are recognized as “merely launching platforms” (Kabat-Zinn et al., 2003, p. 276) for becoming more mindful. Langdon et al. (2011) have suggested that in this sense, mindfulness is “less a health behavior and more an approach to life” (p. 271). Thus, a model focused on understanding the behaviors performed to cultivate mindfulness may not fully capture the development of mindfulness as a flexible and evolving approach of daily living. We suggest that formal practice in responding mindfully to thoughts, feelings, and sensations is likely to transfer to how individuals respond to thoughts, feelings, and sensations in daily life, just as a regular practice of running in the gym might make you more willing and able to run for a bus in everyday life. However, this argument also remains to be tested.
We also acknowledge that the concept of habitual mindfulness may seem like an oxymoron. Surely, the clarity of awareness central to mindfulness practice is diametrically opposed to the automatic and mindless nature of habits? Indeed, mindfulness training curricula explicitly explore the problem of being in “automatic pilot” (Segal et al., 2013, p. 108). We have proposed that habits are helpful for those hoping to establish a regular mindfulness practice, but we draw the distinction between initiation of practice being automatic and practice itself being automatic, as also drawn by Mantzios and Giannou (2018). A behavior such as mindfulness practice can be triggered habitually and automatically, but performed mindfully and reflectively (Phillips & Gardner, 2016). However, future research should explore whether efforts to support the habitual initiation of practice have any qualitative impact on the experience of mindfulness during practice or in daily life.
Considering the implications of our model, we also note that mindfulness meditation could be considered both as a health behavior and as an intervention to support engagement with other health behaviors (as suggested by Langdon et al., 2011). Because mindfulness is associated with better self-regulation of other behaviors (Jordan et al., 2014), developing a mindfulness habit is likely to be both beneficial in itself and also to be part of a “virtuous cycle,” with positive effects expanding beyond mindfulness practice to other areas of life. Getting the mindfulness habit could facilitate healthy habit formation in other life areas, consistent with reports from participants in mindfulness-based interventions of “spillover” effects on other health behaviors (Scarlett et al., 2023). This hypothesis should be explored in multi-behavioral research. While striving to reap these benefits of mindfulness would contradict some of the underlying principles of mindfulness curricula, the existence of these benefits broadens the relevance to behavior change researchers of understanding how mindfulness meditation can best be facilitated.
Finally, we note the limitations of health behavior models that foreground the individual as agent in behavior change. This perspective can be critiqued for minimizing the importance of socio-economic-political environment and its role in supporting and sustaining change (see Kelly & Barker, 2016). Evidence suggests mindfulness practice does not reach all communities who may benefit equally, and that significant work is needed to increase access to practice (Olano et al., 2015; Simonsson et al., 2020). Future research should explore supports and barriers to mindfulness practice that include and extend beyond the individual to the broader social, economic, and political environment.
Conclusion
We have suggested that viewing mindfulness meditation as a health behavior could enable better understanding of the challenges associated with developing and sustaining mindfulness practice as well as more effective solutions for those challenges. As yet we have little evidence on whether our model helps to predict practice, nor whether strategies to promote behavior change and habit formation can help individuals to form a mindfulness habit and/or enhance the effectiveness of mindfulness interventions (cf. Davidson & Dahl, 2018); however, a strong evidence base from health behavior science suggests their potential effectiveness. The SuMMed model generates a programmatic research agenda as well as practical suggestions for real-world impact to optimize the potential benefits of mindfulness practice in a range of populations. Further research is needed to empirically test our account.
Data Availability
Not applicable to this article as no new data were created or analyzed.
References
Ajzen, P. (1991). The Theory of Planned Behavior. Organization Behavior and Human Decision Process, 50(2), 179–211. https://doi.org/10.1016/0749-5978(91)90020-T
Ajzen, I., Czasch, C., & Flood, M. G. (2009). From intentions to behavior: Implementation intention, commitment, and conscientiousness 1. Journal of Applied Social Psychology, 39(6), 1356–1372. https://doi.org/10.1111/j.1559-1816.2009.00485.x
Alidina, S., & Marshall, J. J. (2013). Mindfulness workbook for dummies. John Wiley & Sons.
Ashford, S., Edmunds, J., & French, D. P. (2010). What is the best way to change self-efficacy to promote lifestyle and recreational physical activity? A systematic review with meta-analysis. British Journal of Health Psychology, 15(2), 265–288. https://doi.org/10.1348/135910709X461752
Baldwin, A. S., Rothman, A. J., Hertel, A. W., Linde, J. A., Jeffery, R. W., Finch, E. A., & Lando, H. A. (2006). Specifying the determinants of the initiation and maintenance of behavior change: An examination of self-efficacy, satisfaction, and smoking cessation. Health Psychology, 25, 626–634. https://doi.org/10.1037/0278-6133.25.5.626
Bandura, A. (1998). Personal and collective efficacy in human adaptation and change. In Advances in psychological science: Social, personal, and cultural aspects (Vol. 1, pp. 51–71). Psychology Press/Erlbaum (UK), Hove, Taylor & Francis.
Banerjee, M., Cavanagh, K., & Strauss, C. (2017). A qualitative study with healthcare staff exploring the facilitators and barriers to engaging in a self-help mindfulness-based intervention. Mindfulness, 8(6), 1653–1664. https://doi.org/10.1007/s12671-017-0740-z
Bardacke, N. (2012). Mindful birthing: Training the mind, body and heart for childbirth and beyond. Harper Collins.
Beattie, M., Hankonen, N., Salo, G., Knittle, K., & Volanen, S.-M. (2019). Applying behavioral theory to increase mindfulness practice among adolescents: An exploratory intervention study using a within-trial RCT design. Mindfulness, 10(2), 312–324. https://doi.org/10.1007/s12671-018-0976-2
Berkman, E. T. (2017). Value-based choice: An integrative, neuroscience-informed model of health goals. Psychology & Health, 33(1), 40–57. https://doi.org/10.1080/08870446.2017.1316847
Brewer, J. A., Davis, J. H., & Goldstein, J. (2013). Why is it so hard to pay attention, or is it? Mindfulness, the factors of awakening and reward-based learning. Mindfulness, 4(1), 75–80. https://doi.org/10.1007/s12671-012-0164-8
Britton, W. B. (2019). Can mindfulness be too much of a good thing? The value of a middle way. Current Opinion in Psychology, 28, 159–165. https://doi.org/10.1016/j.copsyc.2018.12.011
Bryan, C. J., Walton, G. M., Rogers, T., & Dweck, C. S. (2011). Motivating voter turnout by invoking the self. Psychological and Cognitive Sciences, 108(31), 12653–12656. https://doi.org/10.1073/pnas.1103343108
Burch, V., & Penman, D. (2013). Mindfulness for health: A practical guide to relieving pain, reducing stress and restoring wellbeing. Hachette UK.
Cayoun, B., Elphinstone, B., Kasselis, N., Bilsborrow, G., & Skilbeck, C. (2022). Validation and factor structure of the Mindfulness-Based Self Efficacy Scale Revised. Mindfulness, 13(3), 751–765. https://doi.org/10.1007/s12671-022-01834-6
Chadwick, P., Strauss, C., Jones, A.-M., Kingdon, D., Ellett, L., Dannahy, L., & Hayward, M. (2016). Group mindfulness-based intervention for distressing voices: A pragmatic randomised controlled trial. Schizophrenia Research, 175(1–3), 168–173. https://doi.org/10.1016/j.schres.2016.04.001
Chang, V. Y., Palesh, O., Caldwell, R., Glasgow, N., Abramson, M., Luskin, F., Gill, M., Burke, A., & Koopman, C. (2004). The effects of a mindfulness-based stress reduction program on stress, mindfulness self-efficacy, and positive states of mind. Stress and Health, 20(3), 141–147. https://doi.org/10.1002/smi.1011
Coupe, N., Peters, S., Rhodes, S., & Cotterill, S. (2019). The effect of commitment-making on weight loss and behavior change in adults with obesity/overweight; A systematic review. BMC Public Health, 19, 816. https://doi.org/10.1186/s12889-019-7185-3
Crandall, A., Cheung, A., Young, A., & Hooper, A. P. (2019). Theory-based predictors of mindfulness meditation mobile app usage: A survey and cohort study. JMIR MHealth and UHealth, 7(3), e10794. https://doi.org/10.2196/10795
Crane, R. S. (2017). Implementing mindfulness in the mainstream: Making the path by walking it. Mindfulness, 8(3), 585–594. https://doi.org/10.1007/s12671-016-0632-7
Creswell, J. D. (2017). Mindfulness interventions. Annual Review of Psychology, 68(1), 491–516. https://doi.org/10.1146/annurev-psych-042716-051139
Cross, A., & Sheffield, D. (2019). Mental contrasting for health behavior change: A systematic review and meta-analysis of effects and moderator variables. Health Psychology Review, 13(2), 209–225. https://doi.org/10.1080/17437199.2019.1594332
Dai, H., Milkman, K. L., & Riis, J. (2014). The fresh start effect: Temporal landmarks motivate aspirational behavior. Management Science, 60(10), 2563–2582. https://doi.org/10.1287/mnsc.2014.1901
Davidson, R. J., & Dahl, C. J. (2018). Outstanding challenges in scientific research on mindfulness and meditation. Perspectives on Psychological Science, 13(1), 62–65. https://doi.org/10.1177/1745691617718358
de Zoysa, N., Ruths, F. A., Walsh, J., & Hutton, J. (2014). Mindfulness based cognitive therapy for mental health professionals: A long-term qualitative follow-up study. Mindfulness, 5(1), 10–17. https://doi.org/10.1007/s12671-012-0141-2
Deci, E. L., & Ryan, R. M. (2002). Self-determination research: Reflections and future directions. In Handbook of self-determination research (pp. 431–441). University of Rochester Press.
Del Re, A. C., Flückiger, C., Goldberg, S. B., & Hoyt, W. T. (2013). Monitoring mindfulness practice quality: An important consideration in mindfulness practice. Psychotherapy Research, 23(1), 54–66. https://doi.org/10.1080/10503307.2012.729275
DiClemente, C. C., & Prochaska, J. O. (1998). Toward a comprehensive, transtheoretical model of change: Stages of change and addictive behaviors. In Treating addictive behaviors (2nd ed., pp. 3–24). Plenum Press. https://doi.org/10.1007/978-1-4899-1934-2_1
Galante, J., Friedrich, C., Dawson, A. F., Modrego-Alarcon, M., Gebbing, P., Delgado-Suarez, I., Gupta, R., Dean, L., Dagleish, T., White, I. R., & Jones, P. B. (2021). Mindfulness-based programmes for mental health promotion in nonclinical settings: A systematic review and meta-analysis of randomised controlled trials. PLOS Medicine, 18(1), e1003481. https://doi.org/10.1371/journal.pmed.1003481
Galante, J., Brabovac, A., Wright, M., Ingram, D. M., Van Dam, N. T., Sanguinetti, J. L., Sparby, T., van Lutterveld, R., & Sacchet, M. D. (2023). A framework for the empirical investigation of mindfulness meditative development. Mindfulness, 14(5), 1054–1067. https://doi.org/10.1007/s12671-023-02113-8
Galla, B. M., Baelen, R. N., Duckworth, A. L., & Baime, M. J. (2016). Mindfulness, meet self-regulation: Boosting out-of-class meditation practice with brief action plans. Motivation Science, 2, 220–237. https://doi.org/10.1037/mot0000045
Gardiner, C. K., & Bryan, A. D. (2017). Monetary incentive interventions can enhance psychological factors relating to fruit and vegetable consumption. Annals of Behavioral Medicine, 51(4), 599–609. https://doi.org/10.1007/s12160-017-9882-4
Gardner, B., Lally, P., & Wardle, J. (2012). Making health habitual: The psychology of “habit-formation” and general practice. British Journal of General Practice, 62(605), 664–666. https://doi.org/10.3399/bjgp12X659466
Geschwind, N., Peeters, F., Drukker, M., van Os, J., & Wichers, M. (2011). Mindfulness training increases momentary positive emotions and reward experience in adults vulnerable to depression: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 79, 618–628. https://doi.org/10.1037/a002459
Gilbert, P., Basran, J., Plowright, P., Matos, M., Kirby, J., & Petrocchi, N. (2023). Fears and resistances to mindfulness: Development of a self-report scale. Mindfulness. https://doi.org/10.1007/s12671-023-02171-y
Gochman, D. S. (Ed.). (1997). Handbook of health behavior research (vols 1–4). Plenum.
Goldberg, S. B. (2022). A common factors perspective on mindfulness-based interventions. Nature Reviews Psychology, 1(10), 605–619. https://doi.org/10.1038/s44159-022-00090-8
Goldberg, S. B., Del Re, A. C., Hoyt, W. T., & Davis, J. M. (2014). The secret ingredient in mindfulness interventions? A case for practice quality over quantity. Journal of Counseling Psychology, 61(3), 491–497. https://doi.org/10.1037/cou0000032
Goldberg, S. B., Tucker, P. P., Greene, P. A., Simpson, T. L., Kearney, D. J., & Davidson, R. J. (2017). Is mindfulness research methodology improving over time? A systematic review. PLoS ONE, 12(10), e0187298. https://doi.org/10.1371/journal.pone.0187298
Goldberg, S. B., Tucker, R. P., Greene, P. A., Davidson, R. J., Wampold, B. E., Kearney, D. J., & Simpson, T. L. (2018). Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clinical Psychology Review, 59, 52–60. https://doi.org/10.1016/j.cpr.2017.10.011
Gollwitzer, P. M. (1999). Implementation intentions: Strong effects of simple plans. American Psychologist, 54, 493–503. https://doi.org/10.1037/0003-066X.54.7.493
Harkin, B., Webb, T. L., Chang, B. P. I., Prestwich, A., Conner, M., Kellar, I., Benn, Y., & Sheeran, P. (2016). Does monitoring goal progress promote goal attainment? A meta-analysis of the experimental evidence. Psychological Bulletin, 142, 198–229. https://doi.org/10.1037/bul0000025
Headspace. (2023). Headspace: Sleep & meditation [Mobile application software]. Apple Store or Google Play. www.headspace.com
Herman, C. P., & Polivy, J. (1984). A boundary model for the regulation of eating. Psychiatric Annals, 13(12), 918–927. https://doi.org/10.3928/0048-5713-19831201-03
Homan, K. J., & Sirois, F. M. (2017). Self-compassion and physical health: Exploring the roles of perceived stress and healthpromoting behaviors. Health Psychology Open, 4(2), 2055102917729542. https://doi.org/10.1177/2055102917729542
Howarth, A., Smith, J. G., Perkins-Porras, L., & Ussher, M. (2019). Effects of brief mindfulness-based interventions on health-related outcomes: A systematic review. Mindfulness, 10(10), 1957–1968. https://doi.org/10.1007/s12671-019-01163-1
Hunt, C. A., Hoffman, M. A., Mohr, J. J., & Williams, A.-L. (2020). Assessing perceived barriers to meditation: the Determinants of Meditation Practice Inventory-Revised (DMPI-R). Mindfulness, 11(5), 1139–1149. https://doi.org/10.1007/s12671-020-01308-7
Iyengar, S. S., & Lepper, M. R. (2000). When choice is demotivating: Can one desire too much of a good thing? Journal of Personality and Social Psychology, 79(6), 995–1006. https://doi.org/10.1037/0022-3514.79.6.995
Jetten, J., Haslam, C., Alexander, & Haslam, S. (Eds.). (2011). The social cure: Identity, health and well-being. Psychology Press. https://doi.org/10.4324/9780203813195.
Jones, F., Harris, P., Waller, H., & Coggins, A. (2010). Adherence to an exercise prescription scheme: The role of expectations, self-efficacy, stage of change and psychological well-being. British Journal of Health Psychology, 10(3), 359–378. https://doi.org/10.1348/135910704X24798
Jordan, C. H., Wang, W., Donatoni, L., & Meier, B. P. (2014). Mindful eating: Trait and state mindfulness predict healthier eating behavior. Personality and Individual Differences, 68, 107–111. https://doi.org/10.1016/j.paid.2014.04.013
Kabat-Zinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. Hyperion.
Kabat-Zinn, J., Lipworth, L., & Burney, R. (1985). The clinical use of mindfulness meditation for the self-regulation of chronic pain. Journal of Behavioral Medicine, 8(2), 163–190. https://doi.org/10.1007/BF00845519
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain and illness. Dell Publishing.
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10(2), 144–156. https://doi.org/10.1093/clipsy.bpg016
Kabat-Zinn, J. (2012). Mindfulness for beginners: Reclaiming the present moment—and your life. Sounds True.
Kabat-Zinn, J. (2013). Full catastrophe living, revised edition: How to cope with stress, pain and illness using mindfulness meditation. Hachette UK.
Kane, R. (2022). 21 One minute mindfulness exercises (that you can do anywhere). https://mindfulnessbox.com/one-minute-mindfulness-exercises. Accessed 24 May 2023
Kaushal, N., & Rhodes, R. E. (2015). Exercise habit formation in new gym members: A longitudinal study. Journal of Behavioral Medicine, 38(4), 652–663. https://doi.org/10.1007/s10865-015-9640-7
Kelly, M. P., & Barker, M. (2016). Why is changing health-related behavior so difficult? Public Health, 136, 109–116. https://doi.org/10.1016/j.puhe.2016.03.030
Koestner, R., Horberg, E. J., Gaudreau, P., Powers, T., Di Dio, P., Bryan, C., Jochum, R., & Salter, N. (2006). Bolstering implementation plans for the long haul: The benefits of simultaneously boosting self-concordance or self-efficacy. Personality and Social Psychology Bulletin, 32(11), 1547–1558. https://doi.org/10.1177/0146167206291782
Kozlov, E., Bantum, E., Pagano, I., Walser, R., Ramsey, K., Taylor, K., Jawprski, B., & Owen, J. (2020). The reach, use, and impact of a free mHealth mindfulness app in the general population: Mobile data analysis. JMIR Mental Health, 7(11), e23377. https://doi.org/10.2196/23377
Krusche, A., Cyhlarova, E., & Williams, J. M. G. (2013). Mindfulness online: An evaluation of the feasibility of a web-based mindfulness course for stress, anxiety and depression. British Medical Journal Open, 3(11), e003498. https://doi.org/10.1136/bmjopen-2013-003498
Kwasnicka, D., Dombrowski, S. U., White, M., & Sniehotta, F. (2016). Theoretical explanations for maintenance of behavior change: A systematic review of behavior theories. Health Psychology Review, 10(3), 277–296. https://doi.org/10.1080/17437199.2016.1151372
Lally, P., & Gardner, B. (2013). Promoting habit formation. Health Psychology Review, 7(1), S137–S158. https://doi.org/10.1080/17437199.2011.603640
Lally, P., van Jaarsveld, C. H. M., Potts, H. W. W., & Wardle, J. (2010). How are habits formed: Modelling habit formation in the real world. European Journal of Social Psychology, 40(6), 998–1009. https://doi.org/10.1002/ejsp.674
Lam, S. U., Kirvin-Quamme, A., & Goldberg, S. B. (2022). Overall and differential attrition in mindfulness-based interventions: A meta-analysis. Mindfulness, 13(11), 2676–2690. https://doi.org/10.1007/s12671-022-01970-z
Langdon, S., Jones, F. W., Hutton, J., & Holttum, S. (2011). A grounded-theory study of mindfulness practice following mindfulness-based cognitive therapy. Mindfulness, 2(4), 270–281. https://doi.org/10.1007/s12671-011-0070-5
Lipschitz, J. M., Pike, C. K., Hogan, T. P., Murphy, S. A., & Burdick, K. E. (2023). The engagement problem: A review of engagement with digital mental health interventions and recommendations for a path forward. Current Treatment Options in Psychiatry, 10, 119–135. https://doi.org/10.1007/s40501-023-00297-3
Mantzios, M., & Giannou, K. (2018). When did coloring books become mindful? Exploring the effectiveness of a novel method of mindfulness-guided instructions for coloring books to increase mindfulness and decrease anxiety. Frontiers in Psychology, 9, 56. https://doi.org/10.3389/fpsyg.2018.00056
Masheder, J., Fjorback, L., & Parsons, C. E. (2020). “I am getting something out of this, so I am going to stick with it”: Supporting participants’ home practice in Mindfulness-Based Programmes. BMC Psychology, 8(1), 91. https://doi.org/10.1186/s40359-020-00453-x
McEachan, R. R. C., Lawton, R. J., & Conner, M. (2010). Classifying health-related behaviors: Exploring similarities and differences amongst behaviors. British Journal of Health Psychology, 15(2), 347–366. https://doi.org/10.1348/135910709X466487
Michie, S., van Stralen, M. M., & West, R. (2011). The behavior change wheel: A new method for characterising and designing behavior change interventions. Implementation Science, 6(1), 42. https://doi.org/10.1186/1748-5908-6-42
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J., & Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. https://doi.org/10.1007/s12160-013-9486-6
Milkman, K. L., Minson, J. A., & Volpp, K. G. M. (2013). Holding the hunger games hostage at the gym: An evaluation of temptation bundling. Management Science, 60(2), 283–299. https://doi.org/10.1287/mnsc.2013.1784
Moore, S., Barbour, R., Ngo, H., Sinclair, C., Chambers, R., Auret, K., Hassed, C., & Playford, D. (2020). Determining the feasibility and effectiveness of brief online mindfulness training for rural medical students: A pilot study. BMC Medical Education, 20(1), 104. https://doi.org/10.1186/s12909-020-02015-6
Mrazek, A. J., Mrazek, M. D., Calcagnotto, L. A., Cloughesy, J. N., Holman, A. M., Masters-Waage, T. C., & Schooler, J. W. (2020). Familiarity, attitudes, and self-regulatory challenges related to mindfulness. Mindfulness, 11(5), 1218–1225. https://doi.org/10.1007/s12671-020-01332-7
Neal, D. T., Wood, W., & Drolet, A. (2013). How do people adhere to goals when willpower is low? The profits (and pitfalls) of strong habits. Journal of Personality and Social Psychology, 104, 959–975. https://doi.org/10.1037/a0032626
Nieuwlaat, R., Wilczynski, N., Navarro, T., Hobson, N., Jeffery, R., Keepanasseril, A., Agoritsas, T., Mistry, N., Iorio, A., Jack, S., Sivaramalingam, B., Iserman, E., Mustafa, R. A., Jedraszewski, D., Cotoi, C., & Haynes, B. R. (2014). Interventions for enhancing medication adherence. Cochrane Database of Systematic Reviews, 2014(11). https://doi.org/10.1002/14651858.CD000011.pub4
Oettingen, G., Wittchen, M., & Gollwitzer, P. M. (2013). Regulating goal pursuit through mental contrasting with implementation intentions. In E. A. Locke & G. P. Latham (Eds.), New developments in goal setting and task performance (pp. 523–548). Routledge/Taylor & Francis Group.
Olano, H. A., Kachan, D., Tannenbaum, S. L., Mehta, A., Annane, D., & Lee, D. J. (2015). Engagement in mindfulness practices by U.S. adults: Sociodemographic barriers. The Journal of Alternative and Complementary Medicine, 21(2), 100–102. https://doi.org/10.1089/acm.2014.0269
Olutende, O. M., Kweyu, I. W., & Wekesa, J. S. (2017). Health behavior intentions and barriers to physical activity among health science students: Exploring general self efficacy as a mediator. Journal of Physical Activity Research, 2(2), 101–106. https://doi.org/10.12691/jpar-2-2-6
Osin, E. N., & Turilina, I. I. (2021). Mindfulness meditation experiences of novice practitioners in an online intervention: Trajectories, predictors, and challenges. Health & Well-Being, 14(1), 101–121. https://doi.org/10.1111/aphw.12293
Parsons, C. E., Crane, C., Parsons, L. J., Fjorback, L. O., & Kuyken, W. (2017). Home practice in mindfulness-based cognitive therapy and mindfulness-based stress reduction: A systematic review and meta-analysis of participants’ mindfulness practice and its association with outcomes. Behavior Research and Therapy, 95, 29–41. https://doi.org/10.1016/j.brat.2017.05.004
Phillips, L. A., & Gardner, B. (2016). Habitual exercise instigation (vs. Execution) predicts healthy adults’ exercise frequency. Health Psychology, 35, 69–77. https://doi.org/10.1037/hea0000249
Prochaska, J. O., & Diclemente, C. C. (1986). Toward a comprehensive model of change. In W. R. Miller & N. Heather (Eds.), Treating addictive behaviors. Applied clinical psychology (Vol. 13, pp. 3–27). Springer. https://doi.org/10.1007/978-1-4613-2191-0_1
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of the structure of change. In Y. Klar, J. D. Fisher, J. M. Chinsky, & A. Nadler (Eds.), Self change: Social psychological and clinical perspectives (pp. 87–114). Springer. https://doi.org/10.1007/978-1-4612-2922-3_5
Remskar, M., Western, M. J., Maynard, O. M., & Ainsworth, B. (2022). Exercising body but not mind: A qualitative exploration of attitudes to combining physical activity and mindfulness practice for mental health promotion. Frontiers in Psychology, 13, 984232. https://doi.org/10.3389/fpsyg.2022.984232
Rogers, R. W., & Prentice-Dunn, S. (1997). Protection motivation theory. In Handbook of health behavior research 1: Personal and social determinants (pp. 113–132). Plenum Press.
Rosen, C. S. (2000). Is the sequencing of change processes by stage consistent across health problems? A meta-analysis. Health Psychology, 19, 593–604. https://doi.org/10.1037/0278-6133.19.6.593
Rosenstock, I. M. (2000). Health Belief Model. In Encyclopedia of psychology, Vol. 4. (pp. 78–80). American Psychological Association. https://doi.org/10.1037/10519-035
Rothman, A. J., Baldwin, A. S., Hertel, A. W., & Fuglestad, P. T. (2011). Self-regulation and behavior change: Disentangling behavioral initiation and behavioral maintenance. In K. D. Vohs & R. F. Baumeister (Eds.), Handbook of self-regulation: Research, theory, and applications (pp. 106–122). The Guilford Press.
Santorelli, S. F., Meleo-Meyer, F., Koerbel, L., & Kabat-Zinn, J. (2017). Mindfulness-based stress reduction (MBSR) authorized curriculum guide. Center for Mindfulness in Medicine, Health Care, and Society (CFM). University of Massachusetts Medical School.
Scarlett, C. A., Strosnider, C., Elahi, H., Dannenfelser, M., Owen-Smith, A., & Spears, C. A. (2023). “I use the meditation to calm myself instead of reaching for a cigarette”: Qualitative study of mindfulness-based addiction treatment among diverse adults. Mindfulness, 14(6), 1383–1394. https://doi.org/10.1007/s12671-023-02151-2
Schumer, M. C., Lindsay, E. K., & Creswell, J. D. (2018). Brief mindfulness training for negative affectivity: A systematic review and meta-analysis. Journal of Consulting and Clinical Psychology, 86, 569–583. https://doi.org/10.1037/ccp0000324
Schüz, B., Sniehotta, F. F., Wiedemann, A., & Seemann, R. (2006). Adherence to a daily flossing regimen in university students: Effects of planning when, where, how and what to do in the face of barriers. Journal of Clinical Periodontology, 33(9), 612–619. https://doi.org/10.1111/j.1600-051X.2006.00967.x
Schüz, B., Sniehotta, F. F., Mallach, N., Wiedemann, A. U., & Schwarzer, R. (2008). Predicting transitions from preintentional, intentional and actional stages of change. Health Education Research, 24(1), 64–75. https://doi.org/10.1093/her/cym092
Schwarzer, R. (2016). Health Action Process Approach (HAPA) as a theoretical framework to understand behavior Change. Actualidades En Psicología, 30(121), 119–130. https://doi.org/10.15517/ap.v30i121.23458
Segal, Z. V., Teasdale, J. D., Williams, J. M., & Gemar, M. C. (2002). The mindfulness-based cognitive therapy adherence scale: Inter-rater reliability, adherence to protocol and treatment distinctiveness. Clinical Psychology & Psychotherapy, 9(2), 131–138. https://doi.org/10.1002/cpp.320
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2013). Mindfulness-based cognitive therapy for depression (2nd ed.). The Guilford Press.
Sheeran, P. (2002). Intention-behavior relations: A conceptual and empirical review. European Review of Social Psychology, 12(1), 1–36.
Sheeran, P., & Webb, T. L. (2016). The intention–behavior gap. Social and Personality Psychology Compass, 10(9), 503–518. https://doi.org/10.1111/spc3.12265
Sheeran, P., Webb, T. L., & Gollwitzer, P. M. (2005). The interplay between goal intentions and implementation intentions. Personality and Social Psychology Bulletin, 31(1), 87–98. https://doi.org/10.1177/0146167204271308
Sheeran, P., Aubrey, R., & Kellett, S. (2007). Increasing attendance for psychotherapy: Implementation intentions and the self-regulation of attendance-related negative affect. Journal of Consulting and Clinical Psychology, 75, 853–863. https://doi.org/10.1037/0022-006X.75.6.853
Sheeran, P., Klein, W. M. P., & Rothman, A. J. (2017). Health behavior change: Moving from observation to intervention. Annual Review of Psychology, 68, 573–600. https://doi.org/10.1146%2Fannurev-psych-010416-044007
Sheeran, P., Wright, C. E, Listrom, O., Klein, W. M., & Rothman, A. J. (2023). Which intervention strategies promote the adoption and maintenance of physical activity? Evidence from behavioral trials with cancer survivors. Annals of Behavioral Medicine, 57(9), 708–721. https://doi.org/10.1093/abm/kaad002
Simonsson, O., Martin, M., & Fisher, S. (2020). Sociodemographic characteristics and health status of mindfulness users in the United States. Mindfulness, 11(12), 2725–2729. https://doi.org/10.1007/s12671-020-01486-4
Sommers-Spijkerman, M., Austin, J., Bohlmeijer, E., & Pots, W. (2021). New evidence in the blooming field of mindfulness: An updated meta-analysis of randomised controlled trials. JMIR Mental Health, 8(7), e28168. https://doi.org/10.2196/28168
Strauss, C., Dunkeld, C., & Cavanagh, K. (2021). Is clinician-supported use of a mindfulness smartphone app a feasible treatment for depression? A mixed-methods feasibility study. Internet Interventions, 5(25), 100413. https://doi.org/10.1016/j.invent.2021.100413
Sullivan, M., Huberty, J., Chung, Y., & Stecher, C. (2023). Mindfulness meditation app abandonment during the COVID-19 pandemic: An observational study. Mindfulness, 14(6), 1504–1521. https://doi.org/10.1007/s12671-023-02125-4
Sutton, S. (2001). Back to the drawing board? A review of applications of the Transtheoretical Model to substance use. Addiction, 96, 175–186. https://doi.org/10.1080/09652140020017049
Tang, Y.-Y., Hölzel, B. K., & Posner, M. I. (2015). The neuroscience of mindfulness meditation. Nature Reviews Neuroscience, 16(4), 213–225. https://doi.org/10.1038/nrn3916
Taylor, H., Strauss, C., & Cavanagh, K. (2021). Can a little bit of mindfulness do you good? A systematic review and meta-analyses of unguided mindfulness-based self-help interventions. Clinical Psychology Review, 89, 102078. https://doi.org/10.1016/j.cpr.2021.102078
Teasdale, J. D., Williams, J. M. G., & Segal, Z. V. (2014). The mindful way workbook: An 8-week program to free yourself from depression and emotional distress. Guilford Press.
Tickell, A., Ball, S., Bernard, P., Kuyken, W., Marx, R., Pack, S., Strauss, C., Sweeney, T., & Crane, C. (2020). The effectiveness of mindfulness-based cognitive therapy (MBCT) in real-world healthcare services. Mindfulness, 11, 279–290. https://doi.org/10.1007/s12671-018-1087-9
Van Gordon, W., Sapthiang, S., & Shonin, E. (2022). Contemplative psychology: History, key assumptions, and future directions. Perspectives on Psychological Science, 17(1), 99–107. https://doi.org/10.1177/1745691620984479
Verplanken, B., & Sui, J. (2019). Habit and identity: Behavioral, cognitive, affective, and motivational facets of an integrated self. Frontiers in Psychology, 10, 1504. https://doi.org/10.3389/fpsyg.2019.01504
Wei, M. (n.d.). You can practice mindfulness in as little as 15 minutes a day. https://www.health.harvard.edu/mind-and-mood/you-can-practice-mindfulness-in-as-little-as-15-minutes-a day. Accessed 24 May 2023.
Weinstein, N. D. (1988). The precaution adoption process. Health Psychology, 7, 355–386. https://doi.org/10.1037/0278-6133.7.4.355
Werner, K. M., Milyavskaya, M., Foxen-Craft, E., & Koestner, R. (2016). Some goals just feel easier: Self-concordance leads to goal progress through subjective ease, not effort. Personality and Individual Differences, 96, 237–242. https://doi.org/10.1016/j.paid.2016.03.002
Wiedemann, A. U., Lippke, S., Reuter, T., Ziegelmann, J. P., & Schwarzer, R. (2011). How planning facilitates behavior change: Additive and interactive effects of a randomized controlled trial. European Journal of Social Psychology, 41(1), 42–51. https://doi.org/10.1002/ejsp.724
Williams, M., & Penman, D. (2011). Mindfulness: A practical guide to finding peace in a frantic world. Hachette UK.
Williams, J. M. G., & Kabat-Zinn, J. (2011). Mindfulness: Diverse perspectives on its meaning, origins, and multiple applications at the intersection of science and dharma. Contemporary Buddhism, 12(1), 1–18. https://doi.org/10.1080/14639947.2011.564811
Winter, N., Russell, L., Ugalde, A., White, V., & Livingston, P. (2022). Engagement strategies to improve adherence and retention in web-based mindfulness programs: Systematic review. Journal of Medical Internet Research, 24(1), e30026. https://doi.org/10.2196/30026
Wood, W., & Neal, D. T. (2016). Healthy through habit: Interventions for initiating & maintaining health behavior change. Behavioral Science & Policy, 2(1), 71–83. https://doi.org/10.1353/bsp.2016.0008
Wood, W., & Rünger, D. (2016). Psychology of habit. Annual Review of Psychology, 67(1), 289–314. https://doi.org/10.1146/annurev-psych-122414-033417
Wood, W., Tam, L., & Witt, M. G. (2005). Changing circumstances, disrupting habits. Journal of Personality and Social Psychology, 88, 918–933. https://doi.org/10.1037/0022-3514.88.6.918
Wyatt, C., Harper, B., & Weatherhead, S. (2013). The experience of group mindfulness-based interventions for individuals with mental health difficulties: A meta-synthesis. Psychotherapy Research, 24(2), 214–228. https://doi.org/10.1080/10503307.2013.864788
Young, K. (n.d.). 13 different ways to practice mindfulness – And the difference it can make. https://www.heysigmund.com/different-ways-to-practice-mindfulness. Accessed 24 May 2023.
Funding
The authors did not receive support from any organization for the submitted work. C.S. and K.C. have received research support from Headspace outside the submitted work.
Author information
Authors and Affiliations
Contributions
E.M. and K.C. had the idea for the article and prepared the original draft. All authors were involved in drafting and critical revision.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Miles, E., Matcham, F., Strauss, C. et al. Making Mindfulness Meditation a Healthy Habit. Mindfulness 14, 2988–3005 (2023). https://doi.org/10.1007/s12671-023-02258-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-023-02258-6