
Abstract
Previous research among experienced meditators suggests that the associations of trait mindfulness with mental health are mediated by emotion regulation, body awareness, and a less static perspective of the self. The present study sought to elucidate whether this mediational model is also applicable to the general population and whether further potential mechanisms of action need to be included. Meditators and nonmeditators differ in overall mindfulness levels, but also in the structural properties of mindfulness facets. Meditation experience might bring about a change of variables that explain the associations of mindfulness with mental health. We examined the confirmatory fit of the mediational model in a large, German-speaking general population sample (N = 1133) with structural equation modeling, and investigated in an exploratory fashion whether further mediating variables needed to be included in the model. As a side goal, the structural properties of a short form of the Five Facet Mindfulness Questionnaire (FFMQ) were re-examined. Results suggest that variables and mechanisms which mediate the associations between trait mindfulness and mental health are the same for meditators and the general population. Differences pertain to the strength and direction of some of these associations. The short-form FFMQ is recommended for further research. It was replicably shown to have a two-factor higher-order structure. Findings are discussed with regard to mindfulness training and intervention. Potential mechanisms of action may not be intervention-specific, but may also explain the links between trait mindfulness and mental health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mindfulness is well-known to have positive effects on mental health. In clinical trials, Mindfulness Based Stress Reduction (MBSR) and other mindfulness-based interventions showed positive effects on mental health among clinical populations (e.g., Bohlmeijer et al. 2010; Grossman et al. 2004; Khoury et al. 2013). Positive effects of mindfulness on mental health have further been observed among experienced meditators (for a review, see Hölzel et al. 2011; for primary data, see, for example, Baer et al. 2008 or Tran et al. 2014), and for mindfulness-based trainings and interventions in community samples (Agee et al. 2009; Szekeres and Wertheim 2015), in an educative context (Langer et al. 2015), and in a workplace context (Ravalier et al. 2016).
Consequently, research increasingly focuses on the mechanisms of mindfulness. Current research suggests that improvements in attention regulation, body awareness, and emotion regulation, and a less static perspective about the self (Hölzel et al. 2011) may be responsible for the positive effects of mindfulness on mental health. This model has been further cast into a neurobiological framework, for which there is ample support from neuroscience studies of meditation practice and among experienced meditators (Vago and Silbersweig 2012). Clinical research has yielded empirical evidence of related postulated mechanisms of mindfulness-based cognitive therapy; however, more data and evidence of causal specificity of these mechanisms still are needed (Van der Velden and Roepstorff 2015).
Mindfulness may be considered as a skill which can be increased by training (Bishop et al. 2004), while it also is a dispositional trait which may be assumed to be present in every person (Brown and Ryan 2003). Individuals are dispositionally more or less mindful, even in the absence of any training, be it formal or informal. These current views of mindfulness as being both a skill and a trait may strike as inconsistent or conflicting, but, empirically, they rather complement each other. Widely used instruments for the assessment of trait mindfulness, like the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al. 2006), are highly sensitive to change (e.g., Bohlmeijer et al. 2011) and are routinely used in intervention studies. Mindfulness-based interventions were found to increase trait mindfulness, and these increases also explain treatment effects on mental health (for meta-analytic evidence and reviews, see Gu et al. 2015; Van der Velden and Roepstorff 2015). Similarly, meditation training is linked with higher trait mindfulness, as measured with the FFMQ (e.g., Baer et al. 2008; Taylor and Millear 2016; Tran et al. 2014). For a recent attempt to disentangle the trait and state components of one specific scale that intends to measure state mindfulness, see Medvedev et al. (2017).
Drawing on the theoretical framework of potential mechanisms of mindfulness, as proposed by Hölzel et al. (2011), research among experienced meditators (Tran et al. 2014) has shown that meditation experience and mindfulness are positively associated with indicators of all proposed mechanisms, i.e., attention regulation, body awareness, emotion regulation, and a change in perspective on the self. However, only improvements in emotion regulation and body awareness, but not in attention regulation, and a less static perspective about the self (nonattachment; see below) explained the effects of trait mindfulness on mental health. Body awareness appeared to be a specific pathway for the effects of trait mindfulness on symptoms of anxiety, whereas nonattachment (i.e., the relative absence of a fixation on ideas, images, or sensory objects, and of internal pressure to get, hold, avoid, or change circumstances or experiences; Sahdra et al. 2010) for symptoms of depression.
In the light of an apparent malleability of trait mindfulness through mindfulness interventions and training, cross-sectional investigations into the potential mechanisms (i.e., mediators) of the associations between trait mindfulness and mental health in nonmeditating samples also appear to be useful, besides longitudinal and prospective research. Trait mindfulness shows associations with mental health not only among meditators, but also among the meditation-naïve. This begs the question which mechanisms explain these associations among the latter: are they the same as among experienced meditators or do they differ? Cross-sectional studies in nonmeditating samples could thus provide information on (1) candidate mechanisms that show promise for further study in longitudinal and intervention studies, because any mechanism that is causally linked with an outcome should also co-vary with this outcome (Kraemer et al. 2002; see also Kraemer et al. 1997); (2) mechanisms that are specific to mindfulness-based trainings and interventions. While cross-sectional mediation analysis cannot provide direct evidence on the causal specificity of candidate mechanisms (because it lacks the necessary temporal dimension), it may provide indirect evidence on whether mechanisms reported for interventions or training might be specific to them or not so, i.e., when mechanisms are not similarly observed to mediate the associations between the “naturally” occurring levels of trait mindfulness and mental health among meditation-naïve individuals. Insight into these issues may help in explaining the associations between trait mindfulness and mental health and may help clarifying the specific mechanisms of mindfulness-based interventions and meditation. It may also promote the development of effective therapies by uncovering mechanisms which might not be specific, but the importance of which may have been underestimated previously.
Meditators and nonmeditators not only differ in the level, but also in the structure of trait mindfulness: The five facets of the FFMQ (Observe, Describe, Acting with Awareness [Actaware], Nonjudging of Inner Experience [Nonjudge], Nonreactivity to Inner Experience [Nonreact]) fit onto a single higher-order factor of mindfulness only among experienced meditators (Baer et al. 2006, 2008). Among nonmeditating samples, Observe does not load on higher-order mindfulness and thus is seemingly not part of a common underlying construct (Baer et al. 2006). Tran et al. (2013, 2014) proposed to explain these structural differences by applying an alternative two-factor higher-order structure to the FFMQ, which factors represent the two quintessential components of mindfulness brought forth by Bishop et al. (2004): Orientation to experience (OTE; being open and curious about the world and accepting experiences without judgment) and self-regulated attention (SRA; the mental ability to concentrate attention on the present moment and to deliberately switch the object of attention). These two higher-order factors provide not only direct empirical support for a widely used theoretical model of mindfulness. They also allow for a parsimonious examination of the associations of the multi-facetted construct of mindfulness with other constructs, as the two higher-order factors of the FFMQ subsume all of its five lower-order factors. Observe and, among meditators, Nonreact and Describe were found to be specifically indicative of SRA, whereas Actaware and Nonjudge of OTE (Tran et al. 2013, 2014). Structural differences between meditators and nonmeditators in the single-factor model were quantified by the strength of association between SRA and OTE in the two-factor model. This association was modest among nonmeditators (r = .20), whereas substantial among meditators (r = .62–.69). Providing further support for the special link between meditation experience and Observe, Taylor and Millear (2016) reported that increases of trait mindfulness apparently level off with more meditation experience, whereas remain stable for Observe.
Changes in the structure of trait mindfulness are further accompanied by changes in the associations of Observe with relevant outcomes. Previous research showed that Observe correlates slightly positively with symptoms of depression and anxiety in nonmeditating samples (e.g., Baer et al. 2006; Tran et al. 2013), possibly reflecting ruminative tendencies (i.e., repetitive thinking about negative outcomes). Only among meditators, all five facets of the FFMQ were consistently negatively associated with psychological symptoms (Baer et al. 2006, 2008; Tran et al. 2014).
It thus appears that there are marked differences between meditators and nonmeditators in trait mindfulness and its associations with mental health. It therefore seems possible that other mechanisms account for the associations of trait mindfulness with mental health among nonmeditators, as compared to meditators. Disentangling the mechanisms of mindfulness that are specific to meditation and intervention from mechanisms that provide common links between trait mindfulness and mental health in the absence of meditation training could help to elucidate the associations between trait mindfulness and mental health, and the effects of mindfulness-based interventions. Previous research suggests that in the general population emotion regulation largely mediates the associations between trait mindfulness and mental health (Freudenthaler et al. 2017); nonattachment mediates the associations between trait mindfulness and satisfaction with life, and life effectiveness (Sahdra et al. 2016). However, there are no studies which would have examined a wider range of candidate mechanisms simultaneously. As well, associations with emotion regulation have been investigated on the aggregate level (i.e., overall emotion regulation), rather than on the subscale level (e.g., impulse control or emotional awareness). This leaves open the question which of the individual aspects of emotion regulation might be the most important ones.
Mindfulness-based trainings and meditation (e.g., yoga) gained popularity in recent years and are also frequently sought after in the general population. Thus, the general population cannot be assumed to be fully meditation-naïve. Hence, meditation experience needs to be assessed and statistically controlled for in studies with general population samples. Further, previous studies by Tran et al. (2014) and Freudenthaler et al. (2017) investigated the associations of trait mindfulness with symptoms of depression and anxiety. Somatic complaints are widely prevalent in the general population as well (e.g., Kroenke 2003); hence, they are an additional outcome of interest.
The current study sought to test and to explore whether the associations between trait mindfulness and mental health are mediated by the same mechanisms among mostly meditation-naïve individuals of the general population as among experienced meditators (Tran et al. 2014). This was our Research Goal 1. Thus, we sought to test the replicability of findings that have previously been reported for meditators with a general population sample. We extend previous evidence (Freudenthaler et al. 2017; Sahdra et al. 2016; Tran et al. 2014) by including somatization symptoms and test the associations of the higher-order factors of mindfulness with a wider array of candidate mechanisms on their subscale level. Meditation experience was controlled for in the analysis. Further, previous studies with meditating and nonmeditating samples (Tran et al. 2013, 2014) proposed short forms of the FFMQ, showing that these had improved measurement properties, and fitted a two-factor higher-order model on the data. Consequently, the current study also utilized a short form of the FFMQ for analysis. Investigating the factorial validity of this short form, and whether the two-factor higher-order model replicably fitted well on new and independent data, was our Research Goal 2. We expected that a good factorial validity of the FFMQ short form and that a two-factor higher-order model of trait mindfulness would fit well to the general population data of the current study. In the absence of prior data suggesting otherwise, we hypothesized that mechanisms of mindfulness, and directions of effects, would broadly stay the same, but that effects would be smaller than in meditating samples (see Tran et al. 2014). Specifically, we expected that the associations of SRA with mental health would be smaller in the current general population sample, and, hence, that intervening mechanisms would explain comparably less variance.
Method
Participants
This study used data of N = 1133 participants (608 [54%] women) from the general population. Participants’ age ranged from 18 to 86 years (M = 37.67, SD = 16.11). Participants mostly were of Austrian (58%) or German (39%) nationality; the remaining 3% were mainly from other European countries. Participants came from various educational backgrounds: most (55%) had completed secondary education, 24% had completed tertiary education, and 21% primary education. Regarding prior meditation experience (see Measures), 829 participants (73%) reported that they had never, or on no regular basis (i.e., less than once a week; see Measures), practiced any form of meditation or relaxation technique, 268 (24%) practiced at least once a week (i.e., regularly), 36 (3%) provided no data. Among the regular practitioners who provided also data on meditation style (178 participants in total), yoga was by far the most common mediation style (82 participants; 46%), followed by zen (16; 9%) and qi gong (15; 8%), Transcendental Meditation and Tai Chi (7 [4%] participants each), and Vipassana and mindfulness-based stress reduction (MBSR; 2 [1%] participants each). A further 43 participants (24%) practiced some form of mind-body meditation (e.g., yoga and zen) or idiosyncratic styles (e.g., Christian repetitive prayer or Tantra meditation practice), and 3 (1%) practiced autogenic training or progressive muscle relaxation.
Procedure
Participants were contacted through personal contacts and word-of-mouth advertising. To minimize recruitment bias and to increase the sample heterogeneity, data collection was crowdsourced and distributed to a larger number of research assistants. Participation in the study was entirely anonymous and participants received no remuneration. All participants gave informed consent prior to inclusion in the study. Testing took place individually in quiet facilities. There were no exclusion criteria, except that persons were required to be at least 18 years of age and fluent in German, as this was the survey language.
Measures
The same scales that had been used in Tran et al. (2014) were also utilized in the current study. German translations of the SBC and the NAS (see the following) were obtained via the parallel blind technique (Behling and Law 2000).
Meditation Experience
The practice of (1) mindfulness or meditation, (2) autogenic training or progressive muscle relaxation, and (3) other relaxation techniques was queried on 6-point scales (0 = never, 1 = not regularly, 2 = once per week, 3 = twice per week, 4 = thrice per week, 5 = four times per week or more often). The highest of these three ratings was transferred to a new variable which captured overall meditation experience, scored from 0 = never or not regularly (condensing responses 0 and 1 of the above items) and 1 = once per week to 5 = four times per week or more often. Consistent with Baer et al. (2008), participants who meditated or practiced at least once a week were considered regular practitioners. Regular practitioners were queried for the type of meditation they had practiced most in the last 6 months.
Mindfulness
Mindfulness was assessed with the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al. 2006; German form: Tran et al. 2013). Items of the FFMQ are scored on a 5-point scale (1 = never or very rarely true, 5 = very often or always true). Eight items each measure the facets of Observe, Describe, Actaware, and Nonjudge; Nonreact is measured with seven items. Observe relates to noticing and attending inner and external experiences. Describe relates to mentally noting, and of being able to verbally describe, internal stimuli. Actaware relates to being consciously aware of one’s own behavior and of the ongoing situation. Nonjudge relates to desisting assessments and evaluations of one’s own feelings and thoughts. Nonreact relates to accepting the continual coming and going of experiences and thoughts. For analysis, only a subset of all 39 FFMQ items was used, selecting only the psychometrically most informative items. Previous research proposed slightly different item selections for Describe, Nonjudge, and Nonreact among nonmeditating (Tran et al. 2013) and meditating samples (Tran et al. 2014). We computed Cronbach αs of these proposed item selections and utilized those for further analysis that yielded the highest coefficients. This resulted for Nonjudge in using the item selection of Tran et al. (2013), and for Describe in using the item selection of Tran et al. (2014). Following Tran et al. (2014), all seven items of Nonreact were used for analysis. Cronbach α of the final scales in the current study was .70 for Observe (4 items), .79 for Describe (4 items), .82 for Actaware (4 items), .81 for Nonjudge (4 items), and .77 for Nonreact (7 items).
Depression, Anxiety, and Somatization
The Brief symptom inventory 18 (BSI-18; Spitzer et al. 2011) was used to assess current psychological distress. The questionnaire assesses the prevalence and level of distress of a variety of psychologically relevant symptoms during the last 7 days. The BSI-18 consists of three subscales with six items each: depression, anxiety, and somatization, scored on a 5-point scale (0 = not at all, 4 = extremely). High scores indicate a high symptom burden. Cronbach α was .84 (depression), .76 (somatization), and .73 (anxiety) in the current study.
Mechanisms of Mindfulness
Attention regulation was assessed with the Effortful Control Scale of the ATQ (Evans and Rothbart 2007; German form: Wiltink et al. 2006). The scale consists of three subscales: attentional control (7 items; the ability to focus and intentionally shift attention), inhibitory control (5 items; the ability to deal with spontaneous, positive impulses and to inhibit inadequate behavioral responses), and activation control (7 items; the ability to suppress negatively toned response that may cause avoidance behavior). The items are scored on a 7-point Likert scale (1 = total disagreement, 7 = total agreement). Cronbach α was .69 (attentional control), .54 (inhibitory control), and .70 (activation control) in the current study.
Body awareness was assessed with a German translation of the Scale of Body Connection (SBC; Price and Thompson 2007). The scale consists of two subscales: body awareness (12 items; attention to sensory signals of bodily state) and body dissociation (8 items; body connection and separation, including emotional connection). The items are scored on a 5-point Likert scale (0 = not at all, 4 = all the time). For ease of interpretation, the items of the body dissociation subscale were reverse scored in the current study and the subscale named body association (see Tran et al. 2014). Cronbach α was .82 (body awareness) and .67 (body association) in the current study.
Aspects of emotion regulation were assessed with the Experience Questionnaire (EQ; Fresco et al. 2007; German form: Gecht et al. 2013) and the Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer 2004; German form: Ehring et al. 2008). The 11-item EQ assesses decentering, the ability to observe one’s own thoughts and feelings as a temporary and objective event of the mind which includes the ability to correctly interpret one’s own emotions and other internal events (Fresco et al. 2007). The EQ consist of three facets (the ability to positively accept the self as a person, the ability to avoid habitual reactions to negative experiences, and a self-view that can distinguish between one’s thoughts and the self), but is considered a unidimensional construct, connected to metacognitive awareness (Teasdale et al. 2002). The items are scored on a 5-point Likert scale (1 = never or very rarely true, 5 = very often or always true). Cronbach α was .71 in the current study.
The DERS assesses difficulties in emotion regulation. It consists of six subscales: Nonacceptance of emotions (6 items), difficulties engaging in goal-directed behavior (5 items), impulse control difficulties (6 items), lack of emotional awareness (6 items), limited access to emotion regulation strategies (8 items), and lack of emotional clarity (5 items). The items are rated on a 5-point Likert scale (1 = almost never, 5 = almost always). High scores in the DERS reflect difficulties in emotion regulation. For ease of interpretation, the items of the DERS were reverse scored in the current study and appropriately renamed (see below) to reflect ability, rather than difficulties, in emotion regulation (see Tran et al. 2014). Cronbach α in the current study was .83 (acceptance of emotions), .85 (goal-directed behavior), .80 (impulse control), .79 (emotional awareness), .89 (access to emotion regulation strategies), and .80 (emotional clarity).
Nonattachment was assessed with a German translation of the 30-item Nonattachment Scale (NAS; Sahdra et al. 2010). Items are scored on a 6-point scale (1 = disagree strongly, 6 = agree strongly). Cronbach α was .90 in the current study.
Data Analyses
The mediational analyses depended on the results of the prior factorial and structural analyses of the FFMQ items (Research Goal 2). Hence, analyses of Research Goal 2 are presented prior to the analyses of Research Goal 1 in this section and in the Results section. All analyses were performed with Mplus 6.11 (Muthén and Muthén 2008). Model fit was assessed with the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), and the Root Mean Square Error of Approximation (RMSEA). For interpretation, we followed the widely used cutoffs proposed by Hu and Bentler (1999): CFI and TLI, good fit ≥ .95 and acceptable fit, ≥ .90; RMSEA, good fit < .06 and acceptable fit < .08.
Structural Analysis of the FFMQ
Exploratory structural equation modeling (ESEM; Asparouhov and Muthén 2009) was used to investigate the factor structure of the five FFMQ facets on the item level. ESEM is specifically useful for testing for item cross-loadings that may otherwise not be recognized in traditional confirmatory SEM and CFA analyses. We fitted a five-factor ESEM to the data (see Tran et al. 2013, 2014). As the items of the FFMQ represent ordered categorical variables, the weighted least square mean- and variance-adjusted (WLSMV) estimator was used, which is based on the polychoric item correlation matrix.
Two-Factor Higher-Order Structure
A two-factor ESEM was fitted to the facet factor scores of the FFMQ analysis of the previous item-level analysis. A genuine higher-order analysis using item-level data is currently not possible with ESEM. For this analysis, robust maximum likelihood estimation (MLR) and oblique quartimax rotation were used (see Tran et al. 2013, 2014). To test for the possibility of a one-factor higher-order structure, the model fit of this alternative model was also obtained and compared with the results of the two-factor model.
Structural Equation Modeling of Mindfulness Mechanisms
In the first step, the associations of the higher-order factors of mindfulness with all candidate mechanisms were explored in the current sample. As in Tran et al. (2014), a path model was fitted to the data, using meditation experience as exogenous (i.e., input) variable, the two higher-order factors as mediating variables, and all candidate mechanisms as endogenous (i.e., output) variables. Thereby, we estimated the relative importance of the two higher-order factors for the various candidate mechanisms and the probable contribution of meditation experience. In this exploratory analysis, only significant (p < .05) paths with standardized coefficients ≥ |.10| were retained in the final model. Thus, only associations with at least small effect size (Cohen 1988) were of interest here.
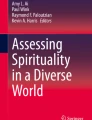
In the second step, the path model of Tran et al. (2014) was fitted to the current data. This served as a confirmatory test of the associations between mindfulness, candidate mechanisms, and mental health among the general population. We were interested in whether a mediational model, as obtained among experienced meditators, fitted equally well to the data of the current general population sample. The model (Fig. 1) included meditation experience as an exogenous variable with paths to the first layer of mediating variables, the higher-order factors of mindfulness. These, in turn, had paths to a second layer of mediating variables which were of special interest here, pertaining to body awareness, acceptance of emotions, impulse control, access to emotion regulation strategies, emotional clarity, and nonattachment. Previous research, utilizing the Spanish form of the DERS, measured the meditators’ impulse control and access to emotion regulation strategies with a single scale (Tran et al. 2014); in the Spanish form, these two scales are part of a single scale.

Confirmatory path model of the associations of meditation experience with mindfulness, mechanisms of mindfulness, and depression and anxiety. Numbers are standardized path coefficients. SRA = self-regulated attention; OTE = orientation to experience; ER = emotion regulation. SRA and OTE were allowed to correlate, as were the mechanisms, and depression and anxiety. All p’s ≤ .004, except for the paths from SRA to impulse control (p = .090), SRA to access to emotion regulation strategies (p = .037), impulse control to depression (p = .759), and nonattachment to depression (p = .031)
In the third step, an exploratory path model was constructed, informed by the foregoing analyses, to optimize the confirmatory model (i.e., by deleting or emending paths) and to examine whether any candidate mechanisms that had not been part of this model explained further increments of variance of the output variables. In this analysis, somatization was utilized as a further output variable. Model building followed a stepwise approach, where we strove to retain in the final model only significant (p < .05) paths with standardized coefficients > |.10| and candidate mechanisms with at least one ingoing and one outgoing significant path with a standardized coefficient ≥ |.10| (see Tran et al. 2014).
Results
Intercorrelations, means, and standard deviations of all investigated variables are provided in the supplemental materials.
Structural Analysis of the FFMQ
The five-factor ESEM had a good data fit: χ2(148) = 497.82, p < .001, CFI = .979, TLI = .964, RMSEA = .046, 95% confidence interval = [.041, .050]. All items loaded highly on their expected factor and had no relevant cross-loadings on any of the other factors (see Table 1). This suggests that all facets were essentially unidimensional. All factors were significantly and positively intercorrelated, except for Observe and Actaware (Table 2).
Two-Factor Higher-Order Structure
A two-factor ESEM had a good fit on the facet factor scores: χ2(1) = 6.35, p = .012, CFI = .993, TLI = .934, RMSEA = .069 [.026, .124]. The loadings of the facets on the higher-order factors are displayed in Table 3. All facets except Observe loaded highly on OTE, whereas only Observe showed a high loading on SRA. This pattern is similar to prior results among nonmeditators (Tran et al. 2013), but differs from the pattern observed among meditators (Tran et al. 2014), where specifically Nonreact, Observe, and Describe loaded on SRA, and only Nonjudge and Actaware had salient loadings on OTE. SRA and OTE correlated with r = .25 (p < .001) in the current sample, which is similar to prior results among nonmeditators (r = .20; Tran et al. 2013).
A model with only one higher-order factor fitted the data considerably worse: χ2(5) = 196.24, p < .001, CFI = .765, TLI = .529, RMSEA = .184 [.162, .206]. Facets loaded between .64 (Nonreact) and .56 (Actaware) on this higher-order factor and particularly the loading of Observe was only low (.35). These results indicate that a two-factor higher-order structure represented the latent structure of mindfulness in the current sample better than a one-factor higher-order structure.
Structural Equation Modeling of Mindfulness Mechanisms
Correlations between meditation experience, SRA, OTE, candidate mechanisms of mindfulness, and depression, somatization, and anxiety are displayed in Table 4. Predicting all candidate mechanisms of mindfulness via meditation experience and the two-higher-order factors of mindfulness resulted in a good model fit: χ2(18) = 43.43, p < .001, CFI = .996, TLI = .974, RMSEA = .035 [.022, .049]. Overall, OTE appeared to be more important than SRA, with exceptions of body awareness and emotional clarity (Table 4). Notably, higher scores in SRA somewhat interfered (negative path coefficients) with attentional control, acceptance of emotions, and goal-directed behavior. Attributable variance was highest for nonattachment, attentional control, decentering, acceptance of emotions, access to emotion regulation strategies, and emotional clarity. The total effect of meditation experience was low for most of the candidate mechanisms in the current sample. Meditation experience explained only about 6 and 4% of the variance of SRA and OTE.
The confirmatory fit of the Tran et al. (2014) model on the current data was good: χ2(12) = 82.38, p < .001, CFI = .983, TLI = .937, RMSEA = .063 [.050, .077]. All paths were significant (p < .05), with exceptions of the paths of SRA to impulse control, and of impulse control to depression scores (see Fig. 1). Some path coefficients appeared to be rather negligible in size (i.e., < |.10|) and/or were not significant in the current analysis, which may explain the amount of relative model misfit (caused by a larger number of estimated parameters with only small effects, which did not contribute much to the overall model fit). Notably, the path of body awareness to anxiety had a positive sign, i.e., higher body awareness was associated with higher anxiety. Among experienced meditators, this path had a negative sign; also, all paths of SRA to the various aspects of emotion regulation had been positive (Tran et al. 2014). The model explained 40% of the variance of depression scores and 24% of the variance of anxiety scores. The total effect of the higher-order factors SRA and OTE on depression and anxiety amounted to .02 and − .41 (depression), and .08 and − .31 (anxiety) (all p’s < .001, except for the total effect of SRA on depression, p = .374). SRA led to a significant net increase of anxiety, mostly through its strong association with body awareness.
The exploratory stepwise approach led to the model in Fig. 2. This model fitted better to the data than the confirmatory model: χ2(25) = 83.80, p < .001, CFI = .987, TLI = .965, RMSEA = .046 [.035, .057]. Having tested all other candidate mechanisms for their incremental validity, the final model resulted in a set of mediators that was identical to that of the confirmatory model. Body awareness was kept in the model for heuristic purposes, even though its path to anxiety had a coefficient < .10 in value. Compared to the confirmatory model, SRA lost its paths to impulse control and access to emotion regulation strategies. Impulse control had paths only to anxiety and somatization, whereas emotional clarity only to somatization and depression. Access to emotion regulation strategies had a path only to depression. Nonattachment gained a connection to anxiety. Acceptance of emotions was the only mediator that had paths to all three mental health outcomes. The model explained 39% of the variance of depression scores, 24% of the variance of anxiety scores, and 13% of the variance of the somatization scores. The total effect of the higher-order factors SRA and OTE on depression, anxiety, and somatization amounted to − .02 and − .41 (depression), .03 and − .32 (anxiety), and − .001 and − .23 (somatization) (all p’s < .001, except for the total effects of SRA on depression, p = .128; on anxiety, p = .021; and on somatization, p = .935).

Exploratory path model of the associations of meditation experience with mindfulness, mechanisms of mindfulness, and depression, anxiety, and somatization. Numbers are standardized path coefficients. SRA = self-regulated attention; OTE = orientation to experience; ER = emotion regulation. SRA and OTE were allowed to correlate, as were the mechanisms, and depression, anxiety, and somatization. All p’s ≤ .003
Discussion
This study found that a mediational model, as previously obtained for experienced meditators (Tran et al. 2014), is equally applicable to the general population to explain the associations between trait mindfulness and mental health (Research Goal 1). However, exploratory analyses also suggested differences in the structure of this model which highlight differential associations of self-regulated attention with the mediating variables and mental health between experienced meditators and the general population. Replicating previous studies (Tran et al. 2013, 2014), we further obtained evidence of good factorial validity of a short form of the FFMQ and of a two-factor higher-order structure of this measure (Research Goal 2).
The results of the current study suggest—with regard to the investigated set of candidate mechanisms—that no differences exist between meditators and the general population in the variables and mechanisms that mediate the associations between mindfulness and mental health cross-sectionally. From all proposed mechanisms of action (Hölzel et al. 2011), emotion regulation appeared to be the most important, corroborating previous results (Freudenthaler et al. 2017; Tran et al. 2014). Extending previous results, we obtained evidence that impulse control and access to emotion regulation strategies might be differentially associated with symptoms of depression, and symptoms of anxiety and somatization. Assessing these two aspects of emotion regulation with a common scale, previous research among meditators was not able to detect this difference.
Acceptance of emotions was the only aspect of emotion regulation that had paths to all three investigated mental health outcomes. It thus appears to be of central importance for the links of mindfulness with mental health, which may also explain part of the apparent efficacy of acceptance and commitment therapy (ACT; Hayes et al. 1999) for a wide range of mental health problems (A-Tjak et al. 2015). Learning to accept, rather than control, painful feelings and sensations is one of the stated goals of ACT. Nonattachment was a major correlate of mindfulness in the current study and showed incremental validity in predicting symptoms of depression, corroborating previous findings among meditators (Tran et al. 2014). The observed similar association with anxiety appears to be a new finding in this context. Nonattachment bears resemblance to the concept and goals of cognitive defusion in ACT. Cognitive defusion aims at decreasing patients’ overidentification with their thoughts and treating them as fixed “truths.” It has been shown to contribute with a large effect size to the positive outcome of ACT (Levin et al. 2012). The authors of the NAS (the scale to measure this construct) built on a Buddhist background in constructing the scale. However, as can be derived from the results of the current study, but also from Sahdra et al. (2016), nonattachment apparently does not depend on such a background. It seems to be a more general construct whose links with cognitive defusion need to be investigated in more detail in the future.
Taken together, the broad structural similarities of the mediational network of mindfulness and mental health of experienced meditators and the current general population sample suggest that mechanisms of mindfulness are not specific to meditation and training. Reconciling the current finding with previous results (Tran et al. 2014), meditation experience apparently modifies the strength and direction of associations of self-regulated attention with mediators and outcomes, but may not introduce new mechanisms of action. As expected, associations of self-regulated attention with mediating variables and mental health were mostly smaller in the current general population sample than among experienced meditators. Consequently, the amount of attributable variance was smaller as well (40 [this study] vs. 59% [Tran et al. 2014] for depression scores, 24 vs. 57% for anxiety scores). Also, the correlation between the higher-order factors of mindfulness was lower in the current general population sample than among experienced meditators, replicating previous findings in the general population (Tran et al. 2013). Thus, meditation experience apparently leads to a more homogeneous construct of psychometric mindfulness.
Future longitudinal and intervention studies should specifically target mechanisms pertaining to emotion regulation (see also Roemer et al. 2015), body awareness, and change of self (nonattachment) to investigate their probable causal role with regard to the effects of mindfulness on mental health. Previous longitudinal research showed that rumination mediates the effects of mindfulness on depressive symptoms (Petrocchi and Ottaviani 2016; Royuela-Colomer and Calvete 2016). Longitudinal studies on further aspects of emotion regulation, as suggested in the current study and elsewhere (e.g., Curtiss et al. 2017), and of nonattachment are needed. The observed specificity of impulse control and access to emotion regulation strategies for symptoms of anxiety, depression, and somatization also needs further study.
Body awareness was reported to mediate the effects of yoga practice on psychological well-being in a cross-sectional study (Tihanyi et al. 2016). Yet, as suggested by the current results, body awareness does not appear to be specific to the context of intervention and training. On the biological level, mindfulness training increases the activity of prefrontal regulatory regions which inhibit central stress processing regions (e.g., the amygdala), and reduces and modulates the reactivity of these regions (Creswell and Lindsay 2014; for meta-analytic evidence of the effects of mindfulness on physiological markers of stress, see Pascoe et al. 2017). Traditional Buddhist meditation typically starts with an initial training of attention regulation, often focusing on localized bodily sensations (e.g., respiration), before proceeding to a more general stage where awareness does not depend on the conscious selection and deselection of the attentional focus and which finally may result in psychological well-being (Hölzel et al. 2011; Lutz et al. 2008). The current data suggest that a bodily focus might pose a privileged starting point for this process, as even among the mostly meditation-naïve individuals of the current study, a connection between bodily awareness with self-regulated attention and mental health (anxiety) was apparent. However, without monitoring and training, this pathway may contribute to heightened symptom levels, as also was apparent in the current data.
Summing up, we obtained evidence that the mediational network that links mindfulness with mental health in the general population is broadly similar to the mediational network among experienced meditators. Differences pertained to the strength and direction of associations of self-regulated attention with the other variables in this network. Emotion regulation, body awareness, and change of self (nonattachment) appeared to be the most important mechanisms of action through which mindfulness exerts its beneficial effects on mental health. These mechanisms should be specifically targeted in longitudinal and intervention studies to examine their probable causal role. The utilized short form of the FFMQ can be recommended for further research for its good factorial validity. Mindfulness was replicably shown to have a two-factor higher-order structure with this measure in the general population.
Limitations
The cross-sectional design of this study precludes any causal interpretation of the presented results. Longitudinal studies are needed to investigate the possible causal role of investigated mediators for the effects of mindfulness on mental health. We used the FFMQ as a measure of trait mindfulness, but did neither investigate, nor intended to do so, the probable state and trait components of this popular measure (cf. Medvedev et al. 2017). State and trait components of mindfulness may be differentially associated with the investigated mediators and mental health outcomes. Our operationalization of meditation experience encompassed different styles of meditation. We were interested in controlling for prior meditation experience, but not to account for possible differences between various meditation styles. These may well differ regarding the extent to which they contribute to mindfulness. We utilized a variable-oriented approach to analysis in the attempt to replicate in the general population results that have previously been reported among meditators with the same methods. Person-centered approaches (e.g., latent profile analysis; see Pearson et al. 2015; Sahdra et al. 2017) may provide further insight into differences between meditators and the general population, or even within the general population itself. Also, facet-level analyses might reveal differences not similarly observable on the level of the higher-order factors. Lastly, the reported results are based on self-reports throughout, and thus potentially are prone to common-method variance effects.
References
Agee, J. D., Danoff-Burg, S., & Grant, C. A. (2009). Comparing brief stress management courses in a community sample: mindfulness skills and progressive muscle relaxation. Explore, 5, 104–109. https://doi.org/10.1016/j.explore.2008.12.004.
Asparouhov, T., & Muthén, B. (2009). Exploratory structural equation modeling. Structural Equation Modeling, 16, 397–438. https://doi.org/10.1080/10705510903008204.
A-Tjak, J. G. L., Davis, M. L., Morina, N., Powers, M. B., Smits, J. A. J., & Emmelkamp, P. M. G. (2015). A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental health and physical health problems. Psychotherapy and Psychosomatics, 84, 30–36.
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13, 27–45. https://doi.org/10.1177/1073191105283504.
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., Walsh, E., Duggan, D., & Williams, J. M. G. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment, 15, 329–342. https://doi.org/10.1177/1073191107313003.
Behling, O., & Law, K. S. (2000). Translating questionnaires and other research instruments: problems and solutions. Thousand Oaks: Sage.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., & Devins, G. (2004). Mindfulness: a proposed operational definition. Clinical Psychology: Science and Practice, 11, 230–241. https://doi.org/10.1093/clipsy.bph077.
Bohlmeijer, E., Prenger, R., Taal, E., & Cuijpers, P. (2010). The effects of mindfulness-based stress reduction therapy on mental health of adults with a chronic medical disease: a meta-analysis. Journal of Psychosomatic Research, 68, 539–544. https://doi.org/10.1016/j.jpsychores.2009.10.005.
Bohlmeijer, E., ten Klooster, P. M., Fledderus, M., Veehof, M., & Baer, R. (2011). Psychometric properties of the Five Facet Mindfulness Questionnaire in depressed adults and development of a short form. Assessment, 18, 308–320. https://doi.org/10.1177/1073191111408231.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84, 822–848. https://doi.org/10.1037/0022-3514.84.4.822.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale: Erlbaum.
Creswell, J. D., & Lindsay, E. K. (2014). How does mindfulness training affect health? A mindfulness stress buffering account. Current Directions in Psychological Science, 23, 401–407. https://doi.org/10.1177/0963721414547415.
Curtiss, J., Klemanski, D. H., Andrews, L., Ito, M., & Hofmann, S. G. (2017). The conditional process model of mindfulness and emotion regulation: an empirical test. Journal of Affective Disorders, 212, 93–100.
Ehring, T., Fischer, S., Schnülle, J., Bösterling, A., & Tuschen-Caffier, B. (2008). Characteristics of emotion regulation in recovered depressed versus never depressed individuals. Personality and Individual Differences, 44, 1574–1584. https://doi.org/10.1016/j.paid.2008.01.013.
Evans, D. E., & Rothbart, M. K. (2007). Developing a model for adult temperament. Journal of Research in Personality, 41, 868–888. https://doi.org/10.1016/j.jrp.2006.11.002.
Fresco, D. M., Moore, M. T., van Dulmen, M. H. M., Segal, Z. V., Ma, S. H., Teasdale, J. D., & Williams, G. (2007). Initial psychometric properties of the experiences questionnaire: validation of a self-report measure of decentering. Behavior Therapy, 38, 234–246. https://doi.org/10.1016/j.beth.2006.08.003.
Freudenthaler, L., Turba, J. D., & Tran, U. S. (2017). Emotion regulation mediates the associations of mindfulness on symptoms of depression and anxiety in the general population. Mindfulness, 8, 1339–1344.
Gecht, J., Kessel, R., Mainz, V., Gauggel, S., Drueke, B., & Scherer, A. (2013). Measuring decentering in self-reports: psychometric properties of the Experiences Questionnaire in a German sample. Psychotherapy Research, 24, 67–79. https://doi.org/10.1080/10503307.2013.821635.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment, 26, 41–54.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: a meta-analysis. Journal of Psychosomatic Research, 57, 35–43. https://doi.org/10.1016/S0022-3999(03)00573-7.
Gu, J., Strauss, C., Bond, R., & Cavanagh, K. (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of meditation studies. Clinical Psychology Review, 37, 1–12. https://doi.org/10.1016/j.cpr.2015.01.006.
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (1999). Acceptance and commitment therapy: an experiential approach to behavior change. New York: Guilford Press.
Hölzel, B. K., Lazar, S. W., Gard, T., Schuman-Olivier, Z., Vago, D. R., & Ott, U. (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6, 537–559. https://doi.org/10.1177/1745691611419671.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. https://doi.org/10.1080/10705519909540118.
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., et al. (2013). Mindfulness-based therapy: a comprehensive meta-analysis. Clinical Psychology Review, 33, 763–771. https://doi.org/10.1016/j.cpr.2013.05.005.
Kraemer, H. C., Kazdin, A. E., Offord, D. R., Kessler, R. C., Jensen, P. S., & Kupfer, D. J. (1997). Coming to terms with the terms of risk. Archives of General Psychiatry, 54, 337–343. https://doi.org/10.1001/archpsyc.1997.01830160065009.
Kraemer, H. C., Wilson, G. T., Fairburn, C. G., & Agras, W. S. (2002). Mediators and moderators of treatment effects in randomized clinical trials. Archives of General Psychiatry, 59, 877–883. https://doi.org/10.1001/archpsyc.59.10.877.
Kroenke, K. (2003). Patients presenting with somatic complaints: epidemiology, psychiatric comorbidity and management. International Journal of Methods in Psychiatric Research, 12, 34–43. https://doi.org/10.1002/mpr.140.
Langer, Á. I., Ulloa, V. G., Cangas, A. J., Rojas, G., & Krause, M. (2015). Mindfulness-based interventions in secondary education: a qualitative systematic review. Estudios de Psicología, 36, 533–570. https://doi.org/10.1080/02109395.2015.1078553.
Levin, M. E., Hildebrandt, M. J., Lillis, J., & Hayes, S. C. (2012). The impact of treatment components suggested by the psychological flexibility model: a meta-analysis of laboratory-based component studies. Behavior Therapy, 43, 741–756.
Lutz, A., Slagter, H. A., Dunne, J. D., & Davidson, R. J. (2008). Attention regulation and monitoring in meditation. Trends in Cognitive Sciences, 12, 163–169. https://doi.org/10.1016/j.tics.2008.01.005.
Medvedev, O. N., Krägeloh, C. U., Narayanan, A., & Siegert, R. J. (2017). Measuring mindfulness: applying generalizability theory to distinguish between state and trait. Mindfulness, 8, 1036–1046.
Muthén, L. K., & Muthén, B. O. (2008). Mplus user’s guide. Los Angeles: Muthén & Muthén.
Pascoe, M. C., Thompson, D. R., Jenkins, Z. M., & Ski, C. F. (2017). Mindfulness mediates the physiological markers of stress: systematic review and meta-analysis. Journal of Psychiatric Research, 95, 156–178.
Pearson, M. R., Lawless, A. K., Brown, D. B., & Bravo, A. J. (2015). Mindfulness and emotional outcomes: identifying subgroups of college students using latent profile analysis. Personality and Individual Differences, 76, 33–38.
Petrocchi, N., & Ottaviani, C. (2016). Mindfulness facets distinctively predict depressive symptoms after two years: the mediating role of rumination. Personality and Individual Differences, 93, 92–96.
Price, C. J., & Thompson, E. A. (2007). Measuring dimensions of body connection: body awareness and bodily dissociation. Journal of Alternative and Complementary Medicine, 13, 945–953. https://doi.org/10.1089/acm.2007.0537.
Ravalier, J. M.,Wegrzynek, P., & Lawton, S. (2016). Systematic review: Complementary therapies and employee well-being. Occupational Medicine, 66, 428-436. https://doi.org/10.1093/occmed/kqw047.
Roemer, L., Williston, S. K., & Rollins, L. G. (2015). Mindfulness and emotion regulation. Current Opinion in Psychology, 3, 52–57.
Royuela-Colomer, E., & Calvete, E. (2016). Mindfulness facets and depression in adolescents: rumination as a mediator. Mindfulness, 7, 1092–1102.
Sahdra, B. K., Shaver, P. R., & Brown, K. W. (2010). A scale to measure nonattachment: a Buddhist complement to Western research on attachment and adaptive functioning. Journal of Personality Assessement, 92, 116–127. https://doi.org/10.1080/00223890903425960.
Sahdra, B. K., Ciarrochi, J., & Parker, P. D. (2016). Nonattachment and mindfulness: related but distinct constructs. Psychological Assessment, 28, 819–829.
Sahdra, B. K., Ciarrochi, J., Parker, P. D., Basarkod, G., Bradshaw, E. L., & Baer, R. (2017). Are people mindful in different ways? Disentangling the quantity and quality of mindfulness in latent profiles, and their links to mental health and life effectiveness. European Journal of Personality, 31, 347–365.
Spitzer, C., Hammer, S., Löwe, B., Grabe, H. J., Barnow, S., Rose, M., … Franke, G. H. (2011). The short version of the brief symptom inventory (BSI-18): preliminary psychometric properties of the German translation. Fortschritte der Neurologie und Psychiatrie, 79, 517–523. doi https://doi.org/10.1055/s-0031-1281602.
Szekeres, R. A., & Wertheim, E. H. (2015). Evaluation of Vipassana meditation course effects on subjective stress, well-being, self-kindness and mindfulness in a community sample: post-course and 6-month outcomes. Stress and Health, 31, 373–381. https://doi.org/10.1002/smi.2562.
Taylor, N. Z., & Millear, P. M. R. (2016). Validity of the Five Facet Mindfulness Questionnaire in an Australian, meditating, demographically diverse sample. Personality and Individual Differences, 90, 73–77. https://doi.org/10.1016/j.paid.2015.10.041.
Teasdale, J. D., Moore, R. G., Hayhurst, H., Pope, M., Williams, S., & Segal, Z. V. (2002). Metacognitive awareness and prevention of relapse in depression: empirical evidence. Journal of Consulting and Clinical Psychology, 70, 275–287. https://doi.org/10.1037/0022-006X.70.2.275.
Tihanyi, B. T., Boor, P., Emanuelsen, L., & Koteles, F. (2016). Mediators between yoga practice and psychological well-being: mindfulness, body awareness and satisfaction with body image. European Journal of Mental Health, 11, 112–127.
Tran, U. S., Glück, T. M., & Nader, I. W. (2013). Investigating the Five Facet Mindfulness Questionnaire (FFMQ): construction of a short form and evidence of a two-factor higher order structure of mindfulness. Journal of Clinical Psychology, 69, 951–965. https://doi.org/10.1002/jclp.21996.
Tran, U. S., Cebolla, A., Glück, T. M., Soler, J., Garcia-Campayo, J., & von Moy, T. (2014). The serenity of the meditating mind: a cross-cultural psychometric study on a two-factor higher order structure of mindfulness, its effects, and mechanisms related to mental health among experienced meditators. PLoS One, 9, e110192. https://doi.org/10.1371/journal.pone.0110192.
Vago, D. R., & Silbersweig, D. A. (2012). Self-awareness, self-regulation, and self-transcendence (S-ART): a framework for understanding the neurobiological mechanisms of mindfulness. Frontiers in Human Neuroscience, 6, 296. https://doi.org/10.3389/fnhum.2012.00296.
Van der Velden, A. M., & Roepstorff, A. (2015). Neural mechanisms of mindfulness meditation: bridging clinical and neuroscience investigations. Nature Reviews Neuroscience, 16, 439. https://doi.org/10.1038/nrn3916-c1.
Wiltink, J., Vogelsang, U., & Beutel, M.E. (2006). Temperament and personality: the German version of the Adult Temperament Questionnaire (ATQ). GMS Psycho-Social-Medicine, 3, Doc10. Retrieved from http://www.egms.de/de/journals/psm/2006-3/psm000030.shtml.
Funding
Open access funding provided by University of Vienna.
Author information
Authors and Affiliations
Contributions
MAB participated in the data analysis, wrote the first draft of the manuscript, and participated in the editing of the final manuscript. MV participated in the editing of the final manuscript. MH participated in the data analysis and in the editing of the final manuscript. UST designed the study, supervised the execution of the study, and participated in the data analysis and in the writing of the final manuscript. All authors approved the final version of the manuscript for submission.
Corresponding author
Ethics declarations
All procedures performed in this study adhere to the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards, and with institutional guidelines of the School of Psychology, University of Vienna. Study participation did not affect the physical or psychological integrity, the right for privacy, or other personal rights or interests of the participants. Such being the case, according to national laws (Austrian Universities Act 2002), this study was exempt from formal ethical approval.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Electronic Supplementary Material
ESM 1
(PDF 138 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Burzler, M.A., Voracek, M., Hos, M. et al. Mechanisms of Mindfulness in the General Population. Mindfulness 10, 469–480 (2019). https://doi.org/10.1007/s12671-018-0988-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-018-0988-y