
Abstract
Purpose
We sought to perform a systematic review and meta-analysis to determine whether indirect laryngoscopy has an advantage over direct laryngoscopy in terms of the tracheal intubation rate, glottic visualization, and intubation time when used by novice operators.
Methods
We extracted adult prospective randomized trials comparing tracheal intubation with indirect vs direct laryngoscopy in novice operators from electronic databases. We extracted the following data from the identified studies: success rate, glottic visualization, and intubation time. Data from each trial were combined via a random-effects model to calculate the pooled relative risk (RR) or weighted mean difference (WMD) with a 95% confidence interval (CI). We also performed a trial sequential analysis.
Results
We included 15 articles (17 trials) comprising 2,290 patients in the systematic review. Compared with the direct laryngoscopy, indirect laryngoscopy improved success rate (RR, 1.15; 95% CI, 1.07 to 1.24; P = 0.0002; I2 = 88%), glottic visualization (RR, 1.76; 95% CI, 1.36 to 2.28; P < 0.001; I2 = 85%), and intubation time (WMD, −9.06 sec; 95% CI, −16.4 to −1.76; P = 0.01; I2 = 98%) in tracheal intubation. Trial sequential analysis showed that the total sample size was sufficient to analyze the success rate and intubation time.
Conclusion
In this systematic review, we found that the tracheal intubation success rate, glottic visualization, and intubation time were improved when novice operators used indirect laryngoscopy rather than direct laryngoscopy. Trial sequential analysis results indicated that the sample size was sufficient for examining the success rate and intubation time.
Study registration
PROSPERO (CRD42022309045); first registered 4 September 2022.
Résumé
Objectif
Nous avons cherché à réaliser une revue systématique et une méta-analyse pour déterminer si la laryngoscopie indirecte présente un avantage par rapport à la laryngoscopie directe en termes de taux de succès d’intubation trachéale, de visualisation glottique et de temps d’intubation lorsqu’elle est utilisée par des opératrices et opérateurs novices.
Méthode
Nous avons extrait des études randomisées prospectives chez l’adulte comparant l’intubation trachéale avec une laryngoscopie indirecte vs directe réalisée par des opérateurs et opératrices novices à partir de bases de données électroniques. Nous avons extrait les données suivantes des études identifiées : taux de succès, visualisation glottique et temps d’intubation. Les données de chaque étude ont été combinées au moyen d’un modèle à effets aléatoires pour le calcul du risque relatif (RR) groupé ou de la différence moyenne pondérée (DMP) avec un intervalle de confiance (IC) de 95 %. Nous avons également réalisé une analyse séquentielle des études.
Résultats
Nous avons inclus 15 articles (17 études) portant sur 2290 patient·es dans notre revue systématique. Par rapport à la laryngoscopie directe, la laryngoscopie indirecte a amélioré le taux de succès (RR, 1,15; IC 95 %, 1,07 à 1,24; P = 0,0002; I2 = 88 %), la visualisation glottique (RR, 1,76; IC 95 %, 1,36 à 2,28; P < 0,001; I2 = 85 %), et le temps d’intubation (DMP, −9,06 s; IC 95 %, −16,4 à −1,76; P = 0,01; I2 = 98 %) pour l’intubation trachéale. L’analyse séquentielle des études a montré que la taille totale de l’échantillon était suffisante pour analyser le taux de succès et le temps d’intubation.
Conclusion
Dans cette revue systématique, nous avons constaté que le taux de succès de l’intubation trachéale, la visualisation glottique et le temps d’intubation étaient améliorés lorsque les opératrices et opérateurs novices utilisaient la laryngoscopie indirecte plutôt que la laryngoscopie directe. L’analyse séquentielle des études a montré que la taille totale de l’échantillon était suffisante pour analyser le taux de succès et le temps d’intubation.
Enregistrement de l’étude
PROSPERO (CRD42022309045); première inscription le 4 septembre 2022.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Indirect laryngoscopes, including videolaryngoscopes, are widely used for tracheal intubation in the clinical setting. They have a number of advantages for tracheal intubation in that they can be used successfully without needing to align the laryngeal, pharyngeal, and oral axes,1,2 and the optical camera attached to the tip of the scope enables more accurate tracheal intubation by visualizing the glottis from a short distance.3,4 Indeed, indirect laryngoscopy is reported to be superior to conventional direct laryngoscopy for tracheal intubation.5,6
Previous meta-analyses have shown that indirect laryngoscopes are also useful in patients in whom intubation is difficult, such as those requiring manual in-line stabilization7,8 and those with severe obesity.9 In addition, indirect laryngoscopes are considered useful for tracheal intubation by novice operators. Studies in mannequins have shown that the intubation rate is higher and intubation time is shorter when novices use an indirect laryngoscope rather than a direct laryngoscope.10,11 Nevertheless, an indirect laryngoscope may not be able to successfully guide the tracheal tube to the glottis, even if the glottis can be visualized,12 and the video images do not visualize the pharynx and hypopharynx, which can lead to visual and cognitive blind spots.13,14 These disadvantages suggest that indirect laryngoscopes may not always be effective in the hands of novice operators. Moreover, clinical studies in humans have not been able to determine whether indirect laryngoscopy is advantageous for tracheal intubation in inexperienced hands.15,16,17
We sought to undertake this systematic review and meta-analysis to determine whether indirect laryngoscopy has an advantage over direct laryngoscopy in terms of the tracheal intubation rate, glottic visualization, and intubation time when used by novice operators. We also aimed to compared the frequency of adverse events, including esophageal intubation, oropharyngeal injury, and desaturation, between indirect laryngoscopes and direct laryngoscopes.
Methods
The manuscript was prepared following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.18 The study protocol was registered at PROSPERO (registration number, CRD42022309045; registered 4 September 2022).
Search strategy
We conducted a comprehensive literature search using the PubMed, Embase, and Cochrane Central Register of Controlled Trials databases. The search strategy used is shown in Electronic Supplementary Material (ESM) eAppendix 1. We also manually searched the reference lists in the reports and reviews extracted to identify further potentially eligible articles. No restrictions were imposed on article type or language of the publication. The search was performed in October 2022.
Selection of included studies
Articles were extracted by each of the authors working independently and assessed for suitability for inclusion in the systematic review. Disagreements regarding interpretation or analysis of the data in the extracted articles were resolved through discussion. In the event of duplicate reporting, only the report that analyzed the most recent data were included. If necessary, the authors of potentially eligible articles were contacted directly to obtain missing data and resolve any inconsistencies. For each included study, we searched online to confirm if the research protocol had been published, and if so, whether its content matched the results subsequently reported. A risk of bias was recorded if the study protocol had not been published.
Studies were eligible for inclusion if they had a prospective randomized design and compared the outcomes of tracheal intubation for adult patients by novice operators using an indirect laryngoscope or a direct laryngoscope. Information on success rate (first attempt), glottic visualization (Cormack–Lehane classification 1 vs ≥ 2), and intubation time was extracted from the eligible articles. The definition of failure of tracheal intubation was recorded for each study. Adverse events during tracheal intubation were also compared between the two types of laryngoscopes.
The research question was framed using the Population, Intervention, Comparison, Outcomes framework as follows: population = patients requiring oral tracheal intubation when undergoing surgery under general anesthesia; intervention = tracheal intubation with an indirect laryngoscope attempted by a novice operator; comparison = tracheal intubation with a direct laryngoscope attempted by a novice operator; and outcomes = tracheal intubation success rate, glottic visualization, and intubation time.
Studies with mannequins; studies in which tracheal intubation was performed during cardiopulmonary resuscitation or nasal intubation, and in pediatric patients; and studies that used double-lumen tubes were excluded. We also divided the indirect laryngoscopy groups and direct laryngoscopy groups into subgroups to compare outcomes according to whether or not a tracheal tube guide was used.
Critical appraisal of study quality
Risk of bias and quality of evidence
We evaluated the risk of bias with reference to the Cochrane Handbook19 (ESM eAppendix 2). The quality of evidence for the main outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation approach20 (ESM eAppendix 3).
Data synthesis and analysis
Statistical analysis was performed using the DerSimonian and Laird random effects model. Binary variable pool effect estimates (success rate, glottic visualization, and adverse events) are expressed as the relative risk (RR) with 95% confidence interval (CI). The pooled difference in intubation time between the indirect and direct laryngoscope groups is expressed as the weighted mean difference (WMD) of the 95% CI. The heterogeneity of effect size was examined using the Cochran Q test and the I2 statistic.21
We also performed a trial sequential analysis (TSA) to assess sensitivity to prevent type I error arising from multiple tests of effect in the meta-analysis.22,23 First, we calculated the required sample size (required information size [RIS]) and set the risk of type I error to 5% and the risk of type II error to 10%. We set the minimum clinically meaningful risk ratio in TSA to 1.33 and the mean difference to ten seconds. Trial Sequential Analysis version 0.9.5.5 beta (Copenhagen Trial Unit, Centre for Clinical Intervention Research, Copenhagen, Denmark) was used for this analysis.
Publication bias was assessed by testing the symmetry of a funnel plot24 and by Begg’s test.25 A P value of < 0.1 from this test indicated publication bias.
Results
Characteristics of included studies
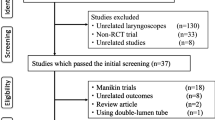
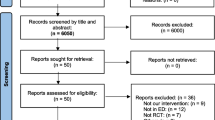
The literature search identified 332 potentially relevant articles. Eighty-six studies were immediately identified to be unrelated and excluded. The remaining 246 articles were carefully read to determine whether they met our eligibility criteria. A further 226 studies were excluded for the following reasons: trial performed in mannequins (n = 88); not a randomized controlled trial (n = 51); laryngeal mask airway used (n = 27); a review article (n = 15); a cardiopulmonary resuscitation trial (n = 14); indirect laryngoscope not used (n = 13); not involving novice operators (n = 9); other reason (n = 8); involving pediatric patients (n = 4); and nasal intubation used (n = 2). The remaining 15 articles (17 trials) met our inclusion criterion and contained the data necessary for comparison (Fig. 1). These 15 articles are summarized in Table 1.2,15,16,17,26,27,28,29,30,31,32,33,34,35,36,37

Systematic review and meta-analysis flow chart
RCT = randomized controlled trial
The included studies were published between 2009 and 2018. The most common indirect laryngoscope used was the Airtraq™ (Mercury Medical®, Clearwater, FL, USA; six trials), followed by the GlideScope® (Verathon Inc., Bothell, WA, USA; four trials), the McGRATH™ (Medtronic PLC, Dublin, Ireland; three trials), the Pentax Airway Scope (Nihon Kohden Corp., Tokyo, Japan; two trials), the C-MAC® (Karl Storz SE & Co. KG, Tuttlingen, Germany; one trial), and the Truview EVO2 (Leica Geosystems AG, Heerbrugg, Switzerland; one trial). The definition of a novice operator was a resident in ten trials and a medical student in the remaining five trials. The preoperative condition of the airway was reported to be normal in all but one trial. All direct laryngoscopes used were Macintosh laryngoscopes (Table 1).
Meta-analysis results
In total, 1,169 patients were intubated using an indirect laryngoscope and 1,121 using a direct laryngoscope.
Intubation performance
In the 17 trials, the tracheal intubation success rate was significantly higher with an indirect laryngoscope than with a direct laryngoscope (RR, 1.15; 95% CI, 1.07 to 1.24; P = 0.0002; Cochrane’s Q = 134.2; I2 = 88%; Fig. 2). Absolute risk reduction was 17.7% (indirect laryngoscopy, 89.1% vs direct laryngoscopy, 71.9%). For success rate, our TSA revealed that the Z-curve crossed the efficacy boundary, although the RIS was not reached (ESM eFig. 4).

Forest plot of the success rate of tracheal intubation using indirect laryngoscopy versus direct laryngoscopy
Glottic visualization was evaluated in nine trials and was better when an indirect laryngoscope was used (RR, 1.76; 95% CI, 1.36 to 2.28; P < 0.001; Cochrane’s Q = 45.5; I2 = 85%; Fig. 3). Absolute risk reduction was 36.6% (indirect laryngoscope 83.3% vs direct laryngoscope 47.6%). The Z curve did not reach the TSA monitoring boundary for benefit, and the accrued sample size (n = 984) was 22.7% of the required sample size (n = 4,328) (ESM eFig. 5).

Forest plot of glottic visualization with indirect laryngoscopy versus direct laryngoscopy (Cormack–Lehane grade 1 and 2 vs other grades)
Intubation time was significantly shorter with an indirect laryngoscope than with a direct laryngoscope (WMD, −9.06 sec; 95% CI, −16.4 to −1.76; P = 0.02; Cochrane’s Q = 508.3; I2 = 98%; Fig. 4). The Z curve crossed the futility boundary. Trial sequential analysis revealed that the accrued information size (n = 1,990) was 76.5% of the estimated RIS (n = 2,600) (ESM eFig. 6).

Forest plot of intubation time for tracheal intubation using indirect laryngoscopy versus direct laryngoscopy
Subgroup analysis
In addition, the indirect and direct laryngoscopy groups were classified and analyzed according to whether a tracheal tube guide was used. The subgroup analysis according to whether or not a tracheal tube guide was used found that successful intubation and glottic visualization rates were significantly better with both indirect laryngoscopes than with a direct laryngoscope (with tracheal tube guide, success rate: RR, 1.24; 95% CI, 1.06 to 1.44; P < 0.006; Cochrane’s Q = 68.7, I2 = 90%; glottic visualization: RR, 2.38; 95% CI, 1.59 to 3.57; P < 0.001; Cochrane’s Q = 14.7; I2 = 80%, without tracheal tube guide, success rate: RR, 1.11; 95% CI, 1.01 to 1.23; P = 0.03; Cochrane’s Q = 61.5, I2 = 88%; glottic visualization: RR, 1.76; 95% CI, 1.36 to 2.28; P < 0.001; Cochrane’s Q = 45.5; I2 = 85%) (Figs 2 and 3). Nevertheless, intubation time using an indirect laryngoscope with or without a tracheal tube guide was comparable to that using a direct laryngoscope (Fig. 4).
Adverse events
Adverse events during tracheal intubation were compared according to whether an indirect laryngoscope or direct laryngoscope was used. The incidence of all adverse events during tracheal intubation was significantly lower with an indirect laryngoscope (esophageal intubation: RR, 0.16; 95% CI, 0.04 to 0.61; P = 0.007; Cochrane’s Q = 2.18; I2 = 8%; oropharyngeal injury: RR, 0.42; 95% CI, 0.23 to 0.76; P = 0.004; Cochrane’s Q = 2.50; I2 = 0.0%; oxygen desaturation; RR, 0.51; 95% CI, 0.27 to 0.97; P = 0.04; Cochrane’s Q = 0.08; I2 = 0.0%; Table 2).
Quality of evidence
The quality of evidence for success rate, glottic visualization, and intubation time according to type of laryngoscope used by a novice operator was graded as “very low.” All of the included studies were found to have a moderate risk of bias because the operator could not be blinded to the type of laryngoscope used. Heterogeneity was high for all parameters, and there was publication bias in terms of the success rate and glottic visualization rate. Accordingly, the quality of evidence was downgraded to “very low” (Fig. 5).

The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach
Results of publication bias
The Begg’s test identified publication bias for success rate (Kendall’s statistic = 50.0; Z = 1.85; P = 0.02) and glottic visualization (Kendall’s statistic = 20.0; Z = 2.09; P = 0.06). No publication bias was found for intubation time (Kendall’s statistic = −12.0; Z = 0.59; P = 0.4). Figure 6 summarizes the risks of bias.

Green circles, red circles, and yellow circles indicate “low risk of bias,” “high risk of bias,” and “unclear risk of bias,” respectively
Discussion
This systematic review and meta-analysis found that tracheal intubation success rate, glottic visualization, and intubation time were improved when a novice operator used an indirect laryngoscope rather than a direct laryngoscope. Use of an indirect laryngoscope by a novice also reduced the risk of adverse events, including esophageal intubation, oropharyngeal injury, and desaturation.
In general, direct laryngoscopy enables tracheal intubation by aligning the oral, pharyngeal, and laryngeal axes.1,2 Nevertheless, indirect laryngoscopy can visualize the glottis without aligning them. Furthermore, use of an indirect laryngoscope allows the glottis to be confirmed in closer proximity by displaying the image obtained by the camera attached to the tip of the laryngoscope blade on an external monitor.3,4 These advantageous features of indirect laryngoscopes are considered to make tracheal intubation easier, thereby contributing to successful tracheal intubation by novice operators.27,38,39
Another advantage of using indirect laryngoscopes for novice operators is that information on the condition of the upper respiratory tract and the area near the glottis can be shared with supervisors during tracheal intubation.27,38,39 By sharing these images, the novice operator can receive appropriate advice and is thus more likely perform tracheal intubation successfully.
Novice operators can also learn to perform tracheal intubation more quickly using an indirect laryngoscope. Previous studies have also shown that the learning curve is less steep for an indirect laryngoscope than for a direct laryngoscope.15,31,40,41 Most of the randomized controlled trials included in the present systematic review and meta-analysis incorporated practicing tracheal intubation using both indirect and direct laryngoscopes on mannequins before use in patients. It may be easier for novices to master tracheal intubation with fewer preclinical exercises when using an indirect laryngoscope.
The subgroup analysis showed that the success rate and glottis visualization were significantly better for both indirect laryngoscopes regardless of whether a tracheal tube guide was used, compared with direct laryngoscope. Furthermore, intubation time was not significantly different between indirect and direct laryngoscopes, regardless of whether a tracheal tube guide was used. This finding suggests that tracheal intubation can be performed successfully using an indirect laryngoscope with or without a tracheal tube guide. Nevertheless, intubation time also varies depending on whether an intubation aid such as a stylet or gum-elastic bougie was used during tracheal intubation.42 In this systematic review and meta-analysis, we were unable to investigate the use of intubation aids, so we were unable to remove these biases. Further studies are warranted, as each study defined intubation time differently and the sample size was insufficient for analysis.
The incidence of adverse events was significantly lower when an indirect laryngoscope was used. The main reason for the reduced incidence of esophageal intubation with an indirect laryngoscope is that novice operators can share accurate information with their supervisor on a video screen and receive better guidance.27,38,39
A previous study found a higher incidence of adverse events, including soft tissue bleeding, oropharyngeal injury, and dental trauma, when video laryngoscopes were used.13 Indirect laryngoscopes create visual and cognitive blind spots that can increase the risk of oropharyngeal injury.14 Nevertheless, in our meta-analysis, the incidence of oropharyngeal injury was significantly lower when an indirect laryngoscope was used. Use of an indirect laryngoscope achieved successful tracheal intubation even if the pharyngeal lifting force of the laryngeal deployment was low.43,44 This low pharyngeal lifting force helps to protect against oropharyngeal injury. Also, indirect laryngoscope blades made of polyethylene are softer and less sharp than a stainless steel blade of an direct laryngoscope. This indirect laryngoscope blade configuration also helps to reduce incidence of oropharyngeal injury. When intubated without a stylet with a videolaryngoscope and an angled blade (GlideScope, McGRATH, C-MAC), it may be difficult to pass the tube through the vocal cords despite a good glottic view.42 On the other hand, the use of stylets contributes to oropharyngeal injury. This systematic review did not include studies that described the use of stylets, so we were unable to establish a clear relationship between stylet use and oropharyngeal injury. The shorter intubation time associated with use of an indirect laryngoscope may also decrease the risk of desaturation.
The results of our study show that indirect laryngoscopes are useful for tracheal intubation in novice operators. This result suggests the possibility of making tracheal intubation safer for residents and nonexperienced anesthesiologists, as well as making tracheal intubation safer for novice operators outside of operating rooms such as hospital wards and emergency departments.
Limitations
This systematic review and meta-analysis has several limitations. First, the type of laryngoscope used could not be blinded, which increased the risk of bias. Second, moderate to high heterogeneity was found in our results, which affected the study quality; however, subgroup analyses were performed. Third, the definition of a novice operator was not consistent between the included trials. Most operators were residents, but were medical students in four trials. Fourth, RIS was not reached for some results in the TSA analysis. Therefore, analysis of the glottis visualization was underpowered. Also, a separate per geometry analysis of individual indirect laryngoscopes was not possible, and detailed data on the preoperative airway status of individual patients were not available. Furthermore, patient age and height, anesthesia method, and definition of intubation time varied across the trials, and these differences also affected the study quality.
Conclusion
In this systematic review and meta-analysis, we found that the tracheal intubation success rate, glottic visualization, and intubation time were improved when novice operators used an indirect laryngoscope rather than a direct laryngoscope. Moreover, the risk of adverse events, including esophageal intubation, oropharyngeal injury, and desaturation, was lower when novices used an indirect laryngoscope. Trial sequential analysis indicated that the sample size was sufficient for examining the success rate and intubation time.
References
Maharaj CH, Costello JF, McDonnell JG, Harte BH, Laffey JG. The Airtraq as a rescue airway device following failed direct laryngoscopy: a case series. Anaesthesia 2007; 62: 598–601. https://doi.org/10.1111/j.1365-2044.2007.05036.x
Hirabayashi Y, Seo N. Tracheal intubation by non-anesthesia residents using the Pentax-AWS airway scope and Macintosh laryngoscope. J Clin Anesth 2009; 21: 268-71. https://doi.org/10.1016/j.jclinane.2008.08.024
Kaplan MB, Ward DS, Berci G. A new video laryngoscope—an aid to intubation and teaching. J Clin Anesth 2002; 14: 620–6. https://doi.org/10.1016/s0952-8180(02)00457-9
Kaplan MB, Hagberg CA, Ward DS, et al. Comparison of direct and video-assisted views of the larynx during routine intubation. J Clin Anesth 2006; 18: 357–62. https://doi.org/10.1016/j.jclinane.2006.01.002
Hoshijima H, Mihara T, Denawa Y, et al. Airtraq® is superior to the Macintosh laryngoscope for tracheal intubation: systematic review with trial sequential analysis. Am J Emerg Med 2019; 37: 1367–8. https://doi.org/10.1016/j.ajem.2018.12.018
Hoshijima H, Mihara T, Maruyama K, et al. C-MAC® videolaryngoscope versus Macintosh laryngoscope for tracheal intubation: a systematic review and meta-analysis with trial sequential analysis. J Clin Anesth 2018; 49: 53–62. https://doi.org/10.1016/j.jclinane.2018.06.007
Suppan L, Tramèr MR, Niquille M, Grosgurin O, Marti C. Alternative intubation techniques vs Macintosh laryngoscopy in patients with cervical spine immobilization: systematic review and meta-analysis of randomized controlled trials. Br J Anaesth 2016; 116: 27–36. https://doi.org/10.1093/bja/aev205
Singleton BN, Morris FK, Yet B, Buggy DJ, Perkins ZB. Effectiveness of intubation devices in patients with cervical spine immobilisation: a systematic review and network meta-analysis. Br J Anaesth 2021; 126: 1055–66. https://doi.org/10.1016/j.bja.2020.12.041
Hoshijima H, Denawa Y, Tominaga A, Nakamura C, Shiga T, Nagasaka H. Videolaryngoscope versus Macintosh laryngoscope for tracheal intubation in adults with obesity: a systematic review and meta-analysis. J Clin Anesth 2018; 44: 69–75. https://doi.org/10.1016/j.jclinane.2017.11.008
Maharaj CH, Costello JF, Higgins BD, Harte BH, Laffey JG. Learning and performance of tracheal intubation by novice personnel: a comparison of the Airtraq and Macintosh laryngoscope. Anaesthesia 2006; 61: 671–7. https://doi.org/10.1111/j.1365-2044.2006.04653.x
Pieters BM, Wilbers NE, Huijzer M, Winkens B, van Zundert AA. Comparison of seven videolaryngoscopes with the Macintosh laryngoscope in manikins by experienced and novice personnel. Anaesthesia 2016; 71: 556–64. https://doi.org/10.1111/anae.13413
Suzuki A, Toyama Y, Katsumi N, et al. The Pentax-AWS® rigid indirect video laryngoscope: clinical assessment of performance in 320 cases. Anaesthesia 2008; 63: 641–7. https://doi.org/10.1111/j.1365-2044.2008.05452.x
Lascarrou JB, Boisrame-Helms J, Bailly A, et al. Video laryngoscopy vs direct laryngoscopy on successful first-pass orotracheal intubation among ICU Patients: a randomized clinical trial. JAMA 2017; 317: 483–93. https://doi.org/10.1001/jama.2016.20603
Williams D, Ball DR. Palatal perforation associated with McGrath™ videolaryngoscope. Anaesthesia 2009; 64: 1144–5. https://doi.org/10.1111/j.1365-2044.2009.06091.x
Walker L, Brampton W, Halai M, et al. Randomized controlled trial of intubation with the McGrath™ Series 5 videolaryngoscope by inexperienced anaesthetists. Br J Anaesth 2009; 103: 440–5. https://doi.org/10.1093/bja/aep191
Bakshi SG, Vanjari VS, Divatia JV. A prospective, randomised, clinical study to compare the use of McGrath™, Truview® and Macintosh laryngoscopes for endotracheal intubation by novice and experienced Anaesthesiologists. Indian J Anaesth 2015; 59: 421–7. https://doi.org/10.4103/0019-5049.160946
Liu ZJ, Yi J, Guo WJ, Ma C, Huang YG. Comparison of McGrath™ Series 3 and Macintosh laryngoscopes for tracheal intubation in patients with normal airway by inexperienced anesthetists: a randomized study. Medicine (Baltimore) 2016; 95: e2514. https://doi.org/10.1097/md.0000000000002514
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Open Med 2009; 3: e123–30.
Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions; 2011. Available from URL: https://training.cochrane.org/handbook (accessed August 2023).
Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ 2004; 328: 1490. https://doi.org/10.1136/bmj.328.7454.1490
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327: 557–60. https://doi.org/10.1136/bmj.327.7414.557
Wetterslev J, Thorlund K, Brok J, Gluud C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J Clin Epidemiol 2008; 61: 64–75. https://doi.org/10.1016/j.jclinepi.2007.03.013
Thorlund K, Engstrøm J, Wetterslev J, Brok J, Imberger G, Gluud C. User manual for trial sequential analysis (TSA); 2011. Available from URL: www.ctu.dk/tsa (accessed August 2023).
Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: 629–34. https://doi.org/10.1136/bmj.315.7109.629
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994; 50: 1088–101.
Nouruzi-Sedeh P, Schumann M, Groeben H. Laryngoscopy via Macintosh blade versus GlideScope®: success rate and time for endotracheal intubation in untrained medical personnel. Anesthesiology 2009; 110: 32–7. https://doi.org/10.1097/aln.0b013e318190b6a7
Ayoub CM, Kanazi GE, Al Alami A, Rameh C, El-Khatib MF. Tracheal intubation following training with the GlideScope® compared to direct laryngoscopy. Anaesthesia 2010; 65: 674–8. https://doi.org/10.1111/j.1365-2044.2010.06335.x
Hirabayashi Y, Otsuka Y, Seo N. GlideScope® videolaryngoscope reduces the incidence of erroneous esophageal intubation by novice laryngoscopists. J Anesth 2010; 24: 303–5. https://doi.org/10.1007/s00540-010-0872-y
Park SJ, Lee WK, Lee DH. Is the Airtraq optical laryngoscope effective in tracheal intubation by novice personnel? Korean J Anesthesiol 2010; 59: 17–21. https://doi.org/10.4097/kjae.2010.59.1.17
Di Marco P, Scattoni L, Spinoglio A, et al. Learning curves of the Airtraq and the Macintosh laryngoscopes for tracheal intubation by novice laryngoscopists: a clinical study. Anesth Analg 2011; 112: 122–5. https://doi.org/10.1213/ane.0b013e3182005ef0
de Oliveira GS, Fitzgerald PC, Beckerly R, McCarthy RJ. A randomized comparison of the use of an optical compared with a rigid laryngoscope on the success rate of novices performing tracheal intubation. Anesth Analg 2011; 112: 615–8. https://doi.org/10.1213/ane.0b013e3182088768
Ferrando C, Aguilar G, Belda FJ. Comparison of the laryngeal view during tracheal intubation using Airtraq and Macintosh laryngoscopes by unskillful anesthesiology residents: a clinical study. Anesthesiol Res Pract 2011; 2011: 301057. https://doi.org/10.1155/2011/301057
Cattano D, Ferrario L, Patel CB, et al. Utilization of C-MAC® videolaryngoscopy for direct and indirect assisted endotracheal intubation. J Anesth Clin Sci 2013; 2: 10. https://doi.org/10.7243/2049-9752-2-10
Hirabayashi Y, Seo N. Airtraq optical laryngoscope: tracheal intubation by novice laryngoscopists. Emerg Med J 2009; 26: 112–3. https://doi.org/10.1136/emj.2008.059659
Zhao H, Feng Y, Zhou Y. Teaching tracheal intubation: Airtraq is superior to Macintosh laryngoscope. BMC Med Educ 2014; 14: 144. https://doi.org/10.1186/1472-6920-14-144
Kim KN, Jeong MA, Oh YN, Kim SY, Kim JY. Efficacy of Pentax airway scope versus Macintosh laryngoscope when used by novice personnel: a prospective randomized controlled study. J Int Med Res 2018; 46: 258–71. https://doi.org/10.1177/0300060517726229
Peirovifar A, Mahmoodpoor A, Golzari SE, Soleimanpour H, Eslampour Y, Fattahi V. Efficacy of video-guided laryngoscope in airway management skills of medical students. J Anaesthesiol Clin Pharmacol 2014; 30: 488–91. https://doi.org/10.4103/0970-9185.142810
Weiss M, Schwarz U, Dillier CM, Gerber AC. Teaching and supervising tracheal intubation in paediatric patients using videolaryngoscopy. Paediatr Anaesth 2001; 11: 343–8. https://doi.org/10.1046/j.1460-9592.2001.00681.x
Hwang SY, Lee SU, Lee TR, et al. Usefulness of C-MAC® video laryngoscope in direct laryngoscopy training in the emergency department: a propensity score matching analysis. PLoS One 2018; 13: e0208077. https://doi.org/10.1371/journal.pone.0208077
Hirabayashi Y, Shimada N, Nagashima S. Tracheal intubation using pediatric Airtraq optical laryngoscope in a patient with Treacher Collins syndrome. Paediatr Anaesth 2009; 19: 915–6. https://doi.org/10.1111/j.1460-9592.2009.03087.x
Shimada M, Hirabayashi Y, Seo N. Nasotracheal intubation using GlideScope® videolaryngoscope or Macintosh laryngoscope by novice laryngoscopists [Japanese]. Masui 2010; 59: 1318–20.
Cooper RM, Pacey JA, Bishop MJ, McCluskey SA. Early clinical experience with a new videolaryngoscope (GlideScope®) in 728 patients. Can J Anesth 2005; 52: 191–8. https://doi.org/10.1007/bf03027728
Hindman BJ, Santoni BG, Puttlitz CM, From RP, Todd MM. Intubation biomechanics: laryngoscope force and cervical spine motion during intubation with Macintosh and Airtraq laryngoscopes. Anesthesiology 2014; 121: 260–71. https://doi.org/10.1097/aln.0000000000000263
Carassiti M, Zanzonico R, Cecchini S, Silvestri S, Cataldo R, Agrò FE. Force and pressure distribution using Macintosh and GlideScope® laryngoscopes in normal and difficult airways: a manikin study. Br J Anaesth 2012; 108: 146–51. https://doi.org/10.1093/bja/aer304
Author contributions
Hiroshi Hoshijima, Takahiro Mihara, Toshiya Shiga, and Kentaro Mizuta contributed to all aspects of this manuscript, including study conception and design; acquisition, analysis, and interpretation of data; and drafting the article. Hiroshi Hoshijima, Toshiya Shiga, and Kentaro Mizuta contributed to the acquisition of data. Hiroshi Hoshijima, Takahiro Mihara, and Toshiya Shiga contributed to the analysis of data.
Disclosures
The authors state that they have no conflicts of interest to declare.
Funding statement
None.
Editorial responsibility
This submission was handled by Dr. Philip M. Jones, Deputy Editor-in-Chief, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hoshijima, H., Mihara, T., Shiga, T. et al. Indirect laryngoscopy is more effective than direct laryngoscopy when tracheal intubation is performed by novice operators: a systematic review, meta-analysis, and trial sequential analysis. Can J Anesth/J Can Anesth 71, 201–212 (2024). https://doi.org/10.1007/s12630-023-02642-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-023-02642-9