
Abstract
Purpose
In-hospital cardiac arrest is associated with high morbidity and mortality, with an overall survival rate at one year of approximately 13%. The first cardiac rhythm is often analyzed by anesthesiologist-intensivists. We aimed to determine the diagnostic performance of anesthesiologist-intensivists when distinguishing between shockable and nonshockable rhythms.
Methods
We conducted a simulation-based, multicentre, prospective, observational study between May 2019 and March 2020. The responses of the participants were used to calculate individual sensitivity (defined as the proportion of decisions to shock for shockable rhythms) and individual specificity (defined as the proportion of decisions not to shock for nonshockable rhythms). The main outcome measure was the overall diagnostic performance, defined as the overall sensitivity and specificity. Secondary outcome measures were the sensitivity and specificity of participants’ decisions for each type of cardiac arrest rhythm and their decision-making times.
Results
Among the 267 physicians contacted, 179 (67%) completed the test. The median [interquartile range (IQR)] overall sensitivity was 88 [79–95]% and the median overall specificity was 86 [77–92]%. Among shockable rhythms, the median [IQR] sensitivity was 100 [100–100]% for ventricular tachycardia (VT), 100 [100–100]% for coarse ventricular fibrillation (VF), and 60 [20–100]% for fine VF. The median [IQR] specificities for nonshockable rhythms were 93 [86–100]% for asystole and 83 [72–86]% for pulseless electrical activity. The median decision times ranged from 2.0 to 3.5 sec.
Conclusion
Anesthesiologist-intensivists were quickly and effectively able to analyze rhythms in this simulation-based study. Participants’ sensitivity in deciding to deliver shocks for VT and coarse VF was excellent, while specificity of their decisions for pulseless electrical activity was insufficient.
Résumé
Objectif
L’arrêt cardiaque intra-hospitalier est associé à une morbidité et mortalité élevées, associées à un taux de survie global à un an d’environ 13 %. Le premier rythme cardiaque est souvent analysé par des anesthésiologistes-intensivistes. Nous avons cherché à déterminer la performance diagnostique des anesthésiologistes-intensivistes à distinguer un rythme choquable d’un rythme non choquable.
Méthode
Nous avons effectué une étude observationnelle prospective, multicentrique basée sur la simulation entre mai 2019 et mars 2020. Les réponses des participants ont été utilisées pour calculer la sensibilité individuelle (définie comme étant la proportion de décisions de choquer pour les rythmes choquables) et la spécificité individuelle (définie comme la proportion de décisions de ne pas choquer pour les rythmes non choquables). Le critère d’évaluation principal était la performance diagnostique globale, définie comme étant la sensibilité et la spécificité globales. Les critères d’évaluation secondaires étaient la sensibilité et la spécificité des décisions des participants pour chaque type de rythme d’arrêt cardiaque, ainsi que le temps de prise de décision.
Résultats
Parmi les 267 médecins contactés, 179 (67 %) ont complété le test. La sensibilité globale médiane [écart interquartile (ÉIQ)] était de 88 [79-95] % et la spécificité globale médiane était de 86 [77-92] %. Parmi les rythmes choquables, la sensibilité médiane [ÉIQ] était de 100 [100-100] % pour la tachycardie ventriculaire (TV), de 100 [100-100] % pour la fibrillation ventriculaire (FV) large et de 60 [20-100] % pour la FV fine. Les spécificités médianes [ÉIQ] pour les rythmes non choquables étaient de 93 [86-100] % pour l’asystolie et de 83 [72-86] % pour l’activité électrique sans pouls. Les temps de décision médians variaient de 2,0 à 3,5 secondes.
Conclusion
Les anesthésiologistes-intensivistes ont été rapidement et efficacement en mesure d’analyser les rythmes dans cette étude basée sur la simulation. La sensibilité de prendre la décision d’administrer un choc pour une TV ou une FV était excellente pour les participants, tandis que la spécificité de cette décision pour l’activité électrique sans pouls était insuffisante.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Although cardiopulmonary resuscitation (CPR) measures have improved continuously since the 1960s, in-hospital cardiac arrest (IHCA) remains associated with high morbidity and mortality.1 A recent meta-analysis found that the overall survival rate from IHCA at one year was 13.4%, with survival more likely from events of cardiac origin (39.3%) than from those of noncardiac origin (10.7%).2 Ninety-two percent of survivors were found to have a cerebral performance category score of 1 or 2, corresponding to a good neurologic prognosis.2
The availability of automated external defibrillators (AEDs) outside of hospitals has been associated with a clear improvement in survival after cardiorespiratory arrest, as witnesses can perform early defibrillation before the emergency services arrive.3,4 In contrast, studies of in-hospital AED use have mostly shown no benefit in terms of survival.5,6,7,8 The proportion of shockable rhythms differs between in-hospital cardiac arrests (20%) and out-of-hospital cardiac arrests (37%).6,9,10
In French hospitals, when AEDs are not available, first assessments of cardiac rhythm are carried out by medical emergency teams led by anesthesiologist-intensivists, who are doubly qualified in critical care medicine and anesthesiology. Many hospitals in France are nevertheless equipped with AEDs, allowing defibrillation to be performed in some cases before the emergency team arrives.
The hypothesis of this study was that anesthesiologist-intensivists would have a lower diagnostic performance than AEDs, but would make decisions faster. Therefore, the primary objective was to determine the diagnostic performance of anesthesiologist-intensivists in identifying rhythms as shockable or nonshockable. The secondary objectives were to analyze decision-making times, to estimate the sensitivity and specificity of the decisions for subgroups of cardiac arrest rhythms, and to search for demographic factors associated with performance.
Methods
Study design
This was a simulation-based, multicentre, prospective, observational study that took place between May 2019 and March 2020. Junior and senior anesthesiologist-intensivists in six French hospitals (four university hospitals and two military hospitals) were sent a link to an online AED simulator along with a standardized questionnaire to record respondents’ age, sex, level of experience, number of CPRs performed per year, preferred mode of defibrillator operation (manual, semiautomatic, or situation-dependent), and main activity (intensive care or operating room). Email reminders were sent every month in the absence of a response. Respondents were excluded if they had incomplete responses to one or several tasks. We chose a convenient sample of 100 participants for this study.
Ethical approval
The study was approved on 10 June 2019, by the research ethics committee of the French Society of Anesthesiology and Intensive Care (Société Française d'Anesthésie et de Réanimation, IRB N° 00010254-2019-099), Paris, France (Chairman Prof. J. E. Bazin), and registered with the French Data Protection Agency (Commission Nationale de l’Informatique et des Libertés). All data were anonymized.
Simulator
The simulator, which is accessible online (https://simul-shock.firebaseapp.com/), presented as a manual defibrillator showing a series of 60 electrocardiograms as recorded in real time, with two buttons to either deliver a shock (“shock”) or not shock and resume chest compressions (“no shock”) (Electronic Supplementary Material [ESM], eFig. 1). The time taken to decide whether to shock was also recorded. Before starting the simulation, participants had to read instructions stating that whatever the proposed rhythm, the patient was in clinical cardiac arrest, therefore unconscious and without a palpable pulse.
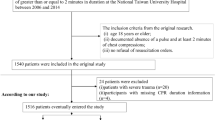
The electrocardiogram recordings shown by the simulator were performed in real use by AEDs (Defigard Touch 7, Schiller, Wissembourg, France) in patients with cardiac arrest. The chosen recordings lasted approximately 10 sec and did not contain signs of shock delivery or chest compression artifacts. Three expert physicians analyzed an initial set of 62 recordings on the simulator to determine whether the rhythms were shockable. If there was disagreement (n = 4), the recordings were assessed a second time, and eliminated if no consensus could be reached (n = 2). Experts’ consensus decisions were defined as the gold standard, with 100% sensitivity and specificity. The testing dataset therefore consisted of 60 electrocardiograms (Fig. 1): 14 (23%) showed asystole, 29 (48%) showed pulseless electrical activity (PEA), four (7%) showed coarse ventricular fibrillation (VF), five (8%) showed fine VF, and the remaining eight (13%) showed ventricular tachycardia (VT).

Several rhythms on the simulator
Outcome measures
The main outcome measure was the performance of participants in diagnosing rhythms as shockable or nonshockable, defined as the overall sensitivity and specificity of their decisions over the entire test dataset. Secondary outcome measures were the sensitivity and specificity of participants’ decisions for each rhythm category, and their decision-making times, as measured from the moment each electrocardiogram, were shown on the screen to the moment participants pressed the “shock” or “no shock” button.
Statistical analyses
For each participant, their responses to the 60 electrocardiograms were used to calculate individual sensitivity (defined as the proportion of decisions to shock for shockable rhythms), and individual specificity (defined as the proportion of decisions not to shock for nonshockable rhythms). Overall diagnostic performance was then presented as the overall median sensitivity and the overall median specificity of the participants together with the interquartile range. Results for each type of rhythm were statistically weighted to match the proportions reported in the literature: asystole (34.9%), PEA (46.5%), VF (10.4%), and VT (8.1%).11 This artificially inflated the number of recordings in each category without affecting the overall diagnostic performance. The median values of sensitivity and specificity were used and substituted into the formulas to calculate the likelihood ratios.
The sensitivity for each type of shockable rhythm (VT, coarse VF, and fine VF) and the specificity for each type of nonshockable rhythm (asystole and PEA) were also calculated. Univariate associations between demographic variables and participants’ sensitivity and specificity were also investigated. Decision-making times are presented as the median value of all delays for each rhythm category.
The demographic values are presented as median [interquartile range (IQR)] and number (%). Continuous variables are summarized as median [IQR]. Decision-making times were compared using the Wilcoxon–Mann–Whitney test. All tests were two-sided. As our study was exploratory, with a target sample size that was set arbitrarily, differences were considered significant at P < 0.01. All statistical analyses were performed using the R software version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Flow chart
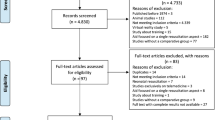
Among the 267 anesthesiologist-intensivists contacted to participate in the study, 186 (70%) participated, seven (4%) of whom did not complete the test (ESM eTable). The final number of participants was 179 (response rate of 67%) (Fig. 2).

Study flow chart
Demographic characteristics
The demographic characteristics of the participants are summarized in Table 1. The median age was 32 yr and most respondents were male (113/179, 63%) and senior physicians (124/179, 69%), with a median of four years of seniority. Most participants performed fewer than six CPRs per year (n = 100, 56%) and preferred to use defibrillators in manual mode (n = 89, 50%).
Sensitivity and specificity
The median [IQR] overall sensitivity was 88 [79–95]% and the median overall specificity was 86 [77–92]%. The positive likelihood ratio was 6.29, and the negative likelihood ratio was 0.14. The corresponding receiver operating characteristic curve is shown in Fig. 3.

Receiver operating characteristic curve for anesthesiologist-intensivists in identifying shockable and nonshockable rhythms. This curve was constructed from the [sensitivity/(1-specificity)] coordinates of each anesthesiologist-intensivist. It allows to graphically apprehend the group performance by visualizing the area under the curve (AUC). Nevertheless, we cannot obtain a regression function represented by a mathematical model so we cannot provide an AUC value.
Among shockable rhythms, the median [IQR] sensitivity was 100 [100–100]% for VT, 100 [100–100]% for coarse VF, and 60 [20–100]% for fine VF. The median [IQR] specificities for nonshockable rhythms were 93 [86–100]% for asystole and 83 [72–86]% for PEA.
Table 2 presents the results of the univariate analysis of the association between sensitivity, specificity, and demographic variables. Senior status was significantly associated with higher sensitivity. There were no significant differences in the of annual number of CPRs performed, main activity, and preferential defibrillator mode of use.
Decision-making times
Decision-making times (Fig. 4) differed between rhythm categories. The most rapidly recognized rhythms were the coarse VF and VT. The median decision times ranged from 2.0 to 3.5 sec. Most responses were made within five seconds (ESM eFig. 2).

Box plots showing physicians' decision-making times for each rhythm category. The black line indicates the median value. The box edges indicate the 25th and 75th quartile (Q25 and Q75), and the whiskers indicate minimum and maximum values.
Discussion
In the present simulation-based multicentre study, the median overall sensitivity and specificity of the studied anesthesiologist-intensivists in recognizing shockable and nonshockable rhythms were 88% and 86%, respectively. A comparative study of two AEDs reported 91% and 99% for the first, and 100% and 96% for the second.12 Compared with USA recommendations for the diagnostic performance of AEDs, the sensitivity of this group of anesthesiologist-intensivists was adequate for VT and coarse VF, but the specificity was insufficient, particularly for PEA.13
The 100% sensitivity determined here for VT and coarse VF suggests that anesthesiologist-intensivists correctly decide to deliver shocks in these situations. In contrast, the specificities of 93% for asystole and 83% for PEA suggest that in some of these cases, shocks are delivered when they should not be. Inappropriate shocks are deleterious during CPR because they require the unwarranted cessation of cardiac massage, resulting in a longer period of no-flow.14,15
Regarding the sensitivity of participants for fine VF (60%), these results are more difficult to interpret. Indeed, 2015 European Resuscitation Council recommendations (that applied during the study) were to not shock in case of diagnostic uncertainty between asystole and very fine VF.16 The fact that the electrocardiograms were presented by the simulator without a y-axis scale or gridlines made differentiating these two rhythms and deciding to shock or not much harder, and the substantially lower sensitivity observed for fine VF may thus be explained by a corresponding increase in false negatives. The latest 2021 European Resuscitation Council recommendations state that when the rhythm is clearly judged to be VF, a shock should be given.17
The availability of AEDs in hospitals has so far not had a significant effect on IHCA survival rates, which have not improved since 2010.5,6,7,8,18 The most important factor in improving survival from IHCA seems to be reducing the time between cardiac arrest and the first shock in cases of VF or VT. Indeed, survival is significantly reduced if the shock is administered more than two minutes after the start of CPR.19,20 In our study, the difference in decision times between rhythms was statistically different but clearly not clinically relevant: most response times were below five seconds. In comparison, recent AEDs can assess electrocardiogram rhythms and advise on whether to shock within five seconds of the interruption of chest compressions.21 Decision-making times are therefore very similar for anesthesiologists-intensivists and AEDs. The second issue in improving survival rates is to limit the time without chest compressions. Operating the defibrillator in manual mode saves time by avoiding the spoken instructions and the sometimes lengthy cardiac rhythm analysis in semiautomatic mode, but increases the number of inappropriate shocks and associated interruptions in chest compressions.14,22 The latter risk is highlighted by the limited specificity of anesthesiologist-intensivists measured here. Koller et al. found error rates of 6–11% in the analyses of five AEDs.23 External artifacts due notably to chest compressions continued despite instructions from the AED to stop can also lead to incorrect decisions.24 A fourth issue in this context is the training of medical emergency teams. Return of spontaneous circulation and survival at one year after IHCA is more likely when CPR is delivered by teams trained in advanced cardiac life support.25 Continuing education for anesthesiologist-intensivists who do not regularly treat IHCAs may increase diagnostic performance and thereby the likelihood of correct defibrillation decisions.
Several strategies have been investigated with AEDs to limit or avoid interruptions in cardiac rhythm analysis during chest compressions or to detect returns of effective spontaneous circulation during rhythm analysis.21,26,27,28 Automatic analysis while chest compressions are ongoing, along with a high diagnostic performance, would certainly reduce the cognitive load of physicians during CPR, leaving more time to lead the emergency team and identifying and treating the cause of cardiac arrest, thereby increasing patient survival rates.29,30,31 At present, limitations in the interpretation of AEDs should encourage the practitioner to be cautious about their use. It is important to remember that responsibility for decision-making rests with the physician and that survival rates for in-hospital cardiac arrest have not been improved by their introduction in wards.5,6,7,8,18
The strengths of the study include its size (n = 179) and high response rate (67%). In terms of methodology, the original design and use of real electrocardiogram recordings are also strengths.
The study is limited by its observational nature and the fact that the tests were conducted under simulated conditions. An investigation of anesthesiologist-intensivists’ decisions in the management of real IHCAs would better reflect actual clinical practice. Nevertheless, decisions taken under real conditions may be difficult to analyze retrospectively because of CPR artifacts, with the added complication that all clinical situations are unique. In contrast, these simulations allowed participants’ performance to be evaluated uniformly, in a controlled environment. Another limitation of the study is the fact that the 60 recordings were analyzed in sequence, and a drop in performance at the end of the test may have led to an underestimation of sensitivity and specificity. Our study may be underpowered with respect to showing differences in diagnostic performance between groups of physicians. A dedicated analysis of the group of critical care consultants, who are responsible for managing cardiac arrest in their daily practice, would have been particularly interesting, but only possible if we had had more participants. Our group of participants may be younger and have less experience compared with other centers, and this may limit the generalizability of our results. Furthermore, while medical emergency teams often include nonanesthesiologist-intensivists or emergency physicians, the performance of these categories of physicians was not evaluated. Finally, as pointed out above, the electrocardiograms were displayed by the simulator without a y-axis scale, which made very fine VF (nonshockable) difficult to distinguish from fine VF (shockable).
In conclusion, the anesthesiologist-intensivists who participated in this simulation-based study classified rhythms as “shockable” or “nonshockable” with a median overall sensitivity of 88%, and a median overall specificity of 86%. Participants’ sensitivity in deciding to deliver shocks for VT and coarse VF was excellent, while the specificity of their decisions to not shock for PEA was inadequate, implying that shocks would have been delivered inappropriately. Their decision-making times were below five seconds. Theoretical and practical training in recognizing cardiac arrest rhythms should be strengthened for anesthesiologist-intensivists who use defibrillators in manual mode. After validation in a larger cohort, the online simulation tool created for this study could be used as part of a continuing education program.
References
Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed-chest cardiac massage. JAMA 1960; 173:1064–67. https://doi.org/10.1001/jama.1960.03020280004002
Schluep M, Gravesteijn BY, Stolker RJ, Endeman H, Hoeks SE. One-year survival after in-hospital cardiac arrest: a systematic review and meta-analysis. Resuscitation 2018; 132: 90–100. https://doi.org/10.1016/j.resuscitation.2018.09.001
Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. N Engl J Med 2000; 343: 1206–9. https://doi.org/10.1056/nejm200010263431701
Hallstrom AP, Ornato JP, Weisfeldt M, et al. Public-access defibrillation and survival after out-of-hospital cardiac arrest. N Engl J Med 2004; 351: 637–46. https://doi.org/10.1056/nejmoa040566
Smith RJ, Hickey BB, Santamaria JD. Automated external defibrillators and in-hospital cardiac arrest: patient survival and device performance at an Australian teaching hospital. Resuscitation 2011; 82: 1537–42. https://doi.org/10.1016/j.resuscitation.2011.06.025
Chan PS, Krumholz HM, Spertus JA, et al. Automated external defibrillators and survival after in-hospital cardiac arrest. JAMA 2010; 304: 2129–36. https://doi.org/10.1001/jama.2010.1576
Huschak G, Dünnebier A, Kaisers UX, Huschens B, Bercker S. Automated external defibrillator use for in-hospital emergency management. Anaesth Intensive Care 2016; 44: 353–8. https://doi.org/10.1177/0310057x1604400304
Forcina MS, Farhat AY, O’Neill WW, Haines DE. Cardiac arrest survival after implementation of automated external defibrillator technology in the in-hospital setting. Crit Care Med 2009; 37: 1229–36. https://doi.org/10.1097/ccm.0b013e3181960ff3
Andersen LW, Holmberg MJ, Berg KM, Donnino MW, Granfeldt A. In-hospital cardiac arrest: a review. JAMA 2019; 321: 1200–10. https://doi.org/10.1001/jama.2019.1696
Oving I, de Graaf C, Karlsson L, et al. Occurrence of shockable rhythm in out-of-hospital cardiac arrest over time: a report from the COSTA group. Resuscitation 2020; 151: 67–74. https://doi.org/10.1016/j.resuscitation.2020.03.014
Girotra S, Nallamothu BK, Spertus JA, et al. Trends in survival after in-hospital cardiac arrest. N Engl J Med 2012; 367: 1912–20. https://doi.org/10.1056/nejmoa1109148
Israelsson J, von Wangenheim B, Årestedt K, Semark B, Schildmeijer K, Carlsson J. Sensitivity and specificity of two different automated external defibrillators. Resuscitation 2017; 120: 108–12. https://doi.org/10.1016/j.resuscitation.2017.09.009
Kerber RE, Becker LB, Bourland JD, et al. Automatic external defibrillators for public access defibrillation: recommendations for specifying and reporting arrhythmia analysis algorithm performance, incorporating new waveforms, and enhancing safety: a statement for health professionals from the American Heart Association Task Force on Automatic External Defibrillation, Subcommittee on AED Safety and Efficacy. Circulation 1997; 95: 1677–82. https://doi.org/10.1161/01.cir.95.6.1677
Kramer-Johansen J, Edelson DP, Abella BS, Becker LB, Wik L, Steen PA. Pauses in chest compression and inappropriate shocks: a comparison of manual and semi-automatic defibrillation attempts. Resuscitation 2007; 73: 212–20. https://doi.org/10.1016/j.resuscitation.2006.09.006
Calle PA, Mpotos N, Calle SP, Monsieurs KG. Inaccurate treatment decisions of automated external defibrillators used by emergency medical services personnel: incidence, cause and impact on outcome. Resuscitation 2015; 88: 68–74. https://doi.org/10.1016/j.resuscitation.2014.12.017
Soar J, Nolan JP, Böttiger BW, et al. European Resuscitation Council guidelines for resuscitation 2015: Section 3. Adult advanced life support. Resuscitation 2015; 95:100–47. https://doi.org/10.1016/j.resuscitation.2015.07.016
Soar J, Böttiger BW, Carli P, et al. European Resuscitation Council guidelines 2021: adult advanced life support. Resuscitation 2021; 161: 115–51. https://doi.org/10.1016/j.resuscitation.2021.02.010
Holmberg MJ, Granfeldt A, Girotra S, Donnino MW, Andersen LW, American Heart Association's Get with the Guidelines–Resuscitation Investigators. Trends in survival and introduction of the 2010 and 2015 guidelines for adult in-hospital cardiac arrest. Resuscitation 2020; 157: 112–20. https://doi.org/10.1016/j.resuscitation.2020.10.022
Bircher NG, Chan PS, Xu Y, American Heart Association's Get with the Guidelines–Resuscitation Investigators. Delays in cardiopulmonary resuscitation, defibrillation, and epinephrine administration all decrease survival in in-hospital cardiac arrest. Anesthesiology 2019; 130: 414–22. https://doi.org/10.1097/aln.0000000000002563
Chan PS, Krumholz HM, Nichol G, Nallamothu BK, American Heart Association National Registry of Cardiopulmonary Resuscitation Investigators. Delayed time to defibrillation after in-hospital cardiac arrest. N Engl J Med 2008; 358: 9–17. https://doi.org/10.1056/nejmoa0706467
Hu Y, Tang H, Liu C, et al. The performance of a new shock advisory algorithm to reduce interruptions during CPR. Resuscitation 2019; 143: 1–9. https://doi.org/10.1016/j.resuscitation.2019.07.026
Pytte M, Pedersen TE, Ottem J, Rokvam AS, Sunde K. Comparison of hands-off time during CPR with manual and semi-automatic defibrillation in a manikin model. Resuscitation 2007; 73: 131–6. https://doi.org/10.1016/j.resuscitation.2006.08.025
Koller AC, Salcido DD, Lawrence GL, Menegazzi JJ. Automated external defibrillator shock advisement discordance among multiple electrocardiographic rhythms and devices: a preliminary report. Prehosp Emerg Care 2019; 23: 740–5. https://doi.org/10.1080/10903127.2019.1586603
Calle PA, De Paepe P, Van Sassenbroeck D, Monsieurs KG. External artifacts by advanced life support providers misleading automated external defibrillators. Resuscitation 2008; 79: 482–9. https://doi.org/10.1016/j.resuscitation.2008.07.016
Moretti MA, Macado Cesar LA, Nusbacher A, Kern KB, Timerman S, Franchini Ramires JA. Advanced cardiac life support training improves long-term survival from in-hospital cardiac arrest. Resuscitation 2007; 72: 458–65. https://doi.org/10.1016/j.resuscitation.2006.06.039
Babaeizadeh S, Firoozabadi R, Han C, Helfenbein ED. Analyzing cardiac rhythm in the presence of chest compression artifact for automated shock advisory. J Electrocardiol 2014; 47: 798–803. https://doi.org/10.1016/j.jelectrocard.2014.07.021
Partridge R, Tan Q, Silver A, Riley M, Geheb F, Raymond R. Rhythm analysis and charging during chest compressions reduces compression pause time. Resuscitation 2015; 90: 133–7. https://doi.org/10.1016/j.resuscitation.2015.02.025
Ruiz JM, Ruiz de Gauna S, González-Otero DM, et al. Circulation assessment by automated external defibrillators during cardiopulmonary resuscitation. Resuscitation 2018; 128: 158–63. https://doi.org/10.1016/j.resuscitation.2018.04.036
Bergum D, Nordseth T, Mjølstad OC, Skogvoll E, Haugen BO. Causes of in-hospital cardiac arrest – incidences and rate of recognition. Resuscitation 2015; 87: 63–8. https://doi.org/10.1016/j.resuscitation.2014.11.007
Wallmuller C, Meron G, Kurkciyan I, Schober A, Stratil P, Sterz F. Causes of in-hospital cardiac arrest and influence on outcome. Resuscitation 2012; 83: 1206–11. https://doi.org/10.1016/j.resuscitation.2012.05.001
Bergum D, Haugen BO, Nordseth T, Mjølstad OC, Skogvoll E. Recognizing the causes of in-hospital cardiac arrest – a survival benefit. Resuscitation 2015; 97: 91–6. https://doi.org/10.1016/j.resuscitation.2015.09.395
Acknowledgements
The authors would like to thank Pierre Taboulet, MD (physician), Daniel Jost, MD (physician), Benoît Frattini, MD (physician), and Pascal Corpet (engineer) for their help in putting together the database and developing the simulator. The translation of this article was supported by the Bibliothèque Scientifique de l’Internat de Lyon and the Hospices Civils de Lyon.
Author information
Authors and Affiliations
Contributions
Jordan Bailly, Antoine Lamblin, Clement Derkenne, and Florian Roquet contributed to all aspects of this manuscript, including conception and design; acquisition, analysis, and interpretation of data; and drafting the article. Clement Hoffmann contributed to the acquisition and the interpretation of the data and drafting the article. Maximilien Cruc, Alexandre Bergis, and Anne Lelong contributed to the acquisition of the data.
Corresponding author
Ethics declarations
Disclosures
Schiller Medical, Wissembourg, France, digitized the cardiac arrest recordings necessary for the functioning of the simulator.
Funding statement
This work was supported by institutional funding of the Paris Fire Brigade and performed at the Anesthesiology and Critical Care Department, Edouard Herriot Hospital, 5, Place d’Arsonval, 69003 Lyon, France.
Editorial responsibility
This submission was handled by Dr. Vishal Uppal, Associate Editor, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bailly, J., Derkenne, C., Roquet, F. et al. In-hospital cardiac arrest rhythm analysis by anesthesiologists: a diagnostic performance study. Can J Anesth/J Can Anesth 70, 130–138 (2023). https://doi.org/10.1007/s12630-022-02346-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-022-02346-6