
Abstract
Purpose
The incidence of difficult and failed intubation is higher in obstetrical patients than in the general population because of anatomic and physiologic changes in pregnancy. Videolaryngoscopy improves the success rate of intubation and reduces complications when compared with direct laryngoscopy in adults; however, it is not known whether this extends to obstetrical surgery. The aim of this study was to examine the efficacy, efficiency, and safety of videolaryngoscopy compared with direct laryngoscopy in obstetrics.
Source
Central, CINAHL, Embase, MEDLINE and Web of Science databases were searched from inception to 27 May 2020 with no restrictions. Inclusion criteria included randomized-controlled trials (RCTs), observational studies, case series, and case reports that reported the application of videolaryngoscopy to intubate the trachea in pregnant patients having general anesthesia.
Principal findings
Overall, four RCTs with 428 participants, nine observational studies, and 35 case reports/series with 100 participants were included. On meta-analysis of three trials, the co-primary outcomes of first-attempt success rate (risk ratio, 1.02; 95% confidence intervals [CI], 0.98 to 1.06; P = 0.29; I2 = 0%) and time to tracheal intubation (mean difference, 1.20 sec; 95% CI, -6.63 to 9.04; P = 0.76; I2 = 95%) demonstrated no difference between videolaryngoscopy and direct laryngoscopy in parturients without difficult airways. Observational studies and case reports underline the role of videolaryngoscopy as a primary choice when difficulty with tracheal intubation is expected or as a rescue modality in difficult or failed intubations.
Conclusions
Evidence for the utility of videolaryngoscopy continues to evolve but supports its increased adoption in obstetrics where videolaryngoscopes should be immediately available for use as a first-line device.
Trial registration
PROSPERO (CRD42020189521); registered 6 July 2020.
Résumé
Objectif
L’incidence des intubations difficiles et de leur échec est plus élevée chez les patientes obstétricales que dans la population générale en raison des changements anatomiques et physiologiques liés à la grossesse. Chez l’adulte, la vidéolaryngoscopie améliore le taux de réussite de l’intubation et réduit les complications par rapport à la laryngoscopie directe; cependant, nous ne savons pas si ces avantages s’étendent également à la population obstétricale. L’objectif de cette étude était d’examiner l’efficacité, l’efficience et la sécurité de la vidéolaryngoscopie par rapport à la laryngoscopie directe en obstétrique.
Source
Les bases de données Central, CINAHL, Embase, MEDLINE et Web of Science ont été recherchées de leur création jusqu’au 27 mai 2020 sans restriction. Les critères d’inclusion comprenaient les études randomisées contrôlées (ERC), les études observationnelles, les séries de cas et les présentations de cas rapportant l’application de la vidéolaryngoscopie pour intuber la trachée de patientes enceintes recevant une anesthésie générale.
Constatations principales
Quatre ERC comptant 428 participantes, neuf études observationnelles et 35 présentations/séries de cas comptant 100 participantes ont été incluses. En effectuant une méta-analyse de trois études, les critères d’évaluation co-primaires du taux de réussite de l’intubation à la première tentative (risque relatif, 1,02; intervalle de confiance [IC] 95 %, 0,98 à 1,06; P = 0,29; I2 = 0 %) et le temps jusqu’à l’intubation endotrachéale (différence moyenne, 1,20 sec; IC 95 %, -6,63 à 9,04; P = 0,76; I2 = 95 %) n’ont démontré aucune différence entre la vidéolaryngoscopie et la laryngoscopie directe chez les parturientes ne présentant pas de difficultés au niveau des voies aériennes. Les études observationnelles et les présentations de cas soulignent le rôle de la vidéolaryngoscopie comme premier choix lorsque des difficultés sont anticipées pour l’intubation endotrachéale ou comme modalité de sauvetage dans les cas d’intubations difficiles ou ratées.
Conclusion
Les données probantes concernant l’utilité de la vidéolaryngoscopie continuent d’évoluer mais appuient son adoption accrue en obstétrique, où des vidéolaryngoscopes devraient être immédiatement disponibles pour être utilisés comme dispositif de première ligne.
Enregistrement de l’étude
PROSPERO (CRD42020189521); enregistrée le 6 juillet 2020.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Neuraxial anesthesia is most often administered to parturients for Cesarean delivery, but general anesthesia is still needed in approximately 6% of cases,1 the majority of these being emergent.2 If general anesthesia is required, supraglottic airway devices are not recommended because of the increased risk of aspiration and secondary aspiration pneumonitis,3 and hence tracheal intubation remains the mainstay of airway management.
Compared with the general population, the incidence of difficult or failed intubation is higher in obstetrical patients.4,5,6,7 This is attributed, in part, to anatomic and physiologic changes during pregnancy, including laryngopharyngeal edema, mucosal engorgement, decreased functional residual capacity, as well as environmental and human factors.8 Should difficult or failed intubation be encountered, pulmonary aspiration can still occur with an incidence of 8% in obstetrical patients relative to 1% in matched controls.4,9 Further, difficult and failed intubation has been associated with other complications such as hypoxia, hypertension, the need for an emergency surgical airway, unanticipated intensive care admission, and death.9,10 The possible consequences of a failed intubation in the parturient cannot only affect the mother but also the fetus.4
In the Obstetric Anaesthetists’ Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation, it has been recommended that videolaryngoscopes should be immediately available for all obstetric general anesthetics, and others have suggested that videolaryngoscopy should become the first-line standard of care.11,12 Comparison of videolaryngoscopy with direct laryngoscopy in a meta-analysis showed that videolaryngoscopy reduced the incidence of failed intubation and decreased the occurrence of complications such as airway trauma and hoarseness.13 Only one of the included trials, however, was performed in the setting of obstetrics, probably owing to the difficulties of research in this context where most general anesthetics are for an emergency Cesarean delivery,14 and airway device performance may vary with the circumstances of the difficult airway.
In view of this, we aimed to undertake a mixed-methods systematic review and meta-analysis to examine the efficacy, efficiency, and safety of videolaryngoscopy compared with direct laryngoscopy in parturients. Our primary objectives were to assess the efficacy through the first-attempt success rate of tracheal intubation and the efficiency via the time taken for tracheal intubation.
Methods
The study was registered in the PROSPERO database (CRD42020189521) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.15
We performed a systematic search of the Central, CINAHL, Embase, MEDLINE, and Web of Science Core Collection electronic databases from inception to 27 May 2020, with no restrictions on language or publication type. Controlled vocabulary terms and text words, relating to the main components of the review were chosen, including obstetrics and videolaryngoscopy. The complete search strategy is provided in Appendix 1.
All retrieved article citations were entered into the reference management software program, Rayyan (Qatar Computing Research Institute, 2016, Doha, Qatar), where duplicates were removed and the remainder were screened for eligibility. Case reports and series, prospective and retrospective observational studies, and randomized-controlled trials (RCTs) that reported on the application of videolaryngoscopy to intubate the trachea during general anesthesia in pregnant patients were considered for inclusion. Search results were independently screened by two authors (R.H. and N.D.) using the title and the abstract. The full texts of potentially eligible citations were subsequently evaluated for inclusion. Discrepancies were resolved by discussion and disagreements by a third author (D.O.). Moreover, the reference lists of all included articles were manually reviewed for additional citations by one author (S.H.).
Once all included articles had been identified, two authors (S.H. and D.O.) independently assessed the methodological quality in each non-randomized study with the Risk of Bias in Non-randomised Studies of Interventions (ROBINS-I)16 and in each RCT with the revised Cochrane risk of bias tool for randomized trials (RoB 2).17 Data were extracted by two authors (R.H. and N.D.), discrepancies were resolved by discussion and disagreements settled by a third author (D.O.).
Characteristics extracted from the observational studies, RCTs, and case reports/series where applicable included the following: sample size and number of patients in each study arm; indication for general anesthesia; predicted difficulty of the intubation; type of videolaryngoscope; experience of intubator; and the definition of failed intubation. Case reports/series were qualitatively summarized to provide information on the advantages, disadvantages, and the technical aspects of videolaryngoscopes. With respect to observational studies and RCTs, our co-primary outcomes were the first-attempt success rate at tracheal intubation and the time to tracheal intubation (defined as the total time for insertion of the laryngoscope, glottic visualization, and the placement of the endotracheal tube [ETT] until obtainment of end-tidal carbon dioxide on capnography). Secondary outcomes included the number of attempts at tracheal intubation, time to optimal laryngeal view (defined as the time taken for insertion of the laryngoscope and glottic visualization), time to place the ETT (defined as the time taken for the placement of the ETT until obtainment of capnography), perceived difficulty of tracheal intubation, reported visualization of the larynx with Cormack and Lehane grade or percentage of glottic opening (POGO),18 change in heart rate and mean arterial pressure after induction of general anesthesia, incidence of failed intubation and serious airway complications, as well as the rate of airway or laryngeal trauma, hoarseness, and sore throat.
Continuous outcomes were extracted as the mean and standard deviation (SD). If the mean and the SD had not been reported, we followed the recommendations from the Cochrane Collaboration, approximating the mean to be equivalent to the median, and the SD to be the interquartile range/1.35 or the range/4.19 Dichotomous outcomes were converted to the overall numbers of incidence. Data only presented in graphical format were extracted with a plot-digitizing software program, Plot Digitizer (Version 2.1, Free Software Foundation, 2015, Boston, MA, USA). If we needed to clarify the details of a study’s methodology or request missing data, we contacted the authors of the respective articles up to three times to request these data.
For the RCTs, data were inputted from a standardized data collection form in Microsoft® Excel (Microsoft Corp, Redmond, WA, USA) to Review Manager (Version 5.3, The Nordic Cochrane Centre, 2014, Copenhagen, Denmark) by one author (N.D.), the accuracy of which was confirmed by another author (R.H.). It was our intention to conduct meta-analysis for an outcome of interest if it was reported by two or more RCTs. Statistical heterogeneity (I2) was calculated for each outcome with predetermined thresholds for low (25–49%), moderate (50–74%), and high (more than or equal to 75%) levels.20 If low heterogeneity was found, it was assumed that the true effect of the intervention was the same in every trial and a fixed-effect model was chosen to represent the best estimate of the intervention effect. In the event that moderate or high heterogeneity was present, it was assumed that the effect of the intervention was not the same in every trial and the DerSimonian and Laird random-effects model was chosen to represent the average intervention effect. For continuous outcomes, data were subjected to the inverse-variance method, where the weight attributed to each trial is the inverse of the variance of the effect estimate, resulting in the calculation of a weighted mean difference with its 95% confidence interval (CI). The mean difference was the absolute difference in the mean between the two groups. For dichotomous outcomes, data were subjected to the Mantel–Haenzel method, resulting in the calculation of a risk ratio (95% CI). The risk ratio is the ratio of the risk of an event in the two groups. All tests were two-tailed and performed at 5% significance level.
To evaluate for the risk of publication bias in relation to all outcomes, a funnel plot was drawn and visually examined for symmetry. Our results were verified by Duval and Tweedie’s trim and fill test, in which the smaller studies producing funnel plot asymmetry are removed and the omitted trials and their missing counterparts are replaced, and by Egger’s linear regression test using Comprehensive Meta-Analysis (Version 3.3, Biostat, 2014, NJ, USA).
Results
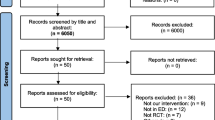
Of the initial 526 unique article citations identified by the search strategy, 35 case reports and series,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55 seven cross-sectional studies,56,57,58,59,60,61,62 one cohort study,63 one crossover study,64 and four RCTs fulfilled our inclusion criteria.65,66,67,68 Details of the screening process are illustrated in Fig. 1. In the 36 instances where we needed to clarify details of trial methodology or request missing data, nine authors responded with the required information.24,38,40,41,42,51,55

PRISMA flow diagram summarizing the retrieved, included, and excluded randomized-controlled trials. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Characteristics of the case reports and series are detailed in Table 1. The case reports/series, describing the use of videolaryngoscopes in 100 patients, provided an indication of the potential value of videolaryngoscopy as a first choice and rescue modality in patients with and without predictors of difficult intubation. Compared with direct laryngoscopy, videolaryngoscopy has been used to improve laryngeal visualization and success at tracheal intubation in patients with morbid obesity and unfavourable airway anatomy (e.g., restricted mouth opening). Videolaryngoscopy has further been utilized in the setting of awake tracheal intubation.24,48 The experience of the intubator was not reported in most cases. Further, our search uncovered some limitations of videolaryngoscopy, including the inability to fully insert a channelled videolaryngoscope (e.g., Airtraq™; Prodol Meditec S.A., Vizcaya, Spain that tends to be bulkier to accommodate the channel for the ETT) in the presence of restricted mouth opening, and the development of complications such as split ETT T-shaped connectors following insertion of the Gliderite® stylet which accompanies the Glidescope® (Verathon; Bothell, Australia), palatal perforation, and postoperative hoarseness.27,28,42
In five cross-sectional studies that examined the incidence of difficult and/or failed intubation in obstetrics,56,57,58,59,60 only one defined difficult intubation (i.e., Cormack and Lehane grade of 3 or 4).57 Kimura showed a difficult intubation incidence of 2.8% (eight in 286 patients), including two patients who were eventually intubated with an unspecified videolaryngoscope (after a first-attempt with direct laryngoscopy), and none of the 286 patients had a failed intubation.57 John et al. found the rate of difficult and failed intubation to be 1.9% (one in 52 patients) and 0.48% (one in 210 patients), respectively.60 Of the four patients who were difficult to intubate, three occurred out of normal working hours, one took place in an elective Cesarean delivery, and all four had subsequent successful tracheal intubation with the McGrath™ videolaryngoscope (Medtronic; Watford, UK). In the one patient where tracheal intubation failed, intubation of the trachea was attempted three times with a videolaryngoscope. Fennessy et al. reported the incidence of difficult intubation to be 0.36% (four in 1,113), and none of the 1,113 patients had a failed intubation.58 Of the four cases who were difficult to intubate, the most senior anesthesiologist present was a consultant in two cases and a speciality registrar in the other two cases. In one patient, the McGrath videolaryngoscope was selected from the start as the patient had retrognathia, and the remaining three had subsequent successful tracheal intubation following use of direct laryngoscopy. Rajagopalan et al. showed that the C-MAC® (KARL STORZ; Tuttlingen, Germany) or the Glidescope were used for the first intubation attempt in ten cases where the intubation was predicted to be difficult.59 Freedman et al. reported six failed intubations in their local hospital over a 20-year period, one of which was subsequently intubated successfully with an unspecified videolaryngoscope by a second anesthesiologist.56
Characteristics of the cohort and crossover studies and RCTs are presented in Table 2. The risk of bias was assessed with ROBINS-I for non-randomized studies (Appendix 2) and RoB 2 for RCTs (Fig. 2). Aziz et al. was the only non-randomized study where ROBINS-I could be conducted, and it was evaluated to be at serious risk of bias due to the possibility of confounding in the study design.63 Kurvey et al. did not present sufficient information in their published abstract to fairly judge the risk of bias.64 Some concerns were uncovered in all RCTs for the potential of bias in the measurement of the outcome as assessors were not blinded to the allocated interventions.

Risk of bias assessment of included randomized-controlled trials using the revised Cochrane risk of bias tool. ! = unclear risk; − = high risk; + = low risk
Overall, the RCTs comprised a total of 428 patients, in whom direct laryngoscopy was used in 184 and videolaryngoscopy in 244. All of the RCTs, unlike in the cohort studies, excluded patients with features suggestive of predicted difficulty in intubation. Further, the intubators were trainees in the cohort studies,63,64 while they were consultants, one trainee or unspecified in two, one, and one RCT, respectively.65,66,67,68
In a crossover simulation study, when a mannequin was prepared to simulate an easy obstetric airway with a corresponding Cormack and Lehane grade 1 laryngeal view, all 30 anesthesiologists were able to successfully intubate the trachea, and no differences were shown between direct laryngoscopy and use of the GlideScope in the average time to tracheal intubation (32.2 vs 35.1 sec; P = 0.26).64 If, however, the mannequin was set up to simulate a difficult obstetric airway (with a corresponding Cormack and Lehane grade 3 laryngeal view), the GlideScope was superior to direct laryngoscopy in the rate of successful tracheal intubation (96.7% vs 66.7%; P = 0.01) but not the time to tracheal intubation (33.1 vs 39.8 sec; P = 0.06). Of 180 intubations in an obstetric unit over a three year period, direct laryngoscopy was chosen as the first-line technique in 163, six of which failed and were rescued with a videolaryngoscope.63 The 18 patients where a videolaryngoscope was selected from the outset were more likely to have predictors of difficult intubation and were all intubated successfully on the first-attempt.
In the RCTs, our first co-primary outcome, the first-attempt success rate at tracheal intubation, was reported in 417 patients by three trials.65,67,68 No difference was shown between videolaryngoscopy and direct laryngoscopy (risk ratio, 1.02; 95% CI, 0.98 to 1.06; P = 0.29; I2 = 0%) (Fig. 3). Duval and Tweedie’s trim and fill test indicated the presence of publication bias (Appendix 3). Our second co-primary outcome, the time to tracheal intubation, was reported in 417 patients by three trials.65,67,68 No difference was found between videolaryngoscopy and direct laryngoscopy (mean difference, 1.20 sec; 95% CI, -6.63 to 9.04; P = 0.76; I2 = 95%) (Fig. 4). Neither the Duval and Tweedie’s trim and fill test nor the Egger’s test suggested the presence of publication bias. Regarding the secondary outcomes, the results of the meta-analyses are presented in Table 3. Sensitivity analysis showed that the use of a fixed-effect model to analyze outcomes when the statistical heterogeneity was less than 50% did not markedly influence the direction, magnitude, or statistical significance of the results. Data were insufficient to facilitate the meta-analysis of the other outcomes. No difference was found between direct laryngoscopy and videolaryngoscopy in the perceived difficulty of tracheal intubation or the change in heart rate and mean arterial pressure.67 Failed intubation or serious airway complications did not occur in any of the trials.

Forest plot of the first-pass success rate at tracheal intubation. For each trial, the square depicts the risk ratio and the horizontal lines either side of it represent the 95% CI. The summary result is presented as a diamond. CI = confidence interval; DL = direct laryngoscopy; SD = standard deviation; VLS = videolaryngoscope

Forest plot of the time to tracheal intubation. For each trial, the square depicts the mean difference and the horizontal lines either side of it represent the 95% CI. The summary result is presented as a diamond. CI = confidence interval; DL = direct laryngoscopy; SD = standard deviation; VLS = videolaryngoscope
In one comparative study, after discussions and staff training, a decision was made to change from direct laryngoscopy to first-line universal videolaryngoscopy with the GlideScope in all operating rooms, including obstetrics.61 Support from the anesthetic department for this paradigm shift in intubation technique increased from 33% prior to the trial phase to 100% 30 months later. The benefits reported included better training for anesthetic assistants and trainees, improved communication and human factors and, importantly, no reported requirement for cricothyroidotomy since 2014. In a tertiary obstetric unit where the McGrath was introduced, it was utilized in 66 of 100 cases and, although predictors of difficult intubation were present in ten of these, all tracheal intubations were successful.62
Discussion
In our meta-analysis of RCTs, no difference was shown between direct laryngoscopy and videolaryngoscopy in either the first-attempt success rate at tracheal intubation, despite improved laryngeal visualization with the latter, or the time to tracheal intubation in obstetrics. The synthesis of observational studies identified the usefulness of videolaryngoscopes as a first-line device for patients with characteristics indicative of a difficult airway and as a rescue tool after failed direct laryngoscopy.
It is likely that the optimal conditions afforded by the exclusion of parturients with characteristics indicative of a possible difficult airway, nature of elective Cesarean delivery, and the experience of intubators contributed towards the first-attempt success rate of 96% with direct laryngoscopy. If videolaryngoscopy were to increase this first-attempt success rate at tracheal intubation to 99%, then more than 800 parturients (as opposed to the 417 included in our analysis) would be needed to attain statistical significance. Consistent with this, under simulation conditions, differences were not found between direct laryngoscopy and videolaryngoscopy in the rate of successful tracheal intubation in a mannequin that had an easy obstetric airway.64 In contrast, however, videolaryngoscopy was superior to direct laryngoscopy in the rate of successful tracheal intubation when the mannequin was prepared to simulate a difficult obstetric airway. In the face of a decreased functional residual capacity and the increased oxygen consumption in a pregnant patient that shortens the safe apneic time,69 it is important to acknowledge that, although videolaryngoscopes did not reduce the time to tracheal intubation, they did not increase it. It has been previously reported that videolaryngoscopy requires the application of less force to the tongue base than direct laryngoscopy does and, as a surrogate measure of the stress response, this could potentially translate into reduced sympathetic stimulation,70,71 something that was not shown in our systematic review.
In order to evaluate the benefits and the drawbacks of videolaryngoscopy vs direct laryngoscopy in obstetrics, we must study a broader cohort indicative of the characteristics of patients we encounter in clinical practice, including those with predictors of difficult intubation having an emergency Cesarean delivery under the care of anesthesiologists with varying experience. Evidence from heterogenous obstetric populations in cross-sectional and comparative studies uncovers the potential role that videolaryngoscopy may have. There are many examples of patients who had direct laryngoscopy that failed and was rescued with videolaryngoscopy,56,57,58,59,60,62,63 as well as those where a videolaryngoscope was chosen as a first-line device when a difficult airway was possible.58,59,60,62,63 Only one study selected a videolaryngoscope as a first-line modality even in the absence of predictors of difficult intubation.62 The success rate for tracheal intubation with videolaryngoscopy across these studies was high, with one failure in a patient who was predicted to have a difficult airway.60 Given that the incidence of difficult intubation may be over 3%,59 immediate access to a videolaryngoscope in the labour ward might be appropriate, especially in view of the emergent nature of many of these Cesarean deliveries. In the UK, however, just over half of obstetric units in 2015 reported the presence of an available videolaryngoscope,72 and in a more recent prospective and multicentre observational study, videolaryngoscopy was used for only 1.9% of parturients who required general anesthesia.73
We suggest that the lack of difference shown between direct laryngoscopy and videolaryngoscopy in our meta-analysis for patients not predicted to have a difficult airway and scheduled for elective surgery should encourage an overall increased adoption of videolaryngoscopy in obstetrics. In doing so, we would obviate the need for a risk stratification to determine which laryngoscope is chosen as first-line, particularly as the positive predictive value and the sensitivity of airway examination is low,74 and have the potential to decrease the incidence of rescue intubations in what is otherwise a stressful and time-critical scenario. Further, this strategy should not increase either the number of attempts at tracheal intubation or the time to tracheal intubation in those patients predicted to have an easy airway. The use of videolaryngoscopy in these situations would contribute to the maintenence of proficiency needed to facilitate optimal and skilled use in difficult scenarios. Such implementation has already been achieved in some obstetric units. Indeed, one hospital that introduced videolaryngoscopes in all clinical areas reported that the requirement for emergency front of neck access reduced from one to two patients per year to none over five years.61 Interestingly, in a decision analysis, rapid sequence induction in conjunction with videolaryngoscopy in the context of a category one emergency Cesarean delivery for a patient with anticipated difficult tracheal intubation was shown to be associated with a failure rate of 21 per 100,000 and a shorter time to successful readiness to surgery relative to awake tracheal intubation.75
Most of our findings are consistent with those of prior systematic reviews including either exclusively or mainly non-obstetric patients.13,76,77,78,79 In a meta-analysis of 7,044 patients, including simulation studies, videolaryngoscopy decreased the failure rate of tracheal intubation with predicted difficult airways but not predicted non-difficult airways and with experienced operators unlike inexperienced operators.13 It did not, however, increase the first-attempt success rate at tracheal intubation. Hoarseness and laryngeal trauma were reduced with the use of a videolaryngoscope. In a further systematic review of 1,329 patients with known difficult airways, videolaryngoscopy increased the first-pass success rate at tracheal intubation.78 In all of these meta-analyses, the laryngeal view was improved with videolaryngoscopy,13,76,77,78,79 and in two of them, no difference between direct laryngoscopy and videolaryngoscopy in the time to tracheal intubation was revealed,77,79 with one showing a shorter time to tracheal intubation in those patients who presented with a difficult intubation.79
Strengths and limitations
Some limitations of our systematic review serve to restrict our conclusions. First, the number of RCTs in obstetrics is limited, and it is recognized that there are inherent problems to performing meta-analysis on a small number of trials.80 Despite this, the number of patients in the meta-analysis was disproportionately large for the number of included trials, which is why we decided to proceed with quantification. The statistical analysis for one of the primary outcomes of first-pass success rate was, however, still underpowered. Second, the assessors in the RCTs were not blinded to the allocated interventions resulting in the potential of bias for the measurement of the outcome. One observational study was at serious risk of bias secondary to the possibility of confounding in the study design. It is not possible, however, to blind the assessor and intubator to the nature of the airway device in these RCTs, and so it should be recognized that the introduction of such bias cannot be obviated. Third, the definition of outcomes was not standardized in the RCTs and this was likely responsible, at least in part, for the high statistical heterogeneity associated with the time to tracheal intubation. In one trial, the time to tracheal intubation was defined from the point at which the videolaryngoscope was held by the anesthetist65 and in two trials, it was specified from the time at which the blade of videolaryngoscope was inserted into the mouth.67,68 Fourth, many of the case reports and observational studies were published as abstracts in conference proceedings and thus had not undergone peer review. Lastly, in the absence of sufficient data, we were unable to determine which videolaryngoscope performs best in the setting of obstetrics.
Conclusions
Research into the use of videolaryngoscopy in obstetrics continues to evolve. In parturients without predictors of difficult intubation, videolaryngoscopy compared with direct laryngoscopy in the hands of experienced operators does not affect the first-pass success rate at tracheal intubation with no difference in the time to tracheal intubation. In a mixed cohort of pregnant patients, nevertheless, the videolaryngoscope has shown its utility both as a first-line device for patients with features suggestive of a difficult airway and as a rescue tool after failed direct laryngoscopy. This supports its increased adoption in obstetrics where videolaryngoscopes should be immediately available for use as the first-line device.
References
Juang J, Rodney RA, Dutton RP, Palanisamy A, Urman RD. Choice of anesthesia for cesarean delivery: an analysis of the National Anesthesia Clinical Outcomes Registry. Anesth Analg 2017; 124: 1914-7.
Traynor AJ, Aragon M, Ghosh D, et al. Obstetric Anesthesia Workforce Survey: a 30-year update. Anesth Analg 2016; 122: 1939-46.
Mendelson CL. The aspiration of stomach contents into the lungs during obstetric anesthesia. Am J Obstet Gynecol 1946; 52: 191-205.
Quinn AC, Milne D, Columb M, Gorton H, Knight M. Failed tracheal intubation in obstetric anaesthesia: 2 year national case-control study in the UK. Br J Anaesth 2013; 110: 74-80.
Kinsella SM, Winton AL, Mushambi MC, et al. Failed tracheal intubation during obstetric general anaesthesia: a literature review. Int J Obstet Anesth 2015; 24: 356-74.
Crosby ET, Cooper RM, Douglas MJ, et al. The unanticipated difficult airway with recommendations for management. Can J Anaesth 1998; 45: 757-76.
Shiga T, Wajima Z, Inoue T, Sakamoto A. Predicting difficult intubation in apparently normal patients: a meta-analysis of bedside screening test performance. Anesthesiology 2005; 103: 429-37.
Delgado C, Ring L, Mushambi MC. General anaesthesia in obstetrics. BJA Educ 2020; 20: 201-7.
Cook TM, Woodall N, Frerk C; Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia. Br J Anaesth 2011; 106: 617-31.
Rose DK, Cohen MM. The airway: problems and predictions in 18,500 patients. Can J Anaesth 1994; 41: 372-83.
Mushambi MC, Kinsella SM, Popat M, et al. Obstetric Anaesthetists’ Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics. Anaesthesia 2015; 70: 1286-306.
Zaouter C, Calderon J, Hemmerling TM. Videolaryngoscopy as a new standard of care. Br J Anaesth 2015; 114: 181-3.
Lewis SR, Butler AR, Parker J, Cook TM, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst Rev 2016; . https://doi.org/10.1002/14651858.CD011136.pub2.
Lucas DN, Vaughan DJ. Videolaryngoscopy and obstetric anaesthesia. Br J Anaesth 2017; . https://doi.org/10.1093/bja/aex289.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009; 151: 264-9.
Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ J 2016; . https://doi.org/10.1136/bmj.i4919.
Sterne JA, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; . https://doi.org/10.1136/bmj.l4898.
Levitan RM, Ochroch EA, Kush S, Shofer FS, Hollander JE. Assessment of airway visualization: validation of the percentage of glottic opening (POGO) scale. Acad Emerg Med 1998; 5: 919-23.
Higgins JP, Green S, The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. 2011. Available from URL: https://handbook-5-1.cochrane.org/ (accessed October 2020).
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: 1539-58.
Cohn AI, Hart RT, McGraw SR, Blass NH. The Bullard laryngoscope for emergency airway management in a morbidly obese parturient. Anesth Analg 1995; 81: 872-3.
Dhonneur G, Ndoko S, Amathieu R, El Housseini L, Poncelet C, Tual L. Tracheal intubation using the Airtraq® in morbid obese patients undergoing emergency cesarean delivery. Anesthesiology 2007; 106: 629-30.
Duffield AT, Smith KA. Anesthetic management for cesarean delivery of a parturient with impetigo herpetiformis. A A Case Rep 2013; 1: 14-6.
Kariya N, Kimura K, Iwasaki R, Ueki R, Tatara T, Tashiro C. Intraoperative awake tracheal intubation using the Airway ScopeTM in caesarean section. Anaesth Intensive Care 2013; 41: 390-2.
Radosevich MA, Finegold H, Goldfarb W, Troianos C. Anesthetic management of the pregnant burn patient: excision and grafting to emergency cesarean section. J Clin Anesth 2013; 25: 582-6.
Wouters B, Sanford DB. Anesthetic management of a simultaneous emergency craniotomy and cesarean delivery. AANA J 2013; 81: 394-8.
Arici S, Dogru S, Karaman S. Palatal perforation with McGrath series 5 videolaryngoscope. J Anesth 2014; . https://doi.org/10.1007/s00540-013-1709-2.
Loyd GE. GlideScope stylet associated with endotracheal tube T-connector split causing a breathing circuit leak. J Clin Anesth 2014; . https://doi.org/10.1016/j.jclinane.2014.04.001.
Nakao K, Komasawa N, Kusaka Y, Minami T. Rapid-sequence intubation in the left-lateral tilt position in a pregnant woman with premature placental abruption utilizing a videolaryngoscope. AJP Rep 2015; 5: e30-2.
Ni J, Luo L, Wu L, Luo D. The AirtraqTM laryngoscope as a first choice for parturients with an expected difficult airway. Int J Obstet Anesth 2014; 23: 94-5.
Cronin J, Bazick Cuschieri H, Dong X, et al. Anesthesia considerations for cesarean delivery in a patient with Loeys-Dietz syndrome. A A Case Rep 2015; 4: 47-8.
Lagoy JS, Kofford ND, Gosselin BJ, Russell MA, Morley BD. Management of a parturient with diastrophic dysplasia. A A Case Rep 2015; 5: 6-8.
Gray K, Lucas DN, Robinson PN, et al. A case series of successful videolaryngoscopic intubations in obstetric patients. Int J Obstet Anesth 2009; 18: S12 (abstract).
Paek G, McConville S, Kennington K, Chortkoff BS. Unanticipated emergency cricothyrotomy in a healthy parturient. Anesth Analg 2015; 120: S459 (abstract).
Rosenbaum T, Rosenbaum ER, Lienhart KL, Choate AI. Obstetric anesthesia for harlequin ichthyosis: a unique challenge. A A Case Rep 2015; 4: 19-21.
Sirico A, Maruotti GM, Martinelli P, et al. Airway management with McGrath series 5 video laryngoscope in a woman with Klippel-Feil syndrome requiring urgent caesarean section. Int J Obstet Anesth 2015; 24: 286-8.
Galey J, Bharadwaj S, Crimmins S, Hong CM, Malinow AM. Anesthetic implications of an obstetric patient with blue rubber bleb nevus syndrome. A A Case Rep 2016; 6: 146-9.
Coffman JC, Legg RL, Coffman CF, Moran KR. Lateral position for cesarean delivery because of severe aortocaval compression in a patient with Marfan syndrome: a case report. A A Case Rep 2017; 8: 93-5.
Laird A. The combination of paraplegia, respiratory failure, pregnancy and anaesthesia. Anaesthesia 2017; 72: 85 (abstract).
Maxey-Jones CL, Palmerton A, Farmer JR, Bateman BT. Difficult airway management caused by local anesthetic allergy during emergent cesarean delivery: a case report. A A Case Rep 2017; 9: 84-6.
Xiao W, Zhao L, Wang F, Sun H, Wang T, Zhao G. Total intravenous anesthesia without muscle relaxant in a parturient with amyotrophic lateral sclerosis undergoing cesarean section: a case report. J Clin Anesth 2017; 36: 107-9.
Creaney M, Moriarty RM, Milner M, Murphy C. Dexmedetomidine, high-flow nasal oxygen and sugammadex-reversal of rocuronium: overcoming anaesthetic challenges in a parturient with congenital muscular dystrophy presenting for caesarean section. Int J Obstet Anesth 2018; 34: 108-12.
Jadin S, Angle P, Berndl A. Anaesthetic management of a woman with limb-girdle muscular dystrophy for elective caesarean section. Int J Obstet Anesth 2018; 35: S57 (abstract).
Riada W, Ansari T. Effect of cricoid pressure on the laryngoscopic view by Airtraq in elective caesarean section: a pilot study. Eur J Anaesthesiol 2009; 26: 981-2.
Cesare AE, Rafer LC, Myler CS, Brennan KB. Anesthetic management for Ehlers-Danlos syndrome, hypermobility type complicated by local anesthetic allergy: a case report. Am J Case Rep 2019; 20: 39-42.
Betkekar SA, Volikas I. Use of high flow nasal oxygen for management of pulmonary oedema in severe preeclampsia. Int J Obstet Anesth 2019; 39: S60 (abstract).
Kormendy F, Jordan PA, Kremin JT, Nel MR. Life-threatening bronchospasm mimicking oesophageal intubation during caesarean delivery. Int J Obstet Anesth 2019; 39: S60 (abstract).
Zbeidy R, Torres Buendia N, Souki FG. Anaesthetic management of a parturient with spondylothoracic dysostosis. BMJ Case Rep 2020; . https://doi.org/10.1136/bcr-2019-232964.
Dinges E, Ortner C, Bollag L, Davies J, Landau R. Osteogenesis imperfecta: cesarean deliveries in identical twins. Int J Obstet Anesth 2015; 24: 64-8.
Turkstra TP, Armstrong PM, Jones PM, Quach T. GlideScope® use in the obstetric patient. Int J Obstet Anesth 2010; 19: 123-4.
Browning RM, Rucklidge MW. Tracheal intubation using the Pentax Airway Scope videolaryngoscope following failed direct laryngoscopy in a morbidly obese parturient. Int J Obstet Anesth 2011; 20: 200-1.
Mustapha B, Chkoura K, Elhassani M, Ahtil R, Azendour H, Kamili ND. Difficult intubation in a parturient with syringomyelia and Arnold-Chiari malformation: use of AirtraqTM laryngoscope. Saudi J Anaesth 2011; 5: 419-22.
Shonfeld A, Gray K, Lucas N, et al. Video laryngoscopy in obstetric anesthesia. J Obstet Anaesth Crit Care 2012; . https://doi.org/10.4103/2249-4472.99330.
Silva M, Swinson A, Halpern S, Margarido C. Transfusion-alternative strategies in a Jehovah’s Witness patient with placenta accreta and severe preeclampsia. Can J Anesth 2011; 58: S87 (abstract).
Chase CJ, Holak EJ, Pagel PS. Anesthetic implications of emergent cesarean section in a parturient with Noonan syndrome and bacterial endocarditis. J Clin Anesth 2013; 25: 403-6.
Freedman RL, Paramanathan S, Lucas DN, Robinson PN. Failed intubations in obstetric anaesthesia: patient or staff factors? Int J Obstet Anesth 2016; 26: S24 (abstract).
Kimura F. The frequency of difficult airway in cesarean section under general anesthesia: a retrospective study in a teaching hospital in Japan. Anesth Analg 2016; 123: 259 (absract).
Fennessy AR, Chevannes CL, Djabatey EA. Videolarygoscopy as a rescue technique for difficult airways in obstetric anaesthesia. Int J Obstet Anesth 2017; 31: S46 (abstract).
Rajagopalan S, Suresh M, Clark SL, Serratos B, Chandrasekhar S. Airway management for cesarean delivery performed under general anesthesia. Int J Obstet Anesth 2017; 29: 64-9.
John A, Hull T, Eccles J, Bhatia K. Difficult and failed intubation following general anaesthesia for caesarean section: incidence, management, maternal and neonatal outcomes. Int J Obstet Anesth 2019; 39: S14 (abstract).
Kelly FE, Penders R, Hughes J, et al. Implementation of universal videolaryngoscopy and development of intubation database accessed via a smart phone app. Trends Anaesth Crit Care 2020; 30: e151-2.
McLenachan J, Alexander N, Theodosiou K, Zhang C, McNarry A. McGrath MAC videolaryngoscope use in a tertiary obstetric unit. Trends Anaesth Crit Care 2020; 30: e106.
Aziz MF, Kim D, Mako J, Hand K, Brambrink AM. A retrospective study of the performance of video laryngoscopy in an obstetric unit. Anesth Analg 2012; 115: 904-6.
Kurvey A, Betharia V, McNamara G, Bewlay A, Pimblett M, Scullian K. GlideScope® video laryngoscopy is better than direct laryngoscopy in a simulated difficult obstetric airway. Int J Obstet Anesth 2016; 26: S42 (abstract).
Arici S, Karaman S, Doǧru S, et al. The McGrath series 5 video laryngoscope versus the Macintosh laryngoscope: a randomized trial in obstetric patients. Turkish J Med Sci 2014; 44: 387-92.
Amini S, Shakib M. Hemodynamic changes following endotracheal intubation in patients undergoing cesarean section with general anesthesia: application of Glidescope® videolaryngoscope versus direct laryngoscope. Anesthesiol Pain Med 2015; . https://doi.org/10.5812/aapm.21836.
Blajic I, Hodzovic I, Lucovnik M, Mekis D, Novak-Jankovic V, Stopar Pintaric T. A randomised comparison of C-MACTM and King Vision® videolaryngoscopes with direct laryngoscopy in 180 obstetric patients. Int J Obstet Anesth 2019; 39: 35-41.
Toker MK, Altıparmak B, Karabay AG. Comparison of the McGrath video laryngoscope and Macintosh direct laryngoscope in obstetric patients: a randomized controlled trial. Pakistan J Med Sci 2019; 35: 342-7.
Archer GW Jr, Marx GF. Arterial oxygen tension during apnoea in parturient women. Br J Anaesth 1974; 46: 358-60.
Russell T, Khan S, Elman J, Katznelson R, Cooper RM. Measurement of forces applied during Macintosh direct laryngoscopy compared with GlideScope® videolaryngoscopy. Anaesthesia 2012; 67: 626-31.
Salman MM, Goetze N, Badrinath M, Shah M. The videolaryngoscope as a first-line intubation device in women with hypertensive disease of pregnancy. Int J Obstet Anesth 2018; 33: 87-8.
Cook TM, Kelly FE. A national survey of videolaryngoscopy in the United Kingdom. Br J Anaesth 2017; 118: 593-600.
Odor PM, Bampoe S, Moonesinghe SR, et al. General anaesthetic and airway management practice for obstetric surgery in England: a prospective, multicentre observational study. Anaesthesia 2020; . https://doi.org/10.1111/anae.15250.
Nørskov AK, Rosenstock CV, Wetterslev J, Astrup G, Afshari A, Lundstrøm LH. Diagnostic accuracy of anaesthesiologists’ prediction of difficult airway management in daily clinical practice: a cohort study of 188 064 patients registered in the Danish Anaesthesia Database. Anaesthesia 2015; 70: 272-81.
Krom AJ, Cohen Y, Miller JP, Ezri T, Halpern SH, Ginosar Y. Choice of anaesthesia for category-1 caesarean section in women with anticipated difficult tracheal intubation: the use of decision analysis. Anaesthesia 2017; 72: 156-71.
Hoshijima H, Kuratani N, Hirabayashi Y, Takeuchi R, Shiga T, Masaki E. Pentax Airway Scope® vs Macintosh laryngoscope for tracheal intubation in adult patients: a systematic review and meta-analysis. Anaesthesia 2014; 69: 911-8.
Griesdale DE, Liu D, McKinney J, Choi PT. Glidescope® video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: a systematic review and meta-analysis. Can J Anesth 2012; 59: 41-52.
Pieters BM, Maas EH, Knape JT, van Zundert AA. Videolaryngoscopy vs. direct laryngoscopy use by experienced anaesthetists in patients with known difficult airways: a systematic review and meta-analysis. Anaesthesia 2017; 72: 1532-41.
Su YC, Chen CC, Lee YK, Lee JY, Lin KJ. Comparison of video laryngoscopes with direct laryngoscopy for tracheal intubation: a meta-analysis of randomised trials. Eur J Anaesthesiol 2011; 28: 788-95.
Afshari A, Wetterslev J, Smith AF. Can systematic reviews with sparse data be trusted? Anaesthesia 2017; 72: 12-6.
Author contributions
Neel Desai designed the systematic review. Ryan Howle and Neel Desai screened the search results, selected studies for inclusion, extracted and analyzed the data, and wrote the manuscript. Desire Onwochei performed the search, undertook the risk of bias assessment, and revised the manuscript. Siew-Ling Harrison selected studies for inclusion and undertook the risk of bias assessment.
Disclosures
None declared.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Editorial responsibility
This submission was handled by Dr. Hilary P. Grocott, Editor-in-Chief, Canadian Journal of Anesthesia.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1: Search strategy
1 | video?laryngoscop*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 1157 |
2 | ((video or indirect) adj3 laryngoscop*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 1725 |
3 | Airtraq.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 377 |
4 | Bullard.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 138 |
5 | C?mac.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 322 |
6 | CoPilot.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 28 |
7 | Glidescope.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 619 |
8 | I?view.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 40 |
9 | King?Vision.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 20 |
10 | McGrath.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 366 |
11 | Pentax.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 412 |
12 | Storz.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 929 |
13 | UEScope.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 4 |
14 | AP advance.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 16 |
15 | Venner.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 104 |
16 | Vividtrac.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 3 |
17 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 | 5082 |
18 | exp Obstetrics/ | 22555 |
19 | obstetric*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 182779 |
20 | exp Delivery, Obstetric/ | 79562 |
21 | obstetric delivery.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 178 |
22 | exp Cesarean Section/ | 45020 |
23 | c?esarean*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 73131 |
24 | exp Anesthesia, Obstetrical/ | 12984 |
25 | obstetric* an?esthesia.mp. | 1488 |
26 | exp Parturition/ | 16987 |
27 | parturi*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 29926 |
28 | 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 | 251951 |
29 | 17 and 28 | 54 |
Appendix 2: Risk of bias domains

Appendix 3: Funnel plots

Rights and permissions
About this article

Cite this article
Howle, R., Onwochei, D., Harrison, SL. et al. Comparison of videolaryngoscopy and direct laryngoscopy for tracheal intubation in obstetrics: a mixed-methods systematic review and meta-analysis. Can J Anesth/J Can Anesth 68, 546–565 (2021). https://doi.org/10.1007/s12630-020-01908-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-020-01908-w