
Abstract
A strain of Alcaligenes faecalis A12C (A. faecalis A12C) isolated from Argyrosomus regius is a probiotic in fish. Previous experiments showed that A. faecalis A12C had inhibitory effects on the growth of multidrug-resistant bacteria. We aimed to confirm whether A. faecalis A12C is safe and has adequate intestinal colonization in experimental rats, and evaluate its efficacy in an animal model of peritonitis. We used 30 male rats, randomly divided into 6 groups (n = 5): three groups (HA7, HA15, HA30) received A. faecalis A12C in drinking water (6 × 108 CFU/mL) for 7 days, and three control groups received drinking water only. All groups were evaluated at 7, 15, and 30 days. Survival after A. faecalis A12C administration was 100% in all groups. Mild eosinophilia (1.5%, p < 0.01) and increased aspartate aminotransferase (86 IU/L, p < 0.05) were observed in HA7, followed by progressive normalization. No histological signs of organ injury were found. We observed significant E. coli decline in faeces, parallel to an increase in A. faecalis A12C at 7 days. E. coli had a tendency to recover initial values, while A. faecalis A12C disappeared from the intestinal microbiota at 30 days. To evaluate its efficacy against peritonitis, we studied two additional groups of animals: IA group pretreated with A. faecalis A12C before E. coli intra-abdominal inoculation, and IC group inoculated with no A. faecalis A12C. We found an increase in C-reactive protein, alanine aminotransferase, urea, and eosinophils in IC animals when compared with IA. Peritonitis was more evident in IC than in IA animals. Our findings suggest that A. faecalis A12C altered clinically relevant parameters in sepsis and was associated with a lesser spread of infection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The abdomen is the most common source of sepsis and is associated with an unacceptably high morbidity and mortality [1]. Sepsis is defined as a life-threatening organ dysfunction caused by a deregulated host response to infection [2]. Despite developments in antisepsis and antibiotic prophylaxis, septic complications are common in surgical patients. Many postoperative infections are caused by intestinal bacteria, and the intestinal barrier and patient's indigenous intestinal microbiota facilitate the development of complications such as peritonitis [3, 4] that could be fatal [5]. Escherichia coli (E. coli) is the most common pathogen in abdominal sepsis, in both human and rodents [6,7,8,9]. Direct administration of E. coli is one of the classic experimental models of peritonitis in rats [4].
Probiotics are living microorganisms that confer health benefits to the host through an interaction with the intestinal microbiota and the immune function when administered in adequate doses [10]. A variety of species of probiotics (including Bifidobacterium spp, Lactobacillus spp, Enterococcus spp, Streptococcus spp, Bacillus spp, and yeasts) have shown to benefit human and animal health both in vivo and in vitro [9, 11,12,13]. There are increasing numbers of studies evaluating the benefits of new candidate bacterial species as probiotics [14,15,16,17,18]. Studies with probiotics strains of Lactococcus spp, Enterococcus spp, Streptococcus spp, Vibrio spp, Bacillus spp, Pseudomonas spp, and Aeromonas spp [19,20,21] have revealed benefits for their natural hosts, by increasing immune response against an specific pathogen, production of inhibiting compounds, or competing for fixation sites.
The use of probiotics and immune stimulants has had a remarkable increase in aquaculture due to the trend of reducing the use of antibiotics. Currently, probiotics and immune stimulants are considered candidates to control fish diseases. In pilot studies from our group, strains of Alcaligenes faecalis, isolated from Argyrosomus regius gills, have shown in vitro excellent conditions as potential probiotic in fish due to inhibitory activity against the main bacterial fish pathogens [22]. These in vitro results have been confirmed in several in vivo experiments, reporting a potent protective effect after infection with the marine pathogen Vibrio anguillarum. In preliminary experiments with several multidrug-resistant bacteria from hospital origin, we found that Alcaligenes faecalis A12C (A. faecalis A12C) had inhibitory effects on the growth of E. coli, Klebsiella pneumoniae, and Enterobacter cloacae. Antibiotics are the first option to control infectious diseases due to their rapid action and availability. However, despite of being an effective strategy in the beginning, the negative effects on environmental and public health justify the need of developing new strategies for the prevention and treatment of bacterial infections in both human and veterinary medicine. Based on these pilot studies, we aimed to evaluate the potential therapeutic effect of A. faecalis A12C in an experimental, clinically relevant animal model of peritonitis.
Materials and Methods
Animals
This study was approved by the Local Animal Ethics Committee, Hospital Universitario Dr. Negrín, Las Palmas de Gran Canaria, Spain, and followed the recommendations of the European Commission (2010/63/EU), and the Spanish Legislation (Law 53/2013) for the protection of animals for scientific purposes. We used forty-two male Crl:Sprague–Dawley® (SD) rats of 12 weeks of age, obtained from a breeding colony kept under semi-barrier conditions from the animal facilities of Hospital Universitario de Gran Canaria, Dr. Negrín, were a third generation of a colony from Charles River (Barcelona, Spain). Rats were housed in pairs in mini-aisled cages of 1500 cm2 (480 × 375 × 210 mm) (Tecniplast, Buguggiate, Italy) with enrichment consisting of an igloo and some nesting material. Cage change was undertaken twice a week. Rats were fed with a diet consisted of rat chow pellets (Teklad® Global 14% Protein Rodent Maintenance Diet, Harlan, Barcelona, Spain) and drinking water (Fonteide®, S/C de Tenerife, Spain) were available ad libitum. The light/dark cycle was 12/12 h. Room temperature was maintained at 21 ± 1 °C, and relative humidity was 55 ± 5% with an air exchange rate of 15 times/h. All the rats were acclimatized for 21 days and were determined to be healthy on the basis of individual physical examinations, and pathogen-free based on the results of routine microbiological screening performed on the colony in accordance with European recommendations [23].
Preparation of A. faecalis A12C for Administration to Rats
The probiotic strain A. faecalis A12C was isolated from Argyrosomus regius gills at the Instituto de Sanidad Animal y Seguridad Alimentaria of the University of Las Palmas de Gran Canaria. The strain was identified at the Microbiology Department of the Hospital Universitario de Gran Canaria Dr Negrín by means of matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) system (Vitek®MS, Biomerieux, Madrid, Spain). A. faecalis A12C strain cultures were stored at − 80 °C with 20% glycerol (v/v) addition in Brain Heart Infusion broth (PanReac-AppliChem, Darmstadt, Germany). Fresh cultures were made prior the assays, and the strain was aerobically incubated in Trypticase Soy with 5% sheep blood (Becton Dickinson, Franklin Lakes, New Jersey, USA) medium for 18 h at 37 °C with shaking (120 rpm) each 2 days. Before the challenge, the bacteria were centrifuged at 2500×g for 10 min and washed three times with sterile 0.9% saline solution. The bacteria were resuspended in dinking mineral water (Fonteide®), and bacterial concentration was measured with a spectrometer at 600 nm. Mineral water (Fonteide®) was used to adjust the suspension to 6 × 108 CFU/mL. Finally, the suspension was stored at 4 °C and protected from light.
E. coli Inocula Preparation
The E. coli strain used in this study to produce peritonitis was isolated from intestinal microbiota of healthy Sprague Dawley rats from the animal facility of the Hospital Universitario de Gran Canaria, Dr. Negrín. The MALDI-TOF MS (Vitek®MS, Biomerieux) technique [24] was used for the strain identification. The strain was designated as E. coli EBETAN-1 HUGCDN. E. coli strain cultures were stored at − 80 °C with 20% glycerol (v/v) addition in Brain Heart Infusion broth (PanReac-AppliChem). Fresh cultures were made prior the assays, and the strain was aerobically incubated in Trypticase Soy broth (Becton Dickinson) medium for 18 h at 37 °C with shaking (120 rpm). Before the challenge, the bacteria were centrifuged at 2500×g for 10 min and washed three times with sterile 0.9% saline solution. The bacterial concentration was measured with a spectrometer at 600 nm. Sterile 0.9% saline solution was used to adjust the suspension to the desired bacterial concentration (2 × 106 CFU/ml).
Experimental Design
This study was performed in two phases. First, 30 healthy rats were randomly divided into 6 groups: (i) healthy (negative controls-1), assessed at 7 days (HC7, n = 5), 15 days (HC15, n = 5), and 30 days (HC30, n = 5) after the first dose of tap water, and (ii) animals treated with A. faecalis A12C (positive controls-1) and assessed after the first dose of probiotics at 7 days (HA7, n = 5), at 15 days (HA15, n = 5), and at 30 days (HA30, n = 5). Animals in groups HA7, HA15 and HA30 received the probiotic strain A. faecalis A12C in the drinking water (Fonteide®) during seven consecutive days. Simultaneously, we administered 2 mL of the same bacterial suspension every 48 h during the first 7 days through an orogastric tube. HC group animals also received the same volume of water (Fonteide®) without probiotic via an orogastric tube. Bottles with the bacterial suspension or only water were replenished daily.
In a second phase, 12 animals were randomly divided into two groups: (i) infected control group (IC) (n = 6), in which A. faecalis A12C was not administered (negative control-2) and peritoneal infection was induced as described below, and (ii) group infected and pretreated with A. faecalis A12C (IA) (n = 6), in which the probiotic was administered during the firsts 7 days (positive control-2) in the drinking water (6 × 108 CFU/mL). Simultaneously, 2 mL of the same bacterial suspension or water (Fonteide®) were administered respectively to the IA or the IC groups every 48 h during the first 7 days through an orogastric tube.
Animals were euthanized at 7, 15, or 30 days after probiotic or mineral water administration (first phase) and at 7 days post E. coli inoculation in IA and IC (second phase). Figure 1 summarizes the experimental design.

Experimental design and timeline. HC7, HC15, and HC30 Healthy control groups assessed at 7 days, 15 days, and 30 days, respectively. HA7, HA15, and HA30 groups treated with A. faecalis A12C and assessed at 7 days, 15 days, and 30 days after the first dose of probiotics. IC Infected Control Group, IA Group treated with A. faecalis A12C and infected. Black tip arrow extra orogastric administration of water or A. faecalis A12C suspension. E euthanatized
Peritonitis Model
For induction of peritonitis, we used a classical model of intraabdominal sepsis [25]. We inoculated an E. coli strain isolated from intestinal microbiota of rat as described above. We administered 2 × 108 CFU/animal intraperitoneally using a 25G needle. We delivered analgesia with 0.05 mg/kg buprenorphine/12 h subcutaneous (Buprex®, Mundipharm, Limburg, Germany) during 3 days after the experimental infection. Animals were evaluated every 12 h according to signs shown in Table 1 [26].
Body Temperature, Weight, and Sample Collection
At the end of each experimental phase (7th day post-inoculation with E. coli, or at 7th, 15th, and 30th days in control animals), animals were weighed; their body temperature was measured in the perianal area using an infrared digital thermometer (T-One. CA-MI srL., Parma, Italy) and anesthetized with 0.3/0.3 mg/kg subcutaneously of a combination of medetomidine (Domtor®, Orion Pharma, Espoo, Finland) and fentanyl (Fentanest®, KERN Pharma, Terrassa, Spain). When animals reached the anesthetic plane, the following samples were collected: blood from external jugular vein for hemogram and biochemistry; intracardiac blood for blood culture and serum collection; urine by direct puncture of urinary bladder for urine culture; bronchoalveolar lavage fluid (BALF) from the right lung (2–3 mL) for microbiological culture; and liver, kidney, spleen, duodenum, pancreas, jejunum, mesenteric lymph nodes, thymus, and lung for histological evaluation. Rats were euthanized by exsanguination after cutting the caudal vena cava and abdominal aorta.
Blood Count and Blood Chemistry
Hematological parameters (hematocrit, red blood cells, platelets, total white cells, lymphocytes, monocytes, neutrophils, monocytes, eosinophils, and basophils) were counted on whole blood samples in EDTA K3 using an autoanalyser Cell-Dyn Sapphire (Abbott Laboratories, Chicago, Illinois, USA). In venous blood, measurements of serum biochemical parameters, including alanine aminotransferase (ALTL), aspartate aminotransferase (ASTL), creatinine (CREA), urea (UREA), and total bilirubin (TBIL) were performed on a Cobas 8000 Modular Analyser Series (Roche Diagnostics, Basel, Switzerland). Blood obtained by cardiac puncture was centrifuged, and serum was collected and stored at − 80 °C. Serum levels of C-reactive protein (CRP) were measured by ELISA using a rat DuoSet ELISA kit and DuoSet Ancillary Reagent Kit2 (R&D Systems, Abingdon, UK) following manufacturer's protocol.
Bacterial Counts in Faeces
To determine the survival capability of probiotic A. faecalis A12C in the intestine and its influence on the growth of E. coli from faecal microbiota, we assessed CFU/g stool of both bacterial species. Faeces were collected from the rectum of animals by abdominal massage at the beginning and at the end of each experimental period. To examine bacterial loads, serial tenfold dilutions were made in 0.9% sterile saline and plated on Brain-Heart infusion Agar (PanReac-AppliChem) modified by adding 4.5 g/100 mL of NaCl, 64 mg/L of vancomycin (SALA, Barcelona, Spain), and 0.02 g/L of bromothymol blue (MERCK, Darmstadt, Germany). After incubation at 37 °C for 24 h (E. coli) or 72 h (A. faecalis A12C), we calculated total viable counts of original samples (CFU/g faeces). Colonies were separated and isolated 2–3 times. We identified bacterial species using colony morphology and Gram stain. MALDI-TOF MS (Vitek®MS, Biomerieux) technique [24] was used for advanced identification.
Microbiological Analysis
Samples were processed within 2 h of collection. To investigate aerobic microorganisms, 100 µL of urine, blood, and BALF from each animal were cultured on 10 mL Brain-Heart Infusion broth (PanReac-AppliChem) overnight at 37 °C; 25 µL from these cultures were plated onto CLED, MacConkey, Mannitol Salt agar, and Sabouraud Dextrose Agar (all four from PanReac-AppliChem), and incubated for 24 h at 37 °C. To investigate anaerobic and anaerobic bacteria, 3 mL of blood were inoculated on 10 mL of BD BACTEC Lytic Anaerobic (Becton Dickinson) and incubated in BD BACTEC FX blood culture system (Becton Dickinson) during 5 days. If any sign of growth was detected, a subculture was made on Blood Chocolate and McConkey agar (both of them from Beckton Dickinson), and plates were incubated for 48 h at 37 °C in 5% CO2 atmosphere and on Brucella Blood Agar with Hemin and Vitamin K1 (Beckton Dickinson) incubated for 4 days at 37 °C in anaerobiosis. Bacterial species were identified using colony morphology and Gram stain. We used MALDI-TOF MS (Vitek®MS, Biomerieux) for advanced identification.
Histological Evaluation
Organ samples were fixed in 4% formalin for 24 h, embedded in paraffin, and cut into 4 μ sections for histological study. Slides were stained with hematoxylin-eosin and examined under light microscope. Slides were evaluated by two pathologists blinded to experimental groups. In all organs, the presence of bacteria inside vessels (microscopic observation of blue bacterial plungers inside the vessels, constituted by small rod-shapes), parenchymal disorganization, interstitial edema, leukocyte infiltration, tissue necrosis, and interstitial haemorrhage was evaluated. Lung injury was determined based on alveolar septa thickening and pleuritis. Heart damage was examined if inflammatory response was present in the epicardium and/or myocardium. Intestinal damage was evaluated at mucosal and serosal levels. Peritoneal injury was assessed based on a severity score of histopathological peritonitis [27], as scores of 0, 1, 2, and 3, according to findings in Table 2.
Statistical Analysis
Analyses were done using Statistical Package R 2019 version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria). To check the normality of quantitative variables, the Shapiro-Wilk test was used. Continuous variables are expressed as medians and 25th and 75th percentiles. Comparisons between more than two groups were performed using Kruskall-Wallis test, with Bonferroni correction for multiple comparisons when needed. Comparisons between two independent groups were performed using Mann–Whitney U test. Data are expressed as box-and whisker diagrams. All tests were two-tailed and statistical significance was considered at P < 0.05.
Results
A. faecalis A12C Safety
Healthy animals pretreated during a week with A. faecalis A12C (positive controls-1) and assessed at 7, 15, and 30 days after the first dose of A. faecalis A12C (HA7, HA15, and HA30) did not show significant changes in body temperature or weight, compared with negative controls-1 (supplementary data). Survival after A. faecalis A12C administration was 100% in all groups. No significant changes were found in most haematological (Table 3) and biochemical (Table 4) parameters. All positive controls-1 (HA7, HA15, HA30) had similar values compared with negative controls-1 (HC) with the exception of blood eosinophils, CREA and ASTL. An increase of eosinophils and CREA at 7 days after A. faecalis A12C administration was observed, followed by a progressive normalization. However, a significant decrease of ASTL was observed after the administration of A. faecalis A12C which was normalized throughout the study period (Table 3). No histological signs of injury were found in any organ of different groups.
Gut Colonization Conditions of A. faecalis A12C
In the positive controls-1 (HA7, HA15, and HA30), concentration of E. coli and A. faecalis A12C C in faeces showed a significant decrease in E. coli, parallel to an increase in A. faecalis A12C, 7 days after the administration of this strain (Fig. 2). Subsequently, E. coli concentration had a tendency to recover the initial values at 30 days, while A. faecalis A12C disappeared from the intestinal microbiota at 30 days.

Faeces concentration of E. coli and A. faecalis A12C at different times in groups treated with A. faecalis A12C and assessed at 0d, 0 days (just before administration of A. faecalis A12C), and 7d 7 days, 15d 15 days, and 30d 30 days, after the first dose of probiotic. Box and whisker diagrams depict the smallest observation, lower quartile, median, upper quartile, and largest observation.*P < 0.003, **P < 0.0005
Clinical Evolution
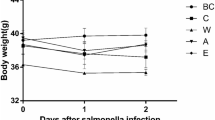
All animals in both groups (IA and IC) had a 100% survival at 15 days after the experiments. However, there was a greater presence of animals with signs of discomfort in IC group (negative control-2) compared with IA group (positive control-2). Ruffled fur was observed in all IC animals, and ocular discharge in 3 of them, while ruffled fur was only observed in 3 animals of the IA group. In both cases, the signs disappeared with analgesic treatment during the first 3 days post-inoculation. In Group IC, a not significant decrease in body weight was observed at day 15 compared with day 7. However, in group IA, a not significant increase was observed in the same period of time (Fig. 3). The only significant changes in serum biochemistry were an increase in ALTL, UREA, and eosinophils in IC respect to IA (Fig. 4).

Loss of bodyweight, expressed as difference in grams between weight just in the moment of E. coli inoculation (7 days), and at euthanatized time (15 days) a, or as percentage of grams lost during the same period of time b. IC Infected control group, IA Infected group pretreated with A. faecalis A12C. Box and whisker diagrams depict the smallest observation, lower quartile, median, upper quartile, and largest observation

Percentage of eosinophils and serum levels of urea, ALTL (alanine aminotransferase) and CRP (C reactive protein), in Infected Control Group (IC) and Infected group pretreated with A. faecalis A12C (IA). **P < 0.01, *P < 0.05
Microbiological Control
All animals from IC and IA had negative urine, BAL, and blood cultures at 7 days post-infection with E. coli, except for one animal in group IC in which Aerococcus viridans and Staphylococcus xylosus were isolated in the blood culture.
Histological Evaluation
In the IC group, four animals were classified with a peritonitis score of 1, and two rats with a score of 2. Dilatation of subserosal capillaries, dulling of peritoneal surface, and swelling of mesothelial cells and focal desquamation of mesothelial cells, thin exudative fibrin film, and mild-to-moderate mixed polymorphonuclear infiltrates were observed in these animals. These lesions were more evident in the peritoneum close to mesenteric lymph nodes, splenic hilum, and jejunum. However, lesions compatible with peritonitis were only found in one animal from group IA, which was scored with a value of 1. On other hand, except for the peritoneum, no significant histological changes were observed in any of the organs analysed in both groups. Representative histological lesions are showed in Fig. 5.

Representative histological images of hematoxilin and eosin stained sections of jejuna peritoneum a, b, mesenteric lymph nodes c, d, and splenic hilum e, f. Dulling of the peritoneal surface, and swelling of mesothelial cell (black arrow) in jejunal peritoneum a and splenic hilum peritoneum e, plus focal desquamation of mesothelial cells (white arrow) in splenic hilum peritoneum e. Mixed polymorphonuclear infiltrate (black arrow) in mesenteric lymphondes c, in a rat from IC group. No sign of inflammation or tissue alteration (red arrow) in peritoneal surface of jejunal peritoneum b, neither mesenteric lymph nodes d nor splenic hilum f in a rat from IA group. × 200 magnification a, b, c, d, and e; × 40 magnification f
Discussion
The major findings of our study are that A. faecalis A12C, isolated from Argyrosomus regius, is safe and has marked effects on the spread of infection in a clinically relevant experimental model of peritonitis. To the best of our knowledge, this is the first study exploring the probiotic effects of A. faecalis on clinical, biochemical, and pathological parameters in an animal model of peritonitis.
A variety of probiotic species have showed to benefit human and animal health, both in vivo and in vitro [9, 11,12,13, 16, 28,29,30]. Although lactic acid bacteria have been the most widely used group of probiotics in human and veterinary medicine, studies evaluating other bacterial species with possible probiotic use are increasingly frequent [14,15,16, 18]. A. faecalis is an aerobic, non-fermentative, oxidase-positive, non-encapsulated, Gram-negative rod [31]. It is the most frequently isolated member of the Alcaligenaceae family in the clinical laboratory, and it is present in soil and water, in human intestinal microbiota, and in hospital environments [31, 32]. Some strains have been reported as cause of sporadic nosocomial infections [33, 34]. Some studies refer to an eosinophilic response related to alveolitis in humans caused by A. faecalis inhalations [35]. Since most probiotic health benefits are strain specific, potential risks are also strain specific. Therefore, generalizing a health risk to probiotics as a class is incorrect, although we do not dispute that there are certain risk groups (e.g., severe immune-compromised patients) where probiotic use should be carefully monitored.
Several experimental and clinical studies reported a decrease in ASTL and ALTL by different probiotics [36,37,38], but we have not found evidence of an exclusive decrease in ASTL in groups of healthy animals treated with probiotics (positive controls-1) versus healthy animals without administration of probiotics (negative controls-1). It is plausible that A. faecalis A12C has a modulating capacity for lipid metabolism, as occurs with other probiotics [39,40,41]. However, this hypothesis should be evaluated in future studies. CRP is an acute phase protein released in hepatocytes after stimulation of IL-6 and IL-8 in response to acute inflammation, including viral infections, localized bacterial, and other inflammatory processes, and is involved in different immune functions. In both experimental and clinical studies on infectious diseases, it has historically been the reference biomarker of inflammatory response and infection [25, 27, 42]. In our study, CPR values, in conjunction with the absence of positive bacterial blood cultures, support the hypothesis that A. faecalis A12C offers safety against a possible spread of this microorganism and a potential risk of sepsis. The observation of a significant decrease in the concentration of E. coli after 7 days of administration of A. faecalis A12C, to a later recovery to initial concentrations once the administration of the probiotic ceases, is consistent with those reported by other authors [43]. Of note, other studies indicated that Lactobacillus spp and inulin supplementation in broilers decreased the numbers of E. coli and pH in ileum and cecum [44]. Although the reasons for this suppression are not clear, there are two potential reasons: (i) the decreased bacterial number may result from the inhibition of bacterial proliferation and (ii) a less bacterial infiltration or promoted bacterial killing [9, 45, 46].
Some authors have indicated that the route of infection can affect the host response. An immediate and overwhelming injection of bacteria into the peritoneum or blood compartments initiates rapid and distinct responses. A peritoneal infection will primarily induce inflammatory and immune-cell migration into the infected compartment, whereas a blood-borne model of infection will have the greatest immediate effect on endothelium and vascular system, with subsequent spread to organs. In case of blood inoculation with E. coli, rapid changes are noted in serum cytokine levels. However, inoculation of the peritoneal cavity with the same dose of E. coli does not generate a robust serum cytokine response [25]. In addition, it has been shown that in infectious peritonitis, the activity of interleukin-10 (IL-10) protects mice from death [47]. Perhaps those effects, together with the slight decrease in the concentration of our E. coli inoculums [4], are the reasons behind the zero mortality in our study.
Our model of sepsis was valid to evaluate the progression of sick animals. Infected animals not receiving A. faecalis A12C (IC) showed clear signs of discomfort, typical of bacterial infections such as ruffled fur, ocular discharge and weight loss [26]. When comparing haematological and biochemical data of animals pretreated with A. faecalis A12C inoculated with E. coli (IA), a marked reduction in blood eosinophils, urea, and ALTL occurred. These findings could be related to an anti-inflammatory and/or immunomodulatory capacity of A. faecalis A12C. Although we did not find inflammatory histopathological lesions in kidney or liver, we found moderate inflammation with polymorphonuclear infiltrates in the peritoneum and fatty tissue in rats from infected control group (negative control-2) or IC, which were significantly reduced in IA animals (positive control-2). This inflammatory improvement at the histological level has also been demonstrated with similar models of peritonitis evaluating different therapies, where the thickness of the peritoneal surface, the desquamation of the mesothelial cells, and the infiltrates of inflammatory cells were evaluated [27]. ALTL is more specific for liver damage than ASTL, because the former is located almost exclusively in the cytosol of the hepatocyte, while ASTL, in addition to the cytosol and mitochondria, is found in the heart, skeletal muscle, kidneys, brain, pancreas, lung, erythrocytes, and leukocytes [48]. The elevations in ALTL and urea in our study correlate with those obtained by other authors in similar models of peritonitis with or without probiotic evaluation. [13, 49]. These biochemical and haematological changes corresponded to an increase in CRP in IC when compared with IA groups. Our data suggest a potential anti-inflammatory/immunomodulatory effect of A. faecalis A12C.
The anti-inflammatory potency at the intestinal level of probiotics has been explained in experimental studies by several mechanisms [50], including suppression of apoptosis, epithelial cell proliferation and migration, increase colonic IL-10, or repair of disruptions of enteric neurotransmissions. β-glucans are glucose polymers of high molecular weight naturally present in the cell wall of living organisms such as bacteria, yeast, fungus, and plants. They are recognized by the innate immune system. This recognition plays important roles in host defense and represents specific opportunities for clinical modulation of the host immune response [51]. Some authors have examined the effects of curdlan, a β-(1-3)- glucan derived from A. faecalis, on allergic airway inflammation using a murine model of asthma, and suggest that curdlan is capable of inducing IL-10-producing CD4+ T cells and inhibiting the development of eosinophilic airway inflammation [52]. This finding could have some similarity with the decrease of eosinophils in IA animals.
Our study has some limitations and strengths. First, a higher sample size could provide more robust results. Second, we do not know the possible effects that A. faecalis A12C may cause in animals after 7 days of its administration and the safety and efficacy at different doses. Third, although the use of a semiquantitative scoring system, as the one used in this study for histological evaluation, is quite common, we are aware that such score does not provide a fully quantitative assessment of histopathological alterations, as a morphometrical assessment would do. However, the major strength of this study is that we used a translational model of peritonitis that allowed us to obtain results of clinical relevance with a global vision of the potential therapeutic role of an A. faecalis strain.
In summary, our findings suggest that A. faecalis A12C could influence clinically relevant parameters in sepsis. Administration of 6 × 108 CFU/mL for 7 days was associated with a lesser spread of infection. Our study may add a piece to the complex puzzle of bacteria-host interactions and new therapeutic possibilities in the prophylaxis of sepsis. However, future studies are necessary to analyse these parameters in more detail.
Data Availability
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Hecker A, Reichert M, Reuß CJ et al (2019) Intra-abdominal sepsis: new definitions and current clinical standards. Langenbeck’s Arch Surg 404:257–271. https://doi.org/10.1007/s00423-019-01752-7
Singer M, Deutschman CS, Seymour C et al (2016) The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA - J Am Med Assoc 315:801–810. https://doi.org/10.1001/jama.2016.0287
Qin HL, Shen TY, Gao ZG et al (2005) Effect of lactobacillus on the gut microflora and barrier function of the rats with abdominal infection. World J Gastroenterol 11:2591–2596. https://doi.org/10.3748/wjg.v11.i17.2591
Shukla P, Verma AK, Dwivedi P et al (2014) Moxifloxacin-loaded nanoemulsions having tocopheryl succinate as the integral component improves pharmacokinetics and enhances survival in E. coli-induced complicated intra-abdominal infection. Mol Pharm 11:4314–4326. https://doi.org/10.1021/mp5003762
Bouza C, López-Cuadrado T (2019) Epidemiology and trends of sepsis in young adults aged 20–44 years: a nationwide population-based study. J Clin Med 9:77. https://doi.org/10.3390/jcm9010077
Bosscha K, Reijnders K, Hulstaert PF et al (1997) Prognostic scoring systems to predict outcome in peritonitis and intraabdominal sepsis. Br J Surg 84:1532–1534. https://doi.org/10.1002/bjs.1800841110
Blanco J, Muriel-Bombín A, Sagredo V et al (2008) Incidence, organ dysfunction and mortality in severe sepsis: a Spanish multicentre study. Crit Care 12:1–14. https://doi.org/10.1186/cc7157
Martín-Barrasa JL, Cordovez CM, De Los MY, Zayas AE et al (2015) Rectal pre-treatment with ozonized oxygen (O3) aggravates clinic status in septic rats treated with amoxicillin/clavulanate. Enfermedades Infecc y Microbiol Clin Monogr 33:469–475. https://doi.org/10.1016/j.eimc.2014.09.006
Gao QY, Bin LH, Li DH, Wu SW (2013) Probiotics improve survival of septic rats by suppressing conditioned pathogens in ascites. World J Gastroenterol 19:4053–4059. https://doi.org/10.3748/wjg.v19.i25.4053
Bielecka M (2006) Probiotics in food Chem Funct Prop Food components, Third Ed 413–426. https://doi.org/10.1201/9781420009613.ch16
Aceti A, Maggio L, Beghetti I et al (2017) Probiotics prevent late-onset sepsis in human milk-fed, very low birth weight preterm infants: systematic review and meta-analysis. Nutrients 9:1–21. https://doi.org/10.3390/nu9080904
Lazarenko L, Babenko L, Sichel LS et al (2012) Antagonistic action of Lactobacilli and Bifidobacteria in relation to Staphylococcus aureus and their influence on the immune response in cases of intravaginal staphylococcosis in mice. Probiotics Antimicrob Proteins 4:78–89. https://doi.org/10.1007/s12602-012-9093-z
Gancarčíková S, Nemcová R, Popper M et al (2019) The influence of feed-supplementation with probiotic strain Lactobacillus reuteri CCM 8617 and alginite on intestinal microenvironment of SPF mice infected with Salmonella typhimurium CCM 7205. Probiotics Antimicrob Proteins 11:493–508. https://doi.org/10.1007/s12602-018-9413-z
Foulquié Moreno MR, Sarantinopoulos P, Tsakalidou E, De Vuyst L (2006) The role and application of enterococci in food and health. Int J Food Microbiol 106:1–24. https://doi.org/10.1016/j.ijfoodmicro.2005.06.026
Pabari K, Pithva S, Kothari C et al (2020) Evaluation of probiotic properties and prebiotic utilization potential of Weissella paramesenteroides isolated from fruits. Probiotics Antimicrob Proteins 12:1126–1138. https://doi.org/10.1007/s12602-019-09630-w
Xiao Z, Liu L, Tao W et al (2018) Clostridium tyrobutyricum protect intestinal barrier function from LPS-induced apoptosis via P38/JNK signaling pathway in IPEC-J2 cells. Cell Physiol Biochem 46:1779–1792. https://doi.org/10.1159/000489364
Annamalai N, Kumar A, Saravanakumar A et al (2011) Characterization of protease from Alcaligens faecalis and its antibacterial activity on fish pathogens. J Environ Biol 32:781–786
Román L, Real F, Sorroza L et al (2012) The in vitro effect of probiotic Vagococcus fluvialis on the innate immune parameters of Sparus aurata and Dicentrarchus labrax. Fish Shellfish Immunol 33:1071–1075. https://doi.org/10.1016/j.fsi.2012.06.028
Ringø E, Bendiksen HR, Wesmajervi MS et al (2000) Lactic acid bacteria associated with the digestive tract of Atlantic salmon (Salmo salar L.). J Appl Microbiol 89:317–322. https://doi.org/10.1046/j.1365-2672.2000.01116.x
Ringø E, Hoseinifar SH, Ghosh K et al (2018) Lactic acid bacteria in finfish-An update. Front Microbiol 9:1–37. https://doi.org/10.3389/fmicb.2018.01818
Irianto A, Austin B (2003) Use of dead probiotic cells to control furunculosis in rainbow trout, Oncorhynchus mykiss (Walbaum). J Fish Dis 26:59–62. https://doi.org/10.1046/j.1365-2761.2003.00414.x
Gutiérrez-Falcón A, Padilla D, Ramos Sosa MJ et al (2020) Characterization in vitro of new bacterial strains showing potentially probiotic crossed effect against vibriosis in relevant fish species for marine aquaculture. J Appl Anim Res 48:553–558. https://doi.org/10.1080/09712119.2020.1844714
Nicklas W, Baneux P, Boot R et al (2002) Recommendations for the health monitoring of rodent and rabbit colonies in breeding and experimental units. Lab Anim 36:20–42. https://doi.org/10.1258/0023677021911740
Bizzini A, Greub G (2010) Matrix-assisted laser desorption ionization time-of-flight mass spectrometry, a revolution in clinical microbial identification. Clin Microbiol Infect 16:1614–1619. https://doi.org/10.1111/j.1469-0691.2010.03311.x
Buras JA, Holzmann B, Sitkovsky M (2005) Model organisms: animal models of sepsis: setting the stage. Nat Rev Drug Discov 4:854–865. https://doi.org/10.1038/nrd1854
Acred P, Hennessey TD, Macarthur-Clark JA et al (1994) Guidelines for the welfare of animals in rodent protection tests: a report from the Rodent Protection Test Working Party. Lab Anim 28:13–18. https://doi.org/10.1258/002367794781065870
Uzunköy A, Özardali I, ÇelIk H, Demirci M (2012) Karbondioksit pnömoperitonyumun peritonitin şiddeti üzerine etkisi. Ulus Travma ve Acil Cerrahi Derg 18:99–104. https://doi.org/10.5505/tjtes.2012.53503
Pratt C, Campbell MD (2019) The effect of bifidobacterium on reducing symptomatic abdominal pain in patients with irritable bowel syndrome: a systematic review. Probiotics Antimicrob Proteins. https://doi.org/10.1007/s12602-019-09609-7
Román L, Acosta F, Padilla D et al (2015) The invitro immunomodulatory effect of extracellular products (ECPs) of Vagococcus fluvialis L21 on European sea bass (Dicentrarchus labrax) leucocytes. Fish Shellfish Immunol 42:517–521. https://doi.org/10.1016/j.fsi.2014.11.037
Gao C, Ganesh BP, Shi Z et al (2017) Gut microbe-mediated suppression of inflammation-associated colon carcinogenesis by luminal histamine production. Am J Pathol 187:2323–2336. https://doi.org/10.1016/j.ajpath.2017.06.011
Tena D, Fernáandez C, Lago MR (2015) Alcaligenes faecalis: an unusual cause of skin and soft tissue infection. Jpn J Infect Dis 68:128–130. https://doi.org/10.7883/yoken.JJID.2014.164
Basharat Z, Yasmin A, He T, Tong Y (2018) Genome sequencing and analysis of Alcaligenes faecalis subsp. phenolicus MB207. Sci Rep 8:1–10. https://doi.org/10.1038/s41598-018-21919-4
Aisenberg G, Rolston KV, Safdar A (2004) Bacteremia caused by Achromobacter and Alcaligenes species in 46 patients with cancer (1989–2003). Cancer 101:2134–2140. https://doi.org/10.1002/cncr.20604
Kavuncuoglu F, Unal A, Oguzhan N et al (2010) First reported case of Alcaligenes faecalis peritonitis. Perit Dial Int 30:118–119. https://doi.org/10.3747/pdi.2009.00058
Milanowski J, Dutkiewicz J, Potoczna H et al (1998) Allergic alveolitis among agricultural workers in eastern Poland: a study of twenty cases. Ann Agric Environ Med 5:31–43
Huang H, Lin Z, Zeng Y et al (2019) Probiotic and glutamine treatments attenuate alcoholic liver disease in a rat model Exp Ther Med 4733–4739. https://doi.org/10.3892/etm.2019.8123
Neag MA, Catinean A, Muntean DM et al (2020) Probiotic bacillus spores protect against acetaminophen induced acute liver injury in rats. Nutrients 12:1–16. https://doi.org/10.3390/nu12030632
Kobyliak N, Abenavoli L, Mykhalchyshyn G et al (2018) A multi-strain probiotic reduces the fatty liver index, cytokines and aminotransferase levels in NAFLD patients: Evidence from a randomized clinical trial. J Gastrointest Liver Dis 27:41–49. https://doi.org/10.15403/jgld.2014.1121.271.kby
Ooi LG, Liong MT (2010) Cholesterol-lowering effects of probiotics and prebiotics: a review of in Vivo and in Vitro Findings. Int J Mol Sci 11:2499–2522. https://doi.org/10.3390/ijms11062499
Martorell P, Llopis S, González N et al (2016) Probiotic strain Bifidobacterium animalis subsp. lactis CECT 8145 reduces fat content and modulates lipid metabolism and antioxidant response in Caenorhabditis elegans. J Agric Food Chem 64:3462–3472. https://doi.org/10.1021/acs.jafc.5b05934
Dehkohneh A, Jafari P, Fahimi H (2019) Effects of probiotic Lactobacillus paracasei TD3 on moderation of cholesterol biosynthesis pathway in rats. Iran J Basic Med Sci 22:1004–1009. https://doi.org/10.22038/ijbms.2019.33933.8073
Julián-Jiménez A, Candel FJ, González-Del Castillo J (2017) Uselfulness of biomarkers to predict bacteremia in patients with infection in the emergency department. Rev Esp Quimioter 30:245–256
Liu Q, Ni X, Wang Q et al (2017) Lactobacillus plantarum BSGP201683 Isolated from giant panda feces attenuated inflammation and improved gut microflora in mice challenged with enterotoxigenic Escherichia coli. Front Microbiol 8:1–12. https://doi.org/10.3389/fmicb.2017.01885
Wu XZ, Wen ZG, Hua JL (2019) Effects of dietary inclusion of Lactobacillus and inulin on growth performance, gut microbiota, nutrient utilization, and immune parameters in broilers. Poult Sci 98:4656–4663. https://doi.org/10.3382/ps/pez166
Sokol H, Pigneur B, Watterlot L et al (2008) Faecalibacterium prausnitzii is an anti-inflammatory commensal bacterium identified by gut microbiota analysis of Crohn disease patients. Proc Natl Acad Sci U S A 105:16731–16736. https://doi.org/10.1073/pnas.0804812105
Ivanov II, Atarashi K, Manel N et al (2009) Induction of intestinal Th17 cells by segmented filamentous bacteria. Cell 139:485–498. https://doi.org/10.1016/j.cell.2009.09.033
van der Poll T, Marchant A, Buurman WA et al (1995) Endogenous IL-10 protects mice from death during septic peritonitis. J Immunol 155:5397–5401
Giannini EG, Testa R, Savarino V (2005) Liver enzyme alteration: A guide for clinicians. CMAJ 172:367–379. https://doi.org/10.1503/cmaj.1040752
Lee MJ, Kim K, Jo YH et al (2016) Dose-dependent mortality and organ injury in a cecal slurry peritonitis model. J Surg Res 206:427–434. https://doi.org/10.1016/j.jss.2016.08.054
Martín R, Chain F, Miquel S et al (2017) Using murine colitis models to analyze probiotics-host interactions. FEMS Microbiol Rev 41:S49–S70. https://doi.org/10.1093/femsre/fux035
Kankkunen P, Teirilä L, Rintahaka J et al (2010) (1,3)-β-Glucans activate both Dectin-1 and NLRP3 inflammasome in human macrophages. J Immunol 184:6335–6342. https://doi.org/10.4049/jimmunol.0903019
Kawashima S, Hirose K, Iwata A et al (2012) β-Glucan Curdlan induces IL-10–producing CD4 + T cells and inhibits allergic airway inflammation. J Immunol 189:5713–5721. https://doi.org/10.4049/jimmunol.1201521
Acknowledgements
We would like to thank Mr. Juan Ramirez Verona from the Illustration and Iconography Service at Hospital Universitario de Gran Canaria Dr. Negrín, and Mr. Miguel Martín Betancor from University of Applied Sciences, Berlin, for their technical assistance.
Funding
This study was funded in part by grants from the Fundación Canaria de Investigación Sanitaria, Spain (PIFUN30/18), and by Ministerio de Economía y Competitividad, Spain (AGL2014-54683-R). A.G.F. was a recipient of a predoctoral grant from the University of Las Palmas de Gran Canaria (PIFULPGC-2015-CCSALUD). The funding agencies have no role in the design of the study, collection, analysis or interpretation of data, or in the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization: Martín-Barrasa JL, Padilla Castillo DF, Real Valcárcel F; Methodology: Gutiérrez Falcón AI, Martín-Barrasa JL, Ramos-Nuez AM, Padilla Castillo DF, Bordes Benítez A, Domínguez Cabrera C, Martín Caballero J, Villar J; Experiments and Data analysis: Martín-Barrasa JL, Gutiérrez Falcón AI, Espinosa de los Monteros y Zayas A, Rivero-Vera JC, Ramos-Nuez AM, García-Laorden MI, Chamizo López FJ, Artiles Campelo F, Nogueira Salgueiro P, González-Martín JM; Writing the manuscript and reviewing: Martín-Barrasa JL, Martín Caballero J, Villar J, Frías Beneito R; Funding: Martín-Barrasa JL, Real Valcárcel F; Resources: Martín-Barrasa JL, Real Valcárcel F, Bordes Benítez A, Domínguez Cabrera C, Espinosa de los Monteros y Zayas A, Villar J; Supervision: Martín-Barrasa JL. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
The animal trial was carried out according to the regulations approved by the Animal Care Committee of Hospital Universitario de Gran Canaria, Dr. Negrín (Cod. REGA: ES 350160024512).
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gutiérrez-Falcón, A.I., Ramos-Nuez, A.M., de los Monteros y Zayas, A.E. et al. Probiotic Properties of Alcaligenes faecalis Isolated from Argyrosomus regius in Experimental Peritonitis (Rat Model). Probiotics & Antimicro. Prot. 13, 1326–1337 (2021). https://doi.org/10.1007/s12602-021-09767-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12602-021-09767-7