
Abstract
While blood is crucial for many surgeries and patient treatments worldwide, it cannot be produced artificially. Fulfilling the demand for blood products on average days is already a major challenge in countries like South Africa and Ghana. In these countries, less than 1 % of the population donates blood and most of the donations come from first-time donors who do not return. Sufficient new, first-time and even lapsed donors must be motivated to donate regularly. This study argues that blood donation behavior change support systems (BDBCSS) can be beneficially applied to support blood donor management in African countries. In this study, the design science research (DSR) approach is applied in order to derive generic design principles for BDBCSS and instantiate the design knowledge in prototypes for a blood donation app and a chatbot. The design principles were evaluated in a field study in South Africa. The results demonstrate the positive effects of BDBCSS on users’ intentional and developmental blood donation behavior. This study contributes to research and practice by proposing a new conceptualization of blood donation information systems support and a nascent design theory for BDBCSS that builds on behavioral theories as well as related work on blood donation information systems. Thus, the study provides valuable implications for designing preventive health BCSS by stating three design principles for a concrete application context in healthcare.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Blood is a very important resource in all healthcare systems worldwide, crucial for many surgeries and certain types of treatments. Unfortunately, blood products cannot be produced artificially, but blood must be donated by volunteers. As blood products also only have a short shelf-life, fulfilling the demand for blood products on average days is a major challenge in countries like South Africa and Ghana (Vermeulen et al. 2019). Already pre-COVID, less than 1 % of the population donated blood (SANBS 2023). Donor management is therefore one of the most important, but at the same time one of the most challenging tasks within the blood supply chain. Not least due to the COVID-19 pandemic, donation numbers have decreased, increasing the shortage of blood products (SANBS 2020). As Dei-Adomakoh et al. (2021, p. 770) stated, "the low recruitment and retention of blood donors in sub-Saharan Africa is a grave concern for blood transfusion services in the region". Overall, of the 60 countries reporting to the World Health Organization (WHO) that they collect less than ten units of blood per 1000 people of the population, which is the minimum recommendation of the WHO, more than half (34), including Ghana, are located in Africa (WHO 2023). In Ghana, of the 300,000 blood donations required every year, only around 60 % are collected, which is mainly due to the loss of first-time donors (Asamoah-Akuoko et al. 2021). Only 15.2 % of them continue donations within 6 months, primarily due to lack of information when and where to donate again. In South Africa, donations by first-time donors further decreased as education programs were shortened significantly during COVID-19. Therefore, it is important for blood services in Ghana and South Africa to recruit a significant number of new (young) donors every year to make up for donors becoming lapsed donors. In addition, they must motivate first-time and lapsed donors to voluntarily donate blood on a regular basis (again). When donations exceed the demand, they will be wasted, though, which should also be avoided. Matching demand and donations as closely as possible is therefore crucial.
While this should be addressed from both sides, the demand side will remain very stochastic (e.g., emergencies are difficult to forecast) and external events like the pandemic can additionally increase the complexity. Therefore, we argue for the importance of donor mobilization and management to enable sufficient supply and prevent "over-donation" as well as for new approaches that are necessary to engage with and provide access and information to all groups of donors. We can distinguish four types of donor groups: regular (rd), lapsed (ld), first-time (fd) and non-donors (nd) (Ferguson 1996). Each group is characterized by different needs and preferences that have to be addressed to reach all types of donors.
The transition to and the retention of regular blood donors requires a long-term relationship with the donor. Digital tools like chatbots can not only support educational programs through their easy access to any kind of information (e.g., current demand, requirements and potential risks) when on-site visits are not possible, but they can also serve as a persuasive and natural way to keep donors engaged (Müller and Reuter-Oppermann 2024). Diederich et al. (2019b) demonstrated that inducing behavior can be achieved by conversations with a chatbot when designed appropriately. Integrated into a blood donation app which allows for additional functionalities for the individual types of donors, by means of a well-known framework for the design and evaluation of persuasive systems (Oinas-Kukkonen and Harjumaa 2009), our previous research has shown both systems’ overall persuasiveness in terms of inducing changes in blood donor behavior (Müller and Reuter-Oppermann 2023b). Since this is achieved without forcing or deceiving the user, they belong to the class of behavior change support systems (BCSS) (Oinas-Kukkonen 2013). According to Oinas-Kukkonen (2013), BCSS are defined as socio-technical systems whose design is deliberately aimed at forming (in our case: nd), altering (in our case: fd and ld) or strengthening (in our case: rd) user behavior.
In the healthcare sector, research interest is increasingly shifting from extensive infrastructural healthcare information and management systems to those enabling individuals to participate proactively (Baird et al. 2020). According to the literature review of Orji and Moffatt (2018), these so-called health behavior change support systems are predominantly used for health promotion and prevention, followed by disease management. Examples for preventive BCSS are virtual coaches (Tropea et al. 2019; Weimann et al. 2022) and digital therapeutics (Makin 2019; Fürstenau et al. 2023) that keep users engaged by providing personalized health recommendations and using appropriate human-like software design features, also called social cues. However, an individual’s health generally not only depends on his/her own behavior, but also on the behavior of others in ways that can affect his/her health negatively (e.g., by passive smoking) or positively (e.g., by receiving donated blood). The latter requires adequate matching of the right donor with the right blood group to the right patient. With the help of BCSS targeting blood donor behavior, when a patient is in need of a specific blood group, individual messages can be sent to matching donors, making them feel unique. By enabling this shift in recruitment strategy, blood donation behavior change support systems (BDBCSS) also belong to health promotion and prevention approaches which meet patients’ needs by steering the scarce resource of blood. In addition, the worldwide blood supply challenges in line with the prevalence of minority groups due to increasing migration (i.e., requiring special blood groups) and aging populations due to demographic changes (i.e., requiring more transfusions and reducing the eligible donor pool) described by van Dongen et al. (2016) can be better addressed. Besides, as blood donation behavior represents prosocial behavior, i.e., benefiting other people instead of oneself (Straub 1978), BCSS targeting blood donor behavior imply a bigger design challenge in terms of user engagement compared to other preventive health BCSS.
To address this challenge, we apply the design science research (DSR) approach in order to derive generic design principles for BDBCSS and instantiate the design knowledge in prototypes for a blood donation app and a chatbot. Consequently, we aim to answer the following research question: How to design BDBCSS to sustainably mobilize and support all types of blood donors regardless of their blood donation culture?
We ground our design on two research streams, namely behavioral change models representing theoretical frameworks as well as blood donation information systems in research and practice, and propose three overarching design principles for BDBCSS. To increase the relevance of our research, throughout the project we collaborated with experts from three blood services from those regions, the National Blood Service Ghana (NBSG), the Western Cape Blood Service (WCBS) in South Africa and the South African National Blood Service (SANBS) that provides its service to all of South Africa’s provinces except of the Western Cape province. The final evaluation was performed by means of a survey-based field study on site at WCBS. We executed our research as part of the research project BISKIT that was funded by the German Federal Ministry of Education and Research (BMBF). Within the BISKIT project, an information and decision support system for blood supply chain management in South Africa and Ghana was developed (Horstkemper and Reuter-Oppermann 2022). While the project originally focused on the blood services themselves, it became evident that access to and support for blood donors is equally important in order to meet patient needs, especially in post-pandemic times. According to WCBS, in South Africa’s Western Cape region alone, around 700 units of whole blood must be collected every day to meet the demand. Since COVID-19, on average only 500 units have been collected daily. One reason for this is the shortage of educational programs at schools, where recruiters managed to obtain 8 % of blood donors before COVID-19 in 2019, which decreased to only 1 % in 2020. Consequently, we address a practically relevant real-world problem with our research.
The remainder of this work is structured as follows. The next section summarizes the related work and theoretical foundations. Then, we present the DSR project and elaborate on the design requirements and principles. The following section deals with the evaluation. After a discussion of the findings and the limitations of our work, the paper closes with a conclusion and an outlook on future research.
2 Related Work and Theoretical Foundations
Our DSR project carried out based on the DSR framework of Kuechler and Vaishnavi (2008) contributes to solving the design problem of crafting user-centered BDBCSS for the transition to and retention of regular blood donors. The BDBCSS design is grounded on two research streams: blood donation information systems in research and practice as well as behavioral change models representing theoretical frameworks. Our overall research background is depicted in Fig. 1 and explained in more detail at the end of this section. In the following, we first describe the blood donation information systems in research and practice and afterwards our BDBCSS design’s underlying behavioral theories.

Research background
2.1 Blood Donation Apps and Chatbots in Research and Practice
The American National Red Cross (2022a), for instance, offers an app that enables users to schedule and manage appointments, find nearby blood donation centers, transfer relevant data prior to appointments, review their donation history and track the journey of their donated blood until it is used for transfusion. Using the app, donors can also earn achievement badges that can be shared with friends.
Similarly, the German Red Cross (DRK) (DRK-Blutspendedienste 2022) provides an app with comparable features. However, this app does not facilitate data transfer or enable donation tracking. Instead, it provides real-time information on when the next donation is allowed again and offers appointment reminders via email. Additionally, it includes an integrated chat forum where users can interact with other blood donors in Germany.
Combining the functionalities of both apps, the “Statusplus Blutspende” app goes one step further by also connecting hospitals. This allows users to have access to their blood values, monitor the current blood supply and receive push notifications for blood donation appeals if necessary (Schäfer 2020). Currently, this app is utilized in Lübeck and Kiel. In the future, “Statusplus Blutspende” aims to enable digital completion of donor questionnaires in order to reduce administrative workload at blood donation centers by half the average processing time. This particular feature, along with others mentioned, is already available in the “Mein Blut” app of the Austrian Red Cross (Oesterreichisches Rotes Kreuz 2022).
Regarding our blood service partners, WCBS has already introduced an app which is still evolving but already accessible for donors in the Google Play Store. However, WCBS reported to us that overall downloads are lower than expected and an improvement is necessary. To date, donors are able to check WCBS’s blood stock levels, read the locations of WCBS’s donation centers as well as patient success stories and look up their blood donation data such as their own blood group, their overall number of blood donations and when they are allowed to donate again. For the latter, they also have the option to set reminders via email. For a comprehensive overview of various blood donation apps used worldwide, we recommend the publication of Ouhbi et al. (2015).
From a research perspective, Sardi et al. (2019b) have been the first to apply the transtheoretical model with regard to the development of blood donation apps. In terms of the design of such apps, however, they mainly focused on the gamification part. They applied the transtheoretical model to ensure the usefulness of their gamified design suggestions for all four blood donor types. That is why we decided to build upon their innovative work by extending the design suggestions and theoretical justification for the complete app.
While apps are used by manually activating existing elements on a graphical interface, the interaction with chatbots is rather intuitive due to their conversational interface enabling input in natural language (McTear et al. 2016). With their roots in healthcare via the psychotherapeutic chatbot ELIZA (Weizenbaum 1966), it is not surprising that users can get the feeling of a human contact and assign personalities to chatbots to which they respond socially even if equipped with only rudimentary human-like cues (Nass et al. 1994; Nass and Moon 2000). According to this phenomenon known as “Computers Are Social Actors” (CASA) paradigm (Nass et al. 1994), these subconscious user responses exhibiting social behavior come from social cues elicited by design features derived from interpersonal communication (e.g., emojis and small talk) (Feine et al. 2019; Gnewuch et al. 2017). Besides in healthcare, chatbots are used in various domains such as customer service and enterprise applications in many industries like banking, air travel and entertainment to support users in searching for relevant information and to automate easy tasks like checking the calendar for booking an appointment (Morana et al. 2017). Apart from domain-specific use, they can also be applied as general-purpose technology such as ChatGPT depending on their scope of application (Gnewuch et al. 2017). By running cost efficiently and offering short resolution times 24/7, chatbots offer advantages to their providers as well as their users (Gnewuch et al. 2017). Being easily implemented on websites and messenger platforms, often used as messaging apps on smartphones for many different application cases, chatbots are spreading rapidly.
However, to the best of our knowledge, there is only little research and practice on chatbots for blood donors. Among them are the chatbot designed by Roman et al. (2020) for a Brazilian blood donation center represented in the center’s mascot that is accessible via Google Assistant, the Facebook Messenger bots of the Canadian Blood Services (Canadian Blood Services 2017) and the Indian start-up BloodLink (Mayroth 2017) as well as “Clara”, the chatbot of the American National Red Cross appearing on its website in the form of a female doctor (The American National Red Cross 2022b). By enabling free text input and providing guidance to the user in the form of buttons and website links, they are all able to educate and mobilize donors.
Even though the aforementioned chatbots are partly represented by avatars and names, overall they only use very few social cues (e.g., no use of small talk, response delays and emojis). This may lead to a lower social presence of the chatbot which negatively influences the quality of interaction (Nass and Moon 2000). In addition, they interact only rarely with the user, just reactively for a quick exchange of information limited to answer specific questions about blood donation and its process as well as making appointments. In contrast, we not only equip our chatbot with a broader and purposefully selected set of social cues, but we are the first who plan its integration into a blood donation app to provide the user with a holistic set of features in order to ensure long-term donor engagement. For addressing this, it is necessary to understand issues related to blood donors. That is why we used behavioral theories to justify our design decisions, which is often lacking in research and practice underlying existing blood donation information systems.
2.2 Behavioral Change Models in the Context of Blood Donation
2.2.1 Theory of Planned Behavior (TPB)
A key theory underlying the prediction of blood donation behavior is the theory of planned behavior (Ajzen 1991). The TPB posits that three determinants, which are mediated by the individual’s behavioral intention, influence changes in behavior: attitude, subjective norm and perceived behavioral control. With regard to the decision-making process of donating blood, attitude reflects the individual’s weighing of pros (such as saving lives of patients in need of blood and being a role model for others) and cons (such as revealed ineligibility to give blood and physical reactions) of donating blood (Burditt et al. 2009). Subjective norm refers to the individual’s perception of blood donation being (un)approved by significant others like friends and family members and perceived behavioral control to its judgment of how easy or difficult donating blood might be.
The impact of the mediator intention differs depending on the donor group (i.e., nd, fd, ld, rd) the individual belongs to: the more experience in donating blood, the smaller the role is that intention plays in predicting behavior (Ferguson and Bibby 2002; Godin et al. 2007). This means, while regular donors made blood donation a habit, the behavior of the other types of donors is mainly influenced by their motivation to give blood. However, past behavior as another main determinant underlying blood donation experience is not considered by the TPB, which is why the theory has been extended by other scholars (e.g., Godin et al. 2005). Despite these extensions and due to the rather cognitive perspectives, the development and progress of the individual’s blood donation behavior change is still hard to predict (Masser et al. 2008).
2.2.2 Transtheoretical Model (TTM)
Another theoretical framework applicable to predict blood donor behavior and complementary to the commonly used TPB is the transtheoretical model (Prochaska and DiClemente 1982) which covers stage perspectives (Amoyal et al. 2013; Burditt et al. 2009; Ferguson and Chandler 2005; Sardi et al. 2019a). The TTM hypothesizes different stages of change (SOC) which the individual goes through during the behavior change process as well as processes of change (POC) that facilitate transitions between the SOC (see Fig. 2). With regard to blood donation, the stage of change describes how ready and willing the individual is to give blood. Overall, the TTM comprises five SOC (precontemplation, contemplation, preparation, action, maintenance) and ten POC, which can be divided into experiential and behavioral transition strategies. According to Ferguson and Chandler (2005), the developmental process of a blood donor career starts with the experiential (see Fig. 2 in the middle on the right, adjacent to the beginner side of the cycle) and ends with the behavioral strategies (see Fig. 2 in the middle on the left, adjacent to the more advanced side of the cycle). Ferguson and Chandler (2005) also demonstrated the matching of blood donor careers and SOC. Accordingly, non-donors are in the precontemplation stage, first-time and lapsed donors are in the contemplation/preparation stages and regular donors are in the action/maintenance stages.

Stages and processes of change in the context of blood donation
The two theories, TPB and TTM, are not only complementary to each other, but also interplay with each other. Research has shown that the determinants of the TPB relate to the SOC of the TTM, i.e., attitude is particularly relevant in earlier stages (e.g., precontemplation) and subjective norm as well as perceived behavioral control have more relevance when transiting through later stages (e.g., France et al. 2014; Vries et al. 1998). The high relevance of attitude at the beginning of a donor career might be due to the stronger impact of negative aspects of donating blood compared to positive ones with disadvantages clearly outweighing advantages in the precontemplation stage and the exact opposite occurring in the preparation and action/maintenance stages (i.e., no clear trend in one direction or the other between contemplation and preparation stages) (Burditt et al. 2009). Passing through the stages, the cons of donating blood become less relevant, whereas the pros gain significantly more relevance at least across the first three SOC, as in the action/maintenance stages habitually donating blood probably means taking the advantages for granted (Burditt et al. 2009).
2.2.3 User Archetypes of Blood Donors
For the user-centered design of BDBCSS, it is essential to know the particular user groups and have an all-embracing understanding of the respective blood donor behavior in order to provide targeted support and induce behavioral changes if necessary (Oinas-Kukkonen 2013). Due to the high abstractness of theories, we therefore derived and developed an adapted model in the form of user archetypes in addition to and on the basis of the interplay between the TPB and TTM by including further intuitive aspects which are more real-world oriented as well as consistent with the literature (e.g., Bednall et al. 2013; Ferguson 1996) and validated by our blood service collaborators (see Table 1) (Floyd et al. 2008). For instance, an individual’s attitude (TPB) towards donating blood depends on how educated s/he is in terms of blood donation and its benefits. The user archetypes refer to the four types of donor groups that can be distinguished in the context of blood donation: non-, first-time, lapsed and regular donors (Ferguson 1996). To reach all types of donors, the BDBCSS design must be tailored to the different motives, challenges and needs of each donor group as depicted in Table 1.
2.2.4 Basic Psychological Needs Satisfaction (BPNS) as Behavior Change Initiator
According to the self-determination theory (SDT) (Deci and Ryan 1985, 2000), motivation for a certain behavior including behavioral changes per se requires that the individual’s basic psychological needs (BPN) are met. This is particularly true with regard to blood donation behavior (Gagné 2003). As donating blood is a purely prosocial behavior, which means it benefits other people (i.e., saving patients’ lives) through certain actions (i.e., giving blood) (Straub 1978), the non-BPNS more likely leads to the individual’s engagement in selfish behaviors lacking the orientation towards others. Deci and Ryan (1985) SDT postulates that there are three complementary BPN: relatedness, competence and autonomy. Within a social milieu, the authors assume that human beings pursue their innate motivational tendency to feel connected to others (i.e., relatedness), to generally be effective (i.e., competence) and at the same time personally autonomous and proactive (i.e., autonomy). In the context of blood donation, BPNS means that the individual feels connected to and supported by others who donate (i.e., relatedness), confident and self-effective in its ability to donate (i.e., competence) as well as free and in control over the decision to donate (i.e., autonomy) (France et al. 2017).
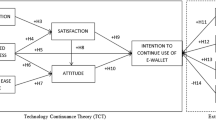
With regard to motivated behavior, according to Hagger et al. (2006), SDT (global-level) and TPB (situational-level) are related in the way that global BPNS influences the individual’s engagement in a specific activity at a particular time. Moreover, BPNS is not only the prerequisite for intentional (TPB - situational-level) but also for developmental (TTM - processual-level) blood donor behavior, which can vary individually (user archetypes - human-level) (see Fig. 1). Therefore, the BDBCSS design needs to ensure BPNS and address each of the three BPN to foster the individual’s motivation needed for intentional as well as developmental blood donor behavior depending on the individual. Through using the implications of the mentioned theoretical frameworks with their different perspectives on behavior as well as behavior change and their origin from a global-level perspective, we respond to the call of empirical blood donation researchers (e.g., Sinclair et al. 2010) and Elliot et al. (2002, p. 373) which have stated that “needs and motives can and often do lead directly to behavior, but these general dispositional desires sometimes need to be strategically channeled in a specific direction to be satisfied in an effective and efficient manner”. Against this background, we argue that it is suitable to apply the DSR methodology.
3 Design Science Research Project
To address our research question and to respond to the call by Burditt et al. (2009) for more theory-based blood donor recruitment and retention interventions due to the lack of effective practical solutions, we apply the DSR approach (Hevner et al. 2004), since we do not only want to understand issues related to blood donors, but rather to solve them by designing and evaluating appropriate BDBCSS. Moreover, as indicated at the end of Sect. 2, the formulation of design principles (DPs) based on justificatory knowledge as well as a nascent design theory for an entire class of BDBCSS has not yet been conducted in research and thus our findings contribute to DSR as well as IS literature. By following the three cycle view of DSR (Hevner 2007), we combine inputs from our three blood service partners (WCBS, SANBS, NBSG) and their blood donors as potential BDBCSS end users ensuring a real-world scenario (relevance) with the extant body of knowledge comprising existing blood donation information systems and behavior change models (rigor) for grounding our BDBCSS design and bridging claims to design science as well as behavioral science. As shown in Fig. 3, our research project is based on the DSR framework proposed by Kuechler and Vaishnavi (2008) and is divided into four consecutive design cycles.

Design cycles with respective research activities (based on Müller and Reuter-Oppermann (2023b))
Our first design cycle served for the derivation of the DPs of a specific BDBCSS, i.e., chatbots for blood donors to increase their willingness to donate blood grounded on design requirements (DRs) extracted form extant literature on chatbots, blood donor mobilization and management solutions as well as blood donor behavior. In addition, to refine and identify requirements that have been and have not been covered by our first set of design requirements, we conducted a semi-structured interview with an expert of the blood donor behavior of African minorities in Western Europe as we did not have access to our blood service experts at that point due to the COVID-19 pandemic. Subsequently, we theoretically instantiated our DPs via fictional blood donation scenarios shown to potential end users from Germany through a survey format. The online survey served for the evaluation of our proposed design and consisted of ten scenarios representing our identified requirements (e.g., making an appointment for blood donation). For the scenarios, respondents could choose from three alternatives, i.e., website, chatbot and app. In each case they had to decide which one met the presented requirement best. Since the survey not only revealed that with regard to the individual donor types, to embrace the “one design fits all” approach, all of our DRs have to be considered for the development of the chatbot as each donor group has different preferences on what and how exactly a chatbot should provide support to them, but also prove the importance of blood donation apps, we further envisioned their design as part of our DSR project. Consequently, we aimed to determine how a helpful and efficient blood donation app should be designed, also investigating the best integration of a chatbot conceivably serving as a complementary artifact. A detailed description of our first design cycle including our research results is presented in Müller and Reuter-Oppermann (2022a).
We then engaged in a second design cycle, where we conducted further research on blood donation app features to get a better understanding of specific design features (DFs) that are suitable for our first conceptual instantiation. Consequently, we translated our derived DPs into concrete DFs, which we identified to be appropriate for a blood donation app. With Marvel, a platform for building clickable app prototypes, we then instantiated the DPs in the form of a conceptual model. Subsequently, in an explorative focus group workshop with potential German end users, we qualitatively evaluated the artifact and its DPs with the help of a strengths, weaknesses, opportunities and threats (SWOT) analysis and quantitatively by asking for their rating of each DF in order to prioritize them. The workshop’s positive results showed us that our proposed design has some validity indicating the usefulness of the BDBCSS artifact. The detailed findings of our second design cycle are described in Müller and Reuter-Oppermann (2022b).
In our third design cycle, we first studied the literature on culture and persuasive system design (PSD) theory to be able to evaluate if our proposed blood donation app design generally is persuasive and to better understand how the perceived persuasiveness of different blood donation cultures might differ. To evaluate our proposed design, we first mapped our blood donation app DFs to the design principles of the PSD model (Oinas-Kukkonen and Harjumaa 2009). Next, before we evaluated the different blood donation cultures’ perceived persuasiveness with the help of our conceptual model developed in our second design cycle, we used the first design cycle’s online survey to determine if our blood donation app is also perceived as useful by potential end users from Africa and if it is also the tool of choice for them when competing with a website or chatbot as our app was originally designed for and evaluated with potential end users from Germany. For the evaluation of the DFs’ perceived persuasiveness of individualist (South Africa) compared to collectivist (Ghana) blood donation cultures, we added the two snapshots underlying our conceptual model to the survey as they both represent all of our blood donation app design features. In terms of the quantitative evaluation of our artifact, we asked the potential African end users for their rating of each DF in order to prioritise them (similar to the second design cycle’s evaluation with the German focus group) and by comparing the participants’ statements on the usage potential of the app, we also evaluated it qualitatively. The survey revealed that while for both countries personal and social features are important for the design, their perceived persuasiveness of the DFs differs in the way that for South Africa representing an individualist blood donation culture, personal features (e.g., reminders and rewards) seem to be more effective in inducing behavioral changes and for Ghana as a collectivist blood donation culture social features (e.g., normative influence and social role) dominate. A detailed description of the third design cycle is given in Müller and Reuter-Oppermann (2023b).
We started our fourth design cycle presented in this paper with further reading on behavioral theories to not only understand the situational-level (TPB) and processual-level needs (TTM) of blood donors, but more importantly also their global-level needs (SDT) representing basic psychological needs underlying each individual’s intentional as well as developmental blood donation behavior. Accordingly, we adapted our third design principle with regard to the BPN relatedness to cover the artifact’s companion capabilities. In collaboration with our BISKIT project partner eHealth Africa, we then instantiated the DPs in the form of a fully functioning but still evolving BDBCSS artifact, which is why our prototype developed in Marvel continues to serve as the instantiation with their full coverage. Subsequently, with the help of both artifacts, we quantitatively evaluated the DPs in a survey-based field study on two consecutive days at WCBS with their real blood donors. To this end, we employed two established questionnaires, one focusing on the POC and the other one on the BPNS. This process served to establish the basis for the formulation of a nascent design theory.
4 Designing Blood Donation Behavior Change Support Systems
To increase donors’ willingness to donate blood and induce changes in blood donor behavior, it is crucial to minimize potential barriers such as inconvenience and lack of knowledge as well as foster motivators, both grounded on the behavioral change models presented in Sect. 2. With this, we ensure a user-centered BDBCSS design specifically focusing on pragmatic and service-oriented capabilities and not on the underlying technical infrastructure necessary for the integration of data sources. Unfortunately, the latter is the focus of most of the studies discussing blood donor mobilization and management systems design solutions, rather considering technical issues such as system requirements than involving user perspectives and focusing on user-centered design (e.g., Ouhbi et al. 2017). Against this background, we consider BDBCSS design from a user’s point of view based on theoretical frameworks as a promising opportunity for the improvement of existing solutions in the blood donation application domain (Gregor and Hevner 2013).
4.1 Design Requirements and Design Principles
We identified three overarching design requirements (DR1-3) comprising the fundamental supportive BDBCSS capabilities to address the three global-level BPN identified as key issues (I1-3) for each individual’s motivated intentional and developmental blood donation behavior (see Fig. 4). For addressing all of our derived design requirements, as shown in Fig. 4, we formulated three design principles (DP1-3) according to the structure proposed by Chandra et al. (2015) and translated them into concrete design features (DF1-15).

Issues, design requirements, design principles and design features for BDBCSS (based on Müller and Reuter-Oppermann (2022b))
DR1.1 – 1.3 refer to the BDBCSS’s ability to support users in organizational and planning issues around the blood donation process. As forgetfulness, convenience or other new plans are the most common reasons why arranged blood donation appointments are not kept, the BDBCSS is supposed to counteract them by sending appointment reminders and assisting users in scheduling their appointments (Bosnes et al. 2005; van Dongen et al. 2014). In this way, they can better plan ahead when they need to postpone or cancel an appointment, which prevents that overwhelming everyday appointments obstruct them from prioritizing blood donation (van Dongen et al. 2012). As there are also blood donors who have doubts about their eligibility to donate again and are concerned about being deferred by the blood service, reminders to donate again and what the requirements are that need to be met are useful (Batis and Albarrak 2021). In addition, in preparation for the appointment, the BDBCSS should be able to notify the user about opening hours, location, free parking and the estimated length of stay in the blood donation center (Batis and Albarrak 2021). Due to the fact that mobile blood donation centers are often preferably visited by new donors a few times at the start of their donor career (Schreiber et al. 2005) and as they are more easily accessible compared to fixed donation centers, they can help to facilitate donors’ transition towards giving blood regularly (Godin et al. 2005; Schreiber et al. 2005). Accordingly, the BDBCSS is supposed to notify the user of mobile blood drives taking place in the near vicinity.
In the event of a crisis with an acute shortage of supply, the necessary timely and appropriate blood supply might be at risk due to the time-consuming and labor-intensive conventional donation requests by post or telephone. In this context, the blood donor survey of Batis and Albarrak (2021) revealed that almost half of the 383 donors are interested in receiving alerts about low blood inventory levels and more than half of them about blood donation shortages. Therefore, the notification of the user about and the insight into current blood stock levels and especially urgently needed blood donations due to shortage are relevant for the BDBCSS. Moreover, the effort around the donor questionnaires, as known from the example of the app “Statusplus Blutspende”, not only means a high administrative workload for blood service employees, but also causes long waiting times for blood donors. As a lengthy stay in the blood donation center demotivates donors to make future donations (Bosnes et al. 2005; Godin et al. 2005), it is a prerequisite for the BDBCSS to be able to assist the user in filling out the donor questionnaire in advance. In conclusion, we propose:
-
DP1: Provide the BDBCSS with proactive planning interventions comprising reminders as well as push notifications and with organizational and planning assistance to enable users to integrate and prioritize blood donations in their busy lifestyles.
DR2.1 – 2.3 relate to the BDBCSS’s ability to shape knowledge and create awareness with regard to blood donation and its benefits. Due to the identification of the different user archetypes 1) “Technologists”, 2) “Biologists” and 3) “Escapists” by Foth et al. (2013) characterized by different interests concerning the blood donation process such as (1) the system behind, (2) the role of blood and (3) methods for distraction during donation as well as due to the huge variety of possible questions of donors, the BDBCSS is supposed to respond to various user inquiries related to the blood donation process. Moreover, as self-education about pre- and post-donation requirements and processes, for example, with the help of tutorials, supports donors to get familiar with the benefits of donating blood (Batis and Albarrak 2021), the BDBCSS should be able to make the user aware of these benefits and the underlying blood donation process. Additionally, since donors often do not know the general pre-requirements to be met (e.g., in terms of weight or age) and the necessary documents they have to bring (e.g., identity card), they frequently come in vain because of getting temporarily deferred by the blood services (Batis and Albarrak 2021), possibly leading to frustration as they may perceive this deferral as a permanent rejection and thus often do not come back (Bednall et al. 2013; Piliavin 1987). Therefore, it is a prerequisite for the BDBCSS to be able to inform the user about blood donation requirements before the blood donation appointment takes place. Concluding, we propose the following:
-
DP2: Provide the BDBCSS with informational and awareness-raising capabilities to enable users to draw their own conclusions and to help them better understand their impact of donating blood.
DR3.1 – 3.3 refer to the BDBCSS’s ability to motivate users as well as give and receive feedback on blood donations. As especially for new blood donors motivation plays a crucial role with regard to their future donations (Godin et al. 2007; van Dongen et al. 2014), making motivational approaches appropriate for their recruitment, the BDBCSS is supposed to motivate the user based on the number of past donations. In addition, as mentioned at the end of Sect. 2, since Sardi et al. (2019b) demonstrated that a well-balanced combination of different gamification elements (e.g., points, badges, quizzes, levels, trophies, progress bars and leaderboards) is necessary to trigger the behavioral transformation of blood donors towards engagement and loyalty, the BDBCSS should be able to motivate the user by providing appropriate elements of gamification. Furthermore, due to the statement of our interviewed blood donation expert that it is also particularly motivating for donors to be informed when the own blood donation has been transfused to a patient, the BDBCSS should be able to notify the user as soon as the transfusion of the blood donation was made.
For making donating blood a habit, providing feedback on the donors’ expressed expectations and experiences regarding the blood donation process is essential (Piliavin et al. 1982). In this way, barriers such as initial anxiety, eligibility doubts, inappropriate donor locations and opening hours or incompetent blood service employees and unsatisfying service qualities could be addressed better, making it possible to respond more effectively to donors’ needs and to build a closer relationship with them, which is why induced expectations and experience exchanges are relevant for the BDBCSS. Related to this, since virtual coaches, which originated in the healthcare sector, are aimed to support users in behavioral transformation through helpful instructions, health-related knowledge forming as well as the provision of motivational support (Tropea et al. 2019) and may also be applicable to the blood donation context, the BDBCSS is supposed to act like a companion embodying a mix of characteristics including friendliness, expertise, trust and support. In conclusion, we propose:
-
DP3: Provide the BDBCSS with motivational and encouraging methods comprising gamification, bidirectional feedback and companion capabilities in order to help users either start donating (again) or keep on track in donating blood (more) regularly.
4.2 Instantiation of the Design Principles
Adapted to our South African blood service partners form the BISKIT research project, we built two artifacts where we instantiated the proposed design principles: a blood donation app and an integrated chatbot. For this, the already existing apps and chatbots described in Sect. 2 provided orientation. To the best of our knowledge, we are the first regarding the design of a chatbot-based blood donation app. We argue that even though both BDBCSS can stand alone with apps providing comparably more functionalities, their integration additionally adds value to the user for three reasons. Following the CASA paradigm (Nass et al. 1994), as one of the main purposes of chatbots is being perceived as human-like with the help of incorporated social cues derived from interpersonal communication (e.g., small talk and emojis) (Feine et al. 2019), they are appropriate to provide the feeling of a human contact (Verhagen et al. 2014). In this way, a chatbot counteracts the missing personal touch when using a blood donation app, which was stated by almost 30 % of the 383 participants in the blood donor survey of Batis and Albarrak (2021). Interacting with a chatbot feels like talking to another human being while writing text messages in natural language back and forth, even though it only mimics human conversation with a software program behind (Dale 2016). Second, a chatbot as part of a blood donation app leads to a deeper engagement with blood donors in offering the opportunity of a follow-up conversation with further questions being answered. Third, in providing short resolution times and being available 24 h on 7 days a week (Gnewuch et al. 2017), a chatbot counteracts concerns about the app’s inability of getting questions answered promptly, which was indicated by more than half of the 383 respondents (54.1 %) in the blood donor survey of Batis and Albarrak (2021).
In the following, before we show a preview of our still evolving BISKIT blood donor app, we first describe the instantiation of the DPs within our blood donation app conceptual model serving as a basis for the BISKIT app followed by the description within the chatbot itself. For the blood donation app conceptual model, we built the artifact and instantiated the DPs using Marvel, a platform for building clickable app prototypes (see Fig. 5).
As shown in the two snapshots in Fig. 5, for the instantiation of the first design principle (DP1) we integrated a digital donor card (DF1) so that the card cannot be left behind as users usually have their smartphone with them at all times. Since the digital donor card contains all the necessary data, after its scan when entering the donation center, the user passes through the donation process more quickly with all the data being already transferred with one click. Similarly, with the donor questionnaire (DF3) to be filled in digitally whenever and wherever the user wants to beforehand, the blood service can read out the result immediately through the generation of a QR code. In addition, as users get insights into their results in advance, it prevents them from coming in vain in case a negative result pops up. Moreover, with the help of an integrated appointment booking system (DF2), the user can organize blood donation appointments quickly and straightforwardly. The arranged and accomplished appointments are stored in the incorporated donation history (DF4) showing users where and when they have donated blood so far to track their blood donations and potentially return to a particular donation center again. By clicking on the profile, besides their own blood donation data, users also get an insight into local blood inventory levels (DF5) to check and decide on their own if it is necessary to donate or not.
Additionally, as depicted in the snapshot on the right in Fig. 5, the activatable or deactivatable chatbot reminds users of their upcoming appointment (DF6.1), the requirements to be met (DF6.2), when they are eligible to donate blood again (DF6.3) and notifies them when and where the donation center can be visited and how much time the whole stay probably will take (DF6.4), so that they do not need to have all that in mind themselves. The chatbot’s push notification about nearby mobile blood drives (DF6.5) enables the users to spontaneously give blood in their immediate vicinity and being notified about critically low blood inventory levels (DF6.6) lets the users know that their blood donation is urgently needed and that they can make a difference through donating blood.
As with making appointments independently, even when users seek information about donating blood, they do not need to call blood service employees or search the internet as the chatbot answers all of their questions promptly (DF7.1) and fitting tutorials (DF11.1) further illustrate the content enabling the user to control their knowledge gain by taking part in subsequent quizzes (DF11.2) (DP2). With the help of both tools, users become aware of blood donation and its benefits, for example, by watching videos with success stories of patients in need of blood who survived due to other people’s blood donations and by the chatbot casually telling the users while interacting, for instance, that with their one blood donation they can save up to three lives (DF7.2). If users are interested in their own blood group and want to know, for example, with which other blood groups it is compatible, they can look up information about their own blood group at any time by clicking on their profile (DF8). In addition, via the integrated chat forum (DF10), users can also inform themselves and become aware of the blood donation process through an information and experience exchange with other blood donors. Here as well as through the app’s connection to the users’ social media channels (DF9), users can post their blood donation appointment, performance records and/or blood journey (i.e., the path of the own blood donation) in order to, for instance, make others aware of donating blood.
Not only the educational material in form of tutorials and subsequent quizzes is appropriately tailored to the user depending on the user’s determined stage of change, but even the chatbot reacts adequately with respect to its initiated exchange of expectations and experiences (DF6.9) as well as motivational and awareness-raising approaches engendered during the interaction with the user (DP3). In line with the proposal of Sardi et al. (2019b), the SOC is initially determined by means of a short survey comprising four questions when the user first registers and logs into the app. The staging algorithm developed by Burditt et al. (2009) builds the basis for the survey, in which the users (1) assess if they are eligible to give blood or not, (2) indicate the number of past blood donations within the last year, (3) assess if they are willing to donate within the next 6 months or not and (4) next month or not. Inspired by Sardi et al. (2019b), if the survey result is “precontemplation”, no status is attributed to the user, whereas for the contemplation stage it is “Blood Beginner” (symbolized by an empty blood drop), for the preparation stage “Good Samaritan” (symbolized by a lifebelt), for the action stage “Blood Ninja” (symbolized by a ninja) and for the maintenance stage it is “Blood Donation Hero” (symbolized by a heartbeat) (see example in Fig. 5 on the left in the upper right corner). While using the blood donation app, users can look up their current status on the home page’s progress bar (DF13) at any time and, by clicking on the corresponding icon, they receive a description of what the SOC they are currently in means and why it is worth it to make further progress. What is needed to change the blood donor behavior and reach the next stage is suggested by the chatbot, which behaves and reacts in a way that is fully adapted to the user according to the user’s determined current stage of change. In providing stage-matched guidance and feedback to the user to foster the developmental process of the user’s blood donor career (Amoyal et al. 2013), the chatbot as a whole acts like a companion embodying a mix of a virtual coach (Tropea et al. 2019; Weimann et al. 2022) and a virtual assistant (Maedche et al. 2016).
Besides the progress bar, the user is incentivized and rewarded for stage transition through the opportunity to earn points, badges, trophies and rankings (DF12) with every single blood donation that was made. As part of the app’s integrated challenge of earning the most points for donating blood, the user’s ranking is shown via leader boards (DF13) at individual as well as at team level, which enables the user to cooperate and compete with other donors. The latter can also be accomplished by taking part in the incorporated blood donation quiz (DF13) and comparing the knowledge gain through the collection of additional points for answers given correctly. In line with this, via push notifications, the chatbot praises users as soon as they have achieved a new score, badge, trophy or ranking as part of their performance records (DF6.8) and whenever they donated blood as soon as their blood donation has been transfused (DF6.7). The latter can also be observed by the users themselves by tracking the path of the own donation from the blood collection, processing, testing and storage to the blood transfusion (DF14). Additionally, the users get insights into their vital parameters measured directly before their blood donation was made as well as into their results of the blood tested afterwards (DF15).
Overall, all of the described design features (DF1-15) encourage the user to go through the individual processes of change that positively influence the user’s willingness to donate blood and promote blood donor behavior change. Our conceptual model in Fig. 5 shows which process of change is triggered by which design feature.

Conceptual model with instantiated DPs through the DFs 1-15 (adapted from Müller and Reuter-Oppermann (2022b))

Chatbot with instantiated design principles
From the diverse software development platforms that emerged in recent years, we purposefully chose Google Dialogflow based on the taxonomy of Diederich et al. (2019a) for the implementation of the chatbot. We built the chatbot and instantiated the DPs using Dialogflow which provides natural language processing capabilities for user intent detection and a custom-built web interface that offers convenient access (see Fig. 6). We collaborated with the blood service project partners to better understand the individual groups of donors and to design the chatbot conversation based on their delivered list of common misconceptions about blood donation as well as on their FAQ websites for modeling the different extracted user intents to approach the chatbot on Google Dialogflow (DP2). For complete coverage considering basic questions, we also took some questions of the known FAQ websites of the German Red Cross into account and reviewed the respective training phrases (i.e., user requests) and responses of the chatbot. In order to address the high variability of user input, we also created a default fallback response in case intent detection was not possible, together with the default welcome intent leading to 86 intents in total. While the chatbot itself already provides as many details as possible, depending on the questions, we added images and links to websites, videos and documents to the responses of the chatbot for extra information that is optionally accessible for the user. In addition, by applying the card sorting method, we also integrated dialogue continuity suggestions in the form of buttons for triggering four related follow-up questions to eleven of our 86 modeled intents on Dialogflow.
To make it possible to book appointments, we included entities on Google Dialogflow representing annotations for parameters like place and time queried during the chatbot interaction as well as contexts allowing sequential dialogues in case users answer with a simple “yes” or “no” (DP1). To support the characteristics of a companion such as friendliness, expertise, trust and support, as shown in Table 2, we purposefully selected and organized a set of social cues for the human-like design of the chatbot based on the taxonomy of Feine et al. (2019) (DP3). As a chatbot per se is a text-based conversational agent (Gnewuch et al. 2017), we eliminated the auditory category as well as all subcategories referring to embodied conversational agents.
By mapping the described design features (DF1-15) of the chatbot-based blood donation app to the PSD model proposed by Oinas-Kukkonen and Harjumaa (2009) for the design and evaluation of persuasive systems in a previous study, we demonstrated that our app overall is persuasive in terms of inducing changes in blood donor behavior (Müller and Reuter-Oppermann 2023b). However, as our previous research revealed that the design features’ perceived persuasiveness differs depending on the user’s blood donation culture in the way that personal features like reminders or rewards seem to be more effective in inducing behavioral changes in an individualist culture (e.g., South Africa) and social features like normative influence or social role in a collectivist culture (e.g., Ghana) (Müller and Reuter-Oppermann 2023b), for the evaluation at our South African blood service partner, we first implemented a preselected set of personal features within the BISKIT blood donor app. Figure 7 shows a preview of the still evolving chatbot-based BISKIT blood donor app, developed in collaboration with our BISKIT project partner eHealth Africa.

Preview of the BISKIT donor app
5 Evaluation
Following the framework for evaluation in design science (FEDS), we structured the evaluations of our BDBCSS design in four steps throughout our four consecutive design cycles (Venable et al. 2016). For the artifact’s evaluation strategy, we decided on the Human Risk & Effectiveness strategy because of major user perception design risks. In our first three cycles, we conducted three formative evaluations by means of online surveys and a focus group (see Fig. 3). As suggested in the FEDS, a summative evaluation episode followed in the fourth design cycle by means of a survey-based field study to increase the generalizability. With this, we aim to provide evidence that an instantiation of our proposed BDBCSS design in the form of an artifact can induce changes in blood donor behavior and addresses the outlined issues with respect to autonomy, competence as well as relatedness.
We conducted our naturalistic evaluation episode on 29 May 2023 and 30 May 2023 on site at our blood service partner WCBS with their real blood donors who are familiar with and partly struggling with the issues around blood donation (Venable et al. 2016). On these 2 days, overall, we recruited 29 donors for participation in our survey-based field study that took around 30 min per participant. Of the 29 blood donors (i.e., nd = 2 (6.90 %), fd = 3 (10.34 %), ld = 3 (10.34 %), rd = 21 (72.41 %)) 19 (65.52 %) were female and 13 (44.83 %) had already used a chatbot before. Our sample represents a fairly balanced age mix ranging from 21 to 68 and ensuring comprehensive feedback from diverse perspectives. Table A1 in the appendix (available online via http://link.springer.com) displays their statistics in detail. Obviously, most of them were regular blood donors serving best for the evaluation of our artifact as they have already been through all these issues throughout their blood donor career. In the following, we present the testable propositions we formulated, the methodology as well as the results from our evaluation.
5.1 Derivation of Testable Propositions
In line with Gregor and Jones (2007) suggestions, we formulated testable propositions (P1-4) to validate that our proposed BDBCSS design promotes blood donor behavior change and targets the underlying global-level BPNS. First, the objective of our DSR project was to design a user-centered BDBCSS that addresses the preferences and needs of all types of blood donors to increase the willingness to donate blood. Hence, the overall utility of the BDBCSS is defined by the extent to which its design satisfies all of the three basic psychological needs which are (1) autonomy, (2) competence and (3) relatedness. This means, the usefulness of the BDBCSS depends on its ability to support blood donors to (1) freely decide and be in control over the decision to donate, (2) be confident and self-effective in the ability to donate and (3) feel connected to as well as supported by others (France et al. 2017) as reflected in the three proposed design principles. Thus, we hypothesized that the users perceive utility of the BDBCSS when it satisfies the three BPN autonomy, competence and relatedness in accordance with our three propositions:
P1: If a BDBCSS follows the proposed design, then it satisfies the user’s need of autonomy.
P2: If a BDBCSS follows the proposed design, then it satisfies the user’s need of competence.
P3: If a BDBCSS follows the proposed design, then it satisfies the user’s need of relatedness.
Second, the BDBCSS design could lead to blood donor behavior change due to the linear relationship between its incorporated design features and the processes of change as depicted in the conceptual model in Fig. 5. With this, the BDBCSS not only fosters the process of intentional blood donation behavior, but also the developmental process of the user’s blood donor career (Amoyal et al. 2013; Burditt et al. 2009; Ferguson and Chandler 2005; Sardi et al. 2019a) as reflected in DP3. Against this background, we suggest that the deliberate selection of design features leads to the BDBCSS having a high level of user engagement and thus the capability of behavioral transformation. Consequently, we formulate the following proposition:
P4: If a BDBCSS follows the proposed design, then it fosters the user’s change in blood donor behavior.
5.2 Evaluation Methodology
We tested the propositions for our BDBCSS design by means of a survey-based field study on site at Western Cape Blood Service. There, participants were invited to interact with the developed chatbot-based BISKIT donor app as well as the underlying Marvel prototype (for coverage of all the proposed design features as the BISKIT donor app is still evolving) and were walked through each of the design features and corresponding functionalities after we had explained the whole procedure as well as our objectives and got their agreement to our privacy policy as well as to the use of Google’s Dialogflow (for interaction with the chatbot) and Forms (to conduct the online survey) services. The interaction with the chatbot itself lasted around ten to 15 min. After the whole walk through, the participants completed an online survey with questions about their demographics, the artifact’s BPNS, the artifact’s coverage of POC and their general feedback.
Regarding the context of blood donation, we adapted established questionnaires from other studies that correspond to our propositions: the Basic Psychological Need Satisfaction for Technology Use (BPN-TU) Scale of Moradbakhti et al. (2022) and the questionnaire of Sardi et al. (2019a) measuring the processes of change. The three constructs with nine items (three items per BPN) of the former are demonstrated in Table A.2 and the ten constructs with thirty items (three items per POC) are shown in Tables A3 and A4 in the appendix. All of the items of both questionnaires were measured by using a five-point Likert-type scale representing the respondents’ level of agreement (i.e., from 1 = “strongly disagree” to 5 = “strongly agree”).
5.3 Results
We analyzed the survey data via Excel by means of descriptive statistics for the quantitative evaluation of our artifact. Tables A2, A3 and A4 in the appendix show the detailed results of our survey (i.e., the results for each item). Table 3 summarizes the overall results of all the constructs evaluated (with the first three belonging to the BPN-TU Scale and the following ten to the POC questionnaire). Overall, when comparing the level of agreements of the participants, it can easily be seen that they agreed to the ability of the artifact to satisfy their basic psychological needs (see also Table A2 in the appendix) and to its ability to promote changes in blood donor behavior through the agreement to the coverage of the POC representing experiential (see also Table A3 in the appendix) and behavioral strategies (see also Table A4 in the appendix) as all of the items’ mean values are above the neutral level of agreement (i.e., 3 = “neutral”). Comparing the mean value of all of the items representing experiential strategies (mean = 4.47) to the one of the behavioral strategies (mean = 4.56), it can be seen that both types of POC strategies are equally fully covered. With regard to BPNS, the latter is also true for the three basic psychological needs autonomy (mean = 4.47), competence (mean = 4.47) and relatedness (mean = 4.25) with a slight tendency towards a better need satisfaction for autonomy and competence. This is also reflected in the values regarding variance and standard deviation, which are comparatively higher for the BPN relatedness (see also Table A2 in the appendix). With a few exceptions, for the ten constructs and 30 items representing the processes of change, both of these values are rather low (see also Tables A3 and A4 in the appendix). In summary, the results of the quantitative survey-based field study support the proposed BDBCSS design and confirm the intended effects described in the three design principles.
6 Discussion
Following the “one design fits all” approach, our presented DSR project aimed to address user-centered BDBCSS design tailored to the different preferences and needs of all types of donors to not only support the process of intentional blood donation behavior, but also the developmental process of the user’s blood donor career. Next, we discuss theoretical and practical implications of our results for BDBCSS design and in the form of a nascent design theory, we summarize the generated prescriptive knowledge.
6.1 Implications for Preventive Health Behavior Change Support Systems Design
With regard to research and practice underlying existing preventive health BCSS, to date their focus was primarily on the development and evaluation of artifacts to be used in a specific context and insights into the BCSS’ design as well as theoretical justification, making them even more effective, are rather limited or completely missing (Oinas-Kukkonen 2013; Orji and Moffatt 2018). We have addressed this gap by providing prescriptive knowledge through the systematic derivation of three theory-based design principles and the following proposal of a nascent design theory for BDBCSS. Through the presentation of our resulting BDBCSS design in the form of a nascent design theory, we demonstrate how the DSR methodology can be applied to address a real-world problem, including the use of established theories and design knowledge for the derivation of new design knowledge ensuring a coherent sequence of evidence from issues to design requirements to design principles and to design features. In this way, researchers and practitioners can orient themselves on our methodological approach as well as make use of our proposed design knowledge to build their own user-centered preventive BCSS instantiations fitting to their health context and to be able to innovate their care delivery.
We instantiated the DPs’ described functionality in two complementary BDBCSS artifacts. Thus, our design enhances the extant knowledge base of preventive health BCSS in general and blood donation information systems in particular, which primarily consist of one distinct application system. Regarding existing research and practice, the combination of graphical and conversational user interfaces for full blood donor support, particularly for providing stage-matched guidance and feedback to not only support intentional blood donor behavior but for the first time also proactively promote the developmental process of the user’s blood donor career, is completely new. Consequently, our BDBCSS design can be classified as an improvement in line with the DSR contribution framework by Gregor and Hevner (2013), as we have developed a new solution to a known problem based on extant research.
Particularly with respect to the conversational part of our BDBCSS design, we respond in several ways to the established research agenda of Weimann et al. (2022) investigating virtual coaches. First, we have answered their question of how the constructs of behavioral theories like the TPB, TTM and SDT predicting behavioral transformation can be effectively mapped to information systems and inform their design. Second, we have responded to their question of what the design can look like to effectively foster persuasiveness and user engagement and, related to this, third, to support habitual change. To address both the BDBCSS’s persuasiveness and user engagement, we integrated a combination of behavior change strategies such as behavioral nudging and gamification. We not only proposed but also instantiated several persuasive techniques (e.g., reminders, rewards and self-monitoring), whose evaluation has demonstrated their potential to induce behavioral changes and which therefore can inform the design of other preventive health BCSS such as virtual coaches or digital therapeutics. Due to the human-like nature of the latter two, their design can also be informed by our identified social cues supporting characteristics of a companion (e.g., friendliness, expertise, trust and support) that similarly to these two provides stage-matched guidance and feedback to the user to foster his/her developmental process. Overall, through our design of a chatbot-based blood donation app we extended the knowledge of how to better manage healthcare with the help of mobile technologies.
Moreover, the research agenda of Weimann et al. (2022) also includes important further questions with respect to future research of our BDBCSS design such as what the user’s guidance through the SOC can exactly look like and if this enhances long-term behavioral transformation. This is part of what we aim at with conducting a following longitudinal field study to demonstrate that the proposed BDBCSS design really leads to intentional as well as developmental blood donation behavior. Even though our BISKIT development team is highly interdisciplinary due to the participation of technicians (eHealth Africa), domain experts (WCBS, SANBS, NBSG) and IS researchers (ourselves), for this future work we particularly want to consider psychologists as they are best knowledgeable in human interaction with regard to the effective conversational design (Gnewuch et al. 2022; Weimann et al. 2022). They also have knowledge about other important factors relevant for BCSS such as cognitive overload (e.g., due to many just in time interventions) (Rieder et al. 2020) and trust (Wang and Benbasat 2009), which is also related to data protection and privacy issues (Sunyaev et al. 2014). Thus, we address the threats and weaknesses regarding our BDBCSS design anticipated by the focus group of our second design cycle (Müller and Reuter-Oppermann 2022b).
6.2 Towards a Nascent Design Theory
Our DSR project provides valuable implications for designing preventive health BCSS in general and contributes to the improvement of current blood donation information systems in particular by presenting a situated instantiation in the form of two BDBCSS artifacts and by formulating more general ones in the form of constructs, DPs and testable propositions (Gregor and Hevner 2013). Table 4 summarizes our contributions in the form of a nascent design theory (Gregor and Hevner 2013; Gregor and Jones 2007).
6.3 Limitations
Even though we conducted our DSR project in accordance with established guidelines, some potential limitations should be mentioned. First, the sample size on which our summative evaluation is based is a seemingly small number of 29 participants. While, at a first glance, this number seems low, increasing the sample size with further participants is not required for the validation of our BDBCSS design, as the results of our on-site evaluation overall are very positive, especially with regard to the values representing standard deviation and variance. Second, even though we collected demographical information of our participants, we did not further consider contextual aspects such as participants’ experience with chatbots or with donating blood that could affect the perceived utility of the chatbot-based blood donation app. Third, due to related biases, data obtained from questionnaires generally need to be treated with caution. Particularly two common biases come to mind. These are the socially desirable bias (Podsakoff et al. 2003), which causes participants to give a positive rating even though this does not reflect reality and the common scale bias (Podsakoff et al. 2003), which may be to the use of similar five-point Likert scales for all of our items. However, due to the fact that our survey is based on adapted questionnaires from existing literature, we consider the received data and resulting implications as reliable. For the confirmation of this paper’s findings, we still invite other scholars to conduct further evaluations and future work.
7 Conclusion and Outlook
Blood is one of the most critical resources in healthcare and the life of many patients depend on it. Therefore, one must take all measures necessary to ensure sufficient blood donations, including providing BDBCSS to all donor types. In this paper, we present theoretically grounded design principles for BDBCSS and evaluate their instantiaton as a blood donation app and a chatbot. Our research can be classified as an improvement (Gregor and Hevner 2013), because we provide a new solution to a problem that was already known. With our findings, we contribute to both theory and practice.
On the practical side, our work offers design knowledge for BDBCSS to support and motivate all donor types to become and stay regular donors. As part of the related research project BISKIT, we built prototypes of an app and a chatbot as instantiations of the DPs for BDBCSS. The final evaluation by means of a survey-based field study on site at Western Cape Blood Service showed great approval of the DPs and overall very positive results. Blood services can build their own BDBCSS instantiations to easily reach donors, provide information, and motivate them to donate (regularly). Additionally, we provided valuable implications for the design of preventive health BCSS practitioners can make use of for their own healthcare interventions.
On the theoretical side, we offer a theoretically grounded and evaluated design for BDBCSS to tackle an important and very challenging real-world problem for healthcare systems worldwide by applying the DSR methodology. In addition to partial evaluations of the individual BDBCSS, i.e., the blood donation app and chatbot, we have carried out an evaluation of the overarching design elements. The results are presented as a nascent design theory for BDBCSS. Future research on the design and impacts of BDBCSS in particular and preventive health BCSS in general can build upon it.
In future studies, we hope that researchers and practitioners will apply, evaluate and extend the proposed nascent design theory for blood donation behavior change support systems to reach a full design theory for blood donation and blood services information systems in general. This includes the transfer to other countries, cultures and healthcare systems, which will make our findings, beyond our previous studies with Germans and Ghanaians, even more generalizable. Future work may also investigate the extent to which our findings are transferable to other preventive health BCSS and healthcare contexts.
References
Ajzen I (1991) The theory of planned behavior. Organ Behav Hum Decis Process 50(2):179–211
Amoyal N, Robbins M, Paiva A, Burditt C, Kessler D, Shaz B (2013) Measuring the processes of change for increasing blood donation in black adults. Transfusion 53(6):1280–1290
Asamoah-Akuoko L, Ullum H, Appiah B, Hassall OW, Ndanu T, Adongo P, Bates I (2021) Determinants of intention to return to donate blood among first-time blood donors in Ghana. Vox Sang 116(3):324–335
Baird A, Angst C, Oborn E (2020) Health information technology. In: Bush A, Rai A (eds) MIS quarterly. Management Information Systems Quarterly-Research, Coventry
Batis AA, Albarrak A (2021) Preferences and features of a blood donation smartphone app: a multicenter mixed-methods study in Riyadh, Saudi Arabia. Comput Methods Program Biomed 1:100005
Bednall TC, Bove L, Cheetham A, Murray AL (2013) A systematic review and meta-analysis of antecedents of blood donation behavior and intentions. Soc Sci Med 96:86–94
Bosnes V, Aldrin M, Heier H (2005) Predicting blood donor arrival. Transfusion 45(2):162–170
Burditt C, Robbins M, Paiva A, Velicer W, Koblin B, Kessler D (2009) Motivation for blood donation among African Americans: developing measures for stage of change, decisional balance, and self-efficacy constructs. J Behav Med 32(5):429–442
Canadian Blood Services (2017) Canadian Blood Services launches new tool to engage young donors. https://www.blood.ca/en/about-us/media/newsroom/canadian-blood-services-launches-new-tool-engage-young-donors. Accessed 28 June 2023
Chandra L, Seidel S, Gregor S (2015) Prescriptive knowledge in IS research: conceptualizing design principles in terms of materiality, action, and boundary conditions. In: Proceedings of the 48th Hawaii international conference on system sciences, Hawaii, USA, pp 4039–4048
Dale R (2016) The return of the chatbots. Nat Lang Eng 22(5):811–817
Deci EL, Ryan RM (1985) Intrinsic motivation and self-determination in human behavior. Plenum, New York
Deci EL, Ryan RM (2000) The “what’’ and “why’’ of goal pursuits: human needs and the self-determination of behavior. Psychol Inq 11(4):227–268
Dei-Adomakoh Y, Asamoah-Akuoko L, Appiah B, Yawson A, Olayemi E (2021) Safe blood supply in sub-Saharan Africa: challenges and opportunities. Lancet Haematol 8(10):770–776
Diederich S, Brendel AB, Kolbe LM (2019a) Towards a taxonomy of platforms for conversational agent design. In: Ludwig T, Pipek V (eds) Human practice. digital ecologies. our future. 14. Internationale Tagung Wirtschaftsinformatik (WI 2019), Siegen, University of Siegen, AISeL, pp 1100–1114
Diederich S, Lichtenberg S, Brendel AB, Trang S (2019b) Promoting sustainable mobility beliefs with persuasive and anthropomorphic design: insights from an experiment with a conversational agent. In: Proceedings of the 40th international conference on information systems, Munich, Germany
DRK-Blutspendedienste (2022) Herzlich Willkommen Beim Digitalen Spenderservice. https://www.spenderservice.net/. Accessed 28 June 2023
Elliot A, McGregor H, Thrash T (2002) The need for competence. In: Deci E, Ryan R (eds) Handbook of self-determination research. University of Rochester Press, New York, NY, pp 361–387
Feine J, Gnewuch U, Morana S, Maedche A (2019) A taxonomy of social cues for conversational agents. Int J Hum Comput Stud 132:138–161
Ferguson E (1996) Predictors of future behaviour: a review of the psychological literature on blood donation. Br J Health Psychol 1:287–308
Ferguson E, Bibby P (2002) Predicting future blood donor returns: past behavior, intentions, and observer effects. J Health Psychol 21(5):513–518
Ferguson E, Chandler S (2005) A stage model of blood donor behaviour: assessing volunteer behaviour. J Health Psychol 10(3):359–372
Floyd I, Cameron Jones M, Twidale M (2008) Resolving incommensurable debates: a preliminary identification of persona kinds, attributes, and characteristics. Artifact 2:12–26
Foth M, Satchell C, Seeburger J, Russell-Bennett R (2013) Social and mobile interaction design to increase the loyalty rates of Young blood donors. In: Proceedings of the 6th international conference on communities and technologies, Munich, Germany, pp 64–73
France JL, Kowalsky JM, France CR, McGlone ST, Himawan LK, Kessler DA, Shaz BH (2014) Development of common metrics for donation attitude, subjective norm, perceived behavioral control, and intention for the blood donation context. Transfusion 54(3pt2):839–847
France CR, France JL, Carlson B, Frye V, Duffy L, Kessler D, Rebosa M, Shaz BH (2017) Applying self-determination theory to the blood donation context: the blood donor competence, autonomy, and relatedness enhancement (Blood Donor Care) trial. Contemp Clin Trials 53:44–51
Fürstenau D, Gersch M, Schreiter S (2023) Digital therapeutics (DTx). Bus Inf Syst Eng 65(3):349–360
Gagné M (2003) The role of autonomy support and autonomy orientation in prosocial behavior engagement. Motiv Emot 27(3):199–223
Gnewuch U, Morana S, Adam MTP, Maedche A (2022) Opposing effects of response time in human-chatbot interaction. Bus Inf Syst Eng 64(6):773–791
Gnewuch U, Morana S, Maedche A (2017) Towards designing cooperative and social conversational agents for customer service. In: Proceedings of the 38th international conference on information systems, Seoul, South Korea
Godin G, Sheeran P, Conner M, Germain M, Blondeau D, Gagné C, Beaulieu D, Naccache H (2005) Factors explaining the intention to give blood among the general population. Vox Sang 89(3):140–149
Godin G, Conner M, Sheeran P, Bélanger A, Germain M (2007) Determinants of repeated blood donation among new and experienced blood donors. Transfusion 47(9):1607–1615
Gregor S, Hevner AR (2013) Positioning and presenting design science research for maximum impact. Manag Inf Syst Q 37(2):337–356
Gregor SD, Jones D (2007) The anatomy of a design theory. J Assoc Inf Syst 8(5):312–335
Hagger MS, Chatzisarantis NLD, Harris J (2006) From psychological need satisfaction to intentional behavior: testing a motivational sequence in two behavioral contexts. Pers Soc Psychol Bull 32(2):131–148
Hevner A (2007) A three cycle view of design science research. Scand J Inf Syst 19(2):87–92
Hevner AR, March ST, Park J, Ram S (2004) Design science in information systems research. Manag Inf Syst Q 28(1):75–105
Horstkemper D, Reuter-Oppermann M (2022) BloodChainSim–a simulation environment to evaluate digital innovations in blood supply chains. In: Proceedings of the 2022 winter simulation conference, Singapore
Kuechler WL, Vaishnavi V (2008) Theory development in design science research: anatomy of a research project. Eur J Inf Syst 17(5):489–504
Maedche A, Morana S, Schacht S, Werth D, Krumeich J (2016) Advanced user assistance systems. Bus Inf Syst Eng 58(5):367–370
Makin S (2019) The emerging world of digital therapeutics. Nature 573(7775):106–109
Masser B, White K, Hyde M, Terry D (2008) The psychology of blood donation: current research and future directions. Transfus Med Rev 22(3):215–233
Mayroth N (2017) Meet the chatbot that helps you donate blood. https://www.thehindu.com/news/cities/mumbai/meet-the-chatbot-that-helps-you-donate-blood/article20735945.ece. Accessed 28 June 2023
McTear M, Callejas Z, Griol D (2016) The conversational interface: talking to smart devices. Springer, Cham
Moradbakhti L, Leichtmann B, Mara M (2022) Development and validation of a basic psychological needs scale for technology use. Preprint
Morana S, Friemel C, Gnewuch U, Maedche A, Pfeiffer J (2017) Interaktion mit smarten systemen–aktueller stand und zukünftige entwicklungen im bereich der nutzerassistenz. WuM 9(5):42–51
Müller HM, Reuter-Oppermann M (2022a) Chatblood – towards designing chatbots for blood donors. In: Proceedings of the 30th European conference on information systems, Timisoara, Romania
Müller HM, Reuter-Oppermann M (2023a) Changebots – designing chatbots to support blood donor behaviour change. In: Proceedings of the 44th international conference on information systems, Hyderabad, India
Müller HM, Reuter-Oppermann M (2024) Designing supportive chatbots for blood donors. In: Proceedings of the 57th Hawaii international conference on system sciences, Hawaii, USA, pp 3454–3463
Müller HM, Reuter-Oppermann M (2022) A design science approach to blood donation apps. In: Drechsler A, Gerber A, Hevner A (eds) The transdisciplinary reach of design science research, DESRIST 2022, LNCS. Springer, Cham, pp 221–232
Müller HM, Reuter-Oppermann M (2023) Persuasive blood donation app design for individualist and collectivist cultures. In: Gerber A, Baskerville R (eds) Design science research for a new society: society 5.0. DESRIST 2023, LNCS. Springer, Cham, pp 157–172
Nass C, Moon Y (2000) Machines and mindlessness: social responses to computers. J Soc Issues 56(1):81–103
Nass C, Steuer J, Tauber ER (1994) Computers are social actors. In: Proceedings of the SIGCHI conference on human factors in computing systems, Boston, USA, pp 72–78
Oesterreichisches Rotes Kreuz (2022) Mein Blut Die App – Jetzt Wird Blutspenden Noch Einfacher! https://www.roteskreuz.at/blutspenden/app-mein-blut. Accessed 28 June 2023
Oinas-Kukkonen H (2013) A foundation for the study of behavior change support systems. Pers Ubiquitous Comput 17(6):1223–1235
Oinas-Kukkonen H, Harjumaa M (2009) Persuasive systems design: key issues, process model, and system features. Commun Assoc Inf Syst 24(28):485–500
Orji R, Moffatt K (2018) Persuasive technology for health and wellness: state-of-the-art and emerging trends. Health Inform J 24(1):66–91
Ouhbi S, Fernández-Alemán JL, Toval A, Idri A, Pozo JR (2015) Free blood donation mobile applications. J Med Syst 39(5):52
Ouhbi S, Fernández-Alemán J, Idri A, Toval A, Pozo J, Bajta M (2017) A reusable requirements catalog for internationalized and sustainable blood donation apps. In: 12th International conference on evaluation of novel approaches to software engineering, Porto, pp 285–292
Piliavin JA (1987) Temporary deferral and donor return. Transfusion 27(2):199–200
Piliavin JA, Callero PL, Evans DE (1982) Addiction to altruism? Opponent-process theory and habitual blood donation. J Pers Soc Psychol 43(6):1200–1213
Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP (2003) Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol 88(5):879–903
Prochaska J, DiClemente C (1982) Transtheoretical therapy: toward a more integrative model of change. Psychother Theory Res Pract 19(3):276–288
Rieder A, Vuckic S, Schache K, Jung R (2020) Technostress from persuasion: wearable users’ stressors, strains, and coping. In: Proceedings of the 41th international conference on information systems, Hyderabad, India
Roman MK, Bellei EA, Biduski D, Pasqualotti A, De Araujo CDSR, De Marchi ACB (2020) “Hey assistant, how can i become a donor?’’ The case of a conversational agent designed to engage people in blood donation. J Biomed Inform 107(103):461
SANBS (2020) Partner with the SANBS to give health and hope to South Africa. https://sanbs.org.za/wp-content/uploads/2016/09/PARTNER-WITH-THE-SANBS-TO-GIVE-HEALTH-AND-HOPE-TO-SOUTH-AFRICA_FINAL.pdf. Accessed 28 June 2023
SANBS (2023) Blood stock levels. https://sanbs.org.za/. Accessed 28 June 2023
Sardi L, Idri A, Carillo de Gea JM, Troval A, Fernández-Alemán JL (2019) Applying trans-theoretical model for blood donation among Spanish adults: a cross-sectional study. BMC Public Health 19:1724
Sardi L, Kharbouch M, Rachad T, Idri A, de Gea JMC, Fernández-Alemán JL (2019) Blood4Life: a mobile solution to recruit and retain blood donors through gamification and trans-theoretical model. In: Rocha A, Adeli H, Reis L, Costanzo S (eds) New knowledge in information systems and technologies, vol 932. Springer, Cham, pp 3–12
Schäfer F (2020) Studenten der FH Kiel und UKSH veröffentlichen Blutspende-App. https://idw-online.de/de/news749190. Accessed 28 June 2023
Schreiber GB, Sharma U, Wright D, Glynn S, Ownby H, Tu Y, Garratty G, Piliavin J, Zuck T, Gilcher R et al (2005) First year donation patterns predict long-term commitment for first-time donors. Vox Sang 88(2):114–121
Sinclair KS, Campbell TS, Carey P, Langevin E, Bowser B, France CR (2010) An adapted postdonation motivational interview enhances blood donor retention. Transfusion 50:1778–1786
Straub E (1978) Positive social behavior and morality. Social and personal influences, vol 1. Academic Press, New York
Sunyaev A, Dehling T, Taylor PL, Mandl KD (2014) Availability and quality of mobile health app privacy policies. J Am Med Inform Assoc 22(e1):e28–e33
The American National Red Cross (2022a) Download the blood donor app today. https://www.redcrossblood.org/blood-donor-app.html. Accessed 28 June 2023
The American National Red Cross (2022b) Meet Clara, the blood donation chatbot. https://www.redcrossblood.org/donate-blood/dlp/meet-clara--the-blood-donation-chatbot-.html. Accessed 28 June 2023
Tropea P, Schlieter H, Sterpi I, Judica E, Gand K, Caprino M, Gabilondo I, Gomez-Esteban JC, Busnatu S, Sinescu C, Kyriazakos S, Anwar S, Corbo M (2019) Rehabilitation, the great absentee of virtual coaching in medical care: scoping review. J Med Internet Res 21(10):e12805
van Dongen A, Abraham C, Ruiter RAC, Schaalma HP, de Kort WLAM, Dijkstra JA, Veldhuizen IJT (2012) Are lapsed donors willing to resume blood donation, and what determines their motivation to do so? Transfusion 52(6):1296–1302
van Dongen A, Ruiter R, Abraham C, Veldhuizen I (2014) Predicting blood donation maintenance: the importance of planning future donations. Transfusion 54(3 Pt 2):821–827
van Dongen A, Mews M, de Kort WLAM, Wagenmans E (2016) Missing minorities–a survey based description of the current state of minority blood donor recruitment across 23 countries. Divers Equal Health Care 13(1):138–145
Venable JR, Pries-Heje J, Baskerville R (2016) FEDS: a framework for evaluation in design science research. Eur J Inf Syst 25:77–89
Verhagen T, Van Nes J, Feldberg F, Van Dolen W (2014) Virtual customer service agents: using social presence and personalization to shape online service encounters. J Comput Mediat Commun 19(3):529–545
Vermeulen M, Lelie N, Coleman C, Sykes W, Jacobs G, Swanevelder R, Busch M, Zyl G, Eduard G, Alex W, Ravi R (2019) Assessment of HIV transfusion transmission risk in South Africa: a 10 years analysis following implementation of individual donation nucleic acid amplification technology testing and donor demographics eligibility changes. Transfusion 59(1):267–276
Vries H, Mudde A, Dijkstra A, Willemsen M (1998) Differential beliefs, perceived social influences, and self-efficacy expectations among smokers in various motivational phases. Prev Med 27(5 Pt 1):681–689
Wang W, Benbasat I (2009) Interactive decision aids for consumer decision making in e-commerce: the influence of perceived strategy restrictiveness. Manag Inf Syst Q 33(2):293–320
Weimann T, Schlieter H, Brendel AB (2022) Virtual coaches. Bus Inf Syst Eng 64(4):515–528
Weizenbaum J (1966) ELIZA–a computer program for the study of natural language communication between man and machine. Commun ACM 9(1):36–45
WHO (2023) Blood safety and availability. https://www.who.int/news-room/fact-sheets/detail/blood-safety-and-availability. Accessed 30 January 2024
Acknowledgements
This research was conducted within the project “Blood Information System for Crisis Intervention and Management” (BISKIT) funded by the German Federal Ministry of Research and Education. The authors would like to thank the reviewers and the editors of the Special Issue for their invaluable feedback and support during the revision process.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Additional information
Accepted after 2 revisions by the editors of the Special Issue.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Müller, H.M., Reuter-Oppermann, M. Designing Behavior Change Support Systems Targeting Blood Donation Behavior. Bus Inf Syst Eng (2024). https://doi.org/10.1007/s12599-024-00878-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12599-024-00878-3