
Abstract
Although it has been traditionally thought that decreasing SpO2 with ascent to high altitudes not only induces acute mountain sickness but also can decrease executive function, the relationship between decreased SpO2 levels and hypoxia-induced lowered executive function is still unclear. Here we aimed to clarify whether hypoxia-induced lowered executive function was associated with arterial oxygen desaturation, using 21 participants performing the color–word Stroop task under normoxic and three hypoxic conditions (FIO2 = 0.165, 0.135, 0.105; corresponding to altitudes of 2000, 3500, and 5000 m, respectively). Stroop interference significantly increased under severe hypoxic condition (FIO2 = 0.105) compared with the other conditions. Moreover, there was a negative correlation between Stroop interference and SpO2. In conclusion, acute exposure to severe hypoxic condition decreased executive function and this negative effect was associated with decreased SpO2. We initially implicated an arterial oxygen desaturation as a potential physiological factor resulting in hypoxia-induced lowered executive function.
Similar content being viewed by others

Introduction
Currently, as an increasing number of sea-level residents access mountains for leisure (e.g., skiing, trekking, and mountaineering) or work (e.g., astronomers, miners, and guides), there is great interest in the impact of increasing altitude on cerebral functions. Barometric pressure decreases with ascent to high altitudes, resulting in a reduction in percutaneous arterial oxygen saturation (SpO2). In the traditional perspective, decreasing SpO2 at high altitudes not only causes acute mountain sickness, including headaches, nausea, and insomnia [1], but also can induce negative neuropsychological effects such as lowered executive function acting in the prefrontal cortex [2,3,4,5]. There is evidence supporting the hypothesis that acute exposure to severe hypoxic conditions at altitudes exceeding 5000 m (fraction of inspired oxygen (FIO2) = 0.100), where SpO2 decreased below 80%, decreases executive function in healthy young adults [6, 7]. Although it is generally considered that cognitive performance markedly decreases as the severity of hypoxic conditions increase, there is no empirical evidence directly examining the relationship between SpO2 and hypoxia-induced lowered executive function.
The color–word Stroop task (CWST) is widely used in experimental and clinical settings to measure executive functions based in the prefrontal cortex [8, 9], and is often used in experiments using hypoxic conditions [10,11,12]. Behavioral performance in the CWST is usually measured by comparing the delayed reaction time (RT) that occurs when a subject names a color in the incongruent trial (e.g., the word “YELLOW” printed in red ink) with that of the neutral trial (e.g., the word “XXXX” printed in red ink). This time delay is referred to as Stroop interference. However, previous studies did not evaluate the Stroop interference [10,11,12], and the impact of expose to hypoxic conditions on executive function is unclear. In this study, we used the CWST and measured Stroop interference to evaluate the executive function and postulated that exposure to hypoxic conditions may also increase Stroop interference, which appears as a slowdown in reaction time, reflecting lowered executive function.
Here we thus postulate that arterial oxygen desaturation is related to lowered executive function. To examine this issue, we aimed to clarify whether lowered executive function is associated with arterial oxygen desaturation in a crossover, within-subject design under hypoxic conditions with different oxygen concentrations. We examined the influence on executive function of acute exposure to hypoxic gas mixtures with different oxygen concentration (FIO2 = 0.209, 0.165, 0.135, 0.105; corresponding to altitudes of 0, 2000, 3500, 5000 m), in which SpO2 gradually decreases.
Methods
Participants
This study was approved by the Institutional Ethics Committee of University of Tsukuba, and was in accordance with the latest version of the Helsinki Declaration. Twenty-one right-handed young adults [mean age 20.5 ± 2.5 years (range, 18–29 years); seven females] participated in this study. No participant stated a history of respiratory, neurological, or psychiatric disorders, or had a disease requiring medical care. All participants had normal or corrected-to-normal vision and normal color vision and were Japanese native speakers, and naive to the experimental procedures for which they had volunteered. All participants were asked to refrain from exercise and the consumption of alcohol and caffeine for at least 24 h prior to each experiment so as to control for outside factors that could affect cardiovascular and executive function.
Experimental procedures
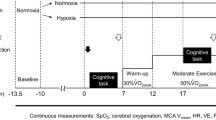
The participants underwent four conditions in 2 days: normoxic, mild hypoxic (mild; FIO2 = 0.165), moderate hypoxic (moderate; FIO2 = 0.135), and severe hypoxic (severe; FIO2 = 0.105) conditions (Fig. 1). Participants attended two conditions per day, and the order was randomized across participants. An interval of at least 48 h was imposed between the first day and the second day. We set 10 min rest between the conditions and confirmed that participants’ heart rates (HR) and SpO2 have returned to the basal levels before they breathed a gas. In all conditions, participants performed the CWST after 10-min exposure to each gas so that all participants could perform the CWST after their SpO2 had settled. Each gas was breathed from a mask that was connected to Douglas bags. Expired air was directly exhausted outside the mask so that the participants did not re-breathe the expired air. Normoxic gas was room air at sea level. Hypoxic gas was a mixture of 16.5% O2 (mild) or 13.5% O2 (moderate) or 10.5% O2 (severe) with 0.03% CO2 in nitrogen N2. Ventilation (VE), respiratory rate (RR) and end-tidal carbon dioxide pressure (PEtCO2) were measured by breath-by-breath measurements every 15 s using an Aero-monitor (AE-300 s, Minato Medical Science, Japan). HR by heart rate monitor (V800, Polar Electro, Finland) and SpO2 by a pulse oximeter (OLV-3100, Nihon Kohden, Japan) placed on the left earlobe were monitored every minute (See Fig. 2 for an overview of experimental setup).

Experimental procedure of four conditions (normoxic, mild, moderate, severe hypoxic conditions) in this study. All participants performed the CWST under four conditions

Representative photo of experimental manipulation. In all conditions, participants breathed sample gases from a mask that was connected to Douglas bags. Heart rate (HR) by heart rate monitor and percutaneous arterial oxygen saturation (SpO2) by a pulse oximeter placed on the left earlobe were monitored every minute. Participants performed the CWST after 10 min exposing to each gas
Behavioral measurements
In the current study, we used the CWST [13,14,15,16,17] in an event-related design (Fig. 3). Two rows of letters were shown on the screen and participants were instructed to decide whether the color of the letters in the top row corresponded to the color name presented in the bottom row. Participants pressed a “yes” or “no” button with their right forefingers or middle finger to respond.

Illustration of the color–word Stroop task (CWST). Examples of single trials for the neutral, congruent, and incongruent trials of the CWST are shown. For the top three examples, the correct answer is “No”. For the bottom three examples, the correct answer is “Yes”. The presented letters were written in Japanese. Translations into English are denoted in parentheses
Each experimental session consisted of 30 trials including ten neutral, ten congruent, and ten incongruent trials presented in random order. For neutral trials, the top row contained groups of X’s (XXXX) printed in red, green, blue, or yellow. For congruent trials, the top row contained the words ‘RED’, ‘GREEN’, ‘BLUE’, or ‘YELLOW’ printed in a color congruent with the color word. For incongruent trials, the color word in the top row was printed in an incongruent color to produce interference between color word and color name. For each trial, the bottom row contained the words ‘RED’, ‘GREEN’, ‘BLUE’, or ‘YELLOW’ printed in black. All words were written in Japanese. The correct answer ratio assigned to yes and no was 50%. The stimulus remained on the screen until the response was given, or for 2 s. Each trial was separated by an inter-stimulus interval showing a fixation cross for 9–13 s to avoid prediction of the timing of the subsequent trial [13, 15]. We measured RT and error rate. In addition, the (incongruent-neutral) difference, which is assumed to represent Stroop interference, was calculated. Prior to the experiment, two practice sessions were performed.
Statistical analysis
All data are presented as mean ± SE. Statistical significance was set a priori at p < 0.05 for all comparisons. A one-way repeated measures ANOVA (normoxia/mild/moderate/severe) was performed on HR and SpO2, followed by Bonferroni post hoc test. The RT and error rates of the CWST were subjected to two-way repeated measures ANOVA with trial (incongruent/neutral) and condition (normoxic/mild hypoxic/moderate hypoxic/severe hypoxic) as within-subject factors to examine whether the general tendencies for the Stroop task could be reproduced in all conditions. Because the purpose of the ANOVA was to examine occurrences of the Stroop effect, we limited the range of our analysis to the main effect of task. The Stroop effect was analyzed using one-way repeated measures ANOVA followed by Bonferroni post hoc test. Moreover, in order to clarify the relationships between executive underperformance and SpO2, we performed Pearson correlation analyses between RT in Stroop interference and SpO2.
Results
Physiological parameters
Table 1 and Fig. 4 summarize the results of the physiological parameters during the CWST in all conditions. There was a main effect on HR, VE, and SpO2 (HR: F(3, 60) = 31.745, p < 0.001; VE: F(3, 60) = 3.727, p < 0.05; SpO2: F(3, 60) = 236.94, p < 0.001). HR in the severe hypoxic condition significantly increased compared with those in the normoxic, mild, and moderate conditions (p < 0.05, Bonferroni-corrected). Moreover, HR in the moderate hypoxic condition significantly increased compared with those in the normoxic and mild hypoxic conditions. SpO2 in the severe hypoxic condition was significantly lower compared with those in the normoxic, mild, and moderate hypoxic conditions (p < 0.05, Bonferroni-corrected). Moreover, SpO2 in the moderate hypoxic condition was significantly lower compared with those in the normoxic and mild hypoxic conditions, and SpO2 in the mild hypoxic condition was significantly lower compared with that in the normoxic condition (Fig. 4; p < 0.05, Bonferroni-corrected).

The box-and-whisker plots for SpO2 under normoxic (0), mild (2000), moderate (3500), and severe (5000) hypoxic conditions. The tops and bottoms of the boxes are third and first quartiles, respectively. The upper and lower ends of the whiskers represent the highest data points within 1.5 interquartile ranges of the upper quartiles and the lowest data points within 1.5 interquartile ranges of the lower quartiles, respectively. The bands inside the boxes indicate medians. The x’s show averages. *p < 0.05 vs. normoxic condition, †p < 0.05 vs. mild hypoxic condition, ‡p < 0.05 vs. moderate hypoxic condition
Cognitive test results: Stroop interference
First, we examined whether a general tendency in the Stroop task could be reproduced in all the conditions used in this study. Reaction time (RT) and error rate were subjected to a repeated-measure two-way ANOVA with trial (incongruent/neutral) and condition (normoxia/mild/moderate/severe) being within-subject factors. The ANOVA for RT and error rate exhibited significant main effects of task (F(1,20) = 185.015, p < 0.001, Fig. 5a, and F(1,20) = 19.896, p < 0.001, Fig. 5b, respectively). These results verified that Stroop interference could be generally observed in all the conditions used in this study. To clarify the effect of exposure hypoxic conditions on a specifically defined cognitive process, we focused on the analyses of Stroop interference. The one-way ANOVA for RT in Stroop intereference (incongruent–neutral) showed a significant main effect of conditions (Fig. 6; F(3, 60) = 5.847, p < 0.01). Post hoc analyses showed that RT in the severe hypoxic condition was significantly slower compared with the other three conditions (p < 0.05, Bonferroni-corrected). On the other hand, there was no significant main effect for error rate.

The mean of reaction times (a) and error rates (b) in the incongruent and neutral trials for each condition (normoxic; 0, mild; 2000, moderate; 3500, severe; 5000). Incongruent trials exhibited significantly slower reaction times and greater error rates (***p < 0.005). Error bars indicate standard error

The mean difference of reaction times in incongruent and neutral conditions indicating the Stroop interference for each condition (normoxic; 0, mild; 2000, moderate; 3500, severe; 5000). Stroop interferences in RT were significantly slower in the severe condition (5000) than in another conditions (*p < 0.05, Bonferroni-corrected). Error bars indicate standard error
Association between cognitive performance and SpO2
We examined the association between Stroop-interference-related reaction time and SpO2 under all conditions. There was a significant negative correlation between RT in Stroop interference and SpO2 (Fig. 7; r = − 0.293, p < 0.01).

Association between Stroop interference in reaction times and SpO2 under all conditions (normoxic: blue, mild: green, moderate: orange, severe: red)
Discussion
The present study aimed to clarify the effect of hypoxic conditions on executive function and underlying mechanism with a focus on SpO2. We thus examined whether exposing subjects to acute normobaric hypoxic conditions (FIO2 = 0.165, 0.135, 0.105; corresponding to altitudes of 2000, 3500, and 5000 m) decreases CWST performance, and if the performance decreases, whether decreasing CWST performance is related to SpO2. The results revealed that Stroop interference in RT increased under severe hypoxic conditions relative to normoxic, mild, and moderate hypoxic conditions. Furthermore, there was a significant negative correlation between Stroop interference in RT and SpO2. To our knowledge, this study presents the first empirical evidence that lowered executive function is related to arterial oxygen desaturation.
Behavioral measurements for all conditions revealed a shorter RT and lower error rate in the neutral trials than in the incongruent trials. Thus, we confirmed that Stroop interference could be stably induced after acute exposure in all conditions. Based on these results, we examined the effect of acute exposure to hypoxic conditions on Stroop interference and found an acute exposure to severe hypoxic condition (FIO2 = 0.105; corresponding to an altitude of 5000 m) increased RT in Stroop interference compared with normoxic, mild, and moderate hypoxic conditions. This is consistent with result of Phillips et al. [6] reporting that acute exposure to severe normobaric hypoxic condition (FIO2 = 0.099; corresponding to an altitude of 5486 m) increased RT in a choice response task. These results suggest that normobaric hypoxic conditions under severe conditions 5000 m, where FIO2 decreased to 0.105, greatly impairs executive performance.
Next, we attempted to explore the physiological mechanisms underlying the lowered executive function. Cerebral hypoxia, which is caused by arterial oxygen desaturation and decreasing cerebral blood flow (CBF), is considered an important factor in lowered executive function. Since SpO2 levels are positively correlated with prefrontal oxygenation, prefrontal oxygenation can be affected by SpO2 [18,19,20]. Interestingly, SpO2 level, which proportionally decreases relative to the severity of hypoxic conditions, was positively correlated with lowered executive performance in the current study. This is consistent with previous studies demonstrating that cognitive performance markedly decreases as the severity of hypoxic conditions increase [4, 5, 10]. Furthermore, the meta-regression analysis showed that PaO2 levels could be the key predictor of cognitive decline [2]. Therefore, these results provide the first experimental evidence suggesting that SpO2 is associated with executive performance under hypoxic conditions in a crossover, within-subject design. In addition to arterial oxygen desaturation, cerebral vasoconstriction induced by hyperventilation can affect prefrontal oxygenation through CBF restriction [21, 22]. In this study, ventilation was increased under severe hypoxic conditions compared with normoxic conditions, however, PEtCO2, which is related to changes in CBF [23], was maintained under all conditions. Thus, we concluded that hyperventilation-induced restriction of CBF had not occurred even under the severe hypoxic conditions in this study. These results suggest that the contribution of CBF restriction to cerebral hypoxia was smaller than that of arterial oxygen desaturation. Supporting this interpretation, VE and PEtCO2 were not significantly correlated with Stroop interference in the present study.
As a neural substrate underlying lowered executive performance under severe hypoxic conditions, dysfunction of the lateral prefrontal cortex would be involved. Previous neuroimaging studies revealed that Stroop interference assessing executive function is associated with the anterior cingulate cortex (ACC) and dorsolateral prefrontal cortex (DLPFC) activation [24,25,26]. We previously showed that decreasing left DLPFC activation leads to decreased CWST performance after an acute bout of moderate exercise under hypoxic conditions [27]. Furthermore, decreasing left DLPFC activation by single-pulse transcranial magnetic stimulation (TMS) was related to a decline in TMT task performance [28]. These results lead us to postulate that decreasing CWST performance under severe hypoxic conditions could be caused by decreased activation in several prefrontal areas, especially in left DLPFC, with arterial oxygen desaturation.
Several limitations of the present study should be noted. First, we did not measure any parameters on cerebral oxygen delivery such as on cerebral oxygenation and CBF. Although we showed a significant correlation between SpO2 and Stroop interference, there is a possibility that cerebral oxygenation or CBF were involved. Future studies should directly measure cerebral oxygenation, CBF, and cerebral oxygen delivery and clarify the mechanisms of lowered executive function under hypoxic conditions. Also, we did not measure cortical activation during CWST, thus the neural substrate of lowered executive function under severe hypoxic conditions is unclear. Our previous study, using a functional near-infrared spectroscopy (fNIRS) method, showed that acute exercise improved executive function with increased task-related activation [13,14,15,16] and decreasing left DLPFC activation leads to decreased CWST performance after an acute bout of moderate exercise under hypoxic conditions [28]. Future studies should be done to reveal the neural basis of executive function decline under severe hypoxic conditions by making an experimental model for using fNIRS.
In conclusion, the current study revealed that acute exposure to severe hypoxic conditions resulting in lowered executive function depends on decreased SpO2. We thus implicate arterial oxygen desaturation as a potential physiological factor resulting in hypoxia-induced lowered executive function. The present study contributes to shedding light on how hypoxic conditions such as high altitude impact executive performance.
References
Mandolesi G, Avancini G, Bartesaghi M et al (2014) Long-term monitoring of oxygen saturation at altitude can be useful in predicting the subsequent development of moderate-to-severe acute mountain sickness. Wilderness Environ Med 25:384–391. https://doi.org/10.1016/j.wem.2014.04.015
McMorris T, Hale BJ, Barwood M et al (2017) Effect of acute hypoxia on cognition: a systematic review and meta-regression analysis. Neurosci Biobehav Rev 74:225–232. https://doi.org/10.1016/j.neubiorev.2017.01.019
Taylor L, Watkins SL, Marshall H et al (2016) The impact of different environmental conditions on cognitive function: a focused review. Front Physiol 6:372. https://doi.org/10.3389/fphys.2015.00372
Virués-Ortega J, Buela-Casal G, Garrido E, Alcázar B (2004) Neuropsychological functioning associated with high-altitude exposure. Neuropsychol Rev 14:197–224. https://doi.org/10.1007/s11065-004-8159-4
Yan X (2014) cognitive impairments at high altitudes and adaptation. High Alt Med Biol 15:141–145. https://doi.org/10.1089/ham.2014.1009
Phillips JB, Hørning D, Funke ME (2015) Cognitive and perceptual deficits of normobaric hypoxia and the time course to performance recovery. Aerosp Med Hum Perform 86:357–365. https://doi.org/10.3357/AMHP.3925.2015
Turner CE, Barker-Collo SL, Connell CJW, Gant N (2015) Acute hypoxic gas breathing severely impairs cognition and task learning in humans. Physiol Behav 142:104–110. https://doi.org/10.1016/j.physbeh.2015.02.006
MacLeod CM (1991) Half a century of research on the Stroop effect: an integrative review. Psychol Bull 109:163–203
Stroop JR (1935) Studies of interference in serial verbal reactions. J Exp Psychol 18:643–662. https://doi.org/10.1037/h0054651
Asmaro D, Mayall J, Ferguson S (2013) Cognition at altitude: impairment in executive and memory processes under hypoxic conditions. Aviat Space Environ Med 84:1159–1165. https://doi.org/10.3357/ASEM.3661.2013
Issa AN, Herman NM, Wentz RJ et al (2016) Association of cognitive performance with time at altitude, sleep quality, and acute mountain sickness symptoms. Wilderness Environ Med 27:371–378. https://doi.org/10.1016/j.wem.2016.04.008
Aquino Lemos V, Antunes HKM, Santos RVT et al (2012) High-altitude exposure impairs sleep patterns, mood, and cognitive functions. Psychophysiology 49:1298–1306. https://doi.org/10.1111/j.1469-8986.2012.01411.x
Byun K, Hyodo K, Suwabe K et al (2014) Positive effect of acute mild exercise on executive function via arousal-related prefrontal activations: an fNIRS study. Neuroimage 98:336–345. https://doi.org/10.1016/j.neuroimage.2014.04.067
Hyodo K, Dan I, Kyutoku Y et al (2016) The association between aerobic fitness and cognitive function in older men mediated by frontal lateralization. Neuroimage 125:291–300. https://doi.org/10.1016/j.neuroimage.2015.09.062
Hyodo K, Dan I, Suwabe K et al (2012) Acute moderate exercise enhances compensatory brain activation in older adults. Neurobiol Aging 33:2621–2632. https://doi.org/10.1016/j.neurobiolaging.2011.12.022
Yanagisawa H, Dan I, Tsuzuki D et al (2010) Acute moderate exercise elicits increased dorsolateral prefrontal activation and improves cognitive performance with Stroop test. Neuroimage 50:1702–1710. https://doi.org/10.1016/j.neuroimage.2009.12.023
Zysset S, Müller K, Lohmann G, von Cramon DY (2001) Color–word Matching Stroop: separating interference and response conflict. Neuroimage 13:29–36. https://doi.org/10.1006/nimg.2000.0665
Eichhorn L, Erdfelder F, Kessler F et al (2015) Evaluation of near-infrared spectroscopy under apnea-dependent hypoxia in humans. J Clin Monit Comput 29:749–757. https://doi.org/10.1007/s10877-015-9662-2
Kusaka T, Isobe K, Nagano K et al (2002) Quantification of cerebral oxygenation by full-spectrum near-infrared spectroscopy using a two-point method. Comp Biochem Physiol Part A Mol Integr Physiol 132:121–132. https://doi.org/10.1016/S1095-6433(01)00538-4
Ricci M, Lombardi P, Schultz S et al (2006) Near-infrared spectroscopy to monitor cerebral oxygen saturation in single-ventricle physiology. J Thorac Cardiovasc Surg 131:395–402. https://doi.org/10.1016/j.jtcvs.2005.07.039
Teppema LJ, Dahan A (2010) The ventilatory response to hypoxia in mammals: mechanisms, measurement, and analysis. Physiol Rev 90:675–754. https://doi.org/10.1152/physrev.00012.2009
Steinback CD, Poulin MJ (2007) Cardiovascular and cerebrovascular responses to acute isocapnic and poikilocapnic hypoxia in humans. J Appl Physiol 104:482–489. https://doi.org/10.1152/japplphysiol.00553.2007
Ide K, Eliasziw M, Poulin MJ (2003) Relationship between middle cerebral artery blood velocity and end-tidal PCO2 in the hypocapnic–hypercapnic range in humans. J Appl Physiol 95:129–137. https://doi.org/10.1152/japplphysiol.01186.2002
MacDonald AW (2000) Dissociating the role of the dorsolateral prefrontal and anterior cingulate cortex in cognitive control. Science (80−) 288:1835–1838. https://doi.org/10.1126/science.288.5472.1835
Bush G, Whalen PJ, Rosen BR et al (1998) The counting Stroop: an interference task specialized for functional neuroimaging–validation study with functional MRI. Hum Brain Mapp 6:270–282
Whalen PJ, Bush G, McNally RJ et al (1998) The emotional counting Stroop paradigm: a functional magnetic resonance imaging probe of the anterior cingulate affective division. Biol Psychiatry 44:1219–1228. https://doi.org/10.1016/S0006-3223(98)00251-0
Ochi G, Yamada Y, Hyodo K et al (2018) Neural basis for reduced executive performance with hypoxic exercise. Neuroimage 171:75–83. https://doi.org/10.1016/j.neuroimage.2017.12.091
Mull BR, Seyal M (2001) Transcranial magnetic stimulation of left prefrontal cortex impairs working memory. Clin Neurophysiol 112:1672–1675. https://doi.org/10.1016/S1388-2457(01)00606-X
Funding
This work was funded by the Special Funds for Education and Research of the Ministry of Education, Culture, Sports, Science and Technology (MEXT) entitled “Global Initiative for Human High Performance (HHP) Research Project (1111501004)”, Program for Advancing Strategic International Networks to Accelerate the Circulation of Talented Researchers of the Japan Society for Promotion of Science (JSPS) entitled “Global Initiative for Sports Neuroscience (GISN): for development of exercise prescription enhancing cognitive function (HFH27016)” and KAKENHI Grants-in-Aid for Scientific Research on Innovative Areas entitled “Next generation exercise program for developing motivation, body and mind performance (16H06405)” to H.S., and KAKENHI Grants-in-Aid for JSPS research Fellow (15J00782) to G.O.
Author information
Authors and Affiliations
Contributions
GO and HS designed the study; GO, YK, KS, and TF collected the data; GO, KH, KS, TS, and HS performed the analysis; GO and HS wrote the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflicts of interest regarding this study.
Ethical approval
All procedures and protocols performed in this study were in accordance with the ethical standards by the Physiological Society of Japan and with the 1964 Helsinki Declaration and its later amendments and were approved by the Institutional Ethical Committee of University of Tsukuba. Informed consent was obtained from all individual participants included in the study.
About this article

Cite this article
Ochi, G., Kanazawa, Y., Hyodo, K. et al. Hypoxia-induced lowered executive function depends on arterial oxygen desaturation. J Physiol Sci 68, 847–853 (2018). https://doi.org/10.1007/s12576-018-0603-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12576-018-0603-y