
Abstract
Although the production-to-consumption pathway is widely promoted to improve diet quality in developing world, its contribution to individual diet and nutrient intake remains unclear. We assessed this relationship among 377 children aged 6 to 59 months in three zones characterized by landscape diversity along an agricultural intensification gradient from the state forest of Munesa to the nearby town of Arsi Negele, Ethiopia during the two harvest seasons. A repeated interactive multiple-pass 24-h recall method was used to collect intake data. Usual intake distributions for energy, protein, iron, zinc and vitamin A were estimated using the National Cancer Institute (NCI) method and compared with estimated average requirement values to determine the prevalence of inadequate intake. The usual intake of protein, zinc and vitamin A among children were inadequate and further exacerbated by seasonality. The extent of nutrient inadequacy was higher in the diverse landscape (“near to forest” zone) than in the less diverse landscape (“distant to forest” zone). However, the diverse landscape tended to provide a better buffering capacity against seasonal energy and nutrient stress than a less diverse landscape. The age of a child positively predicted usual intakes of energy, protein, iron, zinc and vitamin A along the gradient, while breastfeeding negatively predicted these intakes. Most of the food groups and nutrients consumed were derived from on-farm production, whereas fruits and vegetables were via the market. Thus, introduction of nutrient-dense crops and increasing livestock productivity are vital to enhance consumption of diverse diets and thereby nutrients among children.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Consumption of diets low in diversity and quality is considered as the main factor for nutrient inadequacy in the diets of children in developing countries (Allen, 2012; Choudhury et al., 2019; Parikh et al., 2022). This is the case in Ethiopia where four out of five children under five years of age consume diets of inadequate diversity (Alemu et al., 2022; Jalata & Asefa, 2022). Inadequate intake of nutrients has a considerable negative impact on child growth and development (Bliznashka et al., 2021; Kakwangire et al., 2021; Miller et al., 2020). Strategies such as food fortification and supplementation are considered as effective measures to address dietary nutrient inadequacies (Dewey & Adu-afarwuah, 2008; Horton, 2006). However, limited coverage to reach all individuals, high routine intervention costs and inconsistent findings on the impact are some of the factors hindering the scale-up of these strategies in developing countries (Baek et al., 2022; Kannan et al., 2022; Saronga et al., 2022). In such contexts, agriculture-based nutrition interventions, particularly via the production-to-consumption pathway, is considered as a direct pathway to improve the consumption of diverse nutritious foods by the rural poor (Gillespie et al., 2019; Haddad, 2013). This is due to the fact that a significant proportion of the rural poor in the developing world rely on their own farm production as a main source of food for consumption (Diao et al., 2010). Yet market access can also impact consumption of diverse diets (Kiptoo et al., 2021; Nandi et al., 2021; Ogutu et al., 2020). Thus, estimating individual dietary and nutrients intakes, as well as the contribution of the different pathways is fundamental for identifying dietary gaps and developing interventions enhancing consumption of diverse diets.
Ensuring adequate availability and consumption of diversified diets among the various demographic groups is one of the strategic objectives of the food and nutrition policy of Ethiopia (Federal Democratic Republic of Ethiopia, 2018). With this regard, both on-farm production and market could play a key role in securing diverse diets to rural households (Aragie, 2014; Carletto et al., 2015; Hirvonen & Hoddinott, 2017; Kiptoo et al., 2021; Nandi et al., 2021; Ogutu et al., 2020; Sibhatu & Qaim, 2018). However, given poor market infrastructures in most rural areas (Gebiso et al., 2023; Usman & Callo-Concha, 2021), food supply is likely to be dominated by own production. Although own production dominates the supply system, production systems vary in production and diversity of food depending on the agroecology and climatic conditions of a given area and the farmer’s production orientation, targeting either for own consumption or commercial purposes. Therefore, the ability of farms to provide diverse diets to households varies (Jones, 2017) and the extent to which production and diversity in the context of smallholder farming households impact individual diets and nutrient intakes remains unclear.
Moreover, food production in smallholder farming systems is largely rain-fed and varies across seasons. Seasonal fluctuations in food production greatly affect household food availability and consequently consumption, particularly among vulnerable members of the household (Bai et al., 2020; Broaddus-Shea et al., 2018; Kaminski et al., 2016; Oluwatayo, 2019; Shell‐Duncan, 1995). This is true in the context of Ethiopia where seasonality impacts both the nutritional status of children and household food availability. Compared to the post-harvest season, which is between October to December in most parts of the country, the prevalence of wasting among children and household food insecurity were found to be higher while per capita calorie consumption was lower during the pre-harvest season (between June to August) (Belayneh et al., 2020; Hirvonen & Hoddinott, 2017; Sibhatu & Qaim, 2017). However, less is known about the association between seasonality in agricultural food production and nutrient intakes at the individual level.
To better understand the potential of agriculture to improve nutrition (Kadiyala et al., 2014; Sharma et al., 2021), there have been calls to strengthen the nature and scope of evidence on the link and contribution of diverse production systems to individual nutritional outcomes (Carletto et al., 2015; Gergel et al., 2020) in the context of smallholder farming systems. To this end, we conducted a longitudinal dietary intake assessment study that consisted of two harvest seasons to assess the link between and contribution of own production to nutrient consumption among children in three landscapes (zones) different in crop production diversity and livestock ownership across an agricultural intensification gradient in Arsi Negele district, Ethiopia (Baudron et al., 2017, 2019; Duriaux Chavarría et al., 2018). We hypothesized that a diverse production at the landscape scale would provide a diverse diet that could contribute to adequate nutrient intake for children and a better buffering capacity against seasonal energy and nutrient stress than a less diverse landscape. The key questions addressed in this study were: (1) How does the intensification gradient from the forest (a landscape with diverse production) to the nearby town (a landscape with less diverse production) relate to the diet and nutrient intakes of children during the two production seasons? (2) Which factors influence children’s nutrient intakes across the gradient?
2 Materials and methods
2.1 Study area
This study was conducted in Arsi Negele Woreda (district) in the Oromiya region of Ethiopia and covered villages (kebeles) differing in landscape diversity along an agricultural intensification gradient from the state Munesa forest to the nearby Arsi Negele town. The three study zones were characterized by (Baudron et al., 2017), (Duriaux Chavarría et al., 2018) and (Baudron et al., 2019). Zone-1 is close to the forest of Munisa and characterized by diverse crops, high prevalence of home gardens, high livestock ownership and access to the forest for feed and fuel (Fig. 1). Zone-3 is distant to the forest of Munisa but close to the town of Arsi Negele and is characterized by low crop and livestock diversity and low prevalence of home gardens. Zone-2 is intermediate. Agroecologically, the study sites are categorized as midland (“woinadega”) and are generally considered to be food secure areas (Baudron et al., 2017).

Map of the study area (a) and characteristics of the agricultural production seasons (b)
The agricultural activities in the three zones are centered around mixed crop and livestock production and follow three seasons based on the distribution of rainfall throughout the year: a long rainy season that lasts from June to September, a dry season from October to January and a short rainy season from February to April (Duriaux & Baudron, 2016). There are two crop production seasons: the Meher (during the long rainy season) and the Belg (during the short rainy season) (Fig. 1). The Meher crop harvest provides the largest quantity of food for household consumption, while the Belg crop harvest contributes a small share of the household food supply and is associated with the lean season where food stocks are gradually depleted.
2.2 Study design and participants
This study was a longitudinal community-based survey designed to assess the usual nutrient intake in the three zones and across the two harvest seasons. The first phase of the study was conducted after the main harvest season (Meher harvest) (January–February) and the second phase during the Belg harvest (July–August) of 2017. The target groups were children aged 6 to 59 months.
2.3 Sample size determination and sampling technique
We used a single population proportion formula (n) (Lwanga & Lemeshow, 1991) to determine sample size of children within the selected households. The assumptions used for the sample size estimation were a prevalence (P) estimate of 50% for inadequate intake of nutrients, a desired confidence level of 95% (z = 1.96) and desired level of precision (m) of 5%. Based on this, a minimum sample size of 384 children was estimated (n\(={\left(\frac{z}{m}\right)}^{2}P(1-P)\)). Knowing the total number of under five children in the study area (N = 3437), we further corrected the sample size for a finite population proportion using the formula (n = \(\frac{n}{1+n/N}\), where N = target population size), resulting in a sample size of 346. Given the longitudinal design of the study, an additional 20% was considered to compensate for loss to follow-up, resulting in a total sample size of 416 children. We then allocated the estimated sample size (n = 416) to the three zones, according to the proportion of households with children 6–59 months in each zone (1118, 1281 and 1038 in Zone-1, Zone-2 and Zone-3, respectively). We accessed the complete list of households with children 6–59 months in each of the three zones from the health center to construct the sampling frame for each zone. We then selected households with children 6–59 months using a systematic random sampling technique. For households with more than one child 6–59 months, we selected one child randomly using a lottery method. A total of 377 children completed the assessment in both seasons and considered in the analysis (Fig. 2).

Flow chart of sampled children from the three zones during the Meher and the Belg harvest seasons, Arsi Negele, Oromiya region, Ethiopia, 2017
2.4 Data collection
2.4.1 Dietary intake assessment
An interactive multiple-pass 24-h recall method was used to collect details of all the foods and drinks consumed by a child in the previous 24-h using a previously adapted questionnaire in the Ethiopian context (Ethiopian Public Health Institute, 2013; Gibson & Ferguson, 2008). Furthermore, duplicate/second-day recall data were collected from a subsample (20%) of randomly selected children in each zone on nonconsecutive days to adjust for day-to-day variation in the distribution of usual nutrient intakes. Breastfeeding status of each child was recorded. However, nutrients from breast milk were not considered in the intake estimation due to a high variability in composition and quantity among rural mothers in Ethiopia (Abebe et al., 2019; Gebre-Medhin et al., 1976). The interviews were conducted by trained data collectors who had prior experience in dietary data collection. The mother or primary caregiver of the child was asked to recall details, including description, source, list of ingredients, type, amount and cooking method, for each food and drink consumed and was recorded at various steps (passes) in the questionnaire. Weekdays and weekends were proportionally represented during the data collection periods. Moreover, information on the use of supplements (bi-annual vitamin A supplementation for children under five years) was also collected.
The amount of food and drinks consumed by a child was directly weighed and measured in grams using a food scale. Standardized household measures, monetary value, a play dough model and water were used to estimate either the volume or weight equivalent (by developing an item-specific conversion factor) of foods not available in the household during the time of the interview. For mixed dishes, the amount of edible portion of individual raw ingredients, cooking methods and weight of the cooked mixed dish were recorded. Based on this, the amount of each ingredient consumed from the mixed dish was estimated proportionally. Standard local recipe data were developed for foods eaten outside of the home to estimate the amount of individual ingredients consumed.
Nutrient intake from all foods and drinks consumed was calculated using the Ethiopian Food Composition Tables (Ethiopian Health & Nutrition Research Institute, 1998a, b). For missing nutrients in the Ethiopian food composition table, mostly zinc for some foods, values were imputed from the USDA Food and Nutrient Database (USDA, 2007) with adjustment for differences in moisture content. The total intake for each nutrient was estimated from contributions from all foods and drinks consumed and the source was recorded as produced or purchased. For vitamin A, an absorbable vitamin A value of 167 µg RAE for children between 6 to 11 months and 333 µg RAE for children between 12 to 59 months from a supplement (World Health Organization, 2011) was considered in the analysis.
2.4.2 Household food insecurity assessment
The Household Food Insecurity Access Scale (HFIAS) score and the Household Food Insecurity Access Prevalence (HFIAP) were used to assess household food insecurity, particularly the ‘access to food’ dimension, based on a set of nine standardized questions that assess the frequency and severity of experience related to anxiety and uncertainty about food access, insufficient quality or variety of food, and actual experiences of going without food (Coates et al., 2007). The HFIAS score was computed by adding the response value of each item, which could result in a maximum score of 27 (when the household response to all nine frequency of occurrence questions was “often” and coded with response code 3) and a minimum score of 0 (when the household respond “no” to all occurrence questions, frequency of occurrence questions was skipped by the interviewer and subsequently coded as 0). The higher the score, the more frequently the household experienced limited access to food (more food insecure). The Household Food Insecurity Access Prevalence (HFIAP) is calculated by determining the percentage of households that fall into different categories of food insecurity based on the frequency of household experiences with food insecurity conditions. Households are categorized as increasingly food insecure as they respond affirmatively to more severe conditions and/or experience those conditions more frequently. These categories include food secure, mildly food insecure, moderately food insecure and severely food insecure. A food secure household experiences none of the food insecurity (access to food) conditions, or just experiences worry, but rarely. A mildly food insecure household worries about not having enough food, or not being able to eat preferred foods, rarely, but doesn’t experience reduction in food intake pattern. A moderately food insecure household sacrifices quality, variety or desirability of the diet sometimes or often, and reduce the quantity and frequency of foods consumed. A severely food insecure household experiences any of the three most severe conditions (running out of food, going to bed hungry, or going a whole day and night without eating).
2.4.3 Minimum Dietary Diversity (MDD)
We quantified a Minimum Dietary Diversity score as defined in the WHO measurement guidelines as the number of food groups consumed out of seven food groups for nonbreastfeeding children (WHO, 2010) and out of eight food groups (where breast milk is considered the 8th food group in the newly recommended WHO/UNICEF guideline; (World Health Organization and the United Nations Children’s Fund (UNICEF), 2021) consumed for breastfeeding children in the past 24 h for two seasons. A child who received foods from 4 and more food groups when not being breastfed, and 5 and more food groups in case of breastfeeding is classified at a low risk for micronutrient inadequacy (WHO, 2010; World Health Organization and the United Nations Children’s Fund (UNICEF), 2021). Moreover, a 10 g minimum intake restriction on the amount of each food group consumed was considered (Daniels et al., 2009; Diop et al., 2021; Mahmudiono et al., 2020).
2.4.4 Wealth index
A wealth index was constructed using household’s ownership of selected assets, such as television, bicycles, and cars; dwelling characteristics (e.g. flooring materials), type of drinking water source, and toilet and sanitation facilities. Based on the value of the first component of a principal component analysis derived from their ownership data, households were allocated to wealth quantiles following the method of (Vyas & Kumaranayake, 2006) and (Rutstein, 2008).
2.5 Data analysis
Usual intake distributions for energy, protein, iron, zinc and vitamin A were estimated by adjusting for intra-individual (day-to-day) variation using the National Cancer Institute (NCI) method (Tooze et al., 2010). The NCI method models usual intake of nutrients as probability of consumption multiplied by amount consumed. Accordingly, for nutrients consumed “nearly-daily” by “nearly everyone” (nutrients with less than 10% reported zero intakes), the “amount only” (i.e. the probability of consumption is set be one) model was used, while for nutrients episodically consumed (nutrients with more than 10% reported zero intakes), the probability of consumption and amount consumed was estimated using the two-part model. In our case, the two-part model was used only for dietary vitamin A intake during the Belg harvest season (where more than 10% zero intakes were reported). For other nutrients, the “amount-only” model was used. The usual intake of vitamin A was estimated from the food sources and supplement separately for children who were supplemented and not supplemented, and thereafter combined to get the total usual vitamin A intake. We estimated standard errors (SEs) with bootstrap analysis using 200 iterations. Intakes of these nutrients were stratified by age of the child and presented as mean intakes with standard errors (SE).
To assess dietary intake adequacy, the usual intake distribution of protein, zinc and vitamin A was used and compared with the estimated average requirement values proposed by the Institute of Medicine (IOM) (for protein and vitamin A) (Institute of Medicine, 2006) and the International Zinc Nutrition Consultative Group (iZiNCG) for zinc (International Zinc Nutrition Consultative Group, 2019). The prevalence of inadequate intake of these nutrients was calculated as the proportion of the population whose usual intake was below the EAR stated in the reference values. However, for iron, the full probability approach, which compares the usual intake to requirements set at different levels of probability of inadequacy was used (Institute of Medicine, 2006). Moreover, bioavailability factors of 10% for iron and 30% for zinc were considered to assess the prevalence of inadequacy (International Zinc Nutrition Consultative Group, 2019; World Health Organization, 2006).
Due to the repeated measure of the outcome variables (energy and nutrients intake), the data were clustered at two hierarchical levels (level-1: harvest season, and level-2: children). To examine the relationship and variability simultaneously between the factors at the two hierarchical levels and the outcome variables, we used a multilevel model (linear mixed model) with unstructured covariance. However, before applying the model, a stepwise verification of the significance of individual-level effect (level-2) on outcome variation between individuals (in our case between children) was carried out using a restricted maximum likelihood test by comparing a single level model and the null multilevel model. Afterwards, for nutrients with observed individual level variation (level-2), a multilevel regression analysis with a random intercept and slope was performed.
The subsequent multilevel modelling process started with the null model (model-1). In model-1, no explanatory variables were added in the modelling process and were aimed to explain if there is a variation in the outcome variable between children. In model-2 (growth model), a level-1 variable season was included. In model-3, zone (level-2) specific analysis with cross-level interaction (with season) was conducted to assess the influence of the zones on the outcome variation. In model-4 (fully adjusted model), all variables (level-1 and level-2) combined with some cross-level interactions were considered. The detailed model results are provided in the online resource (Appendix 1). The effect of covariates on the outcome variables at different levels was estimated as a regression coefficient in the fixed effects part. The variance estimates in the random effects part were used to determine the variance at each level and the proportion of the observed outcome variation attributed at each level. To estimate the variation explained by covariates at each level, we compared the change in variance from the null model to the subsequent models. On the other hand, for nutrients where the use of a multilevel model approach was not justified (use of a random slope model was not applicable), single level multiple regression analysis was performed. As a result, a regression coefficient that only describes the relationship between the factors at different levels and usual intakes was reported.
All the usual intake and prevalence of inadequacy analysis were performed using SAS software version 9.4 (SAS Institute Inc., Cary, N.C., USA). The Simulating Intake of Micronutrients for Policy Learning and Engagement (SIMPLE) macro and its extensions which are built on the existing National Cancer Institute SAS macros (MIXTRAN and DISTRIB) was used to generate all the required parameters estimates (Luo et al., 2010). The details of this method were described elsewhere (Luo et al., 2021). Other statistical analyses were performed using Stata, version 14.0 (Stata Corp., College Station, TX, USA). Descriptive statistics were calculated and presented as frequencies, means and percentages. Mean differences were tested using a one-way analysis of variance (ANOVA) and a paired comparison test. For all analysis, a statistical level of significance was set at p value less than 0.05.
2.6 Ethical considerations
This study was approved by the Scientific and Ethical Review Committee of the Ethiopian Public Health Institute (EPHI 6.13/736). Written informed consent was obtained from the mothers or guardians of each child who participated in this study.
3 Results
3.1 General sample characteristics
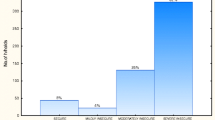
Most (65%) of the children who participated were nonbreastfeeding, aged between 24–59 months and received a biannual vitamin A supplement (59% during the Meher harvest season and 74% during the Belg harvest season) for their respective ages. More than half of the households from which children were selected had a household size between 6 to 10 members (which is more than the national average (Central Statistical Agency (CSA) [Ethiopia] and ICF, 2016)) and were food secure during the Meher harvest season. However, during the Belg harvest season, the majority of the households (67.4%) were moderately food insecure. The general characteristics of children, mothers and households included in this analysis are summarized in Table 1.
3.2 Food consumption pattern, food source and seasonality
Nearly all children consumed foods from the starchy staples (grains, roots and tubers) food group during the Meher harvest and the Belg harvest seasons (Fig. 3). A large proportion of children also consumed foods from other food groups, such as fruits, vegetables, legumes and dairy during the Meher harvest and the Belg harvest seasons respectively. However, for some food groups, in particular legumes and nuts, the proportion of children who consumed these food groups was considerably lower during the Belg harvest season (54.6% vs. 8.2%). Flesh foods and eggs were barely consumed in both harvest seasons (less than 10%). There were no statistically significant differences in the proportions of different food groups consumed across the three zones (Fig. 3b–d). The contribution of own production and market as a source of foods consumed varied among the food groups (Fig. 4). Own production was observed as the dominant source for the consumption of grains, roots and tubers, dairy products and eggs groups (more than 65%), while most consumed legumes, fruits and vegetables of any kind were obtained from the market (more than 85%) in both harvest seasons.

Proportion of children who consumed each food group in the study area and across the three zones during the Meher harvest and the Belg harvest seasons

Contribution (%) of own production and market for each food group consumed across the three zones during the Meher harvest season (a) and the Belg harvest season (b)
The mean dietary diversity score (DDS) for children aged 6–23 months and 24–59 months was low, averaging between 2.1 to 2.6 and 1.6 to 2.4, respectively). Notably, during the Belg harvest season, the DDS was significantly reduced among children aged 24–59 months (Table 2). Moreover, the proportion of children aged 6–23 months and 24–59 months who consumed the minimum recommended food groups per day in the three zones was very low (5% and 11%, respectively) and further reduced during the Belg harvest season (0% and 1.4%, respectively). Across the three zones, there was no significant difference in the mean DDS for both age groups, nor between male and female children during both harvest seasons. However, in the “distant to forest zone”, a significantly higher proportion (20.3%) of children aged 24–59 months had consumed the minimum recommended food groups per day during the Meher harvest season.
3.3 Estimated usual intakes and adequacy of energy, protein and micronutrients
The usual intakes of energy and nutrients among children differed depending on the child’s age, zones and seasons. Children aged 24–59 months generally had higher usual intakes of energy and nutrients compared to those aged 6–23 months. Regarding energy, the mean usual intakes for children aged 6–23 months were lower than those of their older counterparts (446.7 kcal/d vs. 828 kcal/d) (Table 3). Interestingly, during the Belg harvest season, there was a tendency for the mean usual energy intakes to increase for children 6–23 months, while for children aged 24–59 months, the intakes tended to decrease, except for those children in the “middle” zone where intakes slightly increased. Across the three zones, both age groups of children from the “distant to forest” zone had the highest mean usual energy intake during the Meher harvest season (430.1 kcal/d and 907.8 kcal/d among children aged 6–23 months 24–59 months, respectively). Conversely, during the Belg harvest season, the highest mean usual energy intakes for these groups (526.5 kcal/d and 895.2 kcal/d among children aged 6–23 months and 24–59 months, respectively) were observed in the “middle” zone. Children from the “near to forest” zone had the lowest mean usual energy intakes during both harvest seasons.
A large proportion of children aged 6–23 months had usual intakes below the EAR for protein (ranging from 25.4% to 40.2%) and zinc (ranging from 59.5% to 64.1%) across the three zones during the Meher harvest season (Tables 3 and 4). The prevalence of inadequate protein intake further increased, while zinc intake decreased during the Belg harvest season, except for children in the “near to forest” zone. In contrast, for children aged 24–59 months, the prevalence of inadequate intake of protein and zinc was generally low but increased during the Belg harvest season. Although inadequate intake of iron was proportionally lower compared to the other nutrients, over 20% of children aged 6–23 months were at risk in the “near to forest” and the “middle” zone. However, the prevalence decreased across the three zones during the Belg harvest season. Meanwhile, for children aged 24–59 months, the prevalence of inadequate intake of iron was low and differed little between seasons. Inadequate intake of vitamin A was prevalent among both age groups, particularly among younger children, with more than 85% affected by inadequate consumption during the Meher harvest season and increased extremely during the Belg harvest season, especially for children aged 24–59 months across the three zones (Table 4). Within a zone, no noticeable difference in inadequate consumption of nutrients was observed between male and female children of both age groups (Supplemental Tables 1 and 2). The extent of dietary inadequacy for protein, zinc, iron and vitamin A among children in the study zones had shown consistently a similar pattern during the Meher harvest and the Belg harvest seasons: low risk of inadequate intakes in the “distant to forest” zone and high risk of inadequate intakes in the “near to forest” zone.
In addition to dietary vitamin A intake, supplemental vitamin A was considered in our estimation of total vitamin A intake. Accordingly, we found that the mean intake of vitamin A from supplement was high (between 145.8 µg RAE/d to 264.5 µg RAE/d among children aged 6–23 months, and between 180 µg RAE/d to 274 µg RAE/d among children aged 24–49 months) (Table 4) and contributed to a remarkable reduction in the prevalence of inadequate intake of vitamin A among children compared to dietary vitamin A intake alone. In particular, during the Belg harvest season, the prevalence of inadequate intakes of vitamin A reduced by morethan 50% across the three zones when supplemental vitamin A was considered in the analysis. Yet, more than 15% of children across the three zones remained at risk for inadequate intake of vitamin A during the Meher harvest as well as the Belg harvest seasons.
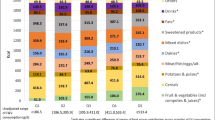
Furthermore, the sources of energy, protein, iron, zinc and vitamin A intakes among children were categorized and quantified in percentages contributed from each source: own production vs. market (Supplemental Fig. 1) and animal vs. plants (Supplemental Fig. 2). Own produced foods contributed to more than 65% of the usual intakes of dietary energy, protein, iron and zinc during both the Meher harvest and the Belg harvest seasons. Compared to the contribution of own production, the market had a limited role; only about one-third of energy, protein, iron and zinc intakes was contributed via foods purchased from the local market. However, for dietary vitamin A intake, the market had a pronounced contribution, particularly during the Belg harvest season where more than 60% of dietary vitamin A intakes in the “near to forest” and the “middle” zones were contributed through foods purchased from the market.
Plant-source foods were the main contributor (about 90%) to the usual intakes of energy, protein, iron and zinc. In contrast, animal source foods were not commonly consumed and had a very limited contribution to the usual intakes of energy and nutrients except for dietary vitamin A intake where the contribution was relatively high. Among the three zones, the contribution of plant source foods to the usual intakes of energy and nutrients was significantly higher in the “near to forest” zone than in the “distant to forest” zone during both harvest seasons. However, in terms of animal source foods contribution, a significantly higher contribution was observed in the “distant to forest” zone than in the “near to forest” zone during both harvest seasons. There was no observed significant difference in the contribution of plant and animal source foods in each zone between harvest seasons.
3.4 Factors that influence usual intakes of energy and nutrients
Based on a preliminary examination on the variability of a particular nutrient between children, two categories of nutrients were identified. The first category includes nutrients with observed variation such as usual intakes of energy, iron and zinc; and the second category includes nutrients without observed variation such as usual intakes of protein and vitamin A. For the former category, the variation attributed to a higher hierarchical level was estimated (Table 5). Accordingly, of the total observed variability, between children differences accounted for the largest source of variation for usual intakes of energy (83%) and zinc (56.0%). In contrast, only 22.3% of the total observed variability in the usual intake of iron was attributed to between children differences.
In the subsequent model, the influence of harvest season (model-2) on the usual intakes of energy, iron and zinc were further elaborated and the proportion of variation explained by seasonality was estimated. Seasonality has shown a positive influence (statistically significant) on the usual intake of energy (higher by 45 kcal during the Belg harvest season) and was able to explain a significant proportion (65.6%) of the variation observed in the usual energy intakes of a child. On the contrary, usual intakes of iron and zinc was negatively influenced by seasonality; intakes tend to decrease by a factor of 12.7 mg/d and 0.9 mg/d for iron and zinc respectively during the Belg harvest season. We found that seasonality was able to explain the majority of the variation observed in the usual intakes of iron (96.8%) and zinc (92.2%).
The estimated average intake of energy, iron and zinc was positively influenced by the position on the agricultural intensification gradient. During the Belg harvest season, intakes of energy, iron and zinc were significantly increased in the “middle” and in the “distant to forest” zones compared to the “near to forest” zone. However, the position on the agricultural intensification gradient alone could explain a very small proportion of the variation observed in the usual intake of energy, iron and zinc (Supplemental Tables 1, 2 and 3). Other factors such as age of a child were found to positively influenced the usual intakes of energy, iron and zinc, while breastfeeding status was found to negatively impact these intakes. DDS has shown no influence on the usual intakes of energy and zinc, but found negatively influence the usual intakes of iron during the Belg harvest season. All level-1 and level-2 factors combined (model-4) explained a large portion of the observed variation in energy (91.4%), iron (98.5%) and zinc (97.2%) intakes at different levels; particularly a variation within a child.
For nutrients without observed variation (second category), results from the adjusted ordinary regression analysis that only describes the relationship between factors at different levels and the outcome variables; usual intakes of protein and vitamin A are presented in Table 6. Compared to the Meher harvest season, usual intakes of protein and vitamin A were significantly lower during the Belg harvest season (by 0.8 g/kg and 500 µg RAE/d respectively). However, the intakes of these nutrients were different in magnitude between the three zones. Children from the “middle” and the “distant to forest” zones had significantly higher protein and vitamin A intakes compared to children from the “near to forest” zone during the Belg harvest season. Factors such as age of a child and position on the agricultural intensification gradient had a significant positive effect while seasonality and breastfeeding status had a significant negative effect on the usual intakes of protein and vitamin A during the Belg harvest season. The other remaining household level factors such as food insecurity status, wealth index and household size had no significant influence on the usual intakes of energy and the other nutrients.
4 Discussion
Although the importance of smallholder farming systems for household food provision is well recognized in the context of developing countries, their contribution to the consumption of adequate nutrients at individual level has seldom been analyzed. To this end, we conducted a longitudinal dietary intake assessment study during two harvest seasons to assess the link and contribution of own farm production to children’s diet and nutrient intake in three zones, located along an agricultural intensification gradient. We found, irrespective of the landscape diversity along the intensification gradient, that the diet and most of the nutrients consumed among children were not adequate and were largely derived from own farm production during both harvest seasons. Usual nutrient intakes appeared to be significantly higher for children from the less diverse landscape (“distant to forest” zone) compared to those from the diverse landscape. Furthermore, this study demonstrates the extent of the variations in the diet quality and nutrient adequacy among children in the three zones and the seasonality of diet and nutrient intakes of children.
Children’s diets in the three study zones were dominated by a limited number of food groups, mainly starchy staples, dairy products, fruits, and vegetables. Consumption of nutrient-dense animal source foods such as flesh foods and eggs were extremely low and made a very small contribution to the diet in the three zones. As a result, a large proportion of children, particularly those aged 6 to 23 months, fell short of meeting average requirements and were at risk of inadequacy for protein, iron, zinc and vitamin A during the Meher harvest season. In contrast, the risk of inadequacy for protein, iron and zinc was low among children aged 24 to 59 months. In particular for iron, less than 6% of children aged 24 to 59 months had inadequate intake. This is, in fact, due to high intake which is attributed to non-dietary sources (e.g. soil iron contamination during threshing of staple grains) via consumption of cereal products (Guja & Baye, 2018). On the other hand, both age groups had a high prevalence of inadequate intake of vitamin A. Fortunately, the routine biannual supplementation of vitamin A given to children had a remarkable contribution in reducing the prevalence of inadequate vitamin A intake among children. The overreliance on plant-based diets, particularly for vulnerable groups such as children, may compromise the diversity of diets and nutrient intakes and increase the risk of inadequacy for these nutrients. Thus, the provision of animal source foods for children in this case would have a two-fold benefit of; improving the diversity of diet as well as nutrient intakes (Neumann et al., 2002; Zhang et al., 2016). This is however conditioned by factors such as livestock ownership and production, and affordability of animal source foods for households that don’t own livestock (Daba et al., 2021; Kim et al., 2019).
Across the three zones, the distribution of low intakes of energy, protein, zinc, and vitamin A, as well as lower DDS among children showed a similar pattern during both seasons. Children from the “near to forest” zone consistently had lower intake compared to those children from the “distant to forest” zone. This deviated from our initial hypothesis which states that a diverse zone along an intensification gradient would provide a diverse diet and adequate nutrient to children. The observed contradiction could be linked to differences in animal sources foods contribution to energy and nutrient intakes (Supplemental Fig. 2), where higher contribution to usual intakes was observed in the “distant to forest” zone. Otherwise there was no significant difference observed in the contribution of market to nutrient intakes due to the proximity of a zone across the gradient to the nearby town. A similar finding has been reported from a study in Kenya, where production diversity was not associated with child dietary diversity (Muthini et al., 2020a, b). On the contrary, in studies where a direct association between production diversity and dietary diversity was demonstrated (Baudron et al., 2017; Esaryk et al., 2021; Kumar et al., 2015; Tobin et al., 2019), differences in the intrahousehold food distribution among household members were not considered and the scale of analysis was often at larger scale (national level) compared to our study which was conducted at village level. Moreover, despite the diversity in production along the gradient, household decision regarding which foods to consume from their own production could contribute to the observed disparities (Aberman & Roopnaraine, 2018).
The extent of nutrient inadequacy and low consumption of diverse diets among children was further exacerbated by seasonal fluctuations in agricultural food production. Compared to the Meher harvest season, the prevalence of inadequate dietary intake of protein, vitamin A and zinc was increased and almost none of the children had the minimum recommended number of food groups per day during the Belg harvest season. The effect of seasonality was more profound among children aged 24 to 59 months. However, the magnitude by which intakes were influenced depended on the age of a child. Except for the intake of energy among children aged 6 to 23 months, nutrients intake among both age groups of children tended to decrease during the Belg harvest season, which coincides with the lean season in the study area. The low prevalence of inadequate intake of iron and zinc among children aged 6 to 23 months during the Belg harvest season was primarily due to differences in the proportion of children between seasons rather than improvement in intake levels. However, the increased intake of energy among children aged 6 to 23 months during the Belg harvest could be due to age related differences in their intake capacity to consume food, as these children had grown older by five months during the Belg harvest season. Across the three zones, seasonality had shown a slight change in energy and nutrient intakes among children, particularly those aged 24 to 59 months, in the “near to forest” zone compared to the “distant to forest” zone. This could partially affirm the hypothesis that a diverse landscape could provide a better buffering capacity against seasonal energy and nutrient stress than a less diverse landscape. Nevertheless, energy and nutrient intakes remained higher in the less diverse landscape (“distant to forest” zone) during both seasons.
Studies have documented seasonal variations in energy and nutrient intake among children in rural African households. These studies consistently reported significantly higher energy and nutrient intake during the post-harvest season. Differences in food consumption pattern, resulting from the seasonality of food production and access, between the harvest and pre-harvest seasons were the main factors contributing to seasonal differences in energy and nutrient intake among children (Arsenault et al., 2014; Caswell et al., 2020; Waswa et al., 2021). Our findings are comparable to these findings on the influence of seasonality on nutrient intake and low consumption of food groups, particularly legumes, nuts and animal source foods during the Belg harvest season, which may explain the seasonal variation in nutrient intake among children in the three zones. Household food insecurity, which is often strongly influenced by seasonality (Aweke et al., 2022; Bonuedi et al., 2022), had no influence on the usual intake of nutrients in our study.
A range of factors related to individual children and households was considered in our analysis to identify the factors that influence the usual intake of energy and nutrients. Individual-level factors, such as the age of a child and breastfeeding status influenced nutrient intakes among children. However, DDS which is often positively associated with nutrient intake adequacy among children (Diop et al., 2021; Kennedy et al., 2007; Moursi et al., 2008; Wondafrash et al., 2016), had no influence except for the usual intake of iron. Moreover, we found that wealth index, household size and household food insecurity had no influence on the usual intake of energy and nutrients. The lack of association between nutrient intake and household characteristics could be related to the fact that young child nutrition is less sensitive to changes in household and demographic characteristics (Saaka & Osman, 2013). The variation observed in the usual intake of energy, iron, and zinc among children was largely (more than two-thirds) explained by seasonality, and very little by the position of the zone across the intensification gradient. Therefore, addressing seasonal nutrient stress could reduce the risk of nutrient inadequacy among children in these three zones.
The interplay of own production and market in the food supply system played a substantial role in terms of the food and nutrients consumed by children in the three zones. Most of the food groups consumed were sourced from farm production, which consequently led to the largest share of energy, protein, iron and zinc being consumed by children. The market contributed a significant share of consumed legumes, fruits and vegetables of any kind, which are good sources of protein and vitamin A. Although own production outweighed the market’s contribution for foods and nutrients consumed, neither of the two pathways provided adequate nutrients for a child to meet the requirements for protein, zinc, and vitamin A. This finding would provide a precautionary measure on the current contrasting views on the relative importance of own production pathway over market and vice versa as an effective strategy for improving dietary quality in the context of developing countries (Chegere & Stage, 2020; Muthini et al., 2020a, b; Olabisi et al., 2021; Sinyolo et al., 2021). A deeper understanding of the context, beyond household-level consumption, is required to draw a conclusive remark on the relative importance of both production and market pathways in the food supply system.
The strength of our study comes from three elements. First, the longitudinal nature of the study design enabled us to assess the consumption pattern and nutrient intakes among children during the Meher harvest and the Belg harvest seasons, which are associated with different degrees of household food availability. In addition to dietary intakes, nutrient intakes from supplement (e.g., biannual vitamin A supplementation) were included in the estimation of nutrient adequacy. Second, the source of each food consumed was recorded and the proportion contributed from own production and market was estimated. Third, we applied an appropriate statistical method and procedure to estimate the usual intake distribution and prevalence of inadequate intakes of nutrients among children. However, some precautions should be considered in interpreting the findings from this analysis. First, given the small area and sample size included in this study, little can be said for the larger and more diverse landscape in rural Ethiopia. Thus, our study could be extended to other landscapes in different parts of the country to explore the role of landscape diversity in the provision of foods and nutrients for a particular group. Second, the contribution of breast milk to the usual intakes of nutrients for breastfeeding children was not considered and at the same time, we refrained from making assumptions based on average breastmilk intake to estimate nutrient intake due to the recent recommendation by the Intake-Center for Dietary Assessment and others (Abebe et al., 2019; Deitchler et al., 2020). Thus, the prevalence of inadequate intake of nutrients for breastfeeding children in this study is less likely to be overestimated.
The present research provided empirical evidence on the relationship between position of a landscape along an agricultural intensification gradient and consumption of foods and nutrients by rural children. DDS, a proxy indicator, has been widely used to demonstrate the link between production diversity and consumption at the household level (Kissoly et al., 2020; Nkonde et al., 2021). However, DDS is reported to be a less sensitive indicator to explicitly measure such an association at an individual level (Muthini et al., 2020a, b). This was also observed in our analysis where DDS was not significantly different across the three zones which differed in production diversity. Measurements that go beyond the use of DDS (e.g., nutrient consumption level) are required to quantify the contribution of the production systems at landscape-level to individual diets and nutrient consumption. Beside the dietary sources, biannual high dose supplemental vitamin A given to children through the health extension program had contributed to the reduction (by more than 50%) of the prevalence of inadequate intake of vitamin A. Thus, understanding the role of production, market and other health interventions will allow policymakers and stakeholders to identify the gaps and opportunities for designing nutrition-sensitive agricultural interventions that could improve nutrient intakes and reduce the influence of seasonality. Moreover, the findings of this study add to our understanding of the contribution of the agricultural pathways (production vs. market) to food and nutrient consumption in the context of developing countries. Future exploratory analysis that aims to address the association between production, market and diet quality should consider the source of foods consumed and intra-household food and nutrient distribution.
5 Conclusion
The diet and nutrients consumed by children in the three zones were inadequate to meet their requirements and were highly influenced by seasonality and individual level factors such as the age and breastfeeding status of a child. However, the extent of nutrient inadequacy for protein, zinc, iron and vitamin A among children was higher in the diverse landscape (“near to forest” zone) than in the less diverse landscape (“distant to forest” zone) along an agricultural intensification gradient. Thus, improving the current production system in these zones through the introduction of nutrient-dense crops, increasing livestock productivity, and using agricultural inputs and technologies are vital to enhance the consumption of diverse diets and to reduce the prevalence of inadequate nutrient intake among children.
Data availability
The data that support the findings of this study are available on request from the corresponding author via the Ethiopian Public Health Institute.
Code availability
Codes used for analysis are available on request from the corresponding author.
References
Abebe, Z., Haki, G. D., Schweigert, F. J., Henkel, I. M., & Baye, K. (2019). Low breastmilk vitamin A concentration is prevalent in rural Ethiopia. European Journal of Clinical Nutrition, 73(8), 1110–1116. https://doi.org/10.1038/s41430-018-0334-4
Aberman, N., & Roopnaraine, T. (2018). Understanding household preferences on the production, consumption, and sale of nutritious crops. (Issue DeWalt). International Food Policy Research Institute (IFPRI), Washington, D.C. https://doi.org/10.2499/9780896292864_03
Alemu, T. G., Techane, M. A., Wubneh, C. A., Assimamaw, N. T., Belay, G. M., Tamir, T. T., Muhye, A. B., Kassie, D. G., Wondim, A., Terefe, B., Tarekegn, B. T., Ali, M. S., Fentie, B., Gonete, A. T., Tekeba, B., Kassa, S. F., Desta, B. K., Ayele, A. D., Dessie, M. T., & Atalell, K. A. (2022). Spatial variation and determinates of dietary diversity among children aged 6–23 months in Ethiopia: Spatial and multilevel analysis using Ethiopian Demography Health Survey (EDHS) 2019. Archives of Public Health, 80(1), 1–13. https://doi.org/10.1186/s13690-022-00905-3
Allen, L. H. (2012). Global dietary patterns and diets in childhood: Implications for health outcomes. Annals of Nutrition and Metabolism, 61, 29–37. https://doi.org/10.1159/000346185
Aragie, E. A. (2014). Household production, home consumption and market supply in peasant economies: The case of Ethiopia. African Journal of Agricultural Economics and Rural Development, 2(6), 155–164. http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.674.8797&rep=rep1&type=pdf
Arsenault, J. E., Nikiema, L., Allemand, P., Ayassou, K. A., Lanou, H., Moursi, M., De Moura, F. F., & Martin-Prevel, Y. (2014). Seasonal differences in food and nutrient intakes among young children and their mothers in rural Burkina Faso. Journal of Nutritional Science, 3. https://doi.org/10.1017/jns.2014.53
Aweke, C. S., Sassi, M., Lahiff, E., & Wordofa, M. G. (2022). Seasonality and food security among smallholder rural households in eastern Ethiopia: Evidence from panel data analysis. Cogent Economics and Finance, 10(1). https://doi.org/10.1080/23322039.2022.2035492
Baek, Y., Ademi, Z., Paudel, S., Fisher, J., Tran, T., Romero, L., & Owen, A. (2022). Economic evaluations of child nutrition interventions in low- and middle-income countries : Systematic review and quality appraisal. Advances in Nutrition, 13, 282–317.
Bai, Y., Naumova, E. N., & Masters, W. A. (2020). Seasonality of diet costs reveals food system performance in East Africa. Science Advances, 6(49), 1–11. https://doi.org/10.1126/sciadv.abc2162
Baudron, F., Duriaux Chavarría, J. Y., Remans, R., Yang, K., & Sunderland, T. (2017). Indirect contributions of forests to dietary diversity in Southern Ethiopia. Ecology and Society, 22(2). https://doi.org/10.5751/ES-09267-220228
Baudron, F., Schultner, J., Duriaux, J. Y., Gergel, S. E., & Sunderland, T. (2019). Agriculturally productive yet biodiverse: Human benefits and conservation values along a forest-agriculture gradient in Southern Ethiopia. Landscape Ecology, 34(2), 341–356. https://doi.org/10.1007/s10980-019-00770-6
Belayneh, M., Loha, E., & Lindtjørn, B. (2020). Seasonal variation of household food insecurity and household dietary diversity on wasting and stunting among young children in a drought prone area in South Ethiopia: A cohort study. Ecology of Food and Nutrition, 60(1), 1–26. https://doi.org/10.1080/03670244.2020.1789865
Bliznashka, L., Perumal, N., Yousafzai, A., & Sudfeld, C. (2021). Diet and development among children aged 36–59 months in low-income countries. Archives of Disease in Childhood, archdischild-2021–323218. https://doi.org/10.1136/archdischild-2021-323218
Bonuedi, I., Kornher, L., & Gerber, N. (2022). Agricultural seasonality, market access, and food security in Sierra Leone. Food Security, 14(2), 471–494. https://doi.org/10.1007/s12571-021-01242-z
Broaddus-Shea, E. T., Thorne-Lyman, A. L., Manohar, S., Nonyane, B. A. S., Winch, P. J., & West, K. P. (2018). Seasonality of consumption of nonstaple nutritious foods among young children from Nepal’s 3 agroecological zones. Current Developments in Nutrition, 2(9), 3–5. https://doi.org/10.1093/cdn/nzy058
Carletto, G., Ruel, M., Winters, P., & Zezza, A. (2015). Farm-level pathways to improved nutritional status: Introduction to the special issue. Journal of Development Studies, 51(8), 945–957. https://doi.org/10.1080/00220388.2015.1018908
Caswell, B. L., Talegawkar, S. A., Siamusantu, W., West, K. P., & Palmer, A. C. (2020). Within-person, between-person and seasonal variance in nutrient intakes among 4- to 8-year-old rural Zambian children. British Journal of Nutrition, 123(12), 1426–1433. https://doi.org/10.1017/S0007114520000732
Central Statistical Agency (CSA) [Ethiopia] and ICF. (2016). Ethiopia Demographic and Health survey. Addis Ababa, Ethiopia and Rockville, Maryland, USA. CSA and ICF.
Chegere, M. J., & Stage, J. (2020). Agricultural production diversity, dietary diversity and nutritional status: Panel data evidence from Tanzania. World Development, 129(December 2019), 104856. https://doi.org/10.1016/j.worlddev.2019.104856
Choudhury, S., Headey, D. D., & Masters, W. A. (2019). First foods: Diet quality among infants aged 6–23 months in 42 countries. Food Policy, 88(August), 101762. https://doi.org/10.1016/j.foodpol.2019.101762
Coates, J., Swindale, A., & Bilinsky, P. (2007). Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide (v3) (Issue August). Washington: Food and Nutrition Technical Assistance II Project (FANTA-II Project), Academy for Educational Development (AED), Washington DC: FANTA.
Daba, A. K., Murimi, M., Abegaz, K., & Hailu, D. (2021). Determinants and constraints to household-level animal source food consumption in rural communities of Ethiopia. Journal of Nutritional Science, 10, 1–10. https://doi.org/10.1017/jns.2021.52
Daniels, M. C., Adair, L. S., Popkin, B. M., & Truong, Y. K. (2009). Dietary diversity scores can be improved through the use of portion requirements : An analysis in young Filipino children. European Journal of Clinical Nutrition, 63, 199–208. https://doi.org/10.1038/sj.ejcn.1602927
Deitchler, M., Arimond, M., Carriquiry, A., Hotz, C., & Tooze, J. A. (2020). Planning and Design Considerations for Quantitative 24-Hour Recall Dietary Surveys in Low-and Middle-Income Countries. (Issue January).
Dewey, K. G., & Adu-afarwuah, S. (2008). Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Maternal and Child Nutrition, 4, 24–85. https://doi.org/10.1111/j.1740-8709.2007.00124.x
Diao, X., Hazell, P., & Thurlow, J. (2010). The role of agriculture in african development. World Development, xx(x). https://doi.org/10.1016/j.worlddev.2009.06.011
Diop, L., Becquey, E., Turowska, Z., Huybregts, L., Ruel, M. T., & Gelli, A. (2021). Standard minimum dietary diversity indicators for women or infants and young children are good predictors of adequate micronutrient intakes in 24–59-month-old children and their nonpregnant nonbreastfeeding mothers in Rural Burkina Faso. Journal of Nutrition, 151(2), 412–422. https://doi.org/10.1093/jn/nxaa360
Duriaux, J. & Baudron, F. (2016). Understanding people and forest interrelations along an intensification gradient in Arsi-Negele, Ethiopia. In Liz Deakin, M. Kshatriya, & T. Sunderland (Eds.), Agrarian change in tropical landscapes (pp. 14–53). Center for International Forestry Research. https://doi.org/10.17528/cifor/005867
Duriaux Chavarría, J. Y., Baudron, F., & Sunderland, T. (2018). Retaining forests within agricultural landscapes as a pathway to sustainable intensification: Evidence from Southern Ethiopia. Agriculture, Ecosystems and Environment, 263(May), 41–52. https://doi.org/10.1016/j.agee.2018.04.020
Esaryk, E. E., Reynolds, S. A., Fernald, L. C. H., & Jones, A. D. (2021). Crop diversity is associated with higher child diet diversity in Ethiopia, particularly among low-income households, but not in Vietnam. Public Health Nutrition, 24(17), 5857–5868. https://doi.org/10.1017/S1368980021003281
Ethiopian Public Health Institute. (2013). Ethiopia National Food Consumption Survey. Addis Ababa, Ethiopia.
Ethiopian Health and Nutrition Research Institute. (1998a). Food Composition Table for Use in Ethiopia. Part III. Addis Ababa, Ethiopia.
Ethiopian Health and Nutrition Research Institute. (1998b). Food Composition Table for Use in Ethiopia. Part IV. Addis Ababa, Ethiopia.
Federal Democratic Republic of Ethiopia. (2018). Food and nutrition policy. Addis Ababa, Ethiopia. https://doi.org/10.1177/156482658600800208
Gebiso, T., Ketema, M., Shumetie, A., & Leggesse, G. (2023). Drivers of crop commercialization in central and southern Oromia. Discover Food. https://doi.org/10.1007/s44187-023-00055-7
Gebre-Medhin, M., Vahlquist, A., Hofvander, Y., Uppsäll, L., & Vahlquist, B. (1976). Breast milk composition in Ethiopian and Swedish mothers. I. Vitamin A and β carotene. American Journal of Clinical Nutrition, 29(4), 441–451. https://doi.org/10.1093/ajcn/29.4.441
Gergel, S. E., Powell, B., Baudron, F., Wood, S. L. R., Rhemtulla, J. M., Kennedy, G., Rasmussen, L. V., Ickowitz, A., Fagan, M. E., Smithwick, E. A. H., Ranieri, J., Wood, S. A., Groot, J. C. J., & Sunderland, T. C. H. (2020). Conceptual links between landscape diversity and diet diversity: A roadmap for transdisciplinary research. BioScience, 70(7), 563–575. https://doi.org/10.1093/biosci/biaa048
Gibson, R., & Ferguson L., E. (2008). An interactive 24-hour recall of assessing the adequacy of iron and zinc intakes in developing countries. ILSI Press, Washington D.C.
Gillespie, S., Poole, N., van den Bold, M., Bhavani, R. V., Dangour, A. D., & Shetty, P. (2019). Leveraging agriculture for nutrition in South Asia: What do we know, and what have we learned? Food Policy, 82(November 2018), 3–12. https://doi.org/10.1016/j.foodpol.2018.10.012
Guja, H., & Baye, K. (2018). Extrinsic iron from soil contributes to Hb regeneration of anaemic rats: Implications for foods contaminated with soil iron. British Journal of Nutrition, 119(8), 880–886. https://doi.org/10.1017/S0007114518000338
Haddad, L. (2013). From nutrition plus to nutrition driven: How to realize the elusive potential of agriculture for nutrition? Food and Nutrition Bulletin, 34(1), 39–44. https://doi.org/10.1177/156482651303400105
Hirvonen, K., & Hoddinott, J. (2017). Agricultural production and children’s diets: Evidence from rural Ethiopia. Agricultural Economics (united Kingdom), 48(4), 469–480. https://doi.org/10.1111/agec.12348
Horton, S. (2006). The Economics of Food Fortificatio. American Society for Nutrition, 136, 1068–1071.
International Zinc Nutrition Consultative Group. (2019). Determining the risk of zinc deficiency: Assessment of dietary zinc intake. In IZiNCG Technical Brief (Vol. 3, Issue 3). https://static1.squarespace.com/static/56424f6ce4b0552eb7fdc4e8/t/5c1abb0870a6adf8eb61d85b/1545255689912/IZiNCG_Technical+Brief+%239_final.pdf
Institute of Medicine. (2006). Dietary DRI Reference Intakes: The Essential Guide to Nutrient Requirements.
Jalata, D. D., & Asefa, B. G. (2022). Trends and determinants of dietary diversity in children aged 6–59 months in Ethiopia: Analysis of 2005–2016 Demographic and health survey. Current Developments in Nutrition, 6(10), nzac135. https://doi.org/10.1093/cdn/nzac135
Jones, A. D. (2017). Critical review of the emerging research evidence on agricultural biodiversity, diet diversity, and nutritional status in low- and middle-income countries. Nutrition Reviews, 75(10), 769–782. https://doi.org/10.1093/nutrit/nux040
Kadiyala, S., Harris, J., Headey, D., Yosef, S., & Gillespie, S. (2014). Agriculture and nutrition in India: Mapping evidence to pathways. Annals of the New York Academy of Sciences, 1331(1), 43–56. https://doi.org/10.1111/nyas.12477
Kakwangire, P., Moss, C., Matovu, N., Atukunda, P., Westerberg, A. C., Iversen, P. O., & Muhoozi, G. (2021). The association between dietary diversity and development among children under 24 months in rural Uganda: Analysis of a cluster-randomised maternal education trial. Public Health Nutrition, 24(13), 4286–4296. https://doi.org/10.1017/S136898002100077X
Kaminski, J., Christiaensen, L., & Gilbert, C. L. (2016). Seasonality in local food markets and consumption: Evidence from Tanzania. Oxford Economic Papers, 68(3), 736–757. https://doi.org/10.1093/oep/gpw013
Kannan, A., Tsoi, D., Xie, Y., Horst, C., Collins, J., & Flaxman, A. (2022). Cost-effectiveness of Vitamin A supplementation among children in three sub-Saharan African countries : An individual- based simulation model using estimates from Global Burden of Disease 2019. PLoS ONE, 1–13. https://doi.org/10.1371/journal.pone.0266495
Kennedy, G. L., Pedro, M. R., Seghieri, C., Nantel, G., & Brouwer, I. (2007). Dietary diversity score is a useful indicator of micronutrient intake in non-breast-feeding Filipino children. The Journal of Nutrition, 137, 472–477. https://doi.org/10.1093/jn/137.2.472
Kim, S. S., Nguyen, P. H., Tran, L. M., Abebe, Y., Asrat, Y., Tharaney, M., & Menon, P. (2019). Maternal behavioural determinants and livestock ownership are associated with animal source food consumption among young children during fasting in rural Ethiopia. Maternal and Child Nutrition, 15, 1–9. https://doi.org/10.1111/mcn.12695
Kiptoo, E., Waswa, L. M., & Ayuya, O. I. (2021). Linking farm production to household diets: Evidence from two low potential areas in Kenya. Cogent Food and Agriculture, 7(1). https://doi.org/10.1080/23311932.2021.1913842
Kissoly, L. D., Karki, S. K., & Grote, U. (2020). Diversity in Farm Production and Household Diets: Comparing Evidence From Smallholders in Kenya and Tanzania. Frontiers in Sustainable Food Systems, 4(June), 1–13. https://doi.org/10.3389/fsufs.2020.00077
Kumar, N., Harris, J., & Rawat, R. (2015). If they grow it, will they eat and grow ? Evidence from Zambia on agricultural diversity and child undernutrition. The Journal of Development Studies, 51(8), 1060–1077. https://doi.org/10.1080/00220388.2015.1018901
Luo, H., Dodd, K. W., Arnold, C. D., Caswell, B., & Engle-stone, R. (2010). Simple Macro User Manual.
Luo, H., Dodd, K. W., Arnold, C. D., & Engle-Stone, R. (2021). Introduction to the simple Macro, a Tool to increase the accessibility of 24-hour dietary recall analysis and modeling. Journal of Nutrition, 151(5), 1329–1340. https://doi.org/10.1093/jn/nxaa440
Lwanga, s. K., & Lemeshow, S. (1991). Sample size determination in health studies: A Practical Manual. World Health Organization.
Mahmudiono, T., Andadari, D. P. P. S., & Segalita, C. (2020). Difference in the association of food security and dietary diversity with and without imposed ten grams minimum consumption. Journal of Public Health Research, 9(3), 316–320. https://doi.org/10.4081/jphr.2020.1736
Miller, L. C., Neupane, S., Joshi, N., Shrestha, M., Neupane, S., Lohani, M., & Thorne-Lyman, A. L. (2020). Diet quality over time is associated with better development in rural Nepali children. Maternal and Child Nutrition, 16(3). https://doi.org/10.1111/mcn.12964
Moursi, M. M., Arimond, M., Dewey, K. G., Trèche, S., Ruel, M. T., & Delpeuch, F. (2008). Dietary diversity is a good predictor of the micronutrient density of the diet of 6- to 23-month-old children in Madagascar. Journal of Nutrition, 138(12), 2448–2453. https://doi.org/10.3945/jn.108.093971
Muthini, D., Nzuma, J., & Nyikal, R. (2020a). Farm production diversity and its association with dietary diversity in Kenya. Food S, 12, 1107–1120.
Muthini, D., Nzuma, J., & Qaim, M. (2020b). Subsistence production, markets, and dietary diversity in the Kenyan small farm sector. Food Policy, 97(July), 101956. https://doi.org/10.1016/j.foodpol.2020.101956
Nandi, R., Nedumaran, S., & Ravula, P. (2021). The interplay between food market access and farm household dietary diversity in low and middle income countries: A systematic review of literature. Global Food Security, 28, 100484. https://doi.org/10.1016/j.gfs.2020.100484
Neumann, C., Harris, D. M., & Rogers, L. M. (2002). Contribution of animal source foods in improving diet quality and function in children in the developing world. Nutrition Research, 22(1–2), 193–220. https://doi.org/10.1016/S0271-5317(01)00374-8
Nkonde, C., Audain, K., Kiwanuka-Lubinda, R. N., & Marinda, P. (2021). Effect of agricultural diversification on dietary diversity in rural households with children under 5 years of age in Zambia. Food Science and Nutrition, 9(11), 6274–6285. https://doi.org/10.1002/fsn3.2587
Ogutu, S. O., Gödecke, T., & Qaim, M. (2020). Agricultural commercialisation and nutrition in smallholder farm households. Journal of Agricultural Economics, 71(2), 534–555. https://doi.org/10.1111/1477-9552.12359
Olabisi, M., Obekpa, H. O., & Liverpool-Tasie, S. (2021). Is growing your own food necessary for dietary diversity? Evidence from Nigeria. Food Policy, 104(July), 102144. https://doi.org/10.1016/j.foodpol.2021.102144
Oluwatayo, I. B. (2019). Vulnerability and adaptive strategies of smallholder farmers to seasonal fluctuations in production and marketing in southwest Nigeria. Climate and Development, 11(8), 659–666. https://doi.org/10.1080/17565529.2018.1521328
Parikh, P., Semba, R., Manary, M., Swaminathan, S., Udomkesmalee, E., Bos, R., Poh, B. K., Rojroongwasinkul, N., Geurts, J., Sekartini, R., & Nga, T. T. (2022). Animal source foods, rich in essential amino acids, are important for linear growth and development of young children in low- and middle-income countries. Maternal and Child Nutrition, 18(1), 1–12. https://doi.org/10.1111/mcn.13264
Rutstein, S. O. (2008). The DHS wealth index : Approaches for Rural and Urban Areas (Issue 60).
Saaka, M., & Osman, S. M. (2013). Does household food insecurity affect the nutritional status of preschool children aged 6–36 months? International Journal of Population Research, 2013, 1–12. https://doi.org/10.1155/2013/304169
Saronga, H. P., Manji, K., Liu, E., Duggan, C. P., & Menzies, N. A. (2022). Cost-effectiveness of zinc supplementation for prevention of childhood diarrhoea in Tanzania. Public Health Nutrition, 25(7), 1979–1988. https://doi.org/10.1017/S1368980022000568
Sharma, I. K., Di Prima, S., Essink, D., & Broerse, J. E. W. (2021). Nutrition-sensitive agriculture: A systematic review of impact pathways to nutrition outcomes. Advances in Nutrition, 12(1), 251–275. https://doi.org/10.1093/advances/nmaa103
Shell-Duncan, B. (1995). Impact of seasonal variation in food availability and disease stress on the health status of nomadic Turkana children: A longitudinal analysis of morbidity, immunity, and nutritional status. American Journal of Human Biology, 7(3), 339–355. https://doi.org/10.1002/ajhb.1310070310
Sibhatu, K. T., & Qaim, M. (2018). Review: The association between production diversity, diets, and nutrition in smallholder farm households. Food Policy, 77(October 2017), 1–18. https://doi.org/10.1016/j.foodpol.2018.04.013
Sibhatu, K. T., & Qaim, M. (2017). Rural food security, subsistence agriculture, and seasonality. PLoS ONE, 12(10), 1–15. https://doi.org/10.1371/journal.pone.0186406
Sinyolo, S., Murendo, C., Nyamwanza, A. M., Sinyolo, S. A., Ndinda, C., & Nwosu, C. O. (2021). Farm production diversification and dietary diversity among subsistence farming households: Panel data evidence from south africa. Sustainability, 13(18). https://doi.org/10.3390/su131810325
Tobin, D., Thiede, B. C., & Tobin, D. (2019). Does crop diversity at the village level influence child nutrition security ? Evidence from 11 sub-Saharan African countries. Population and Environment, 41, 74–97.
Tooze, J. A., Kipnis, V., Buckman, D. W., Carroll, R. J., Freedman, L. S., Guenther, P. M., Krebs-Smith, S. M., Subar, A. F., & W.Dodd, K. (2010). A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. NIH-PA Author Manuscript, 29(27). https://doi.org/10.1002/sim.4063.A
USDA. (2007). Composition of foods raw, processed, prepared. USDA National nutrient database for standard reference SR-19. Available at: www.Nal.Usda.Gov/Fnic/Foodcomp/Data/SR19/Sr19_doc.Pdf, Accessed A September.
Usman, M. A., & Callo-Concha, D. (2021). Does market access improve dietary diversity and food security? Evidence from Southwestern Ethiopian smallholder coffee producers. Agricultural and Food Economics, 9(1). https://doi.org/10.1186/s40100-021-00190-8
Vyas, S., & Kumaranayake, L. (2006). Constructing socio-economic status indices: How to use principal components analysis. Health Policy and Planning, 21(6), 459–468. https://doi.org/10.1093/heapol/czl029
Waswa, L. M., Jordan, I., Krawinkel, M. B., & Keding, G. B. (2021). Seasonal variations in dietary diversity and nutrient intakes of women and their children (6–23 months) in Western Kenya. Frontiers in Nutrition, 8(March). https://doi.org/10.3389/fnut.2021.636872
WHO. (2010). Indicators for assessing infant and young child feeding practices part 2: measurement. WHA55 A55/, 19. http://apps.who.int/iris/bitstream/handle/10665/44306/9789241599290_eng.pdf?sequence=1%0Ahttp://whqlibdoc.who.int/publications/2008/9789241596664_eng.pdf%5Cnhttp://www.unicef.org/programme/breastfeeding/innocenti.htm%5Cnhttp://innocenti15.net/declaration
Wondafrash, M., Huybregts, L., Lachat, C., Bouckaert, K. P., & Kolsteren, P. (2016). Dietary diversity predicts dietary quality regardless of season in 6–12-month-old infants in south-west Ethiopia. Public Health Nutrition, 19(14), 2485–2494. https://doi.org/10.1017/S1368980016000525
World Health Organization. (2006). Guidelines on food fortification with micronutrients.
World Health Organization. (2011). Guideline: Vitamin A supplementation in infants and children 6 – 59 months of age. In World Health Organization.
World Health Organization and the United Nations Children’s Fund (UNICEF). (2021). Indicators for assessing infant and young child feeding practices: definitions and measurement methods.
Zhang, Z., Goldsmith, P. D., & Winter-Nelson, A. (2016). The Importance of Animal Source Foods for Nutrient Sufficiency in the Developing World: The Zambia Scenario. Food and Nutrition Bulletin, 37(3), 303–316. https://doi.org/10.1177/0379572116647823
Funding
The research data collection and logistics was financially supported by Ethiopian Public Health Institute (EPHI).
Author information
Authors and Affiliations
Contributions
Tibebu Moges Chinasho designed the study, performed the statistical analysis and composed the draft manuscript. Frédéric Baudron, Hanqi Luo, Inge D. Brouwer, Roseline Remans, and Jeroen C.J. Groot supervised the analysis, draft manuscript preparation and reviewed the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. The study was approved by the Scientific and Ethical Review Committee of the Ethiopian Public Health Institute (EPHI 6.13/736).
Consent to participate
Written informed consent was obtained from the mothers or guardians of each child who participated in this study.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Moges, T., Baudron, F., Luo, H. et al. Inadequacy of nutrients in children’s diets across seasons along an agricultural intensification gradient in Ethiopia. Food Sec. (2024). https://doi.org/10.1007/s12571-024-01463-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12571-024-01463-y