
Abstract
Background
In Idiopathic Dilated Cardiomyopathy (IDC) an imbalance between myocardial oxygen consumption and supply has been postulated. The ensuing subclinical myocardial ischemia may contribute to progressive deterioration of LV function. β-blocker is the therapy of choice in these patients. However, not all patients respond to the same extent. The aim of this study was to elucidate whether differences between responders and non-responders can be identified with respect to regional myocardial perfusion reserve (MPR) and contractile performance.
Methods
Patients with newly diagnosed IDC underwent Positron Emission Tomography (PET) scanning using both 13N-ammonia as a perfusion tracer (baseline and dipyridamole stress), and 18F-fluoro-deoxyglucose as a metabolism tracer, and a dobutamine stress MRI. MRI and PET were repeated 6 months after maximal β-blocker therapy. MPR (assessed by PET) as well as wall motion score (WMS, assessed by MRI) were evaluated in a 17 segment-model. Functional response to β-blocker therapy was assigned as a stable or improved LVEF or diminished LVEF.
Results
Sixteen patients were included (age 47.9 ± 11.5 years; 12 males, LVEF 28.6 ± 8.4%). Seven patients showed improved LVEF (9.7 ± 3.1%), and nine patients did not show improved LVEF (−3.4 ± 3.9%). MPR improved significantly in responders (1.56 ± .23 to 1.93 ± .49, P = .049), and MPR decreased in non-responders; however, not significantly (1.98 ± .70 to 1.61 ± .28, P = .064), but was significantly different between both groups (P = .017) after β-blocker therapy. A significant correlation was found between change in perfusion reserve and change in LVEF: a decrease in perfusion reserve was associated with a decrease in LVEF and vice versa. Summed rest score of wall motion in responders improved from 26 to 21 (P = .022) whereas in non-responders no change was observed from 26 to 25) (P = ns). Summed stress score of wall motion in responders improved from 23 to 21 (P = .027) whereas in non-responders no change was observed from 27 to 26) (P = ns).
Conclusion
In IDC patients, global as well as regional improvement after initiation of β-blocker treatment is accompanied by an improvement in regional perfusion parameters. On the other hand in IDC patients with further left ventricular function deterioration after initiation of β-blocker therapy this is accompanied by a decrease in perfusion reserve.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
After the description of a beneficial effect of beta-blocker therapy in a first small series of patients1 many reports have followed and at present β-blocker therapy is standard in heart failure patients (ESC guidelines). However, it is known that patients respond highly variable to beta-blocker therapy.2-4 Non-response percentages up to 18% have been found.5 Identification of the cause of this variability may further tailor individual treatment approaches and perhaps give insights in pathophysiologic mechanisms. Elucidation of the relation between myocardial perfusion and contractility in heart failure patients may shed new light on the progressive deterioration of left ventricular (LV) function. In a previous study, we have showed that in idiopathic dilated cardiomyopathy regions with a lower myocardial perfusion reserve (MPR) are present. Furthermore, we found that global systolic wall stress correlated negatively with MPR.6,7 It has therefore been postulated that progressive deterioration is in part a consequence of ischemic episodes.8 One of the possible mechanisms by which β-blocker therapy that are so successful in heart failure may be the effects on oxygen demand and supply.
Idiopathic dilated cardiomyopathy (IDC) is a disease characterized by dilated, poorly contracting ventricles, in the absence of coronary artery disease or primary valvular disease, or other specified causes of myocardial dysfunction.
It has been shown that endothelial function is impaired in patients with IDC,9 although the epicardial coronary arteries do not show significant abnormalities. Also myocardial perfusion abnormalities have been found.10 Myocardial ischemia as a cause for the progression of the disease could be caused by microvascular abnormalities, endothelial dysfunction, autonomic disregulation of the microvasculature, and high intramural pressure, due to increased Laplace wall stress.11 This may cause myocardial stunning or hibernation, and give rise to myocardial fibrosis, which promotes further LV dysfunction and dilatation.12
We have previously found ischemia-like myocardial contractile responses during dobutamine stress echocardiography in patients with IDC.13 Furthermore, we have observed a relation between ischemia and LV dysfunction14 and a decreased MPR in patients with IDC.7 In addition, low MPR was paralleled by high LV systolic wall stress.7 β-blocker therapy has been recognized as an excellent treatment for heart failure, including IDC,15 however, the prognosis of patients in whom β-blockers are ineffective is poor. β-blocker therapy may worsen heart failure.5 Prediction of β-blocker efficacy could be useful in tailoring the treatment regimen of heart failure patients.16 Previously, Bennett et al, described the effects of metoprolol on rest regional perfusion in six patients with chronic heart failure due to IDC. They found a small increase in LVEF without improved regional perfusion.17 The question remains what the effect of early initiation of beta-blocker therapy is in IDC patients in the early stages of the disease. In this respect not just rest perfusion but especially perfusion reserve is of our major interest.18
The purpose of this study was to substantiate whether the relation between MPR assessed with positron emission tomography (PET) and ischemic wall motion abnormalities during dobutamine stress magnetic resonance imaging (MRI) is different between responders and non-responders after β-blocker treatment.
Methods
Study Group
Patients with newly diagnosed IDC and mild chronic heart failure (CHF) were eligible for the study. All patients underwent coronary angiography, which showed normal epicardial coronary arteries. The diagnosis of IDC, was based on a combination of clinical variables (LV dilation, global decreased contraction patterns) and the absence of epicardial coronary artery disease, and the absence of other clear causes of cardiomyopathy (significant valvular disease, alcohol abuse, use of cardiotoxic agents in the past, like adriamycine, or active myocarditis). None of the patients were on β-blocker therapy at the start of this study. PET as well as MRI scanning was performed before initiation of β-blocker therapy. Other medication such as angiotensin converting enzyme (ACE) inhibitors, and diuretics were allowed. After the first PET and MRI scan patients were titrated up to the maximal tolerated β-blocker dose (up to 200 mg metoprolol per day) and PET and MRI were repeated after 6 months. Patients with systemic hypertension (systolic blood pressure >150 mm Hg, diastolic blood pressure >95 mm Hg), diabetes mellitus, hypercholesterolemia (>6 mmol · L−1) or any other systemic illness were excluded. All patients gave written, informed consent, and the protocol was approved by the Institutional Review Board. Patients were identified as responders or non-responders. Functional response to β-blocker therapy was assigned as a stable or improved LV ejection fraction (LVEF) or diminished LVEF.19,20
Protocol for PET Imaging
Patients underwent dynamic rest 13N-ammonia, 13N-ammonia dipyridamole stress and gated 18FDG PET imaging using a one-day protocol. In brief, PET studies were performed after patients had discontinued vasoactive medication for five plasma half-lives and had refrained from caffeinated beverages for a minimum of 12 h before the studies. Imaging was performed in the supine position with a Siemens Ecat Exact HR + PET camera (Siemens CTI, Knoxville Tennessee, USA). Measured resolution of the system was 6 mm at full width half maximum. Data were automatically corrected for accidental coincidence and dead time. Patients were positioned with the help of a rectilinear scan. Photon attenuation was measured using a retractable external ring source filled with germanium-68/gallium-68. Dipyridamole perfusion imaging was performed infusing dipyridamole (.56 mg · kg−1 in 4 minutes). Imaging was started by injecting 400 MBq of 13N-ammonia 6 minutes after the start of dipyridamole infusion and continued for 15 minutes.
To stimulate 18FDG uptake, patients were given 75 g of glucose orally just before scanning or were given 500 mg acipimox (Nedios, Byk, The Netherlands) orally to lower circulating free fatty acids 90 minutes before the scanning procedure. To prevent side-effects of acipimox (e.g., skin rash), 250 mg of aspirin was administered orally 5 minutes before acipimox intake. After completion of the 13N-ammonia data acquisition, 200 MBq of 18FDG was injected intravenously, followed by a PET dynamic acquisition procedure. The total 18FDG PET acquisition time was 40 minutes, with the last 20 minutes acquired in gated mode with 16 frames per cardiac cycle. The length of each gate was based on the current RR-interval. The RR-interval was allowed to vary ±10%. Data were corrected for attenuation using the transmission scan and were reconstructed using filtered back-projection (Hann filter: .5 pixels/cycle).
Analysis of PET Data
From the PET data, dynamic parametric polar maps were constructed.21 Myocardial blood flow data were corrected for partial volume effect and spill over and quantified by the Hutchins model.22 Briefly, myocardial and blood time-activity curves manually derived from regions of interest over the heart and ventricular chamber are fitted using a three compartment model for 13N-ammonia, yielding rate constants for tracer uptake and retention. Rest, stress, and perfusion flow reserve (dipyridamole/rest ratio) was calculated by dividing the dipyridamole 13N-ammonia stress study with the 13N-ammonia rest study. Rest 13N-ammonia was corrected for heart rate and blood pressure product.
Regional FDG metabolism in the segment with the highest myocardial perfusion during dipyridamole stress was assigned as the optimal FDG metabolic value. The remaining FDG segments were normalized on this segment. Regional FDG metabolism was reduced when FDG metabolism was <50% (abnormal FDG segments) and normal when FDG was ≥50% (normal FDG segments). The last frames (20 minutes acquisition time) of the dynamic gated FDG PET studies were summed and transformed into static studies and used for further data analysis with the help of the quantitative gated SPECT (QGS) program. Regional MPR as well as FDG metabolism were evaluated in an automatically derived 17 segment-model. Based on the gated FDG images, left ventricular end systolic (LVESV) and end diastolic volumes (LVEDV) as well as left ventricular ejection fraction (LVEF) were computed.23
Protocol for MRI Imaging
DSMR was performed at a 1.5 Tesla MRI System (Magnetom Sonata; Siemens Medical Solutions; Erlangen; Germany) according to a standard dobutamine-atropine stress protocol (5, 10, 20, and 30 μg · kg−1 · min−1 dobutamine) until 85% of the age-predicted target heart rate was achieved. Imaging at each stress level was performed in 1 long-, and 3 short-axis views and contiguous short-axis views at peak stress using a segmented steady-state free precession sequence (TR 3 ms, TE 1.5 ms, FA 60°, 15 views per segment). Myocardial segments (17 segment-model) were evaluated by a panel of three observers (DL, PvdV, RAT). Wall motion score (WMS) for each individual segment was given: 1 = normal, 2 = hypokinetic, 3 = akinetic, 4 = dyskinetic. Summed rest score (SRS) = the total summed wall motion score during rest MRI; summed stress score (SSS) = the total summed wall motion score during dobutamine stress. Myocardial ischemia was defined by new or worsening wall motion abnormalities in at least one myocardial segment during dobutamine stress.
Statistical Analysis
Data were expressed as mean ± SD. Categorical measures are presented as frequencies with percentages. Patients whose LVEF had improved by more than 5% were defined as responders. Differences between responders and non-responders were compared with t-test, Wilcoxon rank-sum test, and Chi-square when appropriate. A P-value <.05 was considered significant.
Results
Patients
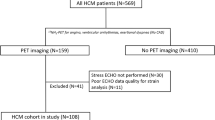
Between May 2003 and March 2007 a total of 29 eligible patients (age 50 ± 13; 21 male) have been selected for this study. Eight of them did not give informed consent or had an indication for ICD implantation, 5 patients had a MRI of low quality, the remaining 16 patients are subject of this study (age 47.9 ± 11.5 years; 12 male). Left ventricular ejection fraction before inclusion was 28.6 ± 8.4%. Four patients were judged to have heart failure NYHA class I, 11 class II, and 1 class III. The majority of patients were treated with an ACE-inhibitor, almost half of the patients with diuretics (Table 1).
Global Analysis Responders and Non-Responders
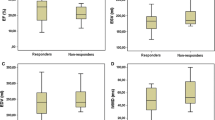
Mean LVEF of responders (n = 7) at baseline was 28.4% ± 7.5 and improved to 38.1% ± 6.9 (P < .0001), whereas mean LVEF of non-responders (n = 9 (56%)) at baseline was 30.3% ± 8.4 and decreased to 27.4% ± 10.2 (P = .029) (Table 2). A lower MPR at baseline was found in the responders vs. the non-responders, whereas a significant relation between change in MPR and change in LVEF was found (Figure 1). MPR improved significantly in responders (1.56 ± .23 to 1.93 ± .49, P = .049), whereas a small non-significant decrease was observed in non-responders (1.98 ± .70 to 1.61 ± .28, P = .064). The change in MPR after β-blocker therapy was different between the two groups (P = .017). The number of normal FDG segments increased in responders while in non-responders a decrease was observed (16 vs. −14, respectively; P = .028). The change in the number of abnormal FDG segments did not show any differences between the two groups (−2 vs. −5, respectively; P = .17). Summed rest score of wall motion in responders improved from 26 to 21 (P = .022) whereas in non-responders no change was observed from 26 to 25) (P = ns). Summed stress score of wall motion in responders improved from 23 to 21 (P = .027) whereas in non-responders no change was observed from 27 to 26) (P = ns).

Relation between change in myocardial perfusion reserve (MPR) and change in left ventricular ejection fraction (LVEF)
Segmental Analysis
At baseline the mean MPR per segment was 1.79 ± .67 and after β-blocker therapy it was 1.75 ± .56 (P = .32). In non-responders the mean MPR per segment was 1.98 ± .70 and after β-blocker therapy it was 1.61 ± .28 (P = .05). Whereas in responders the mean MPR per segment was 1.56 ± .23 and after β-blocker therapy it was 1.93 ± .70 (P = .049). On FDG PET in the responders a lower number of non-viable as well as viable-ischemic segments were found. After β-blocker therapy the number of normal FDG segments increased and the number of abnormal FDG segments decreased in responders. The opposite appeared in non-responders (Table 2).
A total of 269 segments could be analyzed at baseline on MRI, after 6 months of maximal β-blocker treatment 266 segments. Mean WMS per segment at rest baseline was 1.56 ± .83 and during dobutamine stress 1.49 ± .90 (P = ns) with a mean sum difference score (SDS) of −17 (36 segments improved, 20 segments deteriorated). After β-blocker treatment at rest WMS was 1.39 ± .78, and during dobutamine stress of 1.43 ± .83 (P = ns) with a SDS of 9 (23 segments improved, 27 segments deteriorated). Segments that improved during dobutamine stress MRI had an MPR of 2.01 ± .50, segments that deteriorated had an MPR of 1.74 ± .47 (P = .005). MPR difference in segments with WMS improvement and WMS worsening before and after β-blocker treatment was significantly different (P = .01, Figure 2).

MPR is dipyridamole stress 13N-ammonia divided by rest stress 13N-ammonia. Deterioration is a decrease in motion score of at least 1 category. MPR 2 (PET scan 6 months after β-blocker therapy) was significantly different to MPR 1 (PET scan prior to β-blocker therapy) (P = .01). Rest perfusion between no deterioration and deterioration groups was not significantly different (P = .07). *SEM. MPR, myocardial perfusion reserve
Discussion
In the present study we show that patients in whom β-blocker elicited a beneficial MPR response also had an improvement in LVEF. The improvement in MPR significantly related to improvement in LV function. The opposite was found in patients with an unfavorable response to β-blocker therapy. They had a decrease in MPR which was accompanied by a decrease in LVEF. Our present findings corroborate coronary flow reserve measurements in IDC patients.24 In that study also a correlation between regional flow reserve and regional contractile function was found. In responders non-viable segments shifted to an increased number of viable segments, whereas in non-responders the opposite was noticed. Myocardium subjected to repetitive stunning based on microvascular pathology may show a prolonged yet reversible reduction in systolic function that can be associated with a significant downregulation of glucose and oxidative metabolism despite relative normal myocardial blood flow.25 β-blocker therapy restores the wall motion disorder, and this may lead to normalization of glucose metabolism, mainly in segments with relative low MPR, as visible in the non-responders. Hasegawa et al, found that myocardial FDG metabolism in patients with reduced LVEF in the absence of significant coronary artery disease could be used as a predictor of LVEF improvement after β-blocker therapy.16 We observed in our study that the number of normal FDG segments increased in responders while in non-responders a decrease was observed. Heilbrunn et al suggested improved contractility to be directly related to β-receptor upregulation.26 Bennett et al, found conflicting results between patients with ischemic cardiomyopathy and dilated, non-ischemic cardiomyopathy.17 Patients with non-ischemic cardiomyopathy showed no improvement after β-blocker therapy. Their results are in agreement with our study, we also did not find differences in rest myocardial perfusion before and after β-blocker therapy. However, we evaluated the MPR after dipyridamole and observed differences between responders and non-responders. Of note, compared to our study, LVEF in their study was severely reduced (mean LVEF 13%; our study 28.4%) and patients were defined as chronic heart failure whereas we included newly diagnosed patients. Severe LV dysfunction will lead to more remodeling and is accompanied by fibrosis formation.12
The question about cause or consequence of the reduction in MPR cannot precisely be answered. However, it is remarkable that a low perfusion reserve at baseline was not associated with a further deterioration and vice versa a high baseline MPR was not associated with a LV function improvement. This may imply a reverse relationship; however, complicated mechanisms may be involved dealing with redistributing perfusion between epi- and endocardial layers. There may be a significant transmural gradient in the density of β-receptors in ischemic and non-ischemic cardiomyopathy. Measurement of receptor density using PET 11C-CGP as radioligand could also be an important tool for estimation of β-receptor status during treatment, since it directly reflects changes in myocardial contractility.27 A limitation of this study is the relative small number of included patients; however, the segmental analysis justifies our conclusion.
In conclusion IDC patients responding to β-blocker therapy show an improvement in MPR in concert with improved wall motion parameters. These data underscore the importance of subclinical ischemia in patients with IDC and may direct further research in the elucidation of the difference between responders and non-responders.
References
Waagstein F, Hjalmarson A, Varnauskas E, Wallentin I. Effect of chronic beta-adrenergic receptor blockade in congestive cardiomyopathy. Br Heart J 1975;37:1022-36.
Anderson JL, Lutz JR, Gilbert EM, et al. A randomized trial of low-dose beta-blockade therapy for idiopathic dilated cardiomyopathy. Am J Cardiol 1985;55:471-5.
Eichhorn EJ, Grayburn PA, Mayer SA, et al. Myocardial contractile reserve by dobutamine stress echocardiography predicts improvement in ejection fraction with beta-blockade in patients with heart failure: The Beta-Blocker Evaluation of Survival Trial (BEST). Circulation 2003;108:2336-41.
Waagstein F, Caidahl K, Wallentin I, Bergh CH, Hjalmarson A. Long-term beta-blockade in dilated cardiomyopathy. Effects of short- and long-term metoprolol treatment followed by withdrawal and readministration of metoprolol. Circulation 1989;80:551-63.
Lechat P, Escolano S, Golmard JL, et al. Prognostic value of bisoprolol-induced hemodynamic effects in heart failure during the Cardiac Insufficiency BIsoprolol Study (CIBIS). Circulation 1997;96:2197-205.
Tio RA, Slart RH, de Boer RA, et al. Reduced regional myocardial perfusion reserve is associated with impaired contractile performance in idiopathic dilated cardiomyopathy. Neth Heart J 2009;17:470-4.
van den Heuvel AF, van Veldhuisen DJ, van der Wall EE, et al. Regional myocardial blood flow reserve impairment and metabolic changes suggesting myocardial ischemia in patients with idiopathic dilated cardiomyopathy. J Am Coll Cardiol 2000;35:19-28.
de Boer RA, Pinto YM, van Veldhuisen DJ. The imbalance between oxygen demand and supply as a potential mechanism in the pathophysiology of heart failure: The role of microvascular growth and abnormalities. Microcirculation 2003;10:113-26.
Treasure CB, Vita JA, Cox DA, et al. Endothelium-dependent dilation of the coronary microvasculature is impaired in dilated cardiomyopathy. Circulation 1990;81:772-9.
Juilliere Y, Marie PY, Danchin N, et al. Radionuclide assessment of regional differences in left ventricular wall motion and myocardial perfusion in idiopathic dilated cardiomyopathy. Eur Heart J 1993;14:1163-9.
Ingwall JS, Nascimben L, Gwatmey JK. Heart failure: Is the pathology due to calcium overload or to mismatch in energy supply and demand? In: Gwatmey JK, Briggs MG, Allen PD, editors. Heart failure: Basic and clinical aspects. New York: Marcel Dekker; 2008. p. 667-700.
Frangogiannis NG. The pathological basis of myocardial hibernation. Histol Histopathol 2003;18:647-55.
de Jong RM, Cornel JH, Crijns HJ, van Veldhuisen DJ. Abnormal contractile responses during dobutamine stress echocardiography in patients with idiopathic dilated cardiomyopathy. Eur J Heart Fail 2001;3:429-36.
van Veldhuisen DJ, van den Heuvel AF, Blanksma PK, Crijns HJ. Ischemia and left ventricular dysfunction: A reciprocal relation? J Cardiovasc Pharmacol 1998;32:S46-51.
Foody JM, Farrell MH, Krumholz HM. Beta-blocker therapy in heart failure: Scientific review. JAMA 2002;287:883-9.
Hasegawa S, Kusuoka H, Maruyama K, et al. Myocardial positron emission computed tomographic images obtained with fluorine-18 fluoro-2-deoxyglucose predict the response of idiopathic dilated cardiomyopathy patients to beta-blockers. J Am Coll Cardiol 2004;43:224-33.
Bennett SK, Smith MF, Gottlieb SS, et al. Effect of metoprolol on absolute myocardial blood flow in patients with heart failure secondary to ischemic or nonischemic cardiomyopathy. Am J Cardiol 2002;89:1431-4.
Tio RA, Dabeshlim A, Siebelink HM, et al. Comparison between the prognostic value of left ventricular function and myocardial perfusion reserve in patients with ischemic heart disease. J Nucl Med 2009;50:214-9.
de Groote P, Delour P, Mouquet F, et al. The effects of beta-blockers in patients with stable chronic heart failure. Predictors of left ventricular ejection fraction improvement and impact on prognosis. Am Heart J 2007;154:589-95.
Lowes BD, Gilbert EM, Abraham WT, et al. Myocardial gene expression in dilated cardiomyopathy treated with beta-blocking agents. N Engl J Med 2002;346:1357-65.
Choi Y, Hawkins RA, Huang SC, et al. Parametric images of myocardial metabolic rate of glucose generated from dynamic cardiac PET and 2-[18F]fluoro-2-deoxy-d-glucose studies. J Nucl Med 1991;32:733-8.
Hutchins GD, Schwaiger M, Rosenspire KC, et al. Noninvasive quantification of regional blood flow in the human heart using N-13 ammonia and dynamic positron emission tomographic imaging. J Am Coll Cardiol 1990;15:1032-42.
Slart RH, Bax JJ, de Jong RM, et al. Comparison of gated PET with MRI for evaluation of left ventricular function in patients with coronary artery disease. J Nucl Med 2004;45:176-82.
Skalidis EI, Parthenakis FI, Patrianakos AP, Hamilos MI, Vardas PE. Regional coronary flow and contractile reserve in patients with idiopathic dilated cardiomyopathy. J Am Coll Cardiol 2004;44:2027-32.
Di Carli MF, Prcevski P, Singh TP, et al. Myocardial blood flow, function, and metabolism in repetitive stunning. J Nucl Med 2000;41:1227-34.
Heilbron BG, Gin KG. Beta-adrenoceptor blocking agents for the treatment of heart failure. Int J Clin Pharmacol Ther 1996;34:231-5.
de Jong RM, Willemsen ATM, Slart RHJA, et al. Myocardial beta-adrenoceptor downregulation in idiopathic dilated cardiomyopathy measured in vivo with PET using the new radioligand (S)-[C-11]CGP12388. Eur J Nucl Med Mol Imaging 2005;32:443-7.
Acknowledgments
This study was supported by the Netherlands Heart Foundation Grant 2001B099.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Slart, R.H.J.A., Tio, R.A., van der Vleuten, P.A. et al. Myocardial perfusion reserve and contractile pattern after beta-blocker therapy in patients with idiopathic dilated cardiomyopathy. J. Nucl. Cardiol. 17, 479–485 (2010). https://doi.org/10.1007/s12350-010-9216-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-010-9216-4