
Abstract
Introduction
The ACO Registry Study was a multicenter, prospective, observational cohort study aiming to clarify the situation of asthma–chronic obstructive pulmonary disease (COPD) overlap (ACO) within the COPD population using the Japanese Respiratory Society (JRS) criteria. We reported the proportion of patients who met the ACO criteria among the COPD population at study registration.
Methods
Using data collected at registration, we investigated the implementation of each diagnostic examination/test required for ACO diagnosis in the full analysis set. Among patients with data necessary for ACO diagnosis, ACO/non-ACO patients with/without asthma diagnosed by a physician and proportions of inhaled corticosteroid (ICS) treatments for COPD were calculated.
Results
Of 708 patients analyzed, 396 (55.9%) had the data necessary for ACO diagnosis, and 312 (44.1%) did not. The proportions of patients who underwent laboratory and respiratory function tests (peripheral blood eosinophil count [79.8%], fractional exhaled nitric oxide [63.7%], airway reversibility [46.8%], and total immunoglobulin [Ig] E/specific IgE [33.3%]) were lower than those who underwent subjective examinations (perennial allergic rhinitis [100%], asthma before age 40 years [97.2%], and variable/paroxysmal respiratory symptoms [94.5%]). Among patients with the data necessary for ACO diagnosis and without asthma complications according to the physician’s diagnosis, 15.1% (33/219) met the ACO criteria. Of patients who met the ACO criteria, 74.3% (75/101) received ICS, and 25.7% (26/101) did not. By comparison, among patients who did not meet the ACO criteria, 35.6% (105/295) were receiving ICS, and 64.4% (190/295) were not.
Conclusions
The proportion of objective laboratory and physiological tests was lower than expected, despite study sites having the clinical resources for objective tests. Most ACO patients were being treated with ICS as recommended in the JRS treatment guidelines. Attempts should be made to further increase the proper use of ICS among these patients in Japan.
Trial Registration
ClinicalTrials.gov, NCT03577795.
Similar content being viewed by others


Why carry out this study? |
We carried out this study to reveal the implementation of examinations/tests regarding each Asthma–COPD overlap (ACO) diagnostic criterion suggested by Japanese Respiratory Society (JRS) and inhaled corticosteroid (ICS) treatment for chronic obstructive pulmonary disease (COPD) in the multicenter, ACO Registry Study population, using the data collected at the time of registration. |
What were the study outcomes/conclusions? |
Overall, the proportion of objective laboratory and physiological tests implemented was lower than expected despite the study sites having the specialists and resources available to conduct the necessary tests. |
Some patients were not treated with ICS despite having ACO. |
What was learned from the study? |
Our results suggest that, in addition to examinations, objective tests should be conducted to detect asthma complications based on the ACO diagnostic criteria to provide appropriate ICS treatment. |
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent airflow limitation and is the third leading cause of death globally, accounting for over three million deaths in 2019 [1, 2]. COPD-related deaths are projected to increase within the next 15 years because of advancing age and increased risk factors such as environmental pollution, occupational exposure to dust, and cigarette smoking.
Asthma–COPD overlap (ACO) is a condition that displays features of both COPD and asthma [3]. According to current guidelines, the treatment for ACO differs from COPD alone in that the use of inhaled corticosteroids (ICS) is recommended for ACO [4,5,6]. Accurate diagnosis of ACO patients is crucial, as late or inaccurate diagnosis, together with inappropriate treatment, likely results in disease progression [7]. As both asthma and COPD are chronic respiratory conditions, which share common features, it is not easy to determine when both conditions are present. In order to diagnose ACO using objective indicators in daily clinical practice, the Japanese Respiratory Society (JRS) has proposed ACO diagnostic criteria [8]. It is currently unknown to what extent clinical tests to diagnose ACO are carried out in real clinical practice, despite the ACO diagnostic criteria proposed by the JRS.
The prospective, multicenter, epidemiological ACO Registry Study aimed to clarify the proportion of ACO patients within the COPD population in clinical practice using the JRS criteria and to observe patient transition over time [9]. Using data at the time of registration, the first analysis of the ACO Registry Study showed that 25.5% of the 396 patients who had the data necessary for ACO diagnosis met the diagnostic criteria for ACO, and 312 (44.1%) of the overall 708 patients lacked the examinations and test results necessary for an accurate ACO diagnosis [9]. In the present report, we describe the results of a more detailed analysis of the actual status of each ACO diagnostic evaluation and ICS treatment for COPD in the ACO Registry Study population, using the data at the time of registration, which included patients who did not have the data necessary to establish an ACO diagnosis.
Methods
Study Design
The study design has been previously published [9]. This was a multicenter, observational, prospective cohort study with a 2-year follow-up. The study was conducted at 27 sites in Japan, comprising medical institutions with respiratory specialists who were able to perform the examinations/tests required to establish an ACO diagnosis based on the JRS ACO criteria (Table S1 in the supplementary material) [8, 9] as part of routine clinical practice. A program of consecutive patient enrolment, with registration and eligibility checks managed at a single central office, was implemented for this study.
Approval of the protocol and other study documentation was given by the Ethics Committee of Tohoku University Hospital. The study conduct adhered to the general principles outlined in the Declaration of Helsinki, as well as national and international ethical guidelines for medical and health research involving humans. All participants provided informed consent prior to study registration. Data collection, storage, and use complied with the Personal Information Protection Act and local and international laws and regulations related to data protection.
Patients
Full details of the inclusion and exclusion criteria have been previously published [9]. Briefly, the target population included consecutively enrolled male and female outpatients at least 40 years of age, with post-bronchodilator forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) of less than 70%, and any of the COPD characteristics according to the JRS ACO diagnostic criteria.
Study Endpoints
The endpoints for this prespecified analysis were the proportions of patients who underwent the evaluations for each ACO diagnostic criterion in the full analysis set (FAS), which comprised all patients with data necessary for ACO diagnosis and patients lacking the data necessary for ACO diagnosis at the time of registration. Another endpoint was the proportions of patients who met the JRS ACO diagnostic criteria among patients with COPD, with and without a physician’s diagnosis of asthma complications for patients with the data available for ACO diagnosis. Further endpoints included the proportions of ACO and non-ACO patients who were using/not using an ICS at the time of registration, and the demographics, clinical characteristics, and implementation of examinations/tests required for the ACO diagnostic criteria among ACO and non-ACO patients stratified according to the use/non-use of ICS.
Data Collection
Data were collected on examinations and tests to confirm the ACO diagnosis according to the JRS diagnostic criteria as reported in the primary study [3, 8, 9]. Investigators collected data in electronic case report forms, and patients completed self-administered questionnaires.
Statistical Analysis
The details of the statistical analysis have been published elsewhere [9]. The planned sample size was 700 patients determined on the basis of the proportions of patients meeting the ACO diagnostic criteria reported in previous studies [10,11,12]. The data cutoff for this analysis was August 2019 (i.e., identical to that of the baseline analysis [9]). The FAS included patients with available data for at least one item required for ACO diagnosis, collected at one or more of the time points after patient registration. Numbers and proportions of patients were used for categorical variables, and summary statistics, including mean (standard deviation [SD]), median (range), quartiles, or frequency, were used for quantitative variables. For categorical variables, the chi-square test was used to compare groups when more than 80% of cells of the contingency table had values of 5 or more, and Fisher’s exact test was used in other cases. For quantitative variables with homogeneity of variance, a one-way analysis of variance (ANOVA) was used. For quantitative variables with a heterogeneity of variance, Welch’s ANOVA was used. All statistical tests were conducted in an exploratory manner; no multiplicity adjustment or data imputation was performed. The statistical software used for the analysis was Statistical Analysis Software Version 9.4 or higher (SAS Institute Inc., Cary, NC, USA).
Results
Patient Characteristics
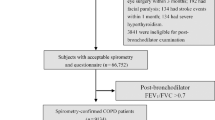
A total of 717 patients were registered; nine were ineligible or withdrew consent and were excluded, and 708 patients were included in the FAS (Fig. 1). The patient background data have been previously described [9] and are shown in Table S2 in the supplementary material. Of note, 90.1% of patients were male and had a mean age of 73.5 years. A history of smoking was reported by 87.1% of patients, and 11.2% were current smokers. Regarding the respiratory function of patients at registration, the mean post-bronchodilator FEV1/FVC% was 52.0%, and the mean predicted post-bronchodilator %FEV1 was 65.1%.

Summary of patient disposition within the study
Proportions of Patients Who Underwent Evaluation for Each ACO Diagnostic Criterion
Figure 2 shows the proportion of patients who underwent examinations/tests among the 708 FAS patients; 396 patients had the data necessary for ACO diagnosis, and 312 patients lacked the data necessary for ACO diagnosis. In the FAS, the proportion of patients who underwent examinations and tests for items corresponding to overall COPD characteristics were as follows: smoking history or exposure to air pollution was recorded in 99.9% (707/708), 77.3% (547/708) underwent chest computed tomography (CT) imaging to detect emphysematous changes, and 46.9% (332/708) underwent pulmonary diffusing capacity tests. The proportion of patients who underwent examinations and tests for items corresponding to characteristics of asthma was high for examinations related to conditions such as perennial allergic rhinitis at 100% (708/708), history of asthma before age 40 years at 97.2% (688/708), and variable or paroxysmal respiratory symptoms at 94.5% (669/708). The proportions of patients who underwent laboratory and respiratory function tests were as follows: peripheral blood eosinophil count, 79.8% (565/708); fractional exhaled nitric oxide (FeNO), 63.7% (451/708); airway reversibility, 46.8% (331/708); and total immunoglobulin (Ig) E or specific IgE, 33.3% (236/708).

Proportions of patients who underwent evaluation for each ACO diagnostic criterion among overall patients (full analysis set, N = 708), patients with data necessary for ACO diagnosis (n = 396), and patients lacking the data necessary for ACO diagnosis (n = 312). ACO asthma–COPD overlap, COPD chronic obstructive pulmonary disease, CT computed tomography, FeNO fractional exhaled nitric oxide, Ig immunoglobulin, LAA low attenuation areas
When comparing the proportions of patients who underwent testing for COPD items among the 396 patients with the data necessary for ACO diagnosis and the 312 patients lacking the data necessary for ACO diagnosis, there was little difference in the proportions of patients examined in these groups. In terms of asthma characteristics, there were no differences in the implementation of examinations for variable or paroxysmal respiratory symptoms and history of asthma before the age of 40 years. However, there were numerical differences in the proportions of patients who underwent examinations/tests for FeNO (89.6% vs 30.8%), total IgE or specific IgE (48.5% vs 14.1%), airway reversibility (60.4% vs 29.5%), and peripheral blood eosinophil count (93.4% vs 62.5%).
Proportions of Patients Who Met the JRS ACO Diagnostic Criteria, Among Patients with COPD, with/without the Physician’s Diagnosis of Asthma Complications
Among the patients who had the data necessary for ACO diagnosis (n = 396), 177 had asthma complications according to the physician’s diagnosis and 38.4% (68/177) of these patients met the ACO criteria. Despite having asthma complications, 61.6% (109/177) were not considered to meet the ACO criteria. In contrast, of 219 patients without asthma complications according to the physician’s diagnosis, 15.1% (33/219) met the ACO criteria (Table 1).
ICS Use in ACO and Non-ACO Patients
Table 2 shows the patterns of ICS use among patients who had the data necessary for ACO diagnosis (n = 396), who met and did not meet the ACO criteria. Among the patients who met the ACO criteria, 74.3% (75/101) received ICS, and 25.7% (26/101) did not receive ICS treatment. In contrast, among patients who did not meet the ACO criteria, 35.6% (105/295) were receiving ICS, and 64.4% (190/295) were not receiving ICS treatment.
Asthma complications based on physician’s diagnosis, biomarkers, patient-reported outcomes, and exacerbations by ICS use in ACO and non-ACO patients are summarized in Table 3. The proportions of patients who had asthma based on a physician’s diagnosis and received ICS were 81.3% (61/75) in the ACO group and 57.1% (60/105) in the non-ACO group (p < 0.001 each). For ACO patients, the mean (SD) FeNO values were 49.4 (39.3) ppb in the ICS-use group and 43.8 (23.4) ppb in the no ICS-use group (p = 0.420). In the ACO group, patients using ICS had higher mean peripheral blood eosinophil count (p = 0.003), mean peripheral blood eosinophil ratio (p = 0.005), and IgE level (total IgE or IgE specific to perennial inhalant antigens) (p = 0.034), and more frequent variable and paroxysmal symptoms (p = 0.041 and p = 0.039) than those not using ICS. In the non-ACO group, a higher proportion of ICS users had positive IgE specific to perennial inhalant antigens than patients not using ICS (p = 0.047), and greater proportions of ICS users had variable symptoms (p = 0.020) and higher COPD Assessment Test (CAT) (p = 0.023) and Asthma Control Questionnaire (ACQ) (p < 0.001) scores than those not using ICS. In both the ACO and non-ACO groups, a higher proportion of patients using ICS had at least one exacerbation in the past year (22.7% and 12.4%, respectively) compared with those not using ICS (11.5% and 9.5%).
Other demographic characteristics by ICS use are described in Table S3 in the supplementary material. In the non-ACO group, a higher proportion of patients in the ICS group had complications/comorbidities compared with the non-ICS patients (88.6% vs 72.1%; p = 0.001). Allergic rhinitis was more frequent among non-ACO patients using ICS than those not using ICS (11.4% vs 4.2%; p = 0.018).
Discussion
The present analysis is based on data collected from the first large-scale ACO Registry study in Japan, which included 708 patients with COPD under the care of respiratory specialists from 27 facilities. The purpose was to clarify the actual implementation status of examinations and tests required for diagnosing ACO by respiratory specialists on the basis of the ACO diagnostic criteria proposed by the JRS [8] and the status of ICS prescription for patients diagnosed with ACO or non-ACO based on the ACO diagnostic criteria.
We consider that the strengths of the present study were that data were obtained from multiple centers across Japan and that patients were assessed by respiratory specialists. In contrast, other studies evaluating the proportions of patients in whom examinations and tests were implemented according to the ACO diagnostic criteria were mainly single-center studies. These studies, however, reported higher proportions of patients with the data necessary for ACO diagnosis than the proportions observed in the present study [13,14,15]. A single-center study retrospectively confirmed that the proportion of patients with the data necessary for ACO diagnosis was 66.9% (111/166 patients), including 23 patients who had test results for all ACO diagnostic items [13]. In that study, the proportion of patients for whom each examination/test was implemented was relatively high for airway reversibility (100%), peripheral blood eosinophils (97.0%), FeNO (94.0%), a history of asthma before the age of 40 years (88.6%), and variable or paroxysmal symptoms (86.7%). In another single-center study, 89.4% (76/85 patients) had the data necessary for ACO diagnosis [14]. Given the features of the present large-scale multicenter observational study, the present results might reflect the actual status of testing and treatment in Japan more accurately than previous studies.
The proportions of patients undergoing examinations that included the presence or absence of variable or paroxysmal respiratory symptoms, history of asthma before the age of 40 years, and the presence or absence of allergic rhinitis were high. Conversely, the proportions of patients undergoing objective indicator tests were lower than expected despite the requirement for study sites to have the specialists and resources available to conduct the necessary tests. The implementation of objective examinations, in addition to subjective assessments, is recommended by the JRS ACO Guidelines [3, 8, 16]. As FeNO quantification is non-invasive and simple, its use as a diagnostic tool should become more widespread. A recent Japanese study concluded that, for ICS-naïve patients, FeNO of at least 25.0 ppb and blood eosinophil count of at least 250 cells/μL had a 96.1% specificity in differentiating ACO from COPD [17]. The proportion of patients tested for peripheral blood eosinophil count was relatively high at 79.8%, but testing for IgE was comparatively low. The acquisition of data necessary for ACO diagnosis can be increased without changing the degree of invasiveness to patients by adding tests for total IgE levels and specific IgE levels for perennial inhalant antigens at the time of blood collection. A recent publication reported that specific IgE positivity for Dermatophagoides pteronyssinus and house dust was significantly higher in patients meeting the criteria for ACO than in those who did not meet the ACO criteria [14]. The proportion of patients undergoing physiological function tests was lower than that of blood sampling and imaging tests. If the time required for airway reversibility tests and the burden on the patient are considered, it may be difficult to improve the proportions of patients tested. Conversely, the pulmonary diffusing capacity test has a short testing time, is cheaper than CT, and places a relatively minor burden on the patient. Therefore, it is desirable to implement this test actively.
An important finding of this study was that 38.4% of the patients diagnosed as having comorbid asthma by physicians had ACO according to the JRS ACO diagnostic criteria and 61.6% did not; for those diagnosed with no comorbid asthma by physicians, 15.1% had ACO according to the JRS criteria, and 84.9% did not. The presence or absence of comorbid asthma according to physicians and that based on objective ACO diagnostic criteria were inconsistent, suggesting that the physician’s diagnosis of comorbid asthma may not be adequate. Possible explanations for this finding may be that the physician’s diagnosis was not based on clear criteria and that diagnosing asthma in patients with COPD is difficult. This finding further emphasizes the need to carefully establish the ACO diagnosis based on the JRS diagnostic criteria. In the analysis of Japanese patients (n = 416) in the KRONOS clinical trial, which was conducted in a COPD population that excluded patients diagnosed with comorbid asthma by physicians, it was reported that 13.2% (55/416) of patients had an eosinophil count of at least 300 cells/μL, which is one of the characteristics of asthma [18]. These results indicate that objective indicators may help discern whether some patients with COPD considered not to have comorbid asthma by a physician may actually be misdiagnosed. Thus, the tests described by the ACO diagnostic criteria should be conducted to confirm the presence or absence of comorbid asthma, regardless of the physician’s diagnosis.
Another aim of the current study was to investigate whether ACO and non-ACO patients in real clinical practice were treated in accordance with the recommendations of treatment guidelines [6, 8]. We found that 74.3% of patients who met the JRS ACO diagnostic criteria used ICS, and 25.7% did not. ACO patients who used ICS had higher proportions of comorbid asthma according to a physician’s diagnosis, variable or paroxysmal respiratory symptoms, higher peripheral blood eosinophil count/percentage, and higher IgE levels, compared with those who did not use ICS, suggesting these factors facilitate the prescription of ICS in ACO patients. However, patients who met these factors did not necessarily use ICS. Of ACO patients who did not use ICS, 44.0% had a peripheral blood eosinophil count/percentage greater than 5% or more than 300 cells/μL, 72.2% had high IgE levels, and 50.0% had variable symptoms. Even in ACO patients who were also diagnosed with comorbid asthma by a physician, 26.9% did not use ICS. The presence or absence of ACO should be accurately detected using the diagnostic criteria, and appropriate treatment, including ICS, should be prescribed for patients diagnosed with ACO per the current guidelines [8].
Conversely, among patients who did not meet the ACO diagnostic criteria, 64.4% were not using ICS and 35.6% used ICS. The proportion of non-ACO patients using ICS in Japan was lower than that reported in studies conducted overseas, such as KRONOS, ETHOS, and IMPACT [18,19,20,21]. Non-ACO patients who used ICS had higher proportions of comorbid asthma based on a physician’s diagnosis, variable symptoms, and higher CAT scores and ACQ scores than those who did not use ICS, suggesting these factors may also affect the usage of ICS. There were no differences in the frequency of exacerbations, FeNO values, or peripheral blood eosinophil count/percentage with or without ICS use in this group, implying that physicians may not attach greater importance to exacerbation occurrence or biomarker levels when considering whether to prescribe ICS. The Global Initiative for Chronic Obstructive Lung Disease 2021 guideline recommends the addition of ICS to a long-acting beta-agonist for patients with moderate to severe exacerbations [5]. This approach may be particularly effective in patients with peripheral blood eosinophil counts of more than 300 cells/µL [5]. In the present study, some non-ACO, ICS-untreated patients had a peripheral blood eosinophil count/percentage greater than 5% or more than 300 cells/μL or exacerbations; these patients may require ICS therapy.
This study had several limitations. Enrollment was limited to patients from sites where tests used for ACO diagnosis were conducted in routine clinical practice, and specialists treated the registered patients in a relatively well-equipped environment. This may have affected patient demographics and clinical outcomes, limiting the application of this study’s results to patient populations in other medical facilities, including those that cannot perform the required tests. As this study was restricted to outpatients who could visit the study sites regularly, the results of this study cannot be directly extrapolated to patients who make irregular visits in primary care or inpatients. The proportion of patients who underwent examinations/tests was evaluated only within 1 year prior to registration. Finally, the study included both treatment-naïve patients and those who had drug treatment. Thus, there may have been patients with ACO who did not meet the ACO diagnostic criteria as a result of prior clinical intervention.
Conclusions
This multicenter study conducted at 27 study sites across Japan revealed the proportions of patients who underwent examinations/tests by respiratory specialists for each item of the ACO diagnostic criteria advocated by the JRS. Overall, the proportion of objective laboratory and physiological tests was lower than expected despite the specification for sites with the specialists and resources available to conduct the necessary tests. The presence or absence of comorbid asthma based on the ACO diagnostic criteria and the presence or absence of comorbid asthma based on the physician’s diagnosis did not always match. In order to properly diagnose comorbid asthma in patients with COPD, it is sensible to actively implement not only examinations but also objective tests that serve as indicators of ACO diagnostic criteria. The present findings clearly show that most patients with ACO were being treated with ICS as recommended in the JRS treatment guidelines. Attempts should be made to further increase the proper use of ICS among these patients in Japan.
Change history
11 August 2022
A Correction to this paper has been published: https://doi.org/10.1007/s12325-022-02287-y
References
World Health Organization. Chronic obstructive pulmonary disease (COPD). Key Facts. June 2021. https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd). Accessed Oct 1, 2021.
Quaderi SA, Hurst JR. The unmet global burden of COPD. Glob Health Epidemiol Genom. 2018;3:e4.
Yanagisawa S, Ichinose M. Definition and diagnosis of asthma–COPD overlap (ACO). Allergol Int. 2018;67:172–8.
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. Updated 2021. https://ginasthma.org/. Accessed Oct 1, 2021.
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Reported 2021. http://goldcopd.org. Accessed Oct 1, 2021.
The Japanese Respiratory Society. Guidelines for diagnosis and treatment of COPD (chronic obstructive pulmonary disease). 5th ed. Tokyo: Medical Review; 2018.
Milewska A, Rysiak E, Zareba I, Holownia A, Mroz RM. Costs of treatment of chronic obstructive pulmonary disease. Adv Exp Med Biol. 2016;885:67–75.
The Japanese Respiratory Society. The JRS guidelines for the management of ACO 2018. Tokyo: Medical Review; 2017.
Hashimoto S, Sorimachi R, Jinnai T, Ichinose M. Asthma and chronic obstructive pulmonary disease overlap according to the Japanese Respiratory Society diagnostic criteria: the prospective, observational ACO Japan cohort study. Adv Ther. 2021;38:1168–84.
Cosio BG, Soriano JB, López-Campos JL, et al. Defining the asthma–COPD overlap syndrome in a COPD cohort. Chest. 2016;149:45–52.
Tamada T, Sugiura H, Takahashi T, et al. Biomarker based detection of asthma–COPD overlap syndrome in COPD populations. Int J Chron Obstruct Pulmon Dis. 2015;10:2169–76.
Nishimura M, Makita H, Nagai K, et al. Annual change in pulmonary function and clinical phenotype in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;185:44–52.
Yamamura K, Hara J, Kobayashi T, et al. The prevalence and clinical features of asthma–COPD overlap (ACO) definitively diagnosed according to the Japanese Respiratory Society Guidelines for the Management of ACO 2018. J Med Invest. 2019;66:157–64.
Toyota H, Sugimoto N, Kobayashi K, et al. Comprehensive analysis of allergen-specific IgE in COPD: mite-specific IgE specifically related to the diagnosis of asthma–COPD overlap. Allergy Asthma Clin Immunol. 2021;17:13.
Kyogoku Y, Sugiura H, Ichikawa T, et al. Nitrosative stress in patients with asthma–chronic obstructive pulmonary disease overlap. J Allergy Clin Immunol. 2019;144:972–83.e14.
Mekov E, Nuñez A, Sin DD, et al. Update on asthma–COPD overlap (ACO): a narrative review. Int J Chron Obstruct Pulmon Dis. 2021;16:1783–99.
Takayama Y, Ohnishi H, Ogasawara F, Oyama K, Kubota T, Yokoyama A. Clinical utility of fractional exhaled nitric oxide and blood eosinophils counts in the diagnosis of asthma–COPD overlap. Int J Chron Obstruct Pulmon Dis. 2018;13:2525–32.
Ichinose M, Fukushima Y, Inoue Y, et al. Efficacy and safety of budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler formulated using co-suspension delivery technology in Japanese patients with COPD: a subgroup analysis of the KRONOS Study. Int J Chron Obstruct Pulmon Dis. 2019;14:2979–91.
Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, phase 3 randomised controlled trial. Lancet Respir Med. 2018;6:747–58.
Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48.
Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378:1671–80.
Acknowledgements
Funding
This research was funded by AstraZeneca K.K., Osaka, Japan, including the journal’s Rapid Services and Open Access fees, in accordance with Good Publication Practice guidelines.
Medical Writing, Editorial, and Other Assistance
The authors wish to thank Keyra Martinez Dunn, MD, of Edanz, Japan, for providing medical writing support, which was funded by AstraZeneca K.K., Japan, through EMC K.K., Japan, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Conceptualization: Shu Hashimoto, Ryoko Sorimachi, Naoki Tashiro, Masakazu Ichinose. Methodology: Shu Hashimoto, Ryoko Sorimachi, Naoki Tashiro, Satoko Sugaya, Masakazu Ichinose. Project administration: Satoko Sugaya. Software: Yoshifumi Arita. Supervision: Satoko Sugaya. Visualization: Shu Hashimoto, Ryoko Sorimachi, Naoyuki Makita, Yoshifumi Arita, Masakazu Ichinose. Writing – original draft: Shu Hashimoto, Ryoko Sorimachi, Naoyuki Makita, Masakazu Ichinose. Writing – review and editing: all authors.
Disclosures
Ryoko Sorimachi, Naoyuki Makita, Naoki Tashiro, Satoko Sugaya, and Yoshifumi Arita are employees of AstraZeneca K.K. Shu Hashimoto and Masakazu Ichinose have nothing to disclose.
Compliance with Ethics Guidelines
This study was conducted following the Declaration of Helsinki and all applicable national and international ethical guidelines for medical and health research involving human participants. The Ethics Committee of Tohoku University Hospital (approval reference 2018-2-147-1) approved all study documentation. All participants gave informed consent before registration. Medical data were collected and stored in compliance with the relevant laws/regulations concerning data protection and the Personal Information Protection Act. This study was registered with ClinicalTrials.gov (identifier NCT03577795).
Data Availability
Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Author information
Authors and Affiliations
Corresponding authors
Additional information
The original online version of this article was revised due to update in caption of Table 2.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hashimoto, S., Sorimachi, R., Makita, N. et al. Real-World Status of Medical Care and Treatment of Chronic Obstructive Pulmonary Disease by Respiratory Specialists in Japan. Adv Ther 39, 4509–4521 (2022). https://doi.org/10.1007/s12325-022-02167-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-022-02167-5