
Abstract
Purpose of Review
We present the risk factors, clinical presentation, and current recommendations for diagnosing and treating cutaneous infections due to Geotrichum spp.
Recent Findings
Skin infections caused by Geotrichum spp. are infrequent. G. candidum and G. klebahnii are the only species of the genus responsible for human infections. In immunocompetent patients, these infections occur due to severe trauma or burns, while in immunosuppressed patients, they are mainly a consequence of dissemination.
Summary
Geotrichum spp. infection is challenging to discriminate with colonization because it is a ubiquitous skin colonizer, in such a way that clinical suspicion is essential to achieve the diagnosis. There are no breakpoints or epidemiological cut-off values to interpret antifungal susceptibility tests. Amphotericin B and voriconazole have been the most widely used antifungals in treatment. Active surveillance studies are required to understand these infections’ characteristics and real burden.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The recent increase in the number of immunosuppressed patients has increased the number of systemic fungal infections, but also cutaneous. The skin is the first line of defense against pathogens; however, in recent years, the number of skin infections caused by pathogenic or opportunistic fungi has been increasing in both immunosuppressed and immunocompetent patients. Skin lesions can result from a local infection, but they can also be a manifestation of a disseminated infection. The primary pathogens involved include yeasts such as Candida or Malassezia furfur or dermatophytes such as Trichophyton, Microsporum, and Epidermophyton, but Aspergillus spp., Fusarium spp., Mucorales, Talaromyces marneffei, Sporothrix spp., and dematiaceous fungi [1]. Another organism responsible for skin infections, although rare, is Geotrichum, an imperfect, filamentous, yeast-like fungus that belongs to the phylum Ascomycota, order Saccharomycetales.
Previously, the species of the genus Geotrichum were singled out to it, based on their morphological characteristics, in such a way that the species most frequently isolated from clinical samples were commonly named Geotrichum candidum (with its teleomorph Galactomyces candidus and its anamorph Geotrichum candidum), Geotrichum capitatum (with its teleomorph Magnusiomyces capitatus and its anamorph Saprochaete capitata), and Geotrichum clavatum (of which its teleomorph is unknown and its anamorph Saprochaete clavata). However, in recent years, this genus, after several phylogenetic analyses based on rDNA and multilocus analyses, underwent a series of changes, placing Saprochaete clavata in the genus Magnusiomyces (Magnusiomyces clavatus), leaving Geotrichum candidum as the only genus pathogenic species of the genus Geotrichum [2, 3]. However, the case of an invasive skin infection by Geotrichum klebahnii in a patient with no known chronic conditions was recently described [4•].
Geotrichum candidum is a ubiquitous, saprophytic fungus found in soil, fruits, dairy products, and vegetables; it is also a commensal that colonizes the skin, digestive, and respiratory tracts of humans [5, 6]; however, it is also an emerging opportunistic pathogen that although rare (less than 100 cases between 1842 and 2006) has high mortality rates, being higher than 60% in cancer patients but less than 40% in other groups of patients [7, 8•, 9].
Risk Factors and Specter of Geotrichum spp. Infections
No specific risk factors have been described for Geotrichum candidum infections, and some case reports have been in immunocompetent people, although diabetes [4•, 5, 10•] and COVID-19 have been associated [11].
According to the reports, the spectrum of disease ranges from skin disease, oral cavity, otomycosis, symptomatic and asymptomatic urinary tract infection, post-surgical and post-trauma infection, and osteoarticular to pulmonary disease, endocarditis, and disseminated infection [11,12,13,14,15,16,17,18,19,20]. However, one case series reports that immunosuppression, such as hematological malignancies and the use of immunosuppressors, is associated with cases of invasive infection at the pulmonary level and even fungemia [9, 21•]. Unlike Magnusiomyces clavatum, there are no reports of outbreaks caused by G. candidum.
Epidemiology of Geotrichosis
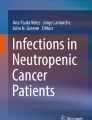
Regarding geographic distribution, we found only a few case reports with a worldwide distribution; countries with more case reports include the USA, with nine reports, followed by Germany and India, shown in Fig. 1A countries with case reports. Interestingly, more recent cases have been observed, which could mean that geotrichosis is an emerging infection.

A Worldwide distribution of case reports or geotrichosis. B Colony morphology of Geotrichum candidum on Sabouraud agar medium at 30 °C for 48 h, culture shows chalk-white, dry, star-shaped colonies with a raised surface and a chamois leatherlike appearance. C Massive growth of Geotrichum candidum on Sabouraud agar medium at 30 °C for 96 h, white, velvety, and moist colonies are observed. D Preparation with lactophenol cotton blue with a magnification of 400×, where septate hyaline hyphae are observed, segmented into chains of rectangular arthroconidia of very variable size of Geotrichum candidum
Cutaneous Geotrichosis
Geotrichum disease is an unusual mycosis. There are few reports of infection by this organism; however, pulmonary and disseminated diseases in immunocompromised hosts, such as leukemia and cancer, are the most common among these. Cutaneous geotrichosis is infrequent and can occur in animals [22, 23] and humans. In the latter, the reported cases are from various countries, including the USA [21•, 24•, 25•], Korea [26•], Greece [10•], Indonesia [27•], and Mexico [28•], and report affection in adults of various ages (20 years until 80 years) as mentioned below.
Cutaneous Geotrichosis Risk Factors
Cutaneous geotrichosis (CG) was described in immunocompetent hosts and was associated with diabetes [4•, 10•], history of local trauma [10•, 26•, 29], and burns [24•, 25•]. CG has also been described in immunosuppressed patients as acute leukemia patients [21•, 30, 31] and solid organ neoplasias (as squamous cell carcinoma) [27•], although associated with disseminated infection in most. In burn and immunosuppressed hosts, the clinical presentation can be severe with disseminated infection; this last group usually has a fatal outcome due to their immune status [21•, 30, 31].
Clinical Presentation of Cutaneous Geotrichosis
It can cause a superficial and deep tissue disease. The superficial cutaneous presentation was described in a patient with diabetes in breast folds, presenting as erythematous scaly plaques with satellite and pruritic lesions. Therefore, the first suspicion was candidiasis [28•]. Another case is a healthy woman who suffered a rock injury to her shin; the lesion presented as mildly itchy, painless, scaly, and secretive. This patient received steroids three times before G. candidum was detected [26•]. In summary, superficial lesions can present with lesions with erythema pruritus; there may or may not be scales, similar to mucocutaneous candida.
Cutaneous deep geotrichosis was described; lesions are described in the finger [10•], hands [29], arms [30], feet [27•], and face [4•, 28•], as well as in the insertion catheter site, which indicates no preference for any particular area. Skin lesions can range from 3 to 12-cm long by 3 to 4-cm wide, are generally characterized by slow growth, with 3–7 months evolution, and may present painlessly or moderately painful and erythema; swelling, edema, mild itching, and nodular and granulomatous lesions may be present. Ulcerative lesions and obstructive arterial disease have also occurred [4•, 10•, 21•, 27•, 29, 30]. In a facial case for G. klebahnii in a patient with no history of trauma and with diabetes mellitus, orbital involvement was found with mild ocular proptosis and visual alteration due to inflammation [4•].
Clinical differential diagnosis must be made with inflammatory and neoplastic cutaneous diseases, other infections such as conventional bacteria or nontuberculous mycobacterial skin diseases, etc. Microbiologically, there are reported cases of coinfection with other fungi such as Rhizopus spp., Fusarium spp. [25•], dematiaceous fungus (Microsphaeropsis arundinis) [27•], and C. orthopsilosis [24•].
Diagnosis
Cutaneous infections tend to be challenging to define an etiologic diagnosis since, as mentioned above, G. candidum is commonly found colonizing the skin and is a ubiquitous fungus; therefore, histopathology demonstration would be required to establish the definitive diagnosis. It is worth mentioning that there are few reports in which tissue invasion has been demonstrated by histopathology [4•, 10•, 21•, 26•, 30]. It is essential to highlight that the mucosal affection of Geotrichum is practically indistinguishable from mucocutaneous candidiasis due to its clinical features. The lack of response to treatment may lead to seeking a diagnosis.
Histopathology
Evidence by pathology is usually a requirement for the proven diagnosis of invasive fungal infections, as the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium (EORTC/MSGERC) indicates [32]. In Grocott-Gomori methenamine silver (GMS) or periodic acid-Schiff (PAS) stains, Geotrichum spp. observed as septate hyphae (arthroconidia) with variable diameter and length without blastospores; rectangular, oval forms observed, and branching is infrequent [4•, 21•, 30]. It is possible to find mixed inflammatory infiltration with lymphocytes, neutrophils, monocytes, and a few eosinophils, as well as a granuloma with the formation of a central neutrophilic microabscess [4•, 10•].
Molecular Diagnosis Tests
To establish proven invasive fungal infection, the EORTC/MSGERC proposes amplifying fungal DNA by PCR combined with DNA sequencing when fungal structures are observed in tissue [32]. Unfortunately, since no reports and guidelines have been used for the molecular detection of Geotrichum spp. and no standardized test, this method is only moderately supported for the detection of G. candidum [8].
Utility of Fungal Biomarkers
Currently, the use of biomarkers for diagnosing Geotrichum spp. infections has not been established because there are very few reports in which galactomannan and 1,3-β-D-glucan detection has been used. Galactomannan detection was negative in one patient with invasive skin infection by G. klebahnii and another with G. candidum, while 1,3-β-D-glucan was positive in the latter case [4•, 33]. The European Society for Clinical Microbiology and Infectious Diseases (ESCMID) and the European Confederation of Medical Mycology (ECMM) joint clinical guidelines for diagnosing and managing rare invasive yeast infections do not recommend its use [34].
Conventional Mycology Tests
Fungal Stain
The KOH and Gram stains from skin samples can provide a rapid and presumptive diagnosis of G. candidum presence, so their use is strongly recommended. However, culture remains essential for diagnosis [8•].
Fungal Culture
Identification at the species level is strongly recommended to understand geotrichosis’s epidemiology and clinical characteristics. In contrast, there is currently no data indicating that identification of Geotrichum to the species level can guide the choice of antifungal treatment; the recommendation for identification at this level, for this purpose, is only moderate [8•].
Historically, the identification of fungi has been based on macroscopic and microscopic characteristics. G. candidum commonly grows on Sabouraud dextrose agar (SDA) after 48 h at 25 °C, while at 36 °C, growth is slower and may take more than 4 days [10•]. Geotrichum spp. grows on SDA as cream-colored, moist, yeast-like, and hairy colonies [16, 35]; in contrast, it grows as a chalky white stellate colony on blood agar with a chamois-like surface and sinks in the agar [17]. Figure 1B shows the colony growth of G. candidum in SDA media at 30 °C for 48 h. Figure 1C shows massive growth of G. candidum in SDA media at 30 °C for 96 h. Microscopically, with lactophenol blue staining, it appears as hyaline septate hyphae segmented into chains of rectangular arthroconidia of quite variable size without producing blastoconidia [4•, 16, 24•, 35]. Figure 1D shows a lactophenol cotton blue preparation from Geotrichum candidum at 400× magnification. Biochemically, it assimilates glucose, galactose, and xylose but not lactose, maltose, and sucrose [24]. The detection of the lack of urease activity has been used for its identification and differentiation mainly from Trichosporon [16, 17, 24•].
Phenotypic identification systems that have been used for the identification of Geotrichum spp. include API 20C (bioMérieux, Marcy l’Etoile, France), VITEK 2 (bioMérieux, Marcy-l’Etoile, France), API ID 32C (bioMérieux, France) and MicroScan (Beckman Coulter), some of which have shown limitations in achieving identification to the species level [4•, 16, 36, 37]. The recent introduction of matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) has come to revolutionize the identification of bacteria and fungi in clinical microbiology laboratories; unfortunately, the cases of infection by Geotrichum spp., in which MALDI-TOF MS has been used for identification, are scarce [4•, 24•] and the few MALDI-TOF MS performance evaluations for identification of this genus include only a few samples [37,38,39,40,41]. It is well described that the number of species and spectra contained in the library used directly influence the identification performance of MALDI-TOF MS. Currently, the MALDI-TOF Biotyper (Bruker Daltonics Bremen, Germany) Filamentous Fungi Library v5.0 includes only 12 spectra of G. candidum and one of Geotrichum sp., which shows the need to enrich the libraries with more species, even non-pathogenic ones, to improve this tool’s performance in identifying Geotrichum species. Regarding the method to achieve identification, using MALDI-TOF is moderately recommended, considering that its performance will depend on the library’s richness [8•].
On the other hand, the gold standard for identification is rDNA molecular analysis; however, most routine laboratories cannot perform it, being limited to only a few research laboratories. There are less than a handful of clinical cases in which molecular sequencing has been used to identify G. candidum [19, 20, 21•]. Molecular identification by ITS or 28S ribosomal DNA sequencing is strongly recommended instead of identification based on morphological characteristics or biochemical behavior [8•].
Antifungal Susceptibility Tests
There are no breakpoints or epidemiological cut-off values (ECV) for interpreting the different antifungals’ minimum inhibitory concentrations (MICs) against G. candidum. There are few studies and few isolates in which susceptibility has been analyzed. The reported MICs are diverse across the different studies (Table 1) [4•, 10•, 11, 14, 20, 21•, 42,43,44,45,46,47,48,49].
Determining susceptibility to antifungals is moderately recommended to guide antifungal treatment; it can be clinically helpful in treatment failure or refractory disease cases. However, the recommendation is strong from the epidemiological data support, and the determination must be made using standardized reference methods [8•].
Treatment Recommendations
Antifungals. The optimal treatment has yet to be established. Data are limited to in vitro data, case reports, and case series. A high index of clinical suspicion is necessary to start antifungal therapy.
The choice of treatment will depend on the severity of the infection. The literature supports the treatment with amphotericin B liposomal plus or not flucytosine in severe or invasive cases, and there is scarce data on voriconazole. Neither echinocandins nor fluconazole can be recommended because of high MICs and no clinical support for efficacy [4•, 21•, 44, 46].
Treatment duration is empirical and should be individualized, guided by clinical response, site and extent of infection, and patient immune status [8•]. The treatment recommended by the authors is from 2 to 12 weeks in invasive infections and with difficulty in controlling the focus of infection. The decision must be individualized and consulted with the expert.
Regarding experience in superficial cutaneous geotrichosis, Bonifaz et al. [28] reported improvement in a patient who self-medicated with topical 1% gentian violet for 20 days; in another case described by Choi et al. [26], the patient was given treatment with 200 mg of itraconazole plus topical 1% isoconazole nitrate for 6 weeks, with recovery and leaving post-inflammatory hyperpigmentation.
Oral geotrichosis treatment is anecdotic; reports described a treatment with topical nystatin vaginal tablets for several weeks; no other data supported this recommendation [50]. Oral geotrichosis should be treated as an alternative therapy, such as posaconazole and isavuconazole, which are promising potential therapies, although not many studies support this information [46].
Surgical Treatment. For the treatment of skin or soft tissue infections, surgical debridement with infection-free margins is recommended, in addition to systemic antifungal therapy. Resection or debridement should be repeated as necessary [8•].
Summary of Geotrichosis Antifungal Treatment Options
Based on the review and the evidence found, the authors summarize the treatment recommendations according to the presentation of geotrichosis. We summarize all treatment recommendations in Table 2.
Invasive Cutaneous Geotrichosis or Systemic Disease
First-line therapy: amphotericin B liposomal formulation +/− flucytosine (Ampho B Lipid complex as 5 mg/kg/day as single infusion or Ampho B Liposomal 3–5 mg/kg/day as single infusion).
The first-line alternative: voriconazole, posaconazole, or isavuconazole (intravenous dosing (IV)/oral formula.
The authors recommend seeing numerous drug interactions with these drug classes regarding azole drugs. Voriconazole IV dosing 6 mg/kg IV 12 × 2 doses (load) and then 3–4 mg/kg IV q12h. Oral dosing of voriconazole 400 mg OR q12h × 2 doses and then 200 mg OR q12h should be an oral dose 1 h before or 1 h after eating.
Superficial Cutaneous Geotrichosis
Topical first-line therapy: ketoconazole or miconazole in topical formulation.
Systemic first-line therapy: voriconazole, posaconazole, or isavuconazole (IV/OR).
G. candidum Industrial Relevance
However, from a clinical point of view, there is an increase in the number of cutaneous and disseminated infection cases by Geotrichum in several regions worldwide. Nevertheless, we must recognize the advantages of its widespread use in the food and beverage industry and many other industrial uses.
A recent review revealed the importance of G. candidum for the food, biotechnology, and agro-industry, pointing out its role as a starter culture in the dairy and brewing industry, its importance as a probiotic nutritional supplement in fish, its role in the production of a large number of biotechnologically necessary enzymes, in addition to pointing out the existence of strains that produce secondary metabolites with antimicrobial activity. Likewise, G. candidum has bioremediation capacity by removing or reducing contaminants and heavy metals from the aquatic environment and degrading various types of organic waste from wastewater [51]. Another recent study showed the potential of G. candidum arthrospore cell wall particles for curcumin encapsulation, proposing it as a new natural encapsulation carrier with potential superiority for practice in the food industry [52].
Sources of Exposure
Sources of exposure to G. candidum are ingestion, inhalation, and contact. The existence of workers exposed to large amounts of G. candidum spores (for example, cheese makers) has been described; however, no occupational disease related to G. candidum has been reported. It has also been described that cheese consumption is an essential source of exposure; however, G. candidum circulates through the digestive tract until it is eliminated in the feces without achieving colonization [7].
The recent review by Pottier et al., in which the dangers and risks of developing an infection by G. candidum concerning its technological use and the consumption of dairy products were evaluated, found that G. candidum has never been reported as a pathogen potentially transmitted by food, nor as a producer of mycotoxins in them, and concluded that the risk is practically nil; therefore, they suggested proposing G. candidum for the status of “Qualified Presumption of Safety” (QPS).
However, more studies are required to establish the potential risk of Geotrichum candidum-based food consumption or use by people with a compromised immune system since the pathogenic role of this organism in these patients has been demonstrated.
Conclusions
Geotrichum species have low virulence; however, they can cause disseminated disease with high mortality, so it is crucial to keep them in mind in the diagnosis when a disseminated fungal infection is suspected in immunocompromised patients. In immunocompetent patients, the diagnosis is even more challenging in skin manifestations because it is a ubiquitous organism commonly found colonizing the skin; the call is to keep them in mind and not rule out their possible pathogenic role. There are no clinical or epidemiological cut-off points. Among the azoles, voriconazole is the one that has shown the lowest MICs; the most widely used antifungals in the treatment of invasive and disseminated skin infections are amphotericin B and voriconazole. Active surveillance studies are required to allow us to detect all cases of skin infection by this organism and thus better understand its clinical behavior and epidemiology, improve the diagnostic approach, and know the susceptibility data to establish cut-off points that allow the choice of the appropriate treatment and thus favor the outcome of the patients. Given its low frequency, it is also associated with less suspicion, and thus, it could be an underestimated disease.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Gunaydin SD, Arikan-Akdagli S, Akova M. Fungal infections of the skin and soft tissue. Curr Opin Infect Dis. 2020;33:130–6. https://doi.org/10.1097/QCO.0000000000000630.
Hoog S, Smith M. Ribosomal gene phylogeny and species delimitation in Geotrichum and its teleomorphs. Stud Mycol. 2004;50:489–515.
Kaplan E, Al-Hatmi AMS, Ilkit M, Gerrits van den Ende AHG, Hagen F, Meis JF, et al. Molecular diagnostics of arthroconidial yeasts, frequent pulmonary opportunists. J Clin Microbiol. 2017;56:e01427–17. https://doi.org/10.1128/JCM.01427-17.
Tshisevhe V, Mitton B, Skosana L. Invasive Geotrichum klebahnii fungal infection: a case report. Access Microbiol. 2021;3:000287. https://doi.org/10.1099/acmi.0.000287. This recent paper described an invasive cutaneous Geotrichum infection by unusual species in a non-immunosuppressed host and showed histopathologic and microbiologic diagnosis and antifungal susceptibility tests.
Bonifaz A, Vázquez GD, Macías B, Paredes FF, Hernández MA, Araiza J, et al. Oral geotrichosis: report of 12 cases. J Oral Sci. 2010;52:477–83. https://doi.org/10.2334/josnusd.52.477.
Edslev SM, Andersen PS, Agner T, Saunte DML, Ingham AC, Johannesen TB, et al. Identification of cutaneous fungi and mites in adult atopic dermatitis: analysis by targeted 18S rRNA amplicon sequencing. BMC Microbiol. 2021;21:72. https://doi.org/10.1186/s12866-021-02139-9.
Pottier I, Gente S, Vernoux JP, Guéguen M. Safety assessment of dairy microorganisms: Geotrichum candidum. Int J Food Microbiol. 2008;126:327–32. https://doi.org/10.1016/j.ijfoodmicro.2007.08.021.
Chen SC, Perfect J, Colombo AL, Cornely OA, Groll AH, Seidel D, et al. Global guideline for the diagnosis and management of rare yeast infections: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis. 2021;21:e375–86. https://doi.org/10.1016/S1473-3099(21)00203-6. Erratum in: Lancet Infect Dis 2021;21:e363. This is a scientific consensus with recommendations for diagnosing and managing infections due to Geotrichum spp., among other rare yeasts, by experts in medical mycology.
Rajme-López S, González-Lara MF, Martínez-Gamboa RA, Rangel-Cordero A, Ponce-de-León A. Geotrichum spp: an overlooked and fatal etiologic agent in immunocompromised patients. A case series from a referral center in Mexico. Med Mycol. 2022;60:myac022. https://doi.org/10.1093/mmy/myac022.
Sfakianakis A, Krasagakis K, Stefanidou M, Maraki S, Koutsopoulos A, Kofteridis D, et al. Invasive cutaneous infection with Geotrichum candidum: sequential treatment with amphotericin B and voriconazole. Med Mycol. 2007;45:81–4. https://doi.org/10.1080/13693780600939948. This case report describes an invasive skin infection after trauma in a patient with no known predisposing risk factors. Shows the histopathological findings and identification methods used in the laboratory and the success of the treatment.
Selvan K, Mutlu G. Geotrichum infection in an immunocompetent host with SARS-CoV-2 infection. Tuberk Toraks. 2021;69:421–4. https://doi.org/10.5578/tt.20219717.
Calado NB, de Sousa Júnior FC, Diniz MG, Fernandes AC, Cardoso FJ, Zaror LC, et al. A 7-year survey of superficial and cutaneous mycoses in a public hospital in Natal, Northeast Brazil. Braz J Microbiol. 2011;42(4):1296–9. https://doi.org/10.1590/S1517-83822011000400008.
Souza E, Almeida L, Guilhermetti E, Mota V, Rossi R, Svidzinski T. Frequency of onychomycoses caused by yeasts in Maringa, Parana, Brazil. An Bras Dermatol. 2007;82:151–6.
Myint T, Dykhuizen MJ, McDonald CH, Ribes JA. Post operative fungal endophthalmitis due to Geotrichum candidum. Med Mycol Case Rep. 2015;10:4–6. https://doi.org/10.1016/j.mmcr.2015.11.001.
Bojanović M, Stalević M, Arsić-Arsenijević V, Ignjatović A, Ranđelović M, Golubović M, et al. Etiology, predisposing factors, clinical features and diagnostic procedure of otomycosis: a literature review. J Fungi. 2023;9:662. https://doi.org/10.3390/jof9060662.
Bilman FB, Yetik M. Geotrichum candidum: a rare infection agent in urinary system: case report and review of the literature. J Clin Expe Investigations Case report. 2017;8:127–9. https://doi.org/10.5799/jcei.382434.
Kandi V, Vaish R, Gurrapu P, Koka SS, Bhoomigari MR. Geotrichosis presenting as funguria and asymptomatic urinary tract infection in a patient with renal cyst. Cureus. 2020;12:e7616. https://doi.org/10.7759/cureus.7616.
Hrdy DB, Nassar NN, Rinaldi MG. Traumatic joint infection due to Geotrichum candidum. Clin Infect Dis. 1995;20:468–9. https://doi.org/10.1093/clinids/20.2.468.
Garcia LT, Sanchez YM, Aznar OE, Ortiz MBA, Guillén BI. Seroma intraabdominal y linfopenia sin leucopenia en un paciente oncológico. Infección por Geotrichum candidum [Intra-abdominal seroma and lymphopenia without leucopenia in a cancer patient. Geotrichum candidum infection]. Rev Iberoam Micol. 2014;31:152–3. https://doi.org/10.1016/j.riam.2012.05.001.
Meena S, Singh G, Dabas Y, Rajshekhar P, Xess I. Geotrichum candidum in infective endocarditis. J Glob Infect. 2017;9:127–8. https://doi.org/10.4103/jgid.jgid_112_16.
Henrich TJ, Marty FM, Milner DA Jr, Thorner AR. Disseminated Geotrichum candidum infection in a patient with relapsed acute myelogenous leukemia following allogeneic stem cell transplantation and review of the literature. Transpl Infect Dis. 2009;11:458–62. https://doi.org/10.1111/j.1399-3062.2009.00418.x. This work reports the case of acute myeloid leukemia with disseminated fungal infection patient from catheter origin. It shows the lesions, histopathological findings, and susceptibility to antifungals.
Figueredo LA, Cafarchia C, Otranto D. Geotrichum candidum as etiological agent of horse dermatomycosis. Vet Microbiol. 2011;148:368–71. https://doi.org/10.1016/j.vetmic.2010.09.025.
Padalino B, Sandy JR, Barrasso R, Trotta A, Bozzo G, Cafarchia C. Rare generalized form of fungal dermatitis in a horse: case report. Animals (Basel). 2020;10:871. https://doi.org/10.3390/ani10050871.
Keene S, Sarao MS, PJ MD, Veltman J. Cutaneous geotrichosis due to Geotrichum candidum in a burn patient. Access Microbiol. 2019;1:e000001. https://doi.org/10.1099/acmi.0.000001. This recent report presents the case of a patient with a burns-related cutaneous invasive infection and successful treatment after several debridement and antifungal treatment.
Welch G, Sabour A, Patel K, Leuthner K, Saquib SF, Medina-Garcia L. Invasive cutaneous mucormycosis: a case report on a deadly complication of a severe burn. IDCases. 2022;30:e01613. https://doi.org/10.1016/j.idcr.2022.e01613. This work describes a case with an unusual presentation of co-infection by Rhizopus spp, Fusarium spp, and G. candidum in a patient with burns >45% of the body surface. It shows the difficulty in establishing the etiology due to the need for laboratories with personnel and equipment that allow the rapid and reliable identification of the causative microorganisms.
Choi HG, Seo SJ, Hong CK, Ro BI. Cutaneous infection by Geotrichum candidum. Korean J Med Mycol. 1999;4:69–74. This article is the second of only two reports of superficial skin infection with G. candidum.
Afany NA, Djawad K. Squamous cell carcinoma with co-infection of Microsphaeropsis arundinis and Geotrichum candidum: a rare case report. Open Access Maced J Med Sci. 2022;10:11–4. https://doi.org/10.3889/oamjms.2022.7994. This recent case report presents a patient with squamous cell carcinoma and cutaneous infection with Microsphaeropsis arundinis and G. candidum.
Bonifaz A, Aristimuño TM. Geotricosis cutánea superficial. Revisión del tema a propósito de tres casos estudiados. Dermatología Rev Mex. 1987;31:25–8. Based on the search, this article is one of only two reports of superficial skin infections.
Goldman S, Lipscomb PR, Ulrich JA. Geotrichum tumefaction of the hand. Report of a case. J Bone Joint Surg Am. 1969 Apr;51(3):587–90.
Kassamali H, Anaissie E, Ro J, Rolston K, Kantarjian H, Fainstein V, Bodey GP. Disseminated Geotrichum candidum infection. J Clin Microbiol. 1987;25:1782–3. https://doi.org/10.1128/jcm.25.9.1782-1783.1987.
Anaissie E, Bodey GP, Kantarjian H, Ro J, Vartivarian SE, Hopfer R, et al. New spectrum of fungal infections in patients with cancer. Rev Infect Dis. 1989;11:369–78. https://doi.org/10.1093/clinids/11.3.369.
Donnelly JP, Chen SC, Kauffman CA, Steinbach WJ, Baddley JW, Verweij PE, et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020;71:1367–76. https://doi.org/10.1093/cid/ciz1008.
Forster J, Koc Ö, Koeppel MB, Hamprecht A, Kurzai O, Suerbaum S, et al. β-1,3-d-Glucan and galactomannan as biomarkers for the detection of invasive Geotrichum and Magnusiomyces infections: a retrospective evaluation. J Clin Microbiol. 2022;60:e0160721. https://doi.org/10.1128/JCM.01607-21.
Arendrup MC, Boekhout T, Akova M, Meis JF, Cornely OA, Lortholary O, et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of rare invasive yeast infections. Clin Microbiol Infect. 2014;20(Suppl 3):76–98. https://doi.org/10.1111/1469-0691.12360.
Ghosh P, Boler AK. Geotrichum candidum: a rare primary pathogen in pulmonary geotrichosis. Indian J Med Res. 2020;152(Suppl 1):S123–4. https://doi.org/10.4103/ijmr.IJMR_2202_19.
Ceballos GA, Cortes G, Morio F, Zamora CEL, Linares MY, Ariza BE, et al. Comparison between MALDI-TOF MS and MicroScan in the identification of emerging and multidrug resistant yeasts in a fourth-level hospital in Bogotá, Colombia. BMC Microbiol. 2019;19:106. https://doi.org/10.1186/s12866-019-1482-y.
Galán F, García-Agudo L, Guerrero I, Marín P, García-Tapia A, García-Martos P, et al. Evaluación de la espectrometría de masas en la identificación de levaduras de interés clínico [Evaluation of mass spectrometry for the identification of clinically interesting yeasts]. Enferm Infecc Microbiol Clin. 2015;33:372–8. https://doi.org/10.1016/j.eimc.2014.10.003.
Marklein G, Josten M, Klanke U, Müller E, Horré R, Maier T, et al. Matrix-assisted laser desorption ionization-time of flight mass spectrometry for fast and reliable identification of clinical yeast isolates. J Clin Microbiol. 2009;47:2912–7. https://doi.org/10.1128/JCM.00389-09.
Westblade LF, Jennemann R, Branda JA, Bythrow M, Ferraro MJ, Garner OB, et al. Multicenter study evaluating the Vitek MS system for identification of medically important yeasts. J Clin Microbiol. 2013;51:2267–72. https://doi.org/10.1128/JCM.00680-13.
Kolecka A, Khayhan K, Groenewald M, Theelen B, Arabatzis M, Velegraki A, et al. Identification of medically relevant species of arthroconidial yeasts by use of matrix-assisted laser desorption ionization-time of flight mass spectrometry. J Clin Microbiol. 2013;51:2491–500. https://doi.org/10.1128/JCM.00470-13.
Bonifaz A, Montelongo MF, Araiza J, González GM, Treviño RR, Flores GA, et al. Evaluación de MALDI-TOF MS para la identificación de levaduras patógenas oportunistas de muestras clínicas [Evaluation of MALDI-TOF MS for the identification of opportunistic pathogenic yeasts of clinical samples]. Rev Chilena Infectol. 2019;36:790–3. https://doi.org/10.4067/S0716-10182019000600790.
Nenoff P, Oswald U, Haustein UF. In vitro susceptibility of yeasts for fluconazole and itraconazole. Evaluation of a microdilution test. Mycoses. 1999;42:629–39. https://doi.org/10.1046/j.1439-0507.1999.00510.x.
Wildfeuer A, Seidl HP, Paule I, Haberreiter A. In vitro evaluation of voriconazole against clinical isolates of yeasts, moulds and dermatophytes in comparison with itraconazole, ketoconazole, amphotericin B and griseofulvin. Mycoses. 1998;41:309–19. https://doi.org/10.1111/j.1439-0507.1998.tb00344.x.
Dannaoui E, Lortholary O, Raoux D, Bougnoux ME, Galeazzi G, Lawrence C, et al. Comparative in vitro activities of caspofungin and micafungin, determined using the method of the European Committee on Antimicrobial Susceptibility Testing, against yeast isolates obtained in France in 2005-2006. Antimicrob Agents Chemother. 2008;52:778–81. https://doi.org/10.1128/AAC.01140-07.
Esposto MC, Prigitano A, Lo Cascio G, Ossi C, Grancini A, Cavanna C, et al. Yeast-like filamentous fungi: molecular identification and in vitro susceptibility study. Med Mycol. 2019;57:909–13. https://doi.org/10.1093/mmy/myy133.
Durán GL, Seidel D, Vehreschild MJ, Hamprecht A, Kindo A, Racil Z, Demeter J, et al. Invasive infections due to Saprochaete and Geotrichum species: report of 23 cases from the FungiScope Registry. Mycoses. 2017;60:273–9. https://doi.org/10.1111/myc.12595.
Córdoba S, Vivot W, Bosco BME, Taverna C, Szusz W, Murisengo O, et al. Species distribution and susceptibility profile of yeasts isolated from blood cultures: results of a multicenter active laboratory-based surveillance study in Argentina. Rev Argent Microbiol. 2011;43:176–85. https://doi.org/10.1590/S0325-75412011000300003.
Buchta V, Otcenásek M. Geotrichum candidum--an opportunistic agent of mycotic diseases. Mycoses. 1988;31(7):363–70. https://doi.org/10.1111/j.1439-0507.1988.tb04432.x.
Cuenca EM, Gomez LA, Mellado E, Buitrago MJ, Monzon A, Rodriguez TJL. Head-to-head comparison of the activities of currently available antifungal agents against 3,378 Spanish clinical isolates of yeasts and filamentous fungi. Antimicrob Agents Chemother. 2006;50:917–21. https://doi.org/10.1128/AAC.50.3.917-921.2006.
Heinic GS, Greenspan D, MacPhail LA, Greenspan JS. Oral Geotrichum candidum infection associated with HIV infection. A case report. Oral Surg Oral Med Oral Pathol. 1992;73(6):726–8. https://doi.org/10.1016/0030-4220(92)90019-m.
Kamilari E, Stanton C, Reen FJ, Ross RP. Uncovering the biotechnological importance of Geotrichum candidum. Foods. 2023;12:1124. https://doi.org/10.3390/foods12061124.
Wu Y, Wang X, Yin Z, Dong J. Geotrichum candidum arthrospore cell wall particles as a novel carrier for curcumin encapsulation. Food Chem. 2023;404(Pt B):134308. https://doi.org/10.1016/j.foodchem.2022.134308.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Román-Montes, C.M., Sifuentes-Osornio, J. & Martínez-Gamboa, A. Cutaneous Infections by Geotrichum spp.. Curr Fungal Infect Rep 18, 60–68 (2024). https://doi.org/10.1007/s12281-024-00481-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12281-024-00481-9