
Abstract
Neoadjuvant therapy is the gold standard treatment of locally advanced rectal cancer. It may induce complete sterilization of tumor cell and decreases its local recurrence rate. While 15–20% of patients were found to have pathological complete response (pCR) with combined multimodal therapy, Asian data were generally scarce. pCR rate can indicate the suitability of applying the “watch-and-wait” strategy, which advocates deferment of surgery that can alleviate surgery-associated morbidity.To determine the percentage of pCR of rectal cancer after neoadjuvant therapy. Patients diagnosed with rectal cancer underwent treatment from 2013 to 2017 were retrieved retrospectively. Demographic data, tumor localization, pre- and post-operative pathological reports, neoadjuvant therapy, and pCR status were collected from patients’ records. A total of 242 out of 259 patients were treated with definitive rectal surgery. Mean age was 67.1 years old. Chinese ethnicity and male gender were predominant (n = 131, 54.1% and n = 146, 64.3% respectively). More than half (n = 124, 51.2%) had tumor located at mid or low rectum. Histologically, moderate differentiated adenocarcinoma was predominant (n = 227, 93.8%). Merely half (n = 123, 50.8%) of the patients received neoadjuvant chemoradiation therapy, but only 12 (9.8%) had a pCR. From follow-up on these 12 pCR patients, most had 2-year disease-free survival but 1 (8.3%) of the pCR had distant metastasis within 1-year post-surgery. The pathological complete response rate in our center was lower than reported. Stringent patient selection with close follow-up for patients should be carried out if the “watch-and-wait” strategy is implemented in our population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer is the second most common cancer and a leading cause of death in Malaysia [1]. Surgical resection is the cornerstone of curative management, with total mesorectal excision (TME) plays a fundamental role in patients who undergo rectal surgery [2,3,4]. With advancement in oncological therapies, neoadjuvant therapy prior to surgical resection of rectal cancer increased overall survival, disease-free survival, and reduced local recurrence rate [5, 6]. Therefore, neoadjuvant therapy is now the gold standard of treatment for locally advanced mid and low rectal cancer before subjecting patients to curative surgery resection (with criteria of T3 and above, positive mesorectal nodes, mesorectal fascia involvement or when mesorectal fascia is threatened) [7]. Neoadjuvant therapy is given to downstage and downsize the rectal tumor, as well as possible for preservation of sphincters for distal rectal tumor.
Neoadjuvant therapy alone may lead to significant regression of tumor, which provides an opportunity for patients to avoid radical surgery [8]. As such, a “watch-and-wait” protocol was suggested for patients with rectal cancer who received neoadjuvant therapy and showed clinical complete response (cCR). This protocol advocates monitoring of these patients frequently—both clinically and radiologically—while holding off the surgery and waiting for the natural progression of disease to take place. This watch-and-wait strategy can preserve patients’ functionality and quality of life, as well as minimize surgical-related morbidities and post-operative mortality [8]. The adaptation of the watch-and-wait approach varies by practice [9]. Some centers tend to proceed with surgical procedure based on initial tumor signs, while some implement the watch-and-wait protocol as post-neoadjuvant re-staging leads to the modification of the initial plan [10].
One challenge in implementing the watch-and-wait protocol is the definition of cCR, which is yet to be standardized but was recommended to be based on very strict clinical, endoscopical, and radiological criteria [11]. From the endoscopic perspective, cCR should harbor no more than whitening of the mucosa or telangiectasia with normal mucosa integrity. Clinically, the presence of any deep or superficial residual ulcer, any palpable nodule or any significant stenosis that impede the proctoscope from sliding through are features described as incomplete clinical response [12]. Radiologically, patients are considered to have a clinical complete response when there is shrinkage of the tumor with homogenous low signal intensity on the T2 magnetic resonance imaging (MRI) images characterizing fibrosis and no residual tumor signal. There must be no lymph node involvement and no signal of extramural vascular involvement [13].
It was reported that neoadjuvant therapy can induce up to 25% cCR, while 20–25% of cCR after surgery had pCR [9,10,11]. However, there are potential risks in applying this protocol, which are attributed to the absence of direct pathologic confirmation of cCR, as cCR patients do not undergo surgery unless they have a recurrence [13,14,15,16,17]. In addition, previous study has shown a poor concordance between pathological assessment of response to preoperative neoadjuvant therapy and clinical assessment based on digital rectal examination on top of sigmoidoscopy [18, 19]. Moreover, a recent study has shown that many patients who achieved pathological complete response (pCR) were found to have mucosal abnormalities that were inconsistent with a cCR [20].
Although there was information reported on pCR after neoadjuvant therapy, a Malaysian cohort from last decade showed low pCR rate compared with other countries, and there is no newer data to date, in which pCR rate might have improved due to medical advances [21]. This study aims in reporting the proportion of patients with rectal adenocarcinoma who had a pCR after treatment with neoadjuvant therapy in a colorectal surgery department, a tertiary care university hospital in Malaysia.
Method
Settings
This retrospective cohort study reviewed all patients who diagnosed with rectal adenocarcinoma and underwent treatment plans over 5 years from January 2013 to December 2017 in a colorectal center and major tertiary referral hospital in Central region of Malaysia, which is also an academic teaching hospital. This study was reported in line with the strengthening the reporting of cohort studies in surgery (STROCSS) criteria [22].
Eligibility Criteria
All patients who diagnosed with rectal adenocarcinoma and underwent curative treatment in our institution from January 2013 to December 2017 were included in analyses.
Surgical Procedures and Associated Care
All patients were diagnosed with rectal adenocarcinoma via histology from the biopsy during colonoscopy. Complete staging was done including computed tomography scan of thorax, abdomen, pelvis (CT TAP) for distance staging and pelvic MRI (magnetic resonance imaging) for local staging. Multidisciplinary discussion (MDT) involving radiologists, pathologists, oncologists, and colorectal team was done for each patient to discuss whether to proceed with upfront curative surgery or neoadjuvant chemoradiotherapy. Neoadjuvant therapy was decided based on distance and local staging of the rectal cancer according to National Comprehensive Cancer Network (NCCN) guideline, with mid and low rectal cancers locally staged T3 and above, or mesorectal nodes positive, or mesorectal fascia (MRF) involved or threatened (MRF < 1 mm) in MRI local staging [7].
Patients who decided with upfront neoadjuvant therapy were then referred to oncologists for administrative chemoradiation. Most of the neoadjuvant regimen were decided by oncologists and involved long course chemoradiation whereby long course radiation was given for 5 weeks with radiation dose of 45–50.4 G in 25 fractions with concurrent 5-fluorouracil-based chemotherapy (either oral or intravenous route) given in week 1 and week 5 of radiation. Some patients with bulky upper rectum involving surrounding structures were given systemic chemotherapy before curative surgery. After completing chemoradiation, patients were referred back to colorectal team with post-neoadjuvant therapy MRI performed for local restaging of the rectal cancer. Colorectal team scheduled the surgeries about 10–12 weeks post-neoadjuvant therapy for all rectal cancers.
Patients subjected to surgery were reviewed by anesthetists preoperatively with optimization of their comorbidities. We adhered to Enhanced Recovery After Surgery (ERAS) protocol. All patients were given bowel preparation before surgery.
Surgeries were performed by colorectal team consisting of two colorectal consultants and colorectal fellows. Patients were operated under general anesthesia in supine lithotomy position. Surgery was performed via laparoscopic technique or open laparotomy depending on the suitability of the cases. The resected specimens were sent to Pathology Department for histopathological analysis. Patients were given standard post-operative care according to ERAS protocol.
Patients were followed up for at least 2 years post-surgery. pCR was defined as absence of tumor cell microscopically in a complete resected specimen.
Data Collection
All patients diagnosed with rectal adenocarcinoma in our institution, whose records were complete and who were treated between 2013 and 2017, were included. For the analysis, patients who did not undergo curative surgical resection were excluded (palliative resection, palliative stoma diversion, open, and closed all excluded).
Information was collected from patients’ admission files which include the following information: patients’ demographic data, histopathological characteristics of the tumor, tumor localization, neoadjuvant regimen, histopathological report of the resected specimens, and recurrence or metastasis during follow-up.
Sample Size Calculation and Statistical Analysis
Sample size estimation was calculated using the population proportion formulae [23]. Prior data indicated that the proportion of patients with rectal adenocarcinoma with pCR after neoadjuvant therapy was 0.105 [21] and population size is 300. With the type I error probability and precision of 0.05 and 0.05 and an additional 20% dropout rate, the sample size required was 123 samples.
The data obtained were entered in a database using Excel 2013. Patients were divided to two groups: those who received neoadjuvant and those who did not. The data analysis was performed by using the IBM SPSS Statistics for Windows version 23.0 (IBM Corp., New York). The categorical variables were summarized as frequencies and percentages, and the numerical variables as means and standard deviations (SD). Chi-square test was used to study association between categorical data, while Fisher’s exact test was used if the assumptions for chi-square test were not met. Independent T test was used to compare continuous variables between both groups. All probability values were two-sided and a level of significance of less than 0.05 (p value < 0.05) was considered as statistically significant.
Results
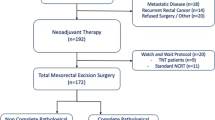
From 2013 till 2017, a total of 259 patients were diagnosed with rectal cancer. However, 242 out of 259 patients (93.4%) successfully completed the definitive curative surgery whereby the tumors were resected out. Seventeen patients (6.6%) with advanced disease during surgery ended up with palliative surgery (defunctioning stoma) or did not proceed with the surgery.
Mean age of patients’ population who had definitive surgery (n = 242) was 67.1 (SD 10.9) years. Chinese ethnicity was predominant in the study population at 60.3% (n = 146), followed by Malays (n = 69, 28.5%) and Indians (n = 27, 11.2%). There was a slight predominance of male gender (n = 131, 54.1%) (Table 1).
Half of the patients received neoadjuvant therapy (n = 123, 50.8%). Both groups did not show significant difference between gender, ethnicity, and when the surgery was performed (Table 1). Mean age of each group were 65.7 (SD 10.6) and 68.6 (SD 11.1) years old, respectively (p = 0.036), implying that patients with neoadjuvant therapy were younger than patients without the neoadjuvant therapy.
Histologically, most tumors were moderately differentiated adenocarcinoma (n = 227, 93.8%). Well-differentiated adenocarcinoma was only reported in five patients (2.1%). Poorly or undifferentiated adenocarcinoma was rather rare in our study population (n = 10, 4.1%). There was no statistically significant difference between both groups for the histological classification (Table 1) (p = 0.92).
Most of mid and low rectal cancer cases were given neoadjuvant therapy (n = 112, 90.3%), while the remaining mid and low rectal cancer cases (n = 12, 9.7%) were not given neoadjuvant therapy, whereby this was the group of mid and low rectal cancers which were in early stage. In contrast with patients with neoadjuvant therapy which comprised of mainly mid or low rectal cancer cases, most patients without neoadjuvant therapy had upper rectal cancer (n = 107, 89.9%) (Table 1) (p < 0.001). There was a small proportion of upper rectal cancers were subjected to neoadjuvant therapy (n = 11, 8.9%), as this was the group whereby the upper rectal tumors were bulky and threaten the surrounding structures in imaging (Table 1).
More than half of the patients who received neoadjuvant therapy were in stages N1-2 and M0 (n = 71, 57.7%). Most patients without metastasis received neoadjuvant therapy, except those without clear evidence of locally advanced rectal adenocarcinoma, whom were the majority of the cases which did not receive neoadjuvant therapy (Table 1).
Among patients who underwent neoadjuvant therapy (n = 123, 50.8%) followed by definitive surgery, 9.8% (n = 12) patients showed pCR in their resected full-post-operative histopathological report. The 2-year follow-up for these 12 pCR patients showed that there was no local recurrence but 1 (8.3%) pCR patient was found to have distant liver metastasis without local recurrence during surveillance with CT thorax, abdomen, and pelvis (Table 2).
Discussion
Our population showed a mere 9.8% pCR that was lower than previously reported [9, 21]. This reflects a potential concern of utilizing the increasingly popular watch-and-wait protocol for these patients with low pCR rate to begin with, as most of these patients would eventually require surgery. As low pCR rates are indicative of prognostically unfavorable biological tumor profiles in our population, the study population might have higher propensity for local recurrence, distant metastasis and poorer survival [8]. Therefore, the watch-and-wait strategy might deprive these prognostically unfavorable patients of the opportunity for cure when the surgery is not performed in the timely manner following the neoadjuvant therapy.
There are many factors influencing cCR and pCR rates post-neoadjuvant therapy. Timing interval between neoadjuvant therapy and curative surgery is a potential factor. Longer duration was shown to have better effects than the traditional 6-week interval [24]. NCCN guideline recommends that surgery to be performed within 5–12 weeks after the end of neoadjuvant therapy [7]. A meta-analysis observed higher pCR in those who waited longer than 7 weeks [9]. Some patients might take longer time to achieve cCR; up to 37% of cCR was reported with 10–16 weeks and 73% was reported with interval of more than 16 weeks [38]. As our center provides a 10- to 12-week interval before subjecting patients for curative surgery, the timing interval might be a factor of low pCR in our center.
Besides the timing of surgery, the disease severity and degree of tumor cell differentiation are important in determining pCR rate. According to a retrospective study, poorly differentiated or undifferentiated tumors had lower pCR rate [25]. Our study population were generally given neoadjuvant therapy in more severe stages of the disease (with most cases were locally advanced at stage T3 and above ± mesorectal nodes positive or MRF positive/threatened and with less than 10% of well-differentiated tumors), which possibly explains the lower pCR rate among our study population. The mid and low rectal cancer cases without neoadjuvant therapy were mainly early rectal cancer (T1 or T2, mesorectal nodes negative, or without involvement of MRF). This contrasts with previous studies that reported higher pCR rates as they recruited patients with milder stages of disease [17, 25, 26]. The criteria for neoadjuvant therapy vary across institutions; some centers would not prefer to expose patients with early stage rectal cancers to potential toxicities of neoadjuvant therapy as the benefits are yet to be confirmed [26]. The study findings highlighted the importance of care in interpreting reported pCR outcomes of existing literature with limited generalizability to local practice.
The location of rectal tumor can affect the pCR rate. Tumors in the lower end or upper third of rectum have been reported to be less likely to have pCR, which possibly explains the low pCR rate among our study population in which 61.0% of the tumors were located in the lower end and upper third of rectum [27]. Most mid and low rectal cancer cases in our study population were given neoadjuvant therapy as the tumors were locally advanced. Less number of patients with upper rectal cancer received neoadjuvant therapy, which was in line with European Society for Medical Oncology (ESMO) guideline in which upper rectal cancers (> 12 cm from the anal verge) above the peritoneal reflection do not benefit from preoperative short-course preoperative radiotherapy or chemoradiation [28]. In addition, resection was given to patients with upper rectal cancer that could be well resected, or that occurred outside the radiotherapy field of pelvis. A small number of upper rectal cancers were given neoadjuvant therapy based on MRI as the tumors were either appeared too bulky or involved surrounding structures (bladder, uterus, prostate, or pelvic side wall) or difficulty to obtain R0 resection, in which oncological safety was taken into consideration before subjecting to definitive surgery. Neoadjuvant therapy was given to downstage and downsize these tumors. The study findings suggest that patients with tumors at the lower end or upper third of rectum should be counseled on the potentially low pCR rate and the implications when deciding for curative surgery or watch-and-wait strategy.
Young age is a reported predictive factor of lower pCR rate following neoadjuvant therapy [29]. Our study population reported a relatively younger patient population who underwent neoadjuvant therapy, which possibly explains the low pCR rate in our study population. It was postulated that these younger patients had more aggressive pathological features, believed to be associated with a higher CD133+ cancer stem cell burden, which contributed to poorer response to neoadjuvant therapy [29]. This warrants more research to evaluate the need to optimize the neoadjuvant therapy in young patients.
In addition, pCR does not necessarily imply complete cure, as shown by the presence of metastasis post-pCR from our study findings. Hence, tumor biology or preoperative radiological staging should be considered during prescribing adjuvant therapy. The 3-year regrowth rate increases based on tumor T-staging. Longer follow-up should be recommended to detect early any recurrence or metastasis.
As pCR can only be confirmed by performing radical surgery, the assessment of tumor response post-neoadjuvant therapy in watch-and-wait protocol will be based on a surrogate measure (cCR) with poorer accuracy than direct histological examination, with only 25% of cCR patients reported to have pCR [19]. In addition, the long-term survival and local recurrence rates with watch-and-wait approach were inconsistent [17, 25]. Therefore, cCR classification must be based on very strict criteria [8]. To adopt watch-and-wait protocol, it is advocated that frequent follow-up should be done with MRI pelvis, colonoscopy, and digital examination every 1–2 months for the first year, every 3 months for the second year, and every 6 months thereafter [8]. Therefore, it is important to be careful in selecting patients for watch-and-wait protocol post-neoadjuvant therapy in rectal adenocarcinoma in population with low pCR, with a need of multidisciplinary approach and various assessments to measure cCR, without compromising the balance of quality of life and achieving good disease/survival outcomes.
Other challenges in implementing “watch-and-wait” strategy in our setting include potential poor patient compliance on the follow-up procedures, as well as potential of interobserver variability [21]. As such, implementation of “watch-and-wait” protocol among our patients might incur more costs with low pCR rate that renders surgery eventually inevitable, while additional healthcare costs are to be incurred by various surveillance procedures at frequent intervals. Therefore, the benefits and cost-effectiveness of this protocol in our study population requires further investigation. Although a study observed decreased costs associated with watch-and-wait protocol, the generalizability is limited, given the lower pCR found among our population, as well as different healthcare costs in our country [30].
Despite the uncertainties and inconveniences of the watch-and-wait protocol, this approach might be required during the challenging times of the COVID-19 pandemic in which surgical prioritisation might be required due to limited healthcare resources [31]. In view of low pCR rates from our center, better tools with higher sensitivity are needed to stratify patients who are likely to benefit from non-operative management after neoadjuvant therapy [18,19,20]. This approach may be useful for to those who have cCR based on radiological and endoscopic criteria and refuse for surgery after thorough discussion and explanation about the risks and benefits [4].
This study had its limitations. This retrospective study was subjected to potential selection bias, but randomization of patients is ethically challenging, when potentially curative options can only be obtainable by chance. Variability in the neoadjuvant regimes exists, but the regimens were all based on the institutional protocols. In addition, cCR is not obtainable from the study population due to the scarcity of credentialed radiologists in our institution. Besides, this study was limited by the limited generalizability of the data to other settings, given that other institutions might have different criteria in providing neoadjuvant therapy for rectal cancer patients. There are other potential factors of low pCR that were not studied, such as genetic polymorphisms [32], as well as variation in gene expression related with tumor biology [33]. The study was not designed to identify the causative factors of low pCR. While the radiotherapy technique, machine, and skills might be related with pCR rate, future studies could be designed to identify the factors of low pCR in our population. In addition, the study was exploratory in nature and not intended for survival analysis (such as the Kaplan-Meier method) as the assumptions required were violated by the unavailability of the exact survival time for each patient.
Conclusion
The pathological complete response rate post-neoadjuvant treatment for rectal cancer in our center showed lower rate than reported, suggesting a need of stringent patient selection process with close surveillance if surgical resection post-neoadjuvant treatment has to be delayed in our population. The benefits must outweigh the risk if watch-and-wait strategy is offered to our patient population.
Data availability
Data are available upon request.
Code Availability
Not applicable
References
National Cancer Registry, National Cancer Institute (2018) Malaysian study on cancer survival (MySCan). Ministry of Health Malaysia, Kuala Lumpur
Phang PT, Wang X (2014) Current controversies in neoadjuvant chemoradiation of rectal cancer. Surg Oncol Clin N Am 23(1):79–92. https://doi.org/10.1016/j.soc.2013.09.008
Torok JA, Palta M, Willett CG, Czito BG (2016) Nonoperative management of rectal cancer. Cancer 122(1):34–41. https://doi.org/10.1002/cncr.29735
Dedemadi G, Wexner SD (2012) Complete response after neoadjuvant therapy in rectal cancer: to operate or not to operate? Dig Dis 30(Suppl 2):109–117. https://doi.org/10.1159/000342039
Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, Martus P, Tschmelitsch J, Hager E, Hess CF, Karstens JH, Liersch T, Schmidberger H, Raab R (2004) Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351(17):1731–1740. https://doi.org/10.1056/NEJMoa040694
Andrade VAD, Coy CSR, Leal RF, Fagundes JJ, Martinez CAR, Ayrizono MDLS (2016) Neoadjuvant therapy and surgery for rectal cancer. Comparative study between partial and complete pathological response. Arq Gastroenterol 53:163–168
Benson A, Venook A, Al-Hawary M, Cederquist L, Chen Y-J, Ciombor K et al (2018) Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Cancer Netw 16:874–901. https://doi.org/10.6004/jnccn.2018.0061
Habr-Gama A, Bruzzi MS, Morici ML, Julião GPS, Perez RO. (2018). The proper treatment for the complete responder after neoadjuvant therapy. In: G. Dapri & J. H. Marks (Eds.), Surgical Techniques in Rectal Cancer: Transanal, Laparoscopic and Robotic Approach. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55579-7
Wang XJ, Zheng ZR, Chi P, Lin HM, Lu XR, Huang Y (2016) Effect of interval between neoadjuvant chemoradiotherapy and surgery on oncological outcome for rectal cancer: a systematic review and meta-analysis. Gastroenterol Res Pract 2016:6756859–6756813. https://doi.org/10.1155/2016/6756859
Habr-Gama A, Perez RO, Proscurshim I, Campos FG, Nadalin W, Kiss D et al (2006) Patterns of failure and survival for nonoperative treatment of stage c0 distal rectal cancer following neoadjuvant chemoradiation therapy. J Gastrointest Surg 10(10):1319–1329. https://doi.org/10.1016/j.gassur.2006.09.005
Habr-Gama A, Perez RO, Wynn G, Marks J, Kessler H, Gama-Rodrigues J (2010) Complete clinical response after neoadjuvant chemoradiation therapy for distal rectal cancer: characterization of clinical and endoscopic findings for standardization. Dis Colon Rectum 53(12):1692–1698. https://doi.org/10.1007/DCR.0b013e3181f42b89
McBrearty A, McCallion K, Moorehead RJ, McAllister I, Mulholland K, Gilliland R, Campbell WJ (2016) Re-staging following long-course chemoradiotherapy for rectal cancer: does it influence management? Ulster Med J 85(3):178–181
Park IJ, You YN, Agarwal A, Skibber JM, Rodriguez-Bigas MA, Eng C, Feig BW, Das P, Krishnan S, Crane CH, Hu CY, Chang GJ (2012) Neoadjuvant treatment response as an early response indicator for patients with rectal cancer. J Clin Oncol 30(15):1770–1776. https://doi.org/10.1200/jco.2011.39.7901
Habr-Gama A, Sabbaga J, Gama-Rodrigues J, Sao Juliao GP, Proscurshim I, Bailao Aguilar P et al (2013) Watch and wait approach following extended neoadjuvant chemoradiation for distal rectal cancer: are we getting closer to anal cancer management? Dis Colon Rectum 56(10):1109–1117. https://doi.org/10.1097/DCR.0b013e3182a25c4e
Habr-Gama A, Sao Juliao GP, Perez RO (2015) Nonoperative management of rectal cancer: identifying the ideal patients. Hematol Oncol Clin North Am 29(1):135–151. https://doi.org/10.1016/j.hoc.2014.09.004
Habr-Gama A, Perez RO, Sao Juliao GP, Proscurshim I, Gama-Rodrigues J (2011) Nonoperative approaches to rectal cancer: a critical evaluation. Semin Radiat Oncol 21(3):234–239. https://doi.org/10.1016/j.semradonc.2011.02.010
van der Valk MJM, Hilling DE, Bastiaannet E, Meershoek-Klein Kranenbarg E, Beets GL, Figueiredo NL, Habr-Gama A, Perez RO, Renehan AG, van de Velde CJH, Ahlberg M, Appelt A, Asoglu O, Bär MT, Barroca R, Beets-Tan RGH, Belgers EHJ, Bosker RJI, Breukink SO, Bujko K, Carvalho C, Cunningham C, Creavin B, D'Hoore A, Gérard JP, Gollins S, Hoff C, Holman FA, Hupkens BJP, Iseas S, Jakobsen A, Keshvari A, Koopal SA, Kusters M, Langheinrich M, Leijtens JWA, Maas M, Malcomson L, Mamedli ZZ, Martling A, Matzel KE, Melenhorst J, Morici ML, Murad-Regadas SM, O'Dwyer ST, Peeters KCMJ, Rosa I, Rossi G, Rutten HJT, Sanchez Loria F, van der Sande ME, São Julião GP, Saunders M, Sun Myint A, van der Sluis H, Schiappa R, Scott N, Stoot JHMB, Talsma AK, Terrasson I, Tokmak H, Vaccaro CA, Vahrmeijer AL, Wasowicz DK, Westreenen HL, Winter DC, Wolthuis AM, Zimmerman DDE (2018) Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): an international multicentre registry study. Lancet 391(10139):2537–2545. https://doi.org/10.1016/s0140-6736(18)31078-x
Guillem JG, Chessin DB, Shia J, Moore HG, Mazumdar M, Bernard B, Paty PB, Saltz L, Minsky BD, Weiser MR, Temple LKF, Cohen AM, Wong WD (2005) Clinical examination following preoperative chemoradiation for rectal cancer is not a reliable surrogate end point. J Clin Oncol 23(15):3475–3479. https://doi.org/10.1200/jco.2005.06.114
Hiotis SP, Weber SM, Cohen AM, Minsky BD, Paty PB, Guillem JG, Wagman R, Saltz LB, Wong WD (2002) Assessing the predictive value of clinical complete response to neoadjuvant therapy for rectal cancer: an analysis of 488 patients. J Am Coll Surg 194(2):131–135; discussion 135-136. https://doi.org/10.1016/s1072-7515(01)01159-0
Smith FM, Wiland H, Mace A, Pai RK, Kalady MF (2014) Clinical criteria underestimate complete pathological response in rectal cancer treated with neoadjuvant chemoradiotherapy. Dis Colon Rectum 57(3):311–315. https://doi.org/10.1097/DCR.0b013e3182a84eba
Lee WC, Yusof MM, Lau FN, Phua VC (2013) Preoperative long course chemoirradiation in a developing country for rectal carcinoma: Kuala Lumpur hospital experience. Asian Pac J Cancer Prev 14(6):3941–3944. https://doi.org/10.7314/apjcp.2013.14.6.3941
Agha R, Abdall-Razak A, Crossley E, Dowlut N, Iosifidis C, Mathew G, Beamishaj, Bashashati M, Millham FH, Orgill DP, Noureldin A, Nixon IJ, Alsawadi A, Bradley PJ, Giordano S, Laskin DM, Basu S, Johnston M, Muensterer OJ, Mukherjee I, Ngu JCY, Valmasoni M, Pagano D, Vasudevan B, Rosin RD, McCaul JA, Albrecht J, Hoffman JR, Thorat MA, Massarut S, Thoma A, Kirshtein B, Afifi RY, Farooq N, Challacombe B, Pai PS, Perakath B, Kadioglu H, Aronson JK, Raveendran K, Machado-Aranda D, Klappenbach R, Healy D, Miguel D, Leles CR, Ather MH (2019) STROCSS 2019 Guideline: Strengthening the reporting of cohort studies in surgery. Int J Surg 72:156–165. https://doi.org/10.1016/j.ijsu.2019.11.002
Lemeshow S, Hosmer DW, Klar J, Lwanga SK, World Health Organization (1990) Adequacy of sample size in health studies. Wiley, Chichester
Wasserberg N (2014) Interval to surgery after neoadjuvant treatment for colorectal cancer. World J Gastroenterol 20(15):4256–4262. https://doi.org/10.3748/wjg.v20.i15.4256
Choi E, Kim JH, Kim OB, Kim MY, Oh YK, Baek SG (2016) Predictors of pathologic complete response after preoperative concurrent chemoradiotherapy of rectal cancer: a single center experience. Radiat Oncol J 34(2):106–112. https://doi.org/10.3857/roj.2015.01585
Esen E, Karahasanoğlu T, Özben V, Aytaç E, Baca B, Hamzaoğlu İ, Remzi FH (2019) Complete response after neoadjuvant treatment for rectal cancer. Lancet 393(10182):1694. https://doi.org/10.1016/s0140-6736(18)33203-3
Patel SV, Roxburgh CS, Vakiani E, Shia J, Smith JJ, Temple LK, Paty P, Garcia-Aguilar J, Nash G, Guillem J, Wu A, Reyngold M, Weiser MR (2016) Distance to the anal verge is associated with pathologic complete response to neoadjuvant therapy in locally advanced rectal cancer. J Surg Oncol 114(5):637–641. https://doi.org/10.1002/jso.24358
Glynne-Jones R, Wyrwicz L, Tiret E, Brown G, Rödel C, Cervantes A, Arnold D, ESMO Guidelines Committee (2017) Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 28:iv22–iv40. https://doi.org/10.1093/annonc/mdx224
Zhang Y, Yan L, Wu Y, Xu M, Liu X, Guan G (2020) Worse treatment response to neoadjuvant chemoradiotherapy in young patients with locally advanced rectal cancer. BMC Cancer 20(1):854. https://doi.org/10.1186/s12885-020-07359-2
Miller JA, Wang H, Chang DT, Pollom EL (2020) Cost-effectiveness and quality-adjusted survival of watch and wait after complete response to chemoradiotherapy for rectal cancer. J Natl Cancer Inst 112(8):792–801. https://doi.org/10.1093/jnci/djaa003
Al-Jabir A, Kerwan A, Nicola M, Alsafi Z, Khan M, Sohrabi C et al (2020) Impact of the Coronavirus (COVID-19) pandemic on surgical practice - Part 2 (surgical prioritisation). Int J Surg 79:233–248. https://doi.org/10.1016/j.ijsu.2020.05.002
Pander J, van Huis-Tanja L, Böhringer S, van der Straaten T, Gelderblom H, Punt C, Guchelaar HJ (2015) Genome wide association study for predictors of progression free survival in patients on capecitabine, oxaliplatin, bevacizumab and cetuximab in first-line therapy of metastatic colorectal cancer. PLoS One 10(7):e0131091. https://doi.org/10.1371/journal.pone.0131091
Gonçalves-Ribeiro S, Sanz-Pamplona R, Vidal A, Sanjuan X, Guillen Díaz-Maroto N, Soriano A, Guardiola J, Albert N, Martínez-Villacampa M, López I, Santos C, Serra-Musach J, Salazar R, Capellà G, Villanueva A, Molleví DG (2017) Prediction of pathological response to neoadjuvant treatment in rectal cancer with a two-protein immunohistochemical score derived from stromal gene-profiling. Ann Oncol 28(9):2160–2168. https://doi.org/10.1093/annonc/mdx293
Acknowledgements
We would like to thank the Director General of Health Malaysia for his permission to publish this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. This is a self-sponsored study.
Author information
Authors and Affiliations
Contributions
Leow Yeen Chin: study design, data collections, data analysis, writing, final revision. Ruben Gregory Xavier: study design, data collection, final revision. April Camilla Roslani: study design, writing, final revision. Lee Fei Yee: data analysis and writing, final revision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study protocol was approved by University Malaya Medical Centre Ethics Committee, Malaysia with protocol number MREC ID: 202074-8863, and registered with the National Medical Research Register, Malaysia, under the protocol number NMRR-20-1858-56252.
Consent to Participate
Not applicable as this is a retrospective observational study.
Consent for Publication
Not applicable as this is a retrospective observational study.
Conflicts of Interest
The authors declare they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Highlights
All locally advanced (T3 and T4, mesorectal nodes positive or mesorectal fascia involved or threatened) rectal adenocarcinoma with curative intention were subjected to neoadjuvant chemoradiation before curative surgical resection.
Near half (123 patients, 50.8%) received neoadjuvant therapy.
Pathological complete response (pCR) rate in our center was about 9.76% which is lower than what have reported implied that many factors could influence pCR rate.
More strict criteria to define complete clinical response (cCR) are required to adopt the “watch-and-wait protocol.”
Rights and permissions
About this article

Cite this article
Leow, Y.C., Roslani, A.C., Xavier, R.G. et al. Pathological Complete Response After Neoadjuvant Therapy in Rectal Adenocarcinoma: a 5-Year Follow-up. Indian J Surg 83 (Suppl 3), 768–775 (2021). https://doi.org/10.1007/s12262-021-02945-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-021-02945-5