
Abstract
The purpose of the present study was to investigate the effects of parental health problems on the probability of youths leaving upper secondary education before completion in Sweden, and to investigate potential gender differences in these effects. Medical and social microdata from Swedish administrative registers were used. The study population consisted of individuals born between 1987 and 1990 (N = 398,748) who were still alive and residing in Sweden in 2010. We employed a quasi-experimental pre-test post-test study design. Logistic regression was used to analyse the relationships between indicators of parental illness and young people’s early school leaving in relation to health and sociodemographic confounders. Having had a mother or father with psychiatric, but not somatic, illness that necessitated hospitalisation after completing compulsory schooling was significantly associated with an increased probability of leaving upper secondary education. We found no significant gender-specific interaction effects. The existence of these effects in Sweden, a country with an extensive institutional welfare system, suggests that similar but more pronounced effects may exist in regions lacking such systems.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
To understand the implications of poor health for young people’s education, one must also consider the effects of their parents’ health. Education profoundly influences individuals’ future life prospects as well as the economic growth and social cohesion of the societies in which they live. Researchers and policy developers therefore devote great attention to the support of disadvantaged children in school and ways of preventing early school leaving (Lyche 2010; OECD 2012). Poor health is one disadvantage that is strongly linked to negative school outcomes (Champaloux and Young 2015; Forrest et al. 2011; Maslow et al. 2011). Importantly, poor health is not just an individual problem that only affects the person who has fallen ill. In families, which are the focal units of this paper, health problems affect other family members as well as the person who is ill (Moffat and Redmond 2016; Wittenberg and Prosser 2013; Wittenberg et al. 2014). While the psychosocial difficulties associated with parental illness are recognized (Pakenham and Cox 2014; Sieh et al. 2010, 2013), its educational consequences have received much less attention in the existing literature.
The few published studies on this topic yielded mixed results and are considered inconclusive (see Chen 2016, 2017). For instance, a study using Taiwanese data (Chen 2014) indicated that parental illness had no adverse effect on children’s learning and academic performance. Conversely, an investigation based on data from Bosnia and Hercegovina (Bratti and Mendola 2014) found that children of ill mothers (but not of ill fathers) were less likely to be enrolled in higher education. This variability in findings is probably due to differences in the contexts of the studies, the illness indicators that were considered, and the measured educational outcomes. In Sweden – a country with a comprehensive welfare system that provides publicly funded health care and education to the entire population, as well as monetary benefits to those who are ill and cannot work – the issue of how parental illness affects children have only recently received serious attention. With the exception of one report (Hjern et al. 2013),Footnote 1 there are virtually no public data on the effects of parental illness on children’s schooling in the Swedish context.
To address this research gap, we investigate whether having a parent with psychiatric (mental) or somatic (physical) health problems is associated with early school leaving (ESL) from upper secondary education (i.e. after ages 15–16) in Sweden. To this end, we use medical and social microdata from several Swedish longitudinal national population registers covering 398,748 individuals born between 1987 and 1990. We begin by discussing ways in which parental illness could affect young people’s schooling, drawing on both theory and prior research findings. Then, we present empirical estimates based on models that adjust for a rich set of health and sociodemographic covariates. The longitudinal character of our dataset enables us to employ a quasi-experimental pre-test post-test study design that isolates exposure to parental illness requiring hospitalisation over a period that begins and ends with a measurement of the child’s academic achievement.
2 Previous Research and Theory
As mentioned, only a few published studies have examined the relationship between having a parent with ill health and young people’s educational outcomes. One study conducted in the Netherlands (Sieh et al. 2013) examined differences in (self-reported) school grades and found that children with parents having a chronic medical condition had an increased risk of poor academic achievement. Conversely, most children in the study conducted by Chen and Fish (2012) in the U.S. appeared to function adequately in terms of academic achievement; the authors found no direct association between parental illness and children’s academic performance. On the other hand, using a sample of 13,556 U.S. adolescents, Boardman et al. (2012) found a small difference in the probability of graduating from high school as a function of parental health. These findings are supported by Johnson and Reynolds (2013), who analysed longitudinal survey-data, also from the U.S., and found that a respondent’s probabilities of graduating from high school, attending college, and graduating from college were all significantly reduced if any member of the respondent’s household, (excluding the respondent youth themselves) had been hospitalised for a week during the preceding 5 years.
Despite some mixed results, most existing studies point to a negative relationship between parental illness and young people’s educational outcomes. In previous studies, two mechanisms are commonly invoked to explain how a parent’s illness could affect a child’s schooling: (1) the strain caused by the parent’s illness could reduce the child’s engagement at school, and (2) the parent’s illness could disrupt their involvement in the child’s education and general parenting activity. The first of these mechanisms is related to the distribution of family roles and its implications.
Theoretically, from a family systems perspective (e.g. Asen 1985; Rolland 1999; Pedersen and Revenson 2005), a family can be regarded as a system in which the family members are interrelating and interacting with each other; each member both affects and is affected by the other members. Families are organized in such a way as to ensure stability and continuity for their members and the family as a whole. Over time, a family goes through different phases and must cope with different challenges. Seen from a systems perspective, illness in the family is one such challenge that affects the family’s stability, disturbs its daily routine (the equilibrium of family functioning), and necessitates reorganisation – a change in one part of the system induces (compensatory) change in other parts. When a parent becomes ill, a common coping strategy is to redistribute family roles (Asen 1985; Rolland 1999). Since the ill parent’s ability to fulfil their responsibilities is reduced, greater demands are placed on other family members. In some cases, parental illness may require a child to take on adult roles prematurely. This may involve increased responsibility for household chores and parent/child role reversal.
Household chores and caring for a family member can be beneficial for a young person’s socialisation, helping them to develop a sense of responsibility and maturity. Extended responsibilities and chores can however be too great a burden, taking up time and energy that would otherwise have been directed towards schoolwork. Having to manage daily chores (e.g. supervising and helping siblings with homework or buying and cooking food) and/or the emotional responsibility of providing substantial or regular care (e.g. comforting siblings and parents who are sad, dissatisfied, angry or unhappy) can significantly affect a child’s development, participation, and opportunities, as well as educational attainment (Aldridge and Becker 2003; Winton 2003).
In parent/child role reversal, the parent-child interactions become centred around the parent’s needs rather than the child’s development (see e.g. Loch 2016), making the child a ‘young carer’ who may be subject to ‘parentification’. ‘Young carers’ are people under the age of eighteen who take on substantial caring tasks and levels of responsibility that would usually be associated with an adult (Warren 2007; Aldridge 2008; Smyth et al. 2011; Wihstutz 2011). The concept of parentification relates to family interactions in which the child takes on a developmentally inappropriate role, acting as a partner of his or her parent (see e.g. Harstone and Charles 2012; Charles et al. 2009; Winton 2003).
Familial role redistributions of the kind described above can deplete a child’s coping resources and reduce their school engagement. A large body of evidence indicates that school disengagement is an important educational indicator and a strong predictor of early school leaving (Appleton et al. 2006; Lee 2014; Skinner and Pitzer 2012; Tarabini et al. 2018). The concept of engagement, as defined by Fredricks et al. (2004), has three dimensions. The first, behavioural engagement, relates to positive conduct, contributing to class discussions and participating in school-related activities (i.e. school governance and extra-curricular activities). The second, emotional engagement, pertains to the sense of belonging and the affective bonds students form with their teachers and peers. The third, cognitive engagement, relates to students’ willingness to learn and the amount of effort they ‘invest’ into completing academic tasks and the learning process. In the absence of adequate support from an extended family network or other support services, parental illness can impede all these forms of engagement by causing worry and emotional distress, inattentiveness during lessons, and feelings of isolation or exclusion.
In addition to the implications of role redistribution within the family, parental illness can affect a child’s schooling by reducing the parent’s involvement in the child’s education. Illness can disrupt many aspects of parenting, not least those relating to the child’s school activities (Chen and Fish 2013). One element that makes the family a key determinant of educational attainment is parental involvement. This involvement includes things such as discussing the child’s school activities, monitoring their homework, encouraging educational aspiration and setting grade expectations, school contact, participation in school meetings, and so on. A synthesis of nine meta-analyses (Wilder 2014) showed that a strong and positive relationship between parental involvement and academic achievement is consistently observed, independently of the chosen definitions of parental involvement and achievement.
The degree to which parental illness disrupts parenting and affects the family system depends on the severity of the illness and the burden of disease. Public health practitioners and policy-makers commonly assess the biomedical impact of health problems in terms of quality-adjusted life years and disability-adjusted life years, both of which quantify the number of years lost due to disease (see e.g. Murray et al. 2012). Based on these metrics, non-communicable diseases such as low back pain, headache disorders, depressive disorders, anxiety disorders, and injuries due to falls are among the health problems that cause the most disability (defined as individual suffering multiplied by problem frequency) in Sweden (Institute for Health Metrics and Evaluation 2019). These problems include both bodily (somatic) ailments and psychiatric conditions. Our analysis divides parental illness into two broad categories – psychiatric and somatic illnesses – to estimate how different types of illness affect the probability of ESL.
Other studies using data from countries undergoing economic transitions have also identified negative associations between parental illness and children’s schooling. For example, Alam (2015) showed that in Tanzania, paternal illness reduced children’s school attendance and likelihood of completing primary school because it reduced their household income and hence the ability to pay for schooling. Similarly, in Vietnam (Mendolia et al. 2019), maternal illness was associated with a decrease in children’s likelihood of being enrolled in education, an increase in their likelihood of being in employment, and an increase in their number of weekly working hours. In these studies, and others conducted in non-Western countries (see also Sun and Yao 2010; Woode 2017; Dhanaraj 2016), the loss of household income appears to be the main reason why parental illness affects children’s schooling, and health insurance emerges as a protective factor.
The Swedish context differs in many ways from those in which previous studies were conducted. Social services, such as education, healthcare and childcare, are tax-funded and universal, i.e. available to all citizens. Additionally, there is a state-run social insurance system (managed by the Swedish Social Insurance Agency) whose purpose is to provide financial security in the event of illness, in old age, and for parents of small children by granting monetary benefits including old age pensions and financial support during periods of sickness and parental leave. These benefits are typically not entirely universal, and are more accurately described as being based on wage-labour (Ankarloo 2009), meaning that the amount of compensation one receives depends on one’s previous income. Parents have the right to income compensation when they are sick and unable to work. Because parents continue to receive an income during periods of illness (albeit one that is lower than their usual wage), children are not forced into the labour market to sustain the household’s finances.
In Sweden, the law requires that all children between the ages of 6 and 15/16 receive an education. In contrast to many other countries, both compulsory and higher education are free of fees, supported by a child allowance up to age 16 and then study grants up to age 20. For higher education, there are student grants and a student loan system managed by the Swedish Board of Student Finance. Free school lunches are provided from preschool to the end of upper secondary school. All pupils have access to a school doctor, school nurse, psychologist and school welfare officer at no cost (although access to student health services and the conditions for the staff within these services varies between schools, see e.g. Rosvall and Nilsson 2016). Young people’s schooling is thus, at least in principle, not dependent on the household’s income or ability to pay for it. Additionally, health care (going to a general practitioner or a hospital) is heavily subsidized, with low patient fees and a high-cost ceiling. Therefore, familial health care costs are capped at a low maximum and should not be an obstacle to receiving care, even for low-income families.
2.1 Gender Differences
The effects of parental illness may depend on the genders of both the ill parent and the child. For example, a German study (Barkmann et al. 2007) found that pubertal girls and boys are “under particular strain when the respective same-sex parent has a serious physical illness” (p. 476), possibly because they tend to identify more with the same-sex parent. In the U.S., Johnson and Reynolds (2013) found that the adverse effect of a one-week household hospitalisation on high school and college completion was stronger for male youths. Additionally, Bratti and Mendola (2014) found that maternal illness had a stronger negative effect on children’s school enrolment than did paternal illness. This was explained as a consequence of the study having been conducted in Bosnia and Herzegovina, where mothers generally spend more time (providing non-monetary inputs) with their children than fathers, who are more likely to be the household’s primary earner (providing monetary inputs). Maternal illness thus reduces non-monetary parental inputs (parenting time and quality), and causing a “significant increase in yearly per capita health expenditures at the household level, which is higher for mother’s poor health” (p. 107) than for paternal ill-health. This increases the probability of children leaving school to enter the labour market. Previous studies thus indicate that there is an underlying interaction effect of the genders of the child and the ill parent on child outcomes.
The Swedish state has long sought to promote gender equality, for example by introducing equal parenting policies. Public childcare and parental leave are cornerstones of these policies. The childcare system encompasses preschool, family day nurseries and after-school recreation centres for children to attend while their parents are working or studying. Childcare fees are income-dependent: low-income families pay nothing, and costs are capped for all families (see e.g. Eurydice 2018). Work-family balance is maintained through a flexible parental leave system that entitles parents to 480 days of paid parental leave, 90 days of which are reserved for each parent. Parental insurance benefits can be utilised until the child’s 8th birthday.Footnote 2 This allows both parents to be involved in both the wage labour workforce and parenthood/family life (the dual earner/dual career model).Footnote 3
3 Research Questions
In view of the above, familial economic resources should have a lesser impact on children’s education in Sweden when a child’s parent falls ill than they do in countries without publicly funded schools, comprehensive social insurance, and universal health care with low direct costs. However, children of ill parents are still likely to experience strain and disruptions of the family system. Likewise, while much care work in Sweden is carried out under public auspices, it is likely that parental illness will increase the caregiving responsibilities of young people (Nordenfors and Melander 2016; Nordenfors et al. 2014), which may affect their engagement with their education. Moreover, given Sweden’s high gender equality (see e.g. European Institute for Gender Equality 2019), it is less likely to find any significant difference between the effects of maternal and paternal illness on our outcome of interest (ESL). However, questions about these issues in the Swedish context remain unaddressed. To obtain empirical answers, we posed the following research questions:
-
RQ1: Is parental (psychiatric and somatic) illness associated with young people’s early school leaving from upper secondary education in Sweden?
-
RQ2: When a child’s parent falls ill, how does the interaction between the gender of the ill parent and that of the child affect the probability of early school leaving from upper secondary education?
4 Data and Variables
To address these questions, we analysed micro-level medical and social data from several national population registers obtained via the Umeå SIMSAM Lab data infrastructure (Lindgren et al. 2016).Footnote 4 The study population consisted of the four cohorts of individuals born between 1987 and 1990 (N = 398,748)Footnote 5 who were still alive and residing in Sweden in 2010 (the most recent year of available observations); these individuals are hereafter referred to as index-persons. The longitudinal character of the dataset means that observations are available at different points in time during the index-person’s life, making it possible to include variables from birth onwards in our analyses.
Population-based register data has several methodological advantages. First, access to the total population ensures representativeness and reduces the risk of selection bias due to non-response. Second, the risk of recall-bias and the influence of chance on the detected effects is lower than for survey-based methods because of the large number of observations in the dataset (Olsen 2011; Thygesen and Ersbøll 2014). Third, administrative records often have high completeness and validity (Jensen and Rasmussen 2011; Ludvigsson et al. 2011). Fourth, each individual is assigned a unique and fully anonymised personal identification number (PIN) that links them to family members across registers, making studies among children and parents possible; this is particularly advantageous for studies such as this one. The Regional Ethical Vetting Board in Umeå approved all research based on data from the Umeå SIMSAM Lab, including the present study (Dnr.2010–157-31).
4.1 Dependent Variable
The dependent variable, ESL, is a binary (no/yes) variable taking a value of ‘yes’ only if an index-person did not complete their upper secondary education within four to seven years of graduating from compulsory school.Footnote 6 Upper secondary education in Sweden normally takes three years. Around one in three students requires more than three years to complete their upper secondary education or terminates their upper secondary school studies completely (SKL 2013). Possible reasons for needing more than three years include a study break, a change of study programme, and participating in a one-year preparatory programme before entering an ordinary three-year (‘national’) upper secondary programme – the latter is done by students with incomplete compulsory school grades. In this study, we defined early school leavers as those who did not obtain a full upper secondary qualification within four to seven years of completing their compulsory schooling. This information was obtained from the Swedish National Agency of Education’s Pupil Register.
4.2 Independent Variables
Two indicators were used to characterise parental health. Both were based on parental hospitalisations occurring after the year of the index person’s graduation from compulsory school at the age of 15–16. The first indicator, maternal or paternal psychiatric illness indicates whether the parent had been hospitalised for at least one day due to a main diagnosis of psychiatric disorder (ICD-9: 290–319, ICD-10: F00-F99) (no/yes) at any point during the years after the index person’s compulsory school graduation. Patients with mental illness in Sweden are treated in outpatient care at primary care centres or psychiatric specialist care units (Bergmark et al. 2017). Psychiatric hospitalisations only occur in response to acute events (e.g. suicide attempts) or if the patient’s health status becomes significantly impaired despite outpatient treatment. A day of hospitalisation therefore corresponds to one psychiatric inpatient care event, so this first indicator is sufficient to indicate severe psychiatric illnesses.
The second indicator, maternal or paternal somatic illness indicates whether the relevant parent had been hospitalised for at least 7 days in a single hospitalisation event at any point during the years after the index person’s compulsory school graduation, based on a diagnosis other than a psychiatric disorder (no/yes). For mothers, we excluded hospitalisations due to normal delivery, care in pregnancy, and delivery (ICD-9: 650–659, ICD-10: O00-O99), even if they lasted for more than 7 days. The Swedish Family Care Competence Centre (2019)Footnote 7 has suggested one week of hospitalisation as a cut-off for identifying severe somatic diseases when using Swedish registries (Hjern and Manhica 2013). This operationalisation also gave us an indicator of severe somatic illness that is fairly comparable to that used by Johnson and Reynolds (2013), which was based on a one-week household hospitalisation that mainly included severe somatic diseases (although their data consisted of self-reported questionnaire responses rather than information retrieved from administrative registers). Data on these variables were drawn from the National Patient Register.
4.3 Covariates
Previous studies on childhood health and later life outcomes, including educational achievement, used information on low birth weight as an indicator of poor childhood health, and have repeatedly demonstrated links between low birth weight and lower achievement (Fletcher 2011; Bhutta et al. 2002). We therefore included variables indicating whether the index child was small for their gestational age (no/yes) or malformed (no/yes) to adjust for selection into poor health from birth. Data on these variables were drawn from the Swedish Medical Birth Register.
Index person’s psychiatric illness indicates whether the index child had or had not been hospitalised for at least one night during their lifetime (from their year of birth to the last year of observation) due to a main diagnosis of a psychiatric disorder (ICD-9: 290–319, ICD-10: F00-F99) (no/yes). This indicator was included to adjust for individual health (psychiatric) problems. Data on this variable were drawn from the National Patient Register.
Parents’ education indirectly influences children’s academic achievement because it affects the parents’ educational expectations and parenting behaviours (Davis-Kean 2005). More highly educated parents also spend more basic, educational, and recreational time with their children (Guryan et al. 2008; Dotti Sani and Treas 2016). We therefore used this variable to adjust for variations in family resources. It was operationalised as the highest level of education attained by the parent when the child was 7 years old (the age at which most Swedish children start compulsory school), and indicates the family resources available to the child throughout their schooling. Three levels were defined: (1) compulsory school, (2) two or three years of upper secondary education, and (3) post-secondary education (reference category). Data on this variable were drawn from the Longitudinal Integration Database for Health and Labour Market Studies (LISA).
Family type indicates what type of household the index person lived in during the year in which they graduated from compulsory school at the age of 15–16. It measures whether (1) the child’s biological parents were married/cohabiting, or (2) if the child lived in a single parent household. Data on this variable were drawn from the Total Population Register.
Residential instability indicates whether the index-person had changed their place of residence at least three times between the age of 7 and the end of their compulsory schooling (no/yes). Residential mobility has been linked to ESL (Dyson and Squires 2016), and children who experience multiple and excessive relocations/transitions are at risk of worse educational outcomes. This indicator was included to adjust for previous disruptions in family stability. Data on this variable were drawn from the Total Population Register.
Prior academic achievement is one of the strongest predictors of subsequent achievement (Khattab 2015; Duncan et al. 2007) because low grades are indicative of worse preparation for progress through the educational system (Lyche 2010). This variable is the sum of the index person’s 16 best subject grades during the final year of compulsory schooling (9th grade), when the index persons were 15–16 years old. For each subject, a student is assigned a grade ranging from 0 to 20, where 0 indicates failure. The grade sums thus range from 0 to 320 and indicate the child’s general academic achievement. An overall grade sum of 0 denotes failure in all subjects, while a grade sum of 320 indicates that the child achieved the highest possible grade in all 16 subjects. We standardised this variable into z-scores (mean = 0, standard deviation = 1). Note that this variable measures achievement prior to the occurrence of a parental illness necessitating hospitalisation. Data on this variable were drawn from the Swedish National Agency of Education’s Pupil Register.
5 Analytical Strategy
We exploited the longitudinal character of our dataset and used a quasi-experimental pre-test post-test design in our analyses. Our approach is based on the fact that we have an initial measure of the index persons’ academic achievement (t1) in the ninth grade (the variable prior academic achievement), which represents the final assessment of their educational achievement in (predominantly lower secondary) compulsory school. After the ninth grade, there was a period during which the index persons did (treatment/exposure) or did not (control) have a parent hospitalised due to ill health. The second measurement of achievement (t2) is the subsequent completion or non-completion of upper secondary education (the dependent variable ESL). The pre-test and post-test in our case are not identical measurements because the curricula of lower and upper secondary school are different. However, both the pre-test and post-test measurements of achievement are based on teacher-assigned grades. The measurement at t1 includes unobserved factors that affected school achievement up to that timepoint, including earlier exposures to parental illness that are not explicitly specified in our models. In this way, we isolate the effects of exposure to parental illness requiring hospitalisation between the two academic achievement measurement points, allowing us to obtain ‘uncontaminated’, i.e. less biased, estimates of the effect of exposure.
Due to the binary structure of the dependent variable, logistic regression models were used. To address RQ1, we estimated a series of models, regressing the dependent variable on the indicators of parental illness and adding covariates representing the index person’s health at birth and in later life as well as their sociodemographic and family characteristics, and the grades they achieved in the ninth grade of compulsory school. To address RQ2, we considered the interaction of the parental illness indicators with the index child’s gender.
Effect estimates derived from logistic regressions are typically reported as odds ratios. However, odds ratios can be misleading and may complicate understanding of substantive effects. An alternative is to report marginal effects in terms of differences in probabilities, which can be more informative than odds ratios. It is also problematic to compare odds ratios between models with different covariates due to unobserved heterogeneity (see e.g. Allison 1999; Mood 2010). This is because a change in covariates across models can reflect both effects on the outcome and unobserved heterogeneity, which may differ across groups or models. For these reasons, we present average marginal effects (AME) estimated using Stata’s margins command (Williams 2012). The advantage of marginal effects is that they predict probability changes (note that probabilities can only take values between 0 and 1), which facilitates model interpretation. AME can be interpreted as the average percentage point change in the dependent variable associated with a one-unit increase in the independent variable.
6 Results
To address RQ1, we primarily focus on whether the indicators of parental illness are significantly associated with an increased probability of ESL. Table 1 presents average marginal effects derived from four logistic regression models. Looking at model 1, which includes the maternal and paternal illness indicators and is only adjusted for gender, we see that having had a mother or father hospitalised because of health problems associated with a psychiatric diagnosis increases the probability of ESL by 11.2% and 9.7%, respectively. The first model also show that parental somatic health problems are significantly associated with an increased probability of ESL. However, the increase was smaller than for psychiatric problems (2.9% and 2.5% for mothers and fathers, respectively).
In models 2 to 4, we add covariates to increase model precision. The addition of the selected covariates also acts as a robustness check, enabling us to test the reliability of the estimate obtained using the first model. Since we are mainly interested in the coefficients of the parental illness indicators, the covariates will not be commented on. Under model 2, in which we adjust for the index person’s birth health and later life psychiatric illness, the increase in the probability of ESL due to parental illness becomes smaller – 9.1% and 8.2% for maternal and paternal psychiatric illness, respectively, and 2.5% and 2.2% for maternal and paternal somatic illness, respectively.
In model 3, we adjust for parental education, family type, and residential instability. As expected, the inclusion of these covariates has noticeable effects and attenuates the effects of parental illness. However, parental illness remains significantly associated with the probability of ESL: maternal and paternal psychiatric illness increase the probability of ESL by 4.3% and 3.8%, respectively, while maternal and paternal somatic illness increase it by 1.2% and 0.8%, respectively.
Finally, model 4 includes prior academic achievement. The explanatory power of the model increases by almost 20% when the index person’s grade sum for the final year of compulsory schooling is included, as is indicated by the pseudo r2. Nevertheless, maternal and paternal psychiatric illness are still significantly associated with an increased probability of ESL (2.1% and 1.7% respectively). However, the effects of parental somatic illnesses become non-significant under this model and, the p value aside, the estimate for paternal somatic illness is equal to zero and for maternal illness almost zero (0.4%).
It thus appears that while parental somatic illnesses may cause a shock or temporary disruption of family functioning, its impact is not strong enough to significantly increase the probability of ESL. Conversely, having at least one parent with a diagnosed psychiatric problem does significantly increase the probability of ESL.
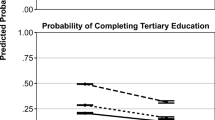
Next, we address RQ2. We present the results of the interaction analyses graphically to facilitate interpretation (the full table with coefficients for both the psychiatric and somatic illness indicators is available in the Appendix Table 3). Figures 1 and 2 illustrate the interaction effect of the ill parent’s gender and the index person’s gender on the index person’s probability of ESL along with marginal effects for a representative range of grade sums (z-score) obtained during the final year of compulsory school. Along the horizontal axis, ten categories of grade sums (z-standardised) are displayed from the lowest on left-hand side to the highest on the right-hand side. The vertical axis shows the probability scale.
Looking at the figures, the probability of ESL seems to be slightly higher when the same sex parent has a psychiatric illness, especially in the case of maternal illness and female index children (Fig. 1). This would at first glance suggest some support for the ‘same-sex hypothesis’; that boys and girls are under particular strain when the respective same-sex parent has an illness. However, this gender gap is small, exists only for certain grade sum ranges, and is less pronounced for more high-performing students. In fact, the figures show that ESL is very strongly dependent on prior academic performance – the most high-performing boys and girls (right-hand side of the figures) have a minimal probability of ESL despite parental illness. Overall, there is no significant interaction effect between the genders of the ill parent and the index child, as demonstrated by the similar slopes in the two figures. In other words, as far as early school leaving from upper secondary education is concerned, there are seemingly no systematic differences in the reactions of boys and girls to parental illness in Sweden, irrespective of the ill parent’s gender.

Average marginal effects of maternal psychiatric illness on the probability of early school leaving by gender (RQ2) and prior academic achievement

Average marginal effects of paternal psychiatric illness on the probability of early school leaving by gender (RQ2) and prior academic achievement
As a sensitivity test, we operationalised the parental somatic illness indicators to include 1 day of hospitalisation, as an alternative to 7 days, to test the effects of less severe somatic illnesses. This increased the number of observations included in the indicators (by approximately 11%) and decreased the average marginal effects (not shown), but the same pattern as presented above remained and does not alter conclusions. We also operationalised the parental illness indicators to include parental hospitalisations during the three preceding years of the index person’s compulsory school graduation (t1). This increased the number of observations included in the indicators by around 1% for each indicator. We then fitted the models described above using the alternatively operationalised indicators. The resulting estimates were not too different from those obtained with the original indicators: the average marginal effects of maternal and paternal illness were reduced by 1% – 1.5% and 0.5%, respectively.
A possible explanation of this decrease due to the inclusion of hospitalisations in the three years preceding t1 is that one hospitalisation may represent either the culmination of a period of illness that has been going on for some time, or something acute that has happened abruptly (a so-called health shock). The hospitalisation itself might be a turning point in terms of health, i.e. a successful treatment leading to an improvement in health status. Thus, if the hospitalisation occurred farther back in time, the family may have recovered due to a successful treatment and re-adjusted from the potentially disrupting event. This may be why the negative effect is reduced by 1.5% – 0.5% if we include observations prior to t1. However, this also implies that we get biased estimates because the baseline measure of achievement, i.e. our pre-test (t1), is affected by prior health events.
7 Discussion
This study examined the relationship between having a parent with ill health and young people’s education. Specifically, we studied the effects of having a parent with health problems on the probability of leaving upper secondary school prior to completion in Sweden, and potential gender differences in these effects. The results show that having had a parent with psychiatric, but not somatic, health problems necessitating hospitalisation after completing compulsory school is associated with an increased probability of leaving upper secondary education.
Interestingly, the effects of parental somatic illness were not significant. One way to view this finding is in the light of Sweden’s institutional welfare system, which appears to protect against some of the adverse effects that parental illness can have on children’s schooling in other national contexts (e.g. Boardman et al. 2012; Johnson and Reynolds 2013; Mendolia et al. 2019). This is particularly striking when considering the similarity of the illness indicators and education outcomes used in this study to those used by Johnson and Reynolds (2013) in a study conducted in the U.S. They used a one-week household hospitalisation as their illness indicator, which is similar to our indicator of somatic illness (hospitalisation for at least 7 days based on a diagnosis other than a psychiatric disorder). Additionally, they used the probabilities of graduating from high school, of attending college, and of graduating from college as outcome measures, all of which are comparable to the outcome measure used in this current study. While they found that a week-long household hospitalisation during the respondent’s adolescence was associated with lower likelihoods of completing high school and attending college, our results indicate that no comparable effect exists in the Swedish context.
However, it is equally notable that the effects of parental psychiatric illness persisted, for both mothers and fathers, even after adjusting for individual health, sociodemographic factors, and children’s prior academic achievement. The existence of this effect in Sweden means that the magnitude of these effects may be even more pronounced in regions lacking similar systems. To understand the difference in effects of parental somatic and psychiatric illnesses on the probability of ESL, one must relate the findings not only to the institutional context but also to the difference in the burden of the health problems imposed by the two types of illness. While it is possible to maintain a functional degree of parenting and involvement in the education of one’s children’s while suffering from some somatic illnesses (Chen and Fish 2012), psychiatric illnesses cause a greater degree of functional disability in comparison to somatic disorders (Linden et al. 2015) and interfere with the fulfilment of complex daily duties and participation across all areas of life. Moreover, processes of parentification are more common when parents have mental illnesses (Loch 2016), and it can be particularly burdensome for a child or adolescent to supervise and emotionally support a parent with mental illness.
Since we only estimated the effects of a parental hospitalisation after the end of the index child’s compulsory schooling (and thus excluded parental hospitalisations during the child’s compulsory school years), we probably excluded cases involving parents having chronic illnesses of longer duration. However, this also strengthens the interpretation of our results that aligns with our discussion on the equilibrium of the family system, i.e. the argument that family stability is greatly disrupted by parental psychiatric illnesses that either arise suddenly or increase in severity to a degree necessitating in-hospital care. This disruption necessitates effort (due to reorganisation of family roles) that consumes the psychosocial resources of both the child and other family members. The child may reallocate time away from school work to fulfil their new family role, reducing their school engagement. While this mechanism was not formally tested here, it is supported by evidence from a recent study (Hamilton and Redmond 2019) that specifically measured school engagement and found that young carers of family members with mental illnesses had significantly lower school engagement than non-carers.
Unlike previous studies, which showed that maternal and paternal illness have different effects on the educational outcomes of girls and boys (Johnson and Reynolds 2013; Mendolia et al. 2019; Bratti and Mendola 2014), we found no significant gender-specific interaction effects. Proposed reasons for the gender differences observed in previous studies have essentially revolved around gender roles. Young females are socialised to assume a caregiver role to a greater extent than young males (Mendolia et al. 2019), who, are more likely to assume the breadwinner role (particularly if they are the oldest in a sibling group) and thus increase their labour market participation (Johnson and Reynolds 2013). Sweden is in many regards a comparatively gender equal country (European Institute for Gender Equality 2019), which may be one explanation for the null difference between boys and girls.
The impact of the parent’s gender in certain national contexts may reflect the fact that the mother and father may provide different inputs to the family household, roughly divided into monetary (the father traditionally being the breadwinner) and non-monetary (the mother spending more time with the children). The loss of these inputs due to illness might have different effects on children’s education depending on the institutional context. (see e.g., Bratti and Mendola 2014 for the case of Bosnia and Herzegovina; cf. Alam 2015 for Tanzania). One contributing factor to Sweden’s high gender equality is its dual earner and dual carer policies, which encourage both parents to both participate in the labour market and care for the household (although women still perform the lion’s share of housework) (European Institute for Gender Equality 2019). Although maternal psychiatric illness was associated with a very slightly (0.4%) higher probability of ESL than paternal psychiatric illness in the fully adjusted model, the results presented here indicate that the health of both mothers and fathers are equally important for both boys’ and girls’ education in Sweden.
7.1 Strengths and Limitations
This is the first investigation into the effects of poor parental health on the probability of early school leaving from upper secondary school in a Scandinavian country. As such, it constitutes a novel contribution to both the literature on how parental health affects the educational attainment of young people and that on children at risk of poor educational outcomes (for example, Hasselhorn et al. 2014). Most of the existing studies on this topic are based on self-reported health data, which may be affected by reporting bias and measurement error due to differences in individual reference points (Johnson and Reynolds 2013). This current study exploited a somewhat more objective measure of health, namely administrative medical records of hospital admissions, which results exclusively from detrimental accidents or severe health problems. Furthermore, in contrast to self-reported grades (as in e.g. Sieh et al. 2013; Boardman et al. 2012), which are less valid measures of school performance (Kuncel et al. 2005), the educational measures used in this study are based on teacher assigned grades from the Swedish National Agency of Education’s Pupil Register. Because our findings are based on data from total population registers, they have high generalisability and may be applicable to countries with health and education systems similar to Sweden’s.
One drawback of relying on registry data stems from the inability to determine which biological parent’s household the index child lives in if their biological parents are divorced. This means that our estimates of the effects of parental illness may be downwardly biased for families with divorced parents where the biological parents share physical custody. Because if negative effects such as those reported here are prevalent for children who do not live in the same household as the ill parent, the effects for a child who does live with an ill parent would be even more pronounced. Another limitation is that the parental illness indicators used in this study are crude and binary. The psychiatric illness indicator included conditions such as substance use along with mental disorders such as depression, generalised anxiety disorders, schizoaffective disorders, psychotic conditions and many others. Therefore, our conclusions relate to illness as a broad concept. Differentiating between specific causes of hospitalisation would have revealed condition-specific effects but was unfortunately unfeasible due to data limitations. Furthermore, the duration and severity of parental illness is of significance and the lack of a chronicity indicator is a limitation.
It is also important to bear in mind that ESL is a complex phenomenon whose determinants include individual characteristics, education systems and wider social and economic conditions as well as familial issues (Dyson and Squires 2016). This study focused only on family-related factors. Similarly, families are complex entities, and each parent and child will have unique relationships with one-another and with networks of others. We were unable to study things such as family cohesion and parent-child interactions. Nor did we consider the potential influence of grandparents, who could mitigate detrimental effects associated with parental illness, or siblings, who could act either as sources of support or as resource ‘diluters’ (see Skog 2019). These issues could be explored in future studies.
7.2 Implications
This paper highlights the academic vulnerability of young people whose parents have health problems necessitating hospitalisation. The educational consequences for these young people can be as far-reaching as leaving school before completing an upper secondary qualification. This is particularly the case for young people whose parent(s) have a mental illness. It is important to connect vulnerable families with great care needs to community resources who can properly support them. Family interventions provided by psychiatric and social care services (e.g. Afzelius 2017) can be one way to support these children and their families. Internet-based support for children with parents having mental illness is also available (Ali 2013; Stjernswärd 2009; Elf 2013); its purpose is to relieve guilt and shame, facilitate sharing of experiences with others in similar situations, and allow knowledge to be gained.
In terms of policy, a provision of the Swedish Health and Medical Service Act introduced in 2010 obliges healthcare professionals who treat adult patients to also consider children’s needs for advice and support when a parent is receiving care for a serious illness. Instead of exclusively focusing on parents and working from an individual-centred perspective, practitioners must be mindful of the adjustment difficulties facing children, which necessitates a family-oriented perspective. This provision may facilitate efforts to identify young carers and connect families with great care needs to community resources. However, for this to be a functional part of a sustainable support system, structures enabling co-operation between the healthcare sector, social services, and schools are required.
Every Swedish school provides access to student health services, which by law are obliged to support students’ development and health so that they can cope effectively in school. The student health services are responsible for investigating the difficulties and barriers that may prevent a child from achieving the goals laid out in the curriculum. Within these services, a school doctor, school nurse, counsellors and special tutors may work together to set up a plan in cases where (for example) a child or adolescent has missed time in school due to a situation at home. They can ensure that the child gets more time to catch up or not have to take tests during certain periods. It is important to raise awareness of the existing young carers among school personnel – for example, by using instruments designed for this specific purpose (Joseph et al. 2009) – to ensure they receive adequate support in their ongoing education.
Notes
These authors find a negative association between having an ill parent and school performance (evaluated on the basis of teacher-assigned school grades) at the end of compulsory school (age 15–16).
If a child is born 2014 or later (not applicable to individuals in this study), parental benefits can be utilised up to and including the day the child turns 12 years old or finishes grade 5 in compulsory school.
The Swedish labour market is however gender segregated in terms of the occupations and positions held by men and women. Gender inequality with respect to education and income persists: women perform better at all levels of education but have lower incomes and positions in the labour market (Statistics Sweden 2018; Korpi et al. 2013).
The national registers from which data were drawn are listed in Table 2 of the Appendix.
This includes only the cases with information (i.e. no missing) on all the selected variables presented below.
Our operationalisation of ESL is based on two observation points: (1) the year of graduation from compulsory school and (2) the year of graduation from upper secondary school. An individual for whom the former was recorded but not the latter was classified as ESL. Since we only had observations up to 2010, the 1990 cohort, most of whom graduated from compulsory school in 2006, had to complete their upper secondary education within four years to avoid being classified as ESL. Likewise, most members of the 1989, 1988, and 1987 cohorts graduated from compulsory school in 2005, 2004, and 2003, respectively, and thus had to complete their upper secondary education within five, six, and seven years, respectively, to avoid being classified as ESL.
In operationalising our dependent variable, we excluded cases with missing academic grade information for the ninth grade of compulsory schooling ( n=48,110). These cases include individuals who (a) received schooling at a special education facility, (b) were foreign-born and immigrated to Sweden (in some cases unaccompanied, so no link to parents was available) at an older age and therefore had not yet completed compulsory schooling, (c) had emigrated abroad with their families and then migrated back into Sweden (4337 individuals had no recorded comprehensive school grades but did complete their upper secondary education within the time-period for which we have observations), or (d) dropped out of school before ninth grade. The latter cases are a separate group of early school leavers, but are outside the scope of this study.
The Swedish Family Care Competence Centre is a national platform commissioned by the National Board of Health and Welfare via the Ministry of Health and Social Affairs to provide expert support to municipalities (who organise the public social services), county councils (responsible for the public health care sector) and private health and care providers. They engage in work that includes all carers regardless of age, disease, diagnosis or disability.
References
Afzelius, M. (2017). Families with parental mental illness. Faculty of Health and Society, Malmö University, Doctoral Dissertation, Malmö.
Alam, S. A. (2015). Parental health shocks, child labor and the educational outcomes: evidence from Tanzania. Journal of Health Economics, 44, 161–175.
Aldridge, J. (2008). All work and no play? Understanding the needs of children with caring responsibilities. Children and Society, 22(4), 253–264.
Aldridge, J., & Becker, S. (2003). Children caring for parents with mental illness: Perspectives of young carers. Parents and professionals. Bristol: The Policy Press.
Ali, L. (2013). Caring situation and provision of web-based support for young persons who support family members or close friends with mental illness. Institute of Health & Care Sciences, University of Gothenburg, Doctoral dissertation, Gothenburg.
Allison, P. D. (1999). Comparing logit and probit coefficients across groups. Sociological Methods and Research, 28(2), 186–208.
Ankarloo, D. (2009). The Swedish welfare model. Counter-arguments to neoliberal myths and assertions. Paper prepared for association of heterodox conference economics conference, London 2009, p, 1–7.
Appleton, J. J., Christenson, S. L., Kim, D., & Reschly, A. L. (2006). Measuring cognitive psychological engagement: validation of the student engagement instrument. Journal of School Psychology, 44(5), 427–445.
Asen, K. (1985). Illness and the family. Journal of the Royal Society of Medicine, 8(78), 21–25.
Barkmann, C., Romer, G., Watson, M., & Schulte-Markwort, M. (2007). Parental physical illness as a risk for psychosocial maladjustment in children and adolescents: epidemiological findings from a national survey in Germany. Psychosomatics, 48(6), 476–481.
Bergmark, M., Bejerholm, U., & Markström, U. (2017). Policy changes in community mental health: Interventions and strategies used in Sweden over 20 years. Social Policy & Administration, 51(1), 95–113.
Bhutta, A., Cleves, M. A., Casey, P. H., & Anand, K. (2002). Cognitive and behavioural outcomes of school-aged children who were born preterm: a meta analysis. JAMA, The Journal of the Medical Association, 288(6), 728–737.
Boardman, J. D., Alexander, K. B., Miech, R. A., MacMillan, R., & Shanahan, M. J. (2012). The association between parent’s health and the educational attainment of their children. Social Science & Medicine, 75, 932–939.
Bratti, M., & Mendola, M. (2014). Parental health and child schooling. Journal of Health Economics, 35, 94–108.
Champaloux, S. W., & Young, D. R. (2015). Childhood chronic health conditions and educational attainment: a social ecological approach. Journal of Adolescent Health, 56(1), 98–105.
Charles, G., Stainton, T., & Marshall, S. (2009). Young carers: mature before their time. Reclaiming Children and Youth, 18(2), 28–41.
Chen, C. Y.-C. (2014). Exploration of the short-term and long-term effects of parental illness on children’s educational and behavioral functioning using a large Taiwanese sample. Western Journal of Nursing Research, 36(5), 664–684.
Chen, C. Y.-C. (2016). Educational functioning of children of parents with chronic physical illness: a systematic review. School Psychology International, 37(6), 606–626.
Chen, C. Y.-C. (2017). Effects of parental chronic illness on children’s psychological and educational functioning: a literature review. Contemporary School Psychology, 21(2), 166–176.
Chen, C. Y.-C., & Fish, M. C. (2012). Parental involvement of mothers with chronic illness and children’s academic achievement. Journal of Family Issues, 34(5), 583–606.
Chen, C. Y.-C., & Fish, M. C. (2013). Demands of maternal chronic illness and children’s educational functioning: an exploratory study. Child and Adolescent Social Work Journal, 30(3), 257–274.
Davis-Kean, P. E. (2005). The influence of parent education and family income on child achievement: the indirect role of parental expectations and the home environment. Journal of Family Psychology, 19(2), 294–304.
Dhanaraj, S. (2016). Effects of parental health shocks on children’s schooling: evidence from Andhra Pradesh, India. International Journal of Educational Development, 49, 115–125.
Dotti Sani, G. M., & Treas, J. (2016). Educational gradients in parents’ child-care time across countries, 1965-2012. Journal of Marriage and Family, 78(4), 1083–1096.
Duncan, G. J., Dowsett, C. J., Claessens, A., Magnuson, K., Huston, A. C., Klebanov, P., Pagani, L. S., Feinstein, L., Engel, M., Brooks-Gunn, J., Sexton, H., Duckworth, K., & Japel, C. (2007). School readiness and later achievement. Developmental Psychology, 43(6), 1428–1446.
Dyson, A. & Squires, G. (Eds.) (2016). European Agency for Special Needs and Inclusive Education. (2016). Early school leaving and learners with disabilities and/or special educational needs: a review of the research evidence focusing on Europe. Odense, Denmark.
Elf, M. (2013). User involvement in designing a web-based support system for young carers- inspiring views and systematic barriers. Department of Psychology, University of Gothenburg, Gothenburg.
European Institute for Gender Equality (2019). Gender Equality Index 2019: Sweden.
Eurydice. (2018). Sweden. Organisation of pre-primary education (preschool). Retrieved from https://eacea.ec.europa.eu/national-policies/eurydice/content/organisation-programmes-pre-primary-education-1_en
Fletcher, J. M. (2011). The medium term schooling and health effects of low birth weight: evidence from siblings. Economics of Education Review, 30(3), 517–527.
Forrest, C. B., Bevans, K. B., Riley, A. W., Crespo, R., & Louis, T. A. (2011). Health and school outcomes during children’s transition into adolescence. Journal of Adolescent Health, 52(2), 186–194.
Fredricks, J. A., Blumenfield, P. C., & Paris, A. H. (2004). School engagement: potential of the concept, state of the evidence. Review of Educational Research, 74(1), 59–109.
Guryan, J., Hurst, E., & Kearney, M. (2008). Parental educational and parental time with children. Journal of Economics Perspectives, 22(3), 23–46.
Hamilton, M., & Redmond, G. (2019). Are young carers less engaged in school than non-carers? Evidence from a representative Australian study. Child Indicators Research, 1–17.
Harstone, A., & Charles, G. (2012). Children of parents with mental illness: young carers, coping and transition into adulthood. Relational Child and Youth Care Practice, 25(2), 14–26.
Hasselhorn, M., Andresen, S., Becker, B., Betz, T., Leuzinger-Bohleber, M., & Schmid, J. (2014). Children at risk of poor educational outcomes: theoretical concepts and empirical results. Child Indicators Research, 7, 695–697.
Hjern, A., & Manhica, H. (2013). Barn som anhöriga till patienter i vården - hur många är de? [Children as next of kin for patients in care - how many are they?]. Nationellt kompetenscentrum anhöriga, skrift 2013:1 [the Swedish family care competence Centre, SFCCC, report 2013:1]. Nka, Linnéuniversitetet, CHESS.
Hjern, A., Berg, L., Rostila, M., & Vinnerljung, B. (2013). Barn som anhöriga: Hur går det i skolan? Rapport 3 från projektet barn som anhöriga [Children that are carers: How does it go for them in school? Report 3 from the project children next to kin] Nationellt kompetenscentrum anhöriga, skrift 2013:3 [The Swedish family care competence Centre, SFCCC, report 2013:3]. Nka, Linnéuniversitetet, CHESS.
Institute of Health Metrics and Evaluation. (2019). Healthdata, Sweden. Retrieved from: http://www.healthdata.org/sweden.
Jensen, V. M., & Rasmussen, A. W. (2011). Danish education registers. Scandinavian Journal of Public Health, 39(7_suppl), 91–94.
Johnson, E., & Reynolds, C. L. (2013). The effect of household hospitalizations on the educational attainment of youth. Economics of Education Review, 37, 165–182.
Joseph, S., Becker, S., Becker, F., & Regel, S. (2009). Assessment of caring and its effects in young people: development of the multidimensional assessment of caring activities checklist (MACA-YC18) and the positive and negative outcomes of caring questionnaire (PANOC-YC20) for young carers. Child: Care, Health and Development, 35(4), 510–520.
Khattab, N. (2015). Students’ aspirations, expectations and school achievement: what really matters? British Educational Research Journal, 41(5), 731–748.
Korpi, W., Ferrarini, T., & Englund, S. (2013). Women’s opportunities under different family policy constellations: gender, class, and inequality tradeoffs in western countries re-examined. Social Politics: International Studies in Gender, State & Society, 20(1), 1–40.
Kuncel, N. R., Credé, M., & Thomas, L. L. (2005). The validity of self-reported grade point averages, class ranks, and test scores: a meta-analysis and review of the literature. Review of Educational Research, 75(1), 63–82.
Lee, J.-S. (2014). The relationship between student engagement and academic performance: is it a myth or reality? The Journal of Educational Research, 107(3), 177–185.
Linden, M., Linden, U., & Schwantes, U. (2015). Disability and functional burden of disease because of mental in comparison to somatic disorders in general practice patients. European Psychiatry, 30(6), 789–792.
Lindgren, U., Nilsson, K., de Luna, X., & Ivarsson, A. (2016). Data resource profile: Swedish microdata research from childhood into lifelong health and welfare (Umeå SIMSAM Lab). International Journal of Epidemiology, 45(4), 1075–1075g.
Loch, U. (2016). The family as a place of education. Between a school-centred focus on education and family needs. CEPS Journal, 6(4), 93–113.
Ludvigsson, J. F., Andersson, E., Ekbom, A., Feychting, M., Kim, J. L., Reuterwall, C., et al. (2011). External review and validation of the Swedish national inpatient register. BMC Public Health, 11(1), 450.
Lyche, C. (2010). Taking on the completion challenge: A literature review on policies to prevent dropout and early school leaving. OECD Education Working Papers, No. 53, OECD, Paris.
Maslow, G. R., Haydon, A., McRee, A.-L., Ford, C. A., & Halpern, C. T. (2011). Growing up with a chronic illness: social success, educational/vocational distress. Journal of Adolescent Health, 49(2), 206–212.
Mendolia, S., Nguyen, N., & Yerokhin, O. (2019). The impact of parental illness on children’s schooling and labour force participation: evidence from Vietnam. Review of Economics of the Household, 17(2), 469–492.
Moffat, A. K., & Redmond, G. (2016). Is having a family member with health concerns bad for young people’s health? Cross-sectional evidence from a national survey of young Australians. BMJ Open, 7(1), e013946.
Mood, C. (2010). Logistic regression: why we cannot do what we think we can do, and what we can do about it. European Sociological Review, 26(1), 67–82.
Murray, C. J., Vos, T., Lozano, R., Naghavi, M., Flaxman, A. D., Michaud, C., et al. (2012). Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet, 380(9859), 2197–2223.
Nordenfors, M., & Melander, C. (2016). Barn och unga som utövar omsorg [Children and youths who care for a relative]. In Nka Barn som anhöriga 2016:6. Kalmar: Nka, Linnéuniversitetet.
Nordenfors, M., Melander, C., & Daneback, K. (2014). Unga omsorgsgivare i Sverige [Young carers in Sweden]. In Nka Barn som anhöriga 2014:5. Kalmar: Nka, Linnéuniversitetet.
OECD. (2012). Equity and quality in education: Supporting disadvantaged students and schools. OECD: Publishing.
Olsen, J. (2011). Register-based research: some methodological considerations. Scandinavian Journal of Public Health, 39(3), 225–229.
Pakenham, K. I., & Cox, S. (2014). The effects of parental illness and other ill family members on the adjustment of children. Annals of Behavioral Medicine, 48(3), 424–437.
Pedersen, S., & Revenson, T. A. (2005). Parental illness family functioning and adolescent well-being: a family ecology framework to guide research. Journal of Family Psychology, 19(3), 404–409.
Rolland, J. S. (1999). Parental illness and disability: a family system framework. Journal of Family Therapy, 21(3), 242–266.
Rosvall, P.-Å., & Nilsson, S. (2016). Challenges of engagement with health services in Sweden’s schools: listening to the views of school nurses and students with recurrent pain. Pastoral Care in Education, 34(1), 3–12.
Sieh, D. S., Meijer, A. M., Oort, F. J., Visser-Meily, J. M. A., & Van der Leij, D. A. V. (2010). Problem behaviour in children of chronically ill parents: a meta-analysis. Clinical Child and Family Psychology Review, 13(4), 384–397.
Sieh, D. S., Visser-Meily, J. M. A., & Meijer, A. M. (2013). Differential outcomes of adolescents with chronically ill and healthy parents. Journal of Child and Family Studies, 22(2), 209–218.
Skinner, E. A., & Pitzer, J. R. (2012). Developmental dynamics of student engagement, coping and everyday resilience. In S. L. Christenson, A. L. Reschly, & C. Wylie (Eds.), Handbook of Student Engagement (pp. 21–44). New York: Springer.
SKL, Sveriges Kommuner och Landsting [Swedish Association of Local Authorities and Regions]. (2013). Preventing early school leaving. The Challenge of Making Sure That All Students Complete Their Upper Secondary Education.
Skog, F. (2019). Sibling effects on adult earnings among poor and wealthy children evidence from Sweden. Child Indicators Research, 12, 917–942.
Smyth, C., Cass, B., & Hill, T. (2011). Children and young people as active agents in care-giving: agency and constraint. Children and Youth Services Review, 33(4), 509–514.
Statistics Sweden (2018). Women and men in Sweden, facts and figures 2018. Örebro.
Stjernswärd, S. (2009). Designing online support for families living with depression. Faculty of Health & Society, Malmo University: Malmo.
Sun, A., & Yao, Y. (2010). Health shocks and children’s school attainments in rural China. Economics of Education Review, 29, 375–382.
Tarabini, A., Curran, M., Montes, A., & Parcerisa, L. (2018). Can educational engagement prevent early school leaving? Unpacking the school’s effect on educational success. Educational Studies, 45(2), 226–241.
The Swedish Family Care Competence Centre (2019). The Swedish family care competence Centre. URL: http://www.anhoriga.se/information-in-english.
Thygesen, L. C., & Ersbøll, A. K. (2014). When the entire population is the sample: strengths and limitations in register-based epidemiology. European Journal of Epidemiology, 29(8), 551–558.
Warren, J. (2007). Young carers: conventional or exaggerated levels of involvement in domestic and caring tasks? Children and Society, 21(2), 136–146.
Wihstutz, A. (2011). Working vulnerability: agency of caring children and children’s rights. Childhood, 18(2), 447–459.
Wilder, S. (2014). Effects of parental involvement on academic achievement: a meta-synthesis. Educational Review, 66(3), 377–397.
Williams, R. (2012). Using the margins command to estimate and interpret adjusted predictions and marginal effects. The Stata Journal, 12(2), 308–331.
Winton, C. A. (2003). Children as caregivers: Parental and parentified children. London: Allyn and Bacon.
Wittenberg, E., & Prosser, L. A. (2013). Disutility of illness for caregivers and families: a systematic review of the literature. Pharmacoeconomics, 31(6), 489–500.
Wittenberg, E., Saada, A., & Prosser, L. A. (2014). How illness affects family members: a qualitative interview survey. Patient, 6(4), 257–268.
Woode, M. E. (2017). Parental health shocks and schooling: The impact of mutual health insurance in Rwanda. Social Science & Medicine, 173, 35–47.
Acknowledgements
The Umeå SIMSAM Lab data infrastructure used in this study was developed with support from the Swedish Research Council and strategic funds from Umeå University. The authors are grateful to Veronica Lövgren at the Umeå Centre for Disability Research for valuable comments and suggestions. Comments from seminar participants at the annual Meeting of the Network for Research on Social Policy and Welfare in Gothenburg 2019 are also appreciated.
Funding
Open access funding provided by Umea University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bortes, C., Strandh, M. & Nilsson, K. Parental Illness and Young People’s Education. Child Ind Res 13, 2069–2091 (2020). https://doi.org/10.1007/s12187-020-09731-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12187-020-09731-x