
Abstract
Emotion regulation and/or obesity have been linked to compassion, self-criticism and ‘dark’ personality traits but the relationship between these factors is unclear as most research has focused on the big five personality traits. Here, we investigated the influence of dark personality traits on emotional dysregulation, compassion and BMI. 300 participants completed measures of emotion dysregulation, compassion, self-criticism and dark tetrad personality traits; also providing their BMI. MLR revealed psychopathy, high self-criticism and low compassion ‘for self’ predicted poor emotion regulation; accounting for > 50% of the variance. Whilst their effects on BMI were also significant, no factors singularly predicted BMI. Our research offers important insights into the complexity of factors that may contribute to poor emotion regulation. Of novel value, we found a link between self-compassion, self-criticism and emotion regulation; with self-criticism emerging as the biggest predictor of emotion dysregulation of all explored variables. Although implications for obesity are limited, it is notable that our population demonstrated less obesity than the general public. This is important, as it ascertains that emotion dysregulation, self-criticism, low self-compassion and dark personality traits are not associated with BMI in those of healthy weight.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Emotion regulation is critical in how individuals respond to stress and control emotion (Ayers & DeVisser, 2017). Typically, this requires an awareness of, and ability to effectively cope with or tolerate emotions. When an individual lacks the skills required to control negative affect, this is termed emotion dysregulation (Stepp et al., 2014). Emotion dysregulation has been associated with disordered eating such as binge eating disorder (Bray et al., 2023), anorexia nervosa (Haynos & Fruzzetti, 2011), bulimia nervosa (Hayaki, 2009), and the development of food addiction (Gearhardt et al., 2012). Changes to eating habits in response to negative emotions can increase the risk of obesity as some people who experience stressful situations are more likely to eat high-sugar and/or high-fat food (Hill et al., 2021). Such individuals may also demonstrate increased food intake during periods of emotional arousal, or increased stress, as a coping response to the stressor - again predisposing them to weight-gain (Hill et al., 2021).
Identifying the causal pathway of emotional regulation in obesity is complex given the range of inter-personal and intra-personal factors known to contribute to obesity risk. Negative emotions and unhealthy emotion processing are factors that could explain some of the mechanisms that perpetuate morbid obesity (Zjilstra et al., 2012). Research has found that women who are overweight/obese have more difficulty with emotional regulation than women from the general population. Emotion regulation difficulties include problems identifying emotions (e.g. alexithymia) and increased suppression of emotions; with higher negative affect and difficulty identifying feelings positively correlated with disordered emotional eating (Guerrini-Usubini et al., 2023). To explain these observed associations between emotions and food intake, a number of theories have been developed. For example, the escape from self-awareness theory (Heatherton & Baumeister, 1991) suggests that individuals overeat after experiencing negative affect that they cannot appropriately regulate. Typically, those who binge eat display exceptionally high standards and are particularly sensitive to the opinions of others. Such eating behaviour is a reaction to negative self-awareness, characterised by emotional distress and concern over how an individual feels they are being perceived by their peers. In order to escape/quell this unpleasant state, the individual may turn their attention away from the immediate environment and onto food. Thus, binge eating may offer a welcome distraction from the original source of stress, allowing the individual to avoid dealing with potentially ego-threatening information (e.g. Heatherton & Baumeister, 1991).
Whilst there have been attempts to understand the role of emotion regulation and dysregulation in obesity and weight loss treatment outcomes, results of individual studies are varied (Teixeira et al., 2005) and highlight the need for future exploration to understand the complexities of this area (e.g. Maratos & Sharpe, 2018). In addition, greater exploration of adaptive strategies for coping with negative affect is needed. To expand, if binge eating or overeating are maladaptive coping strategies for dealing with negative affect, then what are adaptive coping strategies for dealing with negative affect? And would such adaptive coping strategies negatively correlate with emotion dysregulation and obesity? One such emotion regulation strategy, with a burgeoning evidence base, is self-compassion.
One’s ability to be self-compassionate (see Kirby et al., 2017 for review) has received much attention as an adaptive emotion regulation strategy/trait. Self-compassion is the term used to describe a caring, empathic and non-judgemental attitude towards the self, especially when faced with negative or stressful situations (Gilbert et al., 2011). Research reveals that self-compassion is associated with greater positive affect, life satisfaction, happiness and coping (Maratos & Sheffield;, 2020). Importantly, it is hypothesised that the primary mechanism by which self-compassion protects against psychopathology is through effective emotion regulation. Specifically, high levels of self-compassion are positively associated with the use of adaptive regulatory strategies such as problem solving, cognitive reappraisal and emotional acceptance (e.g. Paucsik et al., 2022). As such, self-compassion may aid emotion regulation (and negative affect coping) by creating an accepting, non-judgemental context via which a stressful situation or event is viewed or evaluated (Maratos et al., 2019).
Alongside improved emotional functioning, compassion has been associated with reduced body dissatisfaction, disordered eating and body weight shame (Braun et al., 2016; Carter et al., 2021). Body dissatisfaction is a common factor linked to both weight gain and poor weight maintenance (Lazzeretti et al., 2015). Thus, increased levels of compassion may act as a buffer against obesity and eating disorders. It is suggested that elevated levels of self-compassion may impact positively on body image by encouraging kindness toward oneself. This directly contradicts the notion of body dissatisfaction, where criticising one’s body is the focus (Lazzeretti et al., 2015). Findings indicate that self-compassion could offer a protective factor against disordered eating by encouraging acceptance and non-judgement of a situation or event - whether this relates to acceptance of negative affect or acceptance of a physical body and/or its imagery (Braun et al., 2016; Carter et al., 2021). However, there is still limited research exploring the role of compassion in relation to obesity.
Aside from self-compassion, it is hypothesised that individuals also possess dispositions related to their ability to be compassionate towards others, and to accept compassion from others. Compassion for others is the motivation to help and empathise with others and is linked to a range of physical and mental health benefits (e.g. Jinpa, 2015). Compassion from others refers to our experience and ability (or openness) to accept compassion from others (Gilbert et al., 2017). However, research examining the roles of compassion towards others and acceptance of compassion from others with respect to adaptive coping is limited. Additionally, to the authors’ knowledge, no such research has explored these further factors of compassion in relation to obesity and weight-gain. Yet, self-criticism, which can be conceptualised as an inverse of the compassion triad (i.e. self-compassion, compassion to others and compassion from others) is a key vulnerability in mental illness and weight-gain (Duarte et al., 2017).
To expand, individuals with high levels of self-criticism demonstrate negative self-judgement directed to personal attributes such as their physical appearance, personality and intellect as well as perceptions related to their external behaviour, inner thoughts and emotions (e.g. Duarte et al., 2014; Duarte et al., 2017). Thus, individuals who are highly self-critical are more likely to feel overwhelmed by particularly negative/aversive social situations and feel ill-equipped to cope with adverse or stressful events (Gilbert et al., 2011). In the context of eating, Duarte et al. (2017) have observed that self-criticism was correlated with negative affect and related to eating regulation and weight control. However, this research was conducted with a population participating in a weight-management programme, and the potential influence of personality factors on negative affect was not acknowledged. That is, the buffering effects of the compassion triad were not explored, nor were further personality traits linked to effective and/or maladaptive emotion regulation.
Historically, effective emotion regulation is associated with extraversion, whereas maladaptive emotion regulation is linked to neuroticism (Chen et al., 2023). More recently, self-compassion has been found to show positive relationships with extraversion, openness to experience, agreeableness, and conscientiousness (Oral & Arslan, 2017), although its relationship with neuroticism is debated (see for example Pfattheicher et al., 2017). Often, neuroticism is seen as a ‘negative’ personality trait which implies that the ‘darker’ aspects of personality may be connected to emotion regulation. ‘Dark’ personality traits are not simply an inverse of positive personality traits, but are an underlying ‘dark core’ from which the elements of the dark triad or tetrad of personality emerge (Volmer et al., 2019).
The Dark Triad of personality involves three aspects of personality; narcissism, Machiavellianism, and psychopathy (Paulhus & Williams, 2002). This has recently been extended to incorporate sadism, and is now known as the Dark Tetrad of personality (Chabrol et al., 2015). Of the dark triad (or tetrad), psychopathy has been associated with a variety of maladaptive regulatory techniques including the non-acceptance of emotional responses, impulse control problems and reduced emotional clarity (Pollock et al., 2016). Moreover, whilst narcissism has been traditionally linked to negative or undesirable traits, it is apparent that moderate narcissism has a positive effect on mental health (e.g. increased happiness, lower anxiety and depression: Sedikides et al., 2004). Thus, the extent to which a ‘degree’ of narcissism may offer protection against emotional eating, binge eating and obesity warrants further investigation. Certainly, to gain an understanding of factors related (or otherwise) to negative affect in the context of obesity, greater exploration of all dark tetrad factors alongside those related to positive affect and compassion would be beneficial.
Thus, the purpose of the present research was two-fold, including a fuller exploration of the following theoretical concepts; emotion regulation and dysregulation, compassion, and personality as well as an exploration of these factors in relation to obesity. This is the first study to apply dark personality traits to this area of research and the first to develop a model using these variables. Specifically, we set out to investigate: (i) the influence of compassion, self-criticism and the dark tetrad personality traits in relation to emotional regulation and dysregulation; and (ii) if these factors correlate with an individual’s Body Mass Index (BMI). BMI is a universally recognised measure used to categorise a person as underweight, normal weight, overweight or obese based on tissue mass (i.e. weight) and height. BMI is also considered the gold standard measurement and has been utilised in previous research exploring associations between emotion dysregulation and weight gain (e.g. Jones et al., 2019). By exploring these variables in the context of obesity, we can further develop theoretical insights relating to emotional regulation. Although previous research has examined the big five personality traits, this study will go further and investigate dark personality traits and how they link to regulation strategies; an area under-explored in current research which has potential implications for our understanding of relevant coping strategies. This could be useful for healthcare professionals to consider in terms of how it would contribute to adaptive or maladaptive behaviour in the treatment and prevention of obesity.
Method
Participants
Participants (N = 300) were recruited using opportunity sampling, with an incentive of entry into a prize draw to win one of four £50 Amazon vouchers. Recruitment took place face-to-face (on campus at the University of Derby and at weight loss groups) and online (via social media, including Twitter, Facebook and Reddit, and through Weight Loss forums). All but one participant provided their gender; the sample included 68 males (22.7%) and 228 females (76.0%), while two participants (0.7%) self-described as non-binary and one (0.3%) as genderqueer. Participants’ ages ranged from 18 to 68 years (mean = 29.12, SD = 11.31). Most participants (N = 223, 74.3%) were students, with 10 (3.3%) unemployed, 1 (0.3%) retired and the other 66 (22.0%) employed in a variety of occupations. Most participants were from the United Kingdom (N = 210, 70.0%), with 25 (8.3%) from other European countries, 19 (6.3%) from North America, 6 (2.0%) from Oceania, 2 (0.7%) from Asia, and 1 (0.3%) from Africa; the remaining 35 participants did not provided their nationality. Most participants (N = 275, 91.7%) were white, 7 (2.3%) were Asian, 10 (3.3%) were of mixed ethnicity and 6 (2.0%) were of other ethnic groups, while two participants did not provide their ethnicity. The number of participants was determined based on the effect sizes reported in Duarte et al. (2014) to achieve ∝ = 0.05 and > 80% power (Cohen, 1988). Ethical approval for the study was granted by the University of Derby Research Ethics Committee.
Design and materials
The study used a correlational design, examining relationships between a series of variablesFootnote 1. Qualtrics online survey software (www.qualtrics.com) was used to obtain a measure of these variables through a series of questions and psychometric scales, as follows:
Demographics and BMI
In addition to basic demographic information (gender, age, nationality, ethnicity, and occupation), participants were asked to self-report their height and weight, in either imperial or metric units. This data were used by the researchers to calculate BMI. Generally, BMI scores above 25 kg/m2 indicate individuals who are overweight and are thus at a greater risk of developing a wide range of health problems (Di Angelantonio et al., 2016).
Emotional regulation: difficulties in emotion regulation scale – 16 Item Version (DERS-16)
The DERS-16 (Bjureberg et al., 2016) is a shortened version of the original 36-item DERS (Gratz & Roemer, 2004), containing 16 items measured on a five-point Likert scale. It comprises items relating to lack of emotional clarity (e.g. “I am confused about how I feel”), difficulties engaging in goal-directed behaviour (e.g. “When I am upset, I have difficulty getting work done”), impulse control difficulties (e.g. “When I am upset, I become out of control”), limited access to effective emotional regulation strategies (e.g. “When I am upset, I believe there is nothing I can do to make myself feel better”), and nonacceptance of emotional responses (e.g. “When I am upset, I feel ashamed with myself for feeling that way”). The scale demonstrates excellent internal reliability (α = 0.92 − 0.95) and good convergent validity (Bjureberg et al., 2016).
Compassion: compassionate Engagement and actions scale (CEAS)
The CEAS (Gilbert et al., 2017) is a set of three 10-item scales that assess three different measures of compassion: (1) the compassion we experience for others; (2) the compassion we experience from others; and (3) self-compassion. These are each further divided into “engagement” (6 items) and “action” (4 items) subscales, using a 10-point Likert scale response format from never-always. Engagement items include “I notice and am sensitive to distress in others when it arises”, while action items include “I take the actions and do the things that will be helpful to others”. The scales show good internal reliability (α = 0.72 − 0.94) and convergent validity (Gilbert et al., 2017).
Self-criticism and Self-Reassurance: forms of Self-Criticising/Attacking & self- reassuring scale (FSCRS)
The FSCRS (Gilbert et al., 2004) contains 22 items, measured on a five-point Likert scale. The scale comprises three subscales, termed “inadequate self” (9 items, e.g. “I think I deserve my self-criticism), “reassured self” (8 items, e.g. “I am gentle and supportive with myself”), and “hated self” (5 items, e.g. “I have a sense of disgust with myself”). The subscales show good internal reliability, with α = .90 for inadequate self and α = .86 for reassured self and hated self (Gilbert et al., 2004).
Machiavellianism: MACH-IV
The MACH-IV scale (Christie & Geis, 1970) consists of 20 items, measured on a five-point Likert scale. The scale comprises three subscales: 9 items assess Tactics, (e.g. “It is wise to flatter important people”), 9 items assess Views, (e.g. “It is hard to get ahead without cutting corners here and there”), and 2 items assess Morality (e.g. “All in all, it is better to be humble and honest than to be important and dishonest”, reverse scored). The MACH-IV has demonstrated good internal reliability (α = 0.82), construct validity and criterion validity (Rauthmann, 2012).
Narcissism: narcissistic personality Inventory-13 (NPI-13)
The NPI-13 (Gentile et al., 2013) is a shortened 13-item version of the original 40-item NPI (Raskin & Terry, 1988). Each item consists of a pair of contrasting statements, and participants must select the one with which they most agree; one point is scored for each selected statement that indicates narcissism. The scale comprises three subscales: 4 items assess Leadership/Authority, (e.g. “I like having authority over other people/I don’t mind following orders”), 5 items assess Grandiose Exhibitionism, (e.g. “I try not to be a show off/I will usually show off if I get the chance), and 4 items assess Entitlement/Exploitativeness (e.g. “I expect a great deal from other people/I like to do things for other people”). The scale demonstrates good convergent validity, discriminant validity and overall reliability (α = .82; Gentile et al., 2013).
Psychopathy: Levenson Self-Report psychopathy scale (LSRP)
The LSRP (Levenson et al., 1995) consists of 26 items, measured on a five-point Likert scale. The scale comprises two subscales: 16 items assess primary psychopathy (e.g. “For me, what’s right is whatever I can get away with”) and 10 items assess secondary psychopathy. (e.g. “Before I do anything, I carefully consider the possible consequences”, reverse scored). The primary psychopathy scale demonstrates good overall reliability (α = 0.82), while the secondary psychopathy scale demonstrating acceptable reliability (α = 0.63; Levenson et al., 1995).
Sadism: Assessment of sadistic personality (ASP)
The ASP (Plouffe et al., 2017) contains 20 items, measured on a seven-point Likert scale. The scale contains 6 items relating to subjugation, (e.g. “I have made fun of people so that they know I am in control”), 8 items relating to pleasure-seeking, (e.g. “I enjoy humiliating others”), and 6 items relating to a lack of empathy. (e.g. “I have tormented others without feeling remorse”). The scale demonstrates good convergent validity and excellent internal reliability (α = 0.96; Plouffe et al., 2017).
Procedure
Interested participants were directed to the online survey. This began by detailing the nature of the study and participants’ rights to anonymity and withdrawal, before requesting their informed consent. Participants then completed the questions relating to demographics and their height and weight, before the remaining scales were presented in a randomised order (and with forced responding). Participants were able to complete these at their own pace. A debrief was then provided, giving more information on the study and reminding participants of their right to withdraw their data.
Results
Descriptives
For means, SD’s, correlations and z score ranges for the variables: BMI, emotion dysregulation, Machiavellianism, narcissism, psychopathy, sadism, self-criticism, compassion for others, compassion from others, compassion for self, see Table 1. For frequencies of participants in each BMI category see Table 2.
Investigation 1: The influence of compassion, self-criticism and the dark tetrad personality traits in relation to emotional regulation and dysregulation
The z scores (Table 1) indicated that there were outliers in the data, however, Cooks Distance had a maximum of 0.11. Being < 1 indicated that these potential outliers were not problematic (Field, 2013). Also, no correlations were > 0.8, with Durbin Watson being 1.94 indicating that auto correlation had not occurred, and the VIF scores ranged from 1.37 to 3.12 indicating that multicollinearity was not present. Therefore the data were analysed using Multiple Regression with the Enter Method. The predictor variables were compassion for others, compassion from others, compassion for self, self-criticism, Machiavellianism, narcissism, psychopathy and sadism, and the outcome variable was emotion dysregulation. In this case, the regression produced a large effect size (R2 = 0.56, R2adj = 0.55). The model was significant (F (8, 291) = 46.97, p < .001) and accounted for 55% of the variance. Significant predictors were: psychopathy (β = 0.21, p < .001), self-criticism (β = 0.49, p < .001), and compassion for self (β = − 0.38, p < .001).
Investigation 2: The influence of compassion, self-criticism, the dark tetrad personality traits and emotion dysregulation on BMI
A further Multiple Regression again using the Enter Method was carried out with compassion for others, compassion from others, compassion for self, self-criticism, Machiavellianism, narcissism, psychopathy, sadism and emotion regulation entered as predictor variables, and BMI as the outcome variable. The regression produced a small effect size (R2 = 0.04, R2adj = 0.01) indicating the model accounted for 1% of the variance. However, emotion regulation, Machiavellianism, narcissism, psychopathy, sadism, self-criticism, compassion for others, compassion from others, and compassion for self were not significant predictors of BMI (F (9, 290) = 1.30, p = .236).
Supplementary analyses
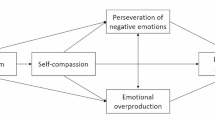
Due to the correlations between some of the variables and our first aim of investigating the influence of self-compassion, self-criticism and the dark tetrad personality traits in relation to emotional regulation and dysregulation, an exploratory SEM model was proposed. Based on the results of the Multiple Regression analyses, BMI was excluded from the proposed model. The following latent variables were constructed using the observed variables shown in Fig. 1: emotion dysregulation, personality, self-criticism, compassion for others and compassion for self. The following model had the best fit to the data: emotion dysregulation predicting self-criticism, and high scores on the dark tetrad and self-criticism predicting lower compassion for self. Also the dark tetrad was found to predict lower levels of compassion for others; although compassion from others was not significantly predicted by any latent variable (see Fig. 1). Various fit indices for the model were measured, with one being close to the threshold (NFI ≥ 0.95) and the rest being beyond the thresholds (RMSEA ≤ 0.06, TLI ≥ 0.95 and SRMR ≤ 0.08 and CFI ≥ 0.95) (Hu & Bentler, 1999). The fit indices for the model are as follows: Χ2 = 226.14, df = 108, p < .001, RMSEA = 0.06, SRMR = 0.05, CFI = 0.96, TLI = 0.95, NFI = 0.93.

SEM Showing Emotion Dysregulation Predicting Self-Criticism, Self-Criticism Predicting Compassion for Self and the Dark Tetrad Personality Traits Predicting Compassion for Others
Discussion
The aim of the present research was two-fold and included a fuller exploration of the factors relating to emotion regulation and dysregulation, as well as exploration of these factors in relation to obesity. In relation to the first aim, psychopathy, high self-criticism and low compassion for self all significantly predicted poor emotion regulation, accounting for over 50% of the variance observed. Supplementary SEM analyses further revealed a significant association between emotion dysregulation and self-criticism. This model further highlighted key differences between the factors associated with compassion for self and those influencing compassion for others. In relation to the second aim, it was found that whilst a significant model emerged, no factors were found to singularly predict BMI and the variance explained was limited (i.e. 1%). Results will now be discussed in turn.
Firstly, findings revealed that self-criticism was the biggest predictor of emotion regulation. Specifically, participants who reported higher levels of self-criticism were found to experience greater difficulties with emotion regulation. The association between emotion regulation deficits and high self-criticism aligns with previous research in the area (e.g. Gilbert et al., 2011), and adds to the idea that self-critics are more likely to engage in maladaptive regulation strategies in order to cope with negative affect. The current findings suggest that in a general population, self-criticism is associated with poor emotion regulation. Examining ways to reduce self-criticism should therefore be an important target for future research. As previously discussed, self-criticism plays a key role in the development of mental illness and is often associated with a variety of potentially destructive behaviours and/or weight gain (Duarte et al., 2017). Thus, it might be the case that high self-criticism increases the likelihood of an individual using ineffective regulation strategies in order to cope with stress or negative emotion. Therefore, health professionals need to consider the role of self-criticism and how it may contribute to potential maladaptive behaviour (e.g. which could include binge eating; Serpell et al., 2020) in those who struggle to regulate negative emotional experiences.
Findings further revealed that self-compassion was a significant predictor of emotion regulation. In the current sample, those reporting low levels of self-compassion were more likely to experience difficulties regulating emotional experience. This finding is supported by previous research demonstrating that compassion to self is associated with the use of more adaptive emotion regulation strategies such as problem solving, cognitive reappraisal and the acceptance of negative emotion (e.g. Paucsik et al., 2022). In this way, self-compassion is thought to help individuals cope with aversive emotions or situations by cultivating feelings of self-acceptance and non-judgement (Maratos et al., 2019). These findings reiterate the importance of self-compassion for successful emotional functioning. Individuals who struggle to regulate their emotional experiences are more likely to develop a variety of mental health problems including problematic eating behaviours (Bray et al., 2023). Potentially, self-compassion works to provide a protective ‘buffer’ by changing the way individuals view negative emotion and experiences (see for example Maratos et al., 2019). However, more qualitative research is needed both in the general population and with healthcare providers to explore this further.
Findings of the first analysis also revealed that psychopathy was predictive of poor emotion regulation. Specifically, those displaying psychopathic personality traits were more likely to experience difficulties with emotion regulation. The link between personality and emotion dysregulation is supported by previous findings, which have shown that dark personality traits are associated with poor emotion regulation including a lack of impulse control and non-acceptance of negative emotion (e.g. Pollock et al., 2016). Given the limited research in this area, these findings add to current understanding of the personality factors that may affect emotion regulation and dysregulation. From the current study, it is suggested that psychopathic traits may increase the likelihood that individuals will choose poor or maladaptive emotion regulatory strategies. As a result, those who display high levels of psychopathy may turn to maladaptive or ineffective regulatory strategies when faced with emotional difficulties. However, further research is needed to explore whether those displaying psychopathic traits can learn to improve their emotion regulation skills. For example, examining whether an empathic and non-judgemental attitude towards the self can be fostered in those with high levels of psychopathy. Tentatively, self-compassion could provide some protection among individuals who might be more at risk of poor emotion dysregulation due to psychopathy and, as such, is suggested as a future research direction.
Supplementary SEM analyses also provided evidence for the role of compassion, self-criticism and personality in emotion regulation. Specifically, in the model generated, difficulties regulating emotion were significantly associated with self-criticism. This aligns with our findings from the main analysis and provides further support for the link between poor emotion regulation and high levels of self-criticism. Here, future research should aim to examine the causal direction of this relationship and whether high self-criticism leads to poor emotion regulation (as previously suggested (Duarte et al., 2017; Gilbert et al., 2011) or whether difficulties regulating emotional experience leads an individual to become more self-critical as a result (as observed in the SEM). Given that self-criticism confers high vulnerability to a whole host of psychological and physical disorders (Kannan & Levitt, 2013), understanding whether it stems from poor emotion regulation or, alternatively, leads to poor emotion regulation could be crucial to informing therapeutic practices. For example, whether to focus on addressing self-criticism specifically, or emotion regulation more broadly.
Findings from the supplementary analysis also help to further our understanding of compassion by highlighting a clear distinction between the factors associated with compassion for self and those influencing compassion for others. Results demonstrated that a combination of dark personality traits, emotion dysregulation and high self-criticism was predictive of low levels of self-compassion. However, emotion dysregulation and high self-criticism did not appear to have any influence on compassion for others. Rather, compassion for others appeared to be influenced by the presence of dark personality traits, with darker traits predicting lower levels of compassion for others. This finding is important as it is the first to demonstrate that factors implicated in the ability to have compassion for others may differ from those implicated in the ability to have compassion for ones self. Indeed, this can explain why some individuals are able to act compassionately towards other people, yet lack the ability to show compassion towards themselves. This is also consistent with anecdotal reports of those in compassion-focused therapy or partaking in compassionate mind training often stating that they ‘do not deserve’ self-compassion.
In relation to the second aim of this study, which sought to investigate the influence of emotion regulation, compassion, self-criticism and the dark tetrad personality traits on BMI, none of the former factors emerged as significant predictors of obesity. Indeed, emotion dysregulation was not predictive of BMI in the current study. This could suggest that emotion regulation is not a factor implicated in unhealthy eating behaviours. However, this seems unlikely given that emotion dysregulation has previously been associated with a range of problematic eating behaviours including binge eating disorder, anorexia nervosa, bulimia nervosa and obesity (e.g. Guerrini-Usubini et al., 2023; Haynos & Fruzzetti, 2011, Hayaki, 2009). Added to this, Serpell et al. (2020) have shown that therapeutic strategies for cultivating self-compassion are associated with improved food-related self-regulation in the context of negative mood. Thus, it is surprising that we found no relationship between emotion regulation, nor compassion and BMI.
One explanation for the above null results is, that by and large, our participants were healthy. Previous findings have demonstrated that as many as 64% of UK adults are overweight or obese (NHS, 2017). However, in this study only 40.9% of participants were classified as overweight or obese suggesting that we may have inadvertently recruited a lower percentage of overweight/obese people than in the general population; despite efforts to target a range of populations. In addition, almost three quarters of our sample were undergraduate students which limits the generality and ecological validity of our findings. As a result, individuals in the current sample may not be representative of a general overweight or obese population, nor be struggling with their weight and as such, did not demonstrate the expected psychological factors associated with increased vulnerability. Whilst individuals attending weight-loss groups/forums (e.g. slimming world, weight watchers) were approached to take part in the current study, a limitation of our research is that we did not actively code for participants drawn from weight-loss groups/forums versus elsewhere. Importantly, many of these groups facilitate the development of skills to help regulate emotions in order to lose weight. Therefore, it might be the case that those who engage with these groups are already being encouraged to use adaptive regulatory strategies such as problem solving or even self-compassion (Slimming World, n.d., Weight Watchers, n.d.). As such, future research should ensure such information is captured to fully inform analyses.
In conclusion, although the implications of the current study findings for obesity are limited, our research does offer important theoretical insights into the complexity of intrapersonal factors that may lead to poor emotional functioning in a general population. To expand, the findings of this study provide novel support for the link between self-compassion, self-criticism and emotion regulation. Indeed, our results suggest that self-criticism is the biggest predictor of emotion dysregulation and additionally highlights a clear distinction between factors associated with compassion for self and those influencing compassion for others. This research is important as it evidences that self-compassion and compassion for others can not only be clearly delineated, but are also associated with different personality facets. Finally, although our data do not support a relationship between obesity, emotion regulation, compassion, self-criticism and the dark tetrad, it is notable that our population demonstrated less obesity (i.e. lower BMI) than the general public at large. Therefore, what can be ascertained is that in a generally healthy population emotion dysregulation, self-criticism, low self-compassion and the dark personality traits are not associated with BMI.
Data availability
The datasets generated during and/or analysed during the current study are available in the UDORA repository, https://repository.derby.ac.uk/item/9224w/exploring-the-role-of-compassion-self-criticism-and-the-dark-triad-on-obesity-and-emotion-regulation.
Notes
The authors did not preregister this research in an independent institutional registry.
References
Ayers, S., & DeVisser, R. (2017). Psychology for medicine and healthcare. SAGE.
Bjureberg, J., Ljótsson, B., Tull, M. T., Hedman, E., Sahlin, H., Lundh, L. G., Bjärehed, J., DiLillo, D., Messman-Moore, T., Gumpert, C. H., & Gratz, K. L. (2016). Development and validation of a brief version of the difficulties in emotion regulation scale: The DERS-16. Journal of Psychopathology and Behavioural Assessment, 38(2), 284–296. https://doi.org/10.1007/s10862-015-9514-x.
Braun, T. D., Park, C. L., & Gorin, A. (2016). Self-compassion, body image, and disordered eating: A review of the literature. Body Image, 17, 117–131. https://doi.org/10.1016/j.bodyim.2016.03.003.
Bray, B., Sadowski, A., Bray, C., Bradley, R., & Zwickey, H. (2023). Clinical aspects of binge eating disorder: A cross-sectional mixed-methods study of binge eating disorder experts’ perspectives. Frontiers in Psychiatry, 13. https://doi.org/10.3389/fpsyt.2022.1087165.
Carter, A., Gilbert, P., & Kirby, J. N. (2021). A systematic review of compassion-based interventions for individuals struggling with body weight shame. Psychology and Health, 38, 94–124. https://doi.org/10.1080/08870446.2021.1955118.
Chabrol, H., Melioli, T., Van Leeuwen, N., Rodgers, R., & Goutaudier, N. (2015). The dark tetrad: Identifying personality profiles in high-school students. Personality and Individual Differences, 83, 97–101. https://doi.org/10.1016/j.paid.2015.03.051.
Chen, L., Liu, X., Weng, X., Huang, M., Weng, Y., Zeng, H., Li, Y., Zheng, D., & Chen, C. (2023). The emotion regulation mechanism in neurotic individuals: The potential role of mindfulness and cognitive bias. International Journal of Environmental Research and Public Health, 20(2), 896. https://doi.org/10.3390/ijerph20020896.
Christie, R., & Geis, F. (1970). Studies in Machiavellianism. Academic Press.
Cohen, J. (1988). Statistical Power Analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum Associates, Publishers.
Di Angelantonio, et al. (2016). Body-mass index and all-cause mortality: Individual-participant-data-analysis of 239 prospective studies in four continents. The Lancet, 388(10046), 776–786. https://doi.org/10.1016/S0140-6736(16)30175-1.
Duarte, C., Matos, M., Stubbs, J., Gale, C., Morris, L., Gouveia, P., J., & Gilbert, P. (2017). The impact of shame, self-criticism and social rank on eating behaviours in overweight and obese women participating in a weight management programme. Plos One, 12(1), e0167571. https://doi.org/10.1371/journal.pone.0167571.
Duarte, C., Pinto-Gouveia, J., & Ferreira, C. (2014). Escaping from body image shame and harsh self-criticism: Exploration of underlying mechanisms of binge eating. Eating Behaviors, 15(4), 638–643. https://doi.org/10.1016/j.eatbeh.2014.08.025.
Field, A. (2013). Discovering statistics using IBM SPSS statistics. SAGE.
Gearhardt, A. N., White, M. A., Masheb, R. M., Morgan, P. T., Crosby, R. D., & Grilo, C. M. (2012). An examination of the food addiction construct in obese patients with binge eating disorder. International Journal of Eating Disorders, 45(5), 657–663. https://doi.org/10.1002/eat.20957.
Gentile, B., Miller, J. D., Hoffman, B. J., Reidy, D. E., Zeichner, A., & Campbell, W. K. (2013). A test of two brief measures of grandiose narcissism: The narcissistic personality inventory (NPI)-13 and NPI-16. Psychological Assessment, 25(4), 1120–1136. https://doi.org/10.1037/a0033192.
Gilbert, P., Catarino, F., Duarte, C., Matos, M., Kolts, R., Stubbs, J., Ceresatto, L., Duarte, J., Pinto-Gouveia, J., & Basran, J. (2017). The development of compassionate engagement and action scales for self and others. Journal of Compassionate Health Care, 4(4). https://doi.org/10.1186/s40639-017-0033-3.
Gilbert, P., Clarke, M., Hempel, S., Miles, J. N. V., & Irons, C. (2004). Criticizing and reassuring oneself: An exploration of forms style and reasons in female students. British Journal of Clinical Psychology, 43, 31–50. https://doi.org/10.1348/014466504772812959.
Gilbert, P., McEwan, K., Matos, M., & Rivis, A. (2011). Fears of compassion: Development of three self-report measures. Psychology and Psychotherapy, 84, 239–255. https://doi.org/10.1348/147608310X526511.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. https://doi.org/10.1023/B:JOBA.0000007455.08539.94.
Guerrini-Usubini, A., Cattivelli, R., Scarpa, A., Musetti, A., Varallo, G., Franceshini, C., & Castelnuovo, G. (2023). The interplay between emotion dysregulation, psychological distress, emotional eating, and weight status: A path model. International Journal of Clinical and Health Psychology, 23(1). https://doi.org/10.1016/j.ijchp.2022.100338.
Hayaki, J. (2009). Negative reinforcement eating expectancies, emotion dysregulation, and symptoms of bulimia nervosa. International Journal of Eating Disorders, 42(6), 552–556. https://doi.org/10.1002/eat.20646.
Haynos, A. F., & Fruzzetti, A. E. (2011). Anorexia Nervosa as a disorder of emotion dysregulation: Evidence and treatment implications. Clinical Psychology: Science and Practice, 18(3), 183–202. https://doi.org/10.1111/j.1468-2850.2011.01250.x.
Heatherton, T., & Baumeister, R. (1991). Binge eating as Escape from self-awareness. Psychological Bulletin, 110(1), 86–108. https://doi.org/10.1037/0033-2909.110.1.86.
Hill, D., Conner, M., Clancy, F., Moss, R., Wilding, S., Bristow, M., & O’Conner, D. B. (2021). Stress and eating behaviours in healthy adults: A systematic review and meta-analysis. Health Psychology Review, 16(2), 280–304. https://doi.org/10.1080/17437199.2021.1923406.
Jinpa, T. (2015). A fearless heart: Why compassion is the key to greater wellbeing. Piatkus.
Jones, J., Kauffman, B., Rosenfield, D., Smits, J. A. J., & Zvolensky, M. J. (2019). Emotion dysregulation and body mass index: The explanatory role of emotional eating among adult smokers. Eating Behaviors, 33, 97–101. https://doi.org/10.1016/j.eatbeh.2019.05.003.
Kannan, D., & Levitt, H. M. (2013). A review of client self-criticism in psychotherapy. Journal of Psychotherapy Integration, 23(2), 166–178. https://doi.org/10.1037/a0032355.
Kirby, J. N., Tellegen, C. L., & Steindl, S. R. (2017). A meta-analysis of compassion-based interventions: Current state of knowledge and future directions. Behavior Therapy, 48(6), 778–792. https://doi.org/10.1016/j.beth.2017.06.003.
Lazzeretti, L., Rotella, F., Pala, L., & Rotella, C. M. (2015). Assessment of psychological predictors of weight loss: How and what for? World Journal of Psychiatry, 5(1), 56–67. https://doi.org/10.5498/wjp.v5.i1.56.
Levenson, M. R., Kiehl, K. A., & Fitzpatrick, C. M. (1995). Assessing psychopathic attributes in a noninstitutionalized population. Journal of Personlaituy & Social Psychology, 68(1), 151–158. https://doi.org/10.1037//0022-3514.68.1.151.
Maratos, F. A., Montague, J., Ashra, H., Welford, M., Wood, W., Barnes, C., Sheffield, D., & Gilbert, P. (2019). Evaluation of a compassionate mind training intervention with school teachers and support staff. Mindfulness, 12, 2245–2258. https://doi.org/10.1007/s12671-019-01185-9.
Maratos, F. A., & Sheffield, D. (2020). Brief Compassion-focused imagery dampens physiological Pain responses. Mindfulness. https://doi.org/10.1007/s12671-020-01485-5.
Maratos, F., & Sharpe, E. E. (2018). The origins of disordered eating and childhood food neophobia: Applying an anxiety perspective. In S. Reilly (Ed.), Food neophobia: Behavioral and biological influences (pp. 305–328). Elsevier.
NHS (2017). Health Survey for England. Retrieved March 2020 from https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2017.
Oral, T., & Arslan, C. (2017). The investigation of university students’ forgiveness levels in terms of self-compassion, rumination and personality traits. Universal Journal of Educational Research, 5(9), 1447–1456. https://doi.org/10.13189/ujer.2017.050902.
Paucsik, M., Nardelli, C., Bortolon, C., Shankland, R., Leys, C., & Baeyens, C. (2022). Self-compassion and emotion regulation: Testing a mediation model. Cognition and Emotion, 37, 49–61. https://doi.org/10.1080/02699931.2022.2143328.
Paulhus, D. L., & Williams, K. M. (2002). The Dark Triad of personality: Narcissism, Machiavellianism and psychopathy. Journal of Research in Personality, 36(6), 556–563. https://doi.org/10.1016/S0092-6566(02)00505-6.
Pfattheicher, S., Geiger, M., Hartung, J., Weiss, S., & Schindler, S. (2017). Old wine in new bottles? The case of self-compassion and neuroticism. European Journal of Personality, 31(2). https://doi.org/10.1002/per.2097.
Plouffe, R. A., Saklofske, D. H., & Smith, M. M. (2017). The assessment of sadistic personality: Preliminary psychometric evidence for a new measure. Personality and Individual Differences, 104, 166–171. https://doi.org/10.1016/j.paid.2016.07.043.
Pollock, N. C., McCabe, G. A., Southard, A. C., & Zeigler-Hill, V. (2016). Pathological personality traits and emotion regulation difficulties. Personality and Individual Differences, 95, 168–177. https://doi.org/10.1016/j.paid.2016.02.049.
Raskin, R., & Terry, H. (1988). A principal-components analysis of the narcissistic personality inventory and further evidence of its construct validity. Journal of Personality and Social Psychology, 54(5), 890–902. https://doi.org/10.1037/0022-3514.54.5.890.
Rauthmann, J. F. (2012). The Dark Triad and interpersonal perception: Similarities and differences in the social consequences of narcissism, Machiavellianism, and psychopathy. Social Psychological and Personality Science, 3(4), 487–496. https://doi.org/10.1177/1948550611427608.
Sedikides, C., Rudich, E. A., Gregg, A. P., Kumashiro, M., & Rusbult, C. (2004). Are normal narcissists psychologically healthy? Self-esteem matters. Journal of Personality and Social Psychology, 87(3), 400–416. https://doi.org/10.1037/0022-3514.87.3.400.
Serpell, L., Amey, R., & Kamboj, S. K. (2020). The role of self-compassion and self-criticism in binge eating behaviour. Appetite, 1(144), 104470. https://doi.org/10.1016/j.appet.2019.104470.
Slimming World. (n.d.). Facilitating behavioural change IMAGE therapy. Retrieved (March 2020). from https://www.slimmingworld.co.uk/health/how-sw-works/behavioural-change.aspx.
Stepp, S. D., Whalen, D. J., Scott, L. N., Zalewski, M., Loeber, R., & Hipwell, A. E. (2014). Reciprocal effects of parenting and borderline personality disorder symptoms in adolescent girls. Development & Psychopathology, 20, 1–18. https://doi.org/10.1017/s0954579413001041.
Teixeira, P. J., Going, S. B., Sardinha, L. B., & Lohman, T. G. (2005). A review of psychosocial pre-treatmant predictors of weight control. Obesity Review, 6, 43–65. https://doi.org/10.1111/j.1467-789X.2005.00166.x.
Volmer, J., Koch, I. K., & Wolff, C. (2019). Illuminating the ‘dark core’: Mapping global versus specific sources of variance across multiple measures of the dark triad. Personality and Individual Differences, 145, 97–102. https://doi.org/10.1016/j.paid.2019.03.024.
Weight, & Watchers (n.d.). Be your own best friend. Retrived March 2020 from https://www.weightwatchers.com/uk/article/be-your-own-best-friend.
Zijlstra, H., van Middendorp, H., Devaere, L., Larsen, J. K., van Ramshorst, B., & Geenen, R. (2012). Emotion processing and regulation in women with morbid obesity who apply for bariatric Surgery. Psychology & Health, 27(12), 1375–1387. https://doi.org/10.1080/08870446.2011.600761.
Author information
Authors and Affiliations
Contributions
Emma E Sharpe: Conceptualisation, Writing – Original Draft, Review & Editing, Visualisation. Malcolm Schofield: Methodology, Software, Formal analysis. Ben L. H. Roberts: Methodology, Software. Atiya Kamal: Writing – Review & Editing. Frances A. Maratos: Supervision, Writing – Review & Editing.
Corresponding author
Ethics declarations
Statement and declarations
This work was supported by funding from the University of Derby’s Early Career Research Grant. The authors have no other competing/conflicting interests to declare that are relevant to the content of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sharpe, E.E., Schofield, M.B., Roberts, B.L.H. et al. Exploring the role of compassion, self-criticism and the dark triad on obesity and emotion regulation. Curr Psychol 43, 11972–11982 (2024). https://doi.org/10.1007/s12144-023-05319-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-05319-0