
Abstract
Early childhood is a critical period for cognitive development and the emergence of attention deficit hyperactivity disorder. Therefore, many researchers have explored the relationship between executive function and attention deficit hyperactivity disorder (ADHD) in young children. However, the findings have been inconsistent. This study used a cross-lagged survey to clarify the interaction between executive function and ADHD in early childhood as well as explore the trends of the same. Data were collected using questionnaires distributed to 376 parents of children aged 4–6 years in October 2018 (Time 1) and June 2019 (Time 2), with components including the Child Executive Functioning Scale (Parent Version) and Child Difficulty and Strengths Scale (Parent Version), and the mean age of the children surveyed at Time 1 was 58.96 ± 11.94 months. Results indicate that executive function and attention deficit hyperactivity disorder were stable, with significant positive and secondary positive correlations between executive function and attention deficit hyperactivity disorder. The cross-lagged regression analysis showed that the inhibition of executive function components at Time 1 predicted the attention deficit hyperactivity disorder at Time 2. Finally, the cross-lagged regression analysis showed that attention deficit hyperactivity disorder at Time 1 significantly predicted the inhibition at Time 2. There was a strong relationship between inhibition and attention deficit hyperactivity disorder in the sample, with some reciprocal causality. The findings indicate the urgent need for early screening and intervention in cognitive and behavioral disorders.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Executive function (EF) refers to an individual’s ability to use thinking skills to achieve goals, develop problem-solving methods, and monitor and adjust their behaviors. It is a higher-level processing activity in the brain. In addition, it is the process by which individuals exercise conscious control over their thoughts and actions (Beck et al., 2011). EF development is particularly important in childhood to establish a foundation for better living and learning in the future (Best & Miller, 2010). Indeed, various studies have shown that it can both immediately affect learning and behavioral problems in children (Diamond & Lee, 2011; Kim et al., 2013) and predict outcomes such as health, wealth, and delinquency in adulthood (age 32 in the specific study; Moffitt et al., 2011).
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder dominated by attention deficit, hyperactivity, and impulsivity (APA, 2013). It typically develops in the preschool years, is most often identified during school age, and can persist into adolescence and adulthood (Thapar & Cooper, 2016). The global prevalence of the disease is 3.4% in children under 18 years of age (Polanczyk et al., 2015), with a detection rate of 6.26% in Chinese children (Thomas et al., 2015). ADHD has gained increasing attention because of its high co-morbidity and high risk (Singh et al., 2015). In addition, numerous studies have demonstrated executive function deficits in school-aged children as well as in the adult ADHD population (Barkley, 1997; Neely et al., 2016), but the relationship between executive function and ADHD in preschool children is controversial (Espy et al., 2011) and warrants further exploration.
The Relationship Between EF and ADHD
Some researchers have suggested that preschool is a critical period for developing executive function. Furthermore, executive function deficits predict later ADHD symptoms (Barkley, 1997). For example, a study by Brocki et al. (2010) found that executive function at age 5 significantly predicted ADHD symptoms at age 7. A study by Bohlin et al. (2012) further showed that inhibitory control at age 5 predicted ADHD symptoms at age 7. The predictive role of executive function in preschoolers for later ADHD symptoms was also demonstrated by Sjöwall et al. (2017) in a 13-year follow-up study of preschoolers. However, some researchers have argued that early executive function does not predict later ADHD symptoms in children. For example, Rajendran et al. (2015) found that executive function did not significantly predict ADHD symptoms in school-aged children in a 6-year follow-up study of children aged 3–4 years. Whether EF is predictive of ADHD remains to be further explored.
In addition to longitudinal studies between the two, more researchers have conducted comparative studies of EF performance in children with ADHD from a cross-sectional perspective. Mahone and Hoffman (2007) conducted an EF experiment with 25 pairs of age-, sex-, and socioeconomically matched preschool children with ADHD and a normal group, finding that those with ADHD had impaired EF in all factors and dimensions by comparison. However, some studies have found inconsistent results. Schoemaker et al. (2012) found that children with preschool ADHD were impaired only in inhibitory abilities. Sjöwall et al. (2015) found that working memory was significantly associated with ADHD symptoms but not inhibitory abilities. In contrast, Tu et al. (2021) concluded that working memory had the most pronounced effect on children with ADHD symptoms, followed by inhibitory abilities. Alternatively, some researchers have found no observable EF deficits in children with ADHD (Willcutt et al., 2005; Xia, 2020).
Current Research
The literature shows that many researchers have explored the relationship between EF and ADHD in children. However, most of these studies have been done at the clinical level. They compare only differences in EF between children with ADHD and average children. With respect to the sequence of ADHD severity from subclinical to clinical, most studies focus their attention on children with a clinical ADHD diagnosis. Thus, children with subclinical features are overlooked (Levy et al., 1997). Yet, children with milder ADHD features, insufficient for a diagnosis of clinical psychiatric symptoms, may suffer from daily impairment (Otterman et al., 2019). Studies have found that younger children and adults with ADHD below clinical features also experience problems with executive function (Brocki et al., 2010). These findings are significant. Children with subclinical impairments frequently go undetected by mental health services for a variety of reasons (Ford et al., 2007). In addition, most studies have focused on school-age and adulthood while generally ignoring preschool, one of the most dramatic periods of human brain plasticity (Otterman et al., 2019). Furthermore, previous studies on EF and ADHD have been primarily cross-sectional, and inconsistencies in the results of the small number of longitudinal studies in combination lead to an inability to draw conclusions about the timing and temporality of the association. If a causal relationship between cognitive (EF) and ADHD subclinical characteristics can be identified in early childhood, early screening and interventions can be developed to substantially change individuals’ maladaptive behaviors (especially in those with subclinical ADHD).
Furthermore, early childhood is known as a stage of both rapid EF development and the initiation of ADHD onset (Best & Miller, 2010; Tu et al., 2020), along with significant age differences in the developmental rates of different EF components (Best & Miller, 2010; Wang et al., 2019). Regarding the age of ADHD development, the debate on whether ADHD is a self-healing disorder has led more researchers to focus on changing trends in the incidence of ADHD from school age to adulthood (Faraone et al., 2006). Meanwhile, this has neglected the age-related development of ADHD in preschool children, even though such trends have essential clinical value and implications for early detection and treatment by clinicians and parents (Daley et al., 2009). This gap in the literature highlights an important area of further research into age differences in EF and ADHD in preschool children.
Based on this, two research questions are proposed. First, to explore the temporal and age-specific trends in the components of executive function (working memory, inhibition, and regulation) and ADHD in children aged 4–6 years, investigating whether different characteristics of changes in executive function and ADHD emerge over time. Second, to explore the potential causal relationships between the three components of executive function and ADHD in young children by selecting the beginning and end of a school year as two time points to measure first the effect of EF/ADHD and then that of ADHD/EF.
Method
Participants
Using whole-class sampling, we recruited parents with young children enrolled at two kindergartens in a city in Henan Province. The first questionnaire was administered in October 2018 (Time 1; T1). The second was administered in June 2019 (Time 2; T2). The study protocol followed the ethical guidelines outlined by the American Psychological Association (APA). Respective principals at each kindergarten, the parents of all participating young children, and the institutional review board of Henan University approved the study. A total of 398 participants responded at T1. However, 22 were excluded at T2 due to missing or incomplete data, leaving 376 total valid responses (94.5% from T1, including 217 boys and 159 girls). Of these participants, 103 were 4 years of age (mean of 46.56 ± 3.87 monthsFootnote 1), 136 were 5 years of age (mean of 56.75 ± 4.72 months), and 137 participants were 6 years of age (mean age of 70.43 ± 10.74 months), all of whom were thus placed into respective groups for analysis. Additional family-related information about the children is shown in Table 1.
Research Tools
EF
To measure EF, we used the Chinese version of the Childhood Executive Functioning Inventory (CHEXI) developed by Thorell and Nyberg (2008), later translated and revised by Wei et al. (2018). The parents of participants were requested to rate their child’s EF. The CHEXI consists of 24 questions across the three dimensions of working memory, regulation, and inhibition; items are rated on a scale ranging from 1 to 5, with higher scores indicating a higher problem rate related to EF. In this study, the CHEXI received Cronbach’s alpha coefficients of 0.86 and 0.88 for T1 and T2, respectively.
ADHD
To measure ADHD, we used the ADHD subscale of the Strengths and Difficulties in Childhood Scale (parent version) (Goodman, 1997). This subscale has good measures of ADHD in young children (Xu et al., 2019). The subscale contains five items with scores ranging from 0 to 2. Higher scores indicate more severe ADHD problems. In this study, the scale received Cronbach’s alpha coefficients of 0.65 and 0.68 for T1 and T2, respectively.
Research Procedures
This study implemented a cross-lagged design in which parents responded to questionnaires concerning EF and ADHD in their young children. Specifically, this included the Executive Functioning Questionnaire for Young Children (parent version) and Attention Deficit Hyperactivity Disorder subscale (parent version), collected uniformly after completion. Following the time-lagged design, the questionnaires were completed at two time points, including October 2018 (T1), or within one month of the start of the school year, and June 2019 (T2), or within one month before the end of the school year. There was an eight-month interval between measurements.
Data Analysis and Common Method Deviation Test
We used the IBM SPSS 23.0 software package to enter, organize, and analyze the collected data. Four main steps were carried out. We used Harman’s one-way test to assess the common method effect in the first step. In the second step, we conducted repeated-measures ANOVAs with the three components of EF and ADHD set as dependent variables, the measurement times (T1 and T2) set as within-group variables, and age as between-group variables. This design was aimed at understanding the differences in changes in EF and ADHD between T1 and T2 between ages. In the third step, we investigated the relationship between EF and ADHD at different time points using the Pearson correlation method. Finally, we conducted a linear regression analysis to investigate any causal relationships between EF and ADHD in the fourth step.
As the questionnaires represented the measurement instruments and were rated by the children’s parents, there was a potential for common method bias. Therefore, we tested for the common method effect. The results showed that eight and seven principal component factors were extracted for T1 and T2 without rotation, respectively. The first principal component factor explained 23.53% and 26.23% of the total variance. These values were below the critical criterion of 40% (Zhou & Long, 2004). This result indicated that no significant common method bias effect was present.
Results
Descriptive Statistical Results for EF and ADHD
Table 2 shows the EF and ADHD scores for both T1 and T2.
There was a trend toward a decrease in both EF problems and ADHD tendencies over time. A repeated-measures ANOVA with ADHD set as the dependent variable, time of measurement (T1 and T2) set as the within-group variable, and age set as the between-group variable revealed that the main effect of time of measurement was not significant (F(1, 373) = 0.10, p > 0.05). The main effect of age was not significant (F(1, 373) = 2.24, p > 0.05). In addition, the age and time of measurement interaction effect was not significant (F(1, 373) = 0.28, p > 0.05). Separate repeated-measures ANOVAs with the three factors of EF set as dependent variables, measurement time set as a within-group variable, and age set as a between-group variable revealed significant main effects on measurement time only for working memory (F(1,373) = 20.59, p < 0.001, η2 = 0.052), with higher working memory problems in T1 than in T2. The other main and interaction effects were not significant (p > 0.05).
Correlation Analysis of EF and ADHD
We conducted a Pearson correlation analysis to correlate the variables associated with the two data points. As shown in Table 3, there were significant correlations between the T1 and T2 scores for the four variables of inhibition, working memory, regulation, and ADHD, thus indicating that the dimensions of EF and ADHD showed some stability over the investigated period. In addition, the three dimensions of EF were significantly correlated with ADHD at both T1 and T2. This result indicates that all three dimensions were significantly correlated with the simultaneity of ADHD. In addition, the immediate correlation between the three dimensions of EF and ADHD was significant. Therefore, the three dimensions of EF at T1 were significantly correlated with ADHD at T2, while ADHD at T1 was significantly correlated with the three dimensions of EF at T2. This result satisfied the basic study hypothesis.
Results of Cross-lagged Analysis of EF and ADHD
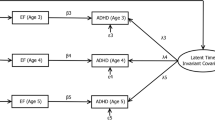
The interaction between inhibition ability and ADHD in young children was first examined. In the first step, a linear regression analysis was conducted with the ADHD score at T1 as the control variable, the inhibition on at T1 as the independent variable, and the ADHD at T2 as the dependent variable. The results (see Fig. 1) revealed that the inhibition at T1 significantly predicted the ADHD at T2 (β = 0.12, p < 0.05). In the second step, a linear regression analysis was conducted with the inhibition at T1 as the control variable, the ADHD at T1as the independent variable, and the inhibition at T2 as the dependent variable. It was found that the ADHD at T1 significantly predicted the inhibition at T2 (β = 0.12, p < 0.05).

Cross-lagged analysis of inhibition and ADHD
The results of the cross-lagged analysis of the interactions between working memory and regulation ability and ADHD according to the above two-step linear regression analysis are shown in Figs. 2 and 3, respectively, and it was found that the inter-predictive relationships between working memory and regulation ability and ADHD were both non-significant, ps > 0.05.

Cross-lagged analysis of working memory and ADHD

Cross-lagged analysis of regulation and ADHD
Discussion
Stability and Developmental Course of EF and ADHD in Young Children
Over the eight-month study interval, the participants showed some stability in their regulation and inhibition abilities. However, variability in their working memories, which gradually improved over time, was reported. This pattern may be related to the rate at which EF components develop. Indeed, a previous study on EF development in young children found a linear developmental trend in working memory from 4 to 14 years of age (Best & Miller, 2010). In other words, children’s working memories continuously develop over time, which is consistent with the current results; as the working memory capacity improves over time, problems in working memory become less frequent.
In contrast with the current results, the same previous study reported that early childhood was a period of rapid EF development, both for regulation and inhibition (Best & Miller, 2010). However, this discrepancy may be related to different measurement methods and contents. First, in terms of measurement methods, the questionnaire approach used in this study focused more on the comprehensive performance of EF in complex real-life situations. In contrast, previous research has mainly used task-operated laboratory tests that focused more on the highest performance of EF in optimal situations (Silver, 2014). Second, while previous experimental studies measured developmental indicators of executive function, the questionnaire used in this study focused on symptom indicators of executive function problems (Thorell & Nyberg, 2008). In this regard, developmental and symptomatology indicators should belong to different dimensions of EF. As such, the current results do not suggest that the regulation and inhibitory abilities of participants did not develop over the eight months. Rather, they most likely indicate that the symptoms of both types of EF problems in young children remain stable over time. These findings also remind us that EF development and symptoms in young children are separate factors requiring different treatments when studying EF.
Both the significant correlation in ADHD between T1 and T2 and the absence of significant differences in measurement time based on the ANOVA results suggest that ADHD was relatively stable over the eight-month study period. It did not fluctuate excessively over time. This may reflect the stability of the symptoms, i.e., they remain constant over a period of time. However, this study also used a parental perception questionnaire rather than a clinical diagnostic questionnaire. While specific questions in the ADHD dimension of the Strengths and Difficulties Questionnaire are consistent with the diagnostic criteria of the ICD-10 and DSM-IV (Xu et al., 2019), non-professional parents are more likely to equate these symptoms with developmental immaturity. Therefore, they tend to ignore or remain unaware of specific indicators. Thus, they may not detect ADHD in their young children until they reach school age, at which time abnormalities in learning and other areas will appear but are not clinically diagnosed until a later time. This result suggests that ADHD symptoms are very subtle in preschool years, and thus overlooked by many parents. The current results also suggest that we can increase awareness and knowledge about ADHD symptoms in young children from the clinical and scientific perspectives. This information will help parents in the daily identification of these symptoms, therefore increasing the potential for early intervention.
Interactions Between EF and ADHD in Young Children
This study reported an interaction between inhibitory ability and ADHD. More inhibitory ability problems at T1 were associated with more severe ADHD symptoms at T2, just as more severe ADHD symptoms at T1 were associated with more inhibitory ability problems at T2. Previous studies on the differences in inhibition abilities between children with ADHD and controls also showed a strong connection between these two factors (Wen & Chen, 2016). First, many studies have pointed out that young children’s inhibitory abilities predict the subsequent emergence of ADHD (Berlin et al., 2004; Brocki et al., 2007). Meanwhile, the EF deficit model also considers inhibition deficits a core deficit in ADHD (Barkley, 1997). Considering that inhibition is the foundation of cognitive functioning in young children (Berlin et al., 2004; Brocki et al., 2010; Espy & Bull, 2005), they must successfully develop this ability to accomplish complex tasks that require the purposeful control of irrelevant targets. In cases of impaired inhibition, young children will show worse cognitive outcomes, as they cannot inhibit irrelevant activities that limit their focus on target tasks. Therefore, in the long-term context, ADHD symptoms such as attention deficits will occur. Second, young children who develop ADHD symptoms and cannot focus their attention on target tasks will also have problems developing their inhibitory abilities. Studies on neurophysiological mechanisms in children with ADHD have found delays and abnormalities in their brain development associated with impaired inhibitory abilities (Krain & Castellanos, 2006). In cases where these delays and abnormalities exist, children with ADHD cannot successfully develop their inhibitory abilities and instead exhibit lower levels of inhibition.
We did not find an interaction between working memory, regulatory ability, and ADHD. This finding is consistent with Schoemaker et al. (2012). Moreover, working memory deficits in school-aged children are strongly associated with ADHD (Brocki & Bohlin, 2006; Willcutt et al., 2005). Regarding the lack of a relationship between working memory, regulatory ability, and ADHD, although young children experience rapid EF development, they still have lower developmental levels for working memory and regulatory ability, which are complex components of EF (Tu & Yang, 2018), and have therefore not yet failed to show differences in the relationship with ADHD. Furthermore, various theoretical (Diamond et al., 2007) and empirical studies (Berlin et al., 2004; Brocki et al., 2010; Espy & Bull, 2005) have suggested that more basic EF processes (e.g., inhibition) underlie the development of more complex EF components. Therefore, reinforced inhibitory deficits with increased age will directly impede the normal development of the working memory and regulation, and the impairment of these abilities leads to individuals exhibiting ADHD symptoms upon reaching school age. However, continued research is needed to verify the developmental dependence of the EF components.
Implications and Limitations
This study found that EF problems and ADHD symptoms were relatively stable in a sample of young children. Executive dysfunction and ADHD symptoms remained at a fixed level, with an interaction between inhibition and ADHD. In this context, impaired inhibition affects the subsequent emergence of ADHD, the symptoms of which exacerbate inhibition difficulties in early childhood. Thus, an urgent need exists to design trainning to help parents and teachers screen particular groups of young children for inhibition difficulties or ADHD symptoms early in life. Such trainning would facilitate interventions to mitigate the emergence or exacerbation of other cognitive impairments. Early identification and corrective treatments must be implemented promptly to ensure positive development in young children.
Although we found an interaction between inhibition and ADHD in young children, the association between working memory, regulation, and ADHD is more likely to emerge in school age. Therefore, it is essential to state the limitations of this study. First, we used questionnaires to collect data. Some researchers have suggested that different data collection methods affect the relationships between variables (Tu et al., 2021). Future studies should integrate multiple methods (e.g., questionnaires and experiments) to synthesize and verify the relationships between factors. Second, we only investigated two specific periods with an eight-month interval, which did not cover critical changes in participants’ EF development. Therefore, future studies should track the development of cognitive functions in young children over a more extended period to illustrate better the developmental change patterns of cognition. Finally, we only selected a normal group. We explored the relationship between subclinical manifestations of ADHD and EF problems in young children, failing to cover children with a clinical diagnosis of ADHD. Our study could not clarify the relationship between ADHD on a continuum from subclinical to clinical and EF, which requires further research in the future.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Notes
The mean age was the average at T1.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association. https://doi.org/10.1176/appi.books.9780890425596
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin,121(1), 65–94. https://doi.org/10.1037/0033-2909.121.1.65
Beck, D. M., Schaefer, C., Pang, K., & Carlson, S. M. (2011). Executive function in preschool children: Test–retest reliability. Journal of Cognition and Development,12(2), 169–193. https://doi.org/10.1080/15248372.2011.563485
Berlin, L., Bohlin, G., & Rydell, A. M. (2004). Relations between inhibition, executive functioning, and ADHD symptoms: A longitudinal study from age 5 to 8½ years. Child Neuropsychology,9(4), 255–266. https://doi.org/10.1076/chin.9.4.255.23519
Best, J. R., & Miller, P. H. (2010). A developmental perspective on executive function. Child Development,81(6), 1641–1660. https://doi.org/10.1111/j.1467-8624.2010.01499.x
Bohlin, G., Eninger, L., Brocki, K. C., & Thorell, L. B. (2012). Disorganized attachment and inhibitory capacity: Predicting externalizing problem behaviors. Journal of Abnormal Child Psychology,40(3), 449–458. https://doi.org/10.1007/s10802-011-9574-7
Brocki, K. C., & Bohlin, G. (2006). Developmental change in the relation between executive functions and symptoms of ADHD and co-occurring behaviour problems. Infant and Child Development,15(1), 19–40. https://doi.org/10.1002/icd.413
Brocki, K. C., Eninger, L., Thorell, L. B., & Bohlin, G. (2010). Interrelations between executive function and symptoms of hyperactivity/impulsivity and inattention in preschoolers: A two year longitudinal study. Journal of Abnormal Child Psychology,38(2), 163–171. https://doi.org/10.1007/s10802-009-9354-9
Brocki, K. C., Nyberg, L., Thorell, L. B., & Bohlin, G. (2007). Early concurrent and longitudinal symptoms of ADHD and ODD:Relations to different types of inhibitory control and working memory. Journal of Child Psychology and Psychiatry,48(10), 1033–1041. https://doi.org/10.1111/j.1469-7610.2007.01811.x
Daley, D., Jones, K., Hutchings, J., & Thompson, M. (2009). Attention deficit hyperactivity disorder in pre-school children: Current findings, recommended interventions and future directions. Child: Care Health and Development,35(6), 754–766. https://doi.org/10.1111/j.1365-2214.2009.00938.x
Diamond, A., Barnett, W. S., Thomas, J., & Munro, S. (2007). Preschool program improves cognitive control. Science,318(5855), 1387–1388. https://doi.org/10.1126/science.1151148
Diamond, A., & Lee, K. (2011). Interventions shown to aid executive function development in children 4 to 12 years old. Science,333(6045), 959–964. https://doi.org/10.1126/science.1204529
Espy, K. A., & Bull, R. (2005). Inhibitory processes in young children and individual variation in short-term memory. Developmental Neuropsychology,28(2), 669–688. https://doi.org/10.1207/s15326942dn2802_6
Espy, K. A., Sheffield, T. D., Wiebe, S. A., Clark, C. A., & Moehr, M. J. (2011). Executive control and dimensions of problem behaviors in preschool children. Journal of Child Psychology and Psychiatry,52(1), 33–46. https://doi.org/10.1111/j.1469-7610.2010.02265.x
Faraone, S. V., Biederman, J., & Mick, E. (2006). The age-dependent decline of attention deficit hyperactivity disorder: A meta-analysis of follow-up studies. Psychological Medicine,36(2), 159–165. https://doi.org/10.1017/s003329170500471x
Ford, T., Hamilton, H., Meltzer, H., & Goodman, R. (2007). Child mental health is everybody’s business: The prevalence of contact with public sector services by type of disorder among British school children in a three-year period. Child and Adolescent Mental Health,12(1), 13–20. https://doi.org/10.1111/j.1475-3588.2006.00414.x
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry,38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x
Kim, S., Nordling, J. K., Yoon, J. E., Boldt, L. J., & Kochanska, G. (2013). Effortful control in “Hot” and “Cool” tasks differentially predicts children’s behavior problems and academic performance. Journal of Abnormal Child Psychology,41(1), 43–56. https://doi.org/10.1007/s10802-012-9661-4
Krain, A. L., & Castellanos, F. X. (2006). Brain development and ADHD. Clinical Psychology Review,26(4), 433–444. https://doi.org/10.1016/j.cpr.2006.01.005
Levy, F., Hay, D. A., Mcstephen, M., Wood, C., & Waldman, I. (1997). Attention-deficit hyperactivity disorder: A category or a continuum? Genetic analysis of a large-scale twin study. Journal of the American Academy of Child & Adolescent Psychiatry,36(6), 737–744. https://doi.org/10.1097/00004583-199706000-00009
Mahone, E. M., & Hoffman, J. (2007). Behavior ratings of executive function among preschoolers with ADHD. The Clinical Neuropsychologist,21(4), 569–586. https://doi.org/10.1080/13854040600762724
Moffitt, T. E., Arseneault, L., Belsky, D., Dickson, N., Hancox, R. J., Harrington, H. … Caspi, A. (2011). A gradient of childhood self-control predicts health, wealth, and public safety. Proceedings of the National Academy of Sciences, 108(7), 2693–2698. https://doi.org/10.1073/pnas.1010076108
Neely, R. J., Green, J. L., Sciberras, E., Hazell, P., & Anderson, V. (2016). Relationship between executive functioning and symptoms of attention-deficit/hyperactivity disorder and autism spectrum disorder in 6–8 year old children. Journal of Autism and Developmental Disorders,46(10), 3270–3280. https://doi.org/10.1007/s10803-016-2874-6
Otterman, D. L., Koopman-Verhoeff, M. E., White, T. J., Tiemeier, H., Bolhuis, K., & Jansen, P. W. (2019). Executive functioning and neurodevelopmental disorders in early childhood: A prospective population-based study. Child and Adolescent Psychiatry and Mental Health,13(1), 1–12. https://doi.org/10.1186/s13034-019-0299-7
Polanczyk, G. V., Salum, G. A., Sugaya, L. S., Caye, A., & Rohde, L. A. (2015). Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry,56(3), 345–365. https://doi.org/10.1111/jcpp.12381
Rajendran, K., O’Neill, S., Marks, D. J., & Halperin, J. M. (2015). Latent profile analysis of neuropsychological measures to determine preschoolers’ risk for ADHD. Journal of Child Psychology and Psychiatry,56(9), 958–965. https://doi.org/10.1111/jcpp.12434
Schoemaker, K., Bunte, T., Wiebe, S. A., Espy, K. A., Deković, M., & Matthys, W. (2012). Executive function deficits in preschool children with ADHD and DBD. Journal of Child Psychology and Psychiatry,53(2), 111–119. https://doi.org/10.1111/j.1469-7610.2011.02468.x
Silver, C. H. (2014). Sources of data about children’s executive functioning: Review and commentary. Child Neuropsychology,20(1), 1–13. https://doi.org/10.1080/09297049.2012.727793
Singh, A., Yeh, C. J., Verma, N., & Das, A. K. (2015). Overview of attention deficit hyperactivity disorder in young children. Health Psychology Research,3(2), 2115. https://doi.org/10.4081/hpr.2015.2115
Sjöwall, D., Backman, A., & Thorell, L. B. (2015). Neuropsychological heterogeneity in preschool ADHD: Investigating the interplay between cognitive, affective and motivation-based forms of regulation. Journal of Abnormal Child Psychology,43(4), 669–680. https://doi.org/10.1007/s10802-014-9942-1
Sjöwall, D., Bohlin, G., Rydell, A. M., & Thorell, L. B. (2017). Neuropsychological deficits in preschool as predictors of ADHD symptoms and academic achievement in late adolescence. Child Neuropsychology,23(1), 111–128. https://doi.org/10.1080/09297049.2015.1063595
Thapar, A., & Cooper, M. (2016). Attention deficit hyperactivity disorder. The Lancet,387(10024), 1240–1250. https://doi.org/10.1016/s0140-6736(15)00238-x
Thomas, R., Sanders, S., Doust, J., Beller, E., & Glasziou, P. (2015). Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Pediatrics,135(4), e994–e1001. https://doi.org/10.1542/peds.2014-3482
Thorell, L. B., & Nyberg, L. (2008). The childhood executive functioning inventory (CHEXI): A new rating instrument for parents and teachers. Developmental Neuropsychology,33(4), 536–552. https://doi.org/10.1080/87565640802101516
Tu, M. L., Hou, T. T., & Yang, F. Y. (2020). Progress of research on children with attention deficit hyperactivity disorder in preschools abroad. Chinese Journal of Special Education,09, 53–59. https://doi.org/10.3969/j.issn.1007-3728.2020.09.009 (In Chinese)
Tu, M. L., Liu, Q., Yang, F. Y., & Wang, Q. (2021). A meta-analysis of executive function and attention deficit hyperactivity symptoms in preschool children: the role of inhibitory control and working memory. Journal of Special Education,02, 67–76. https://doi.org/10.3969/j.issn.1007-3728.2021.02.010 (In Chinese)
Tu, M. L., & Yang, F. Y. (2018). Progress of foreign research on executive functions of preschool children in the last decade. Studies in Preschool Education,09, 27–38. https://doi.org/10.13861/j.cnki.sece.2018.09.003 (In Chinese)
Wang, J. M., Zhang, Y. B., Zheng, C. Y., Lu, Y. J., & Qin, J. L. (2019). A study on the development of executive function subcomponents in children aged 3–6 years. Psychological Development and Education,35(01), 1–10. https://doi.org/10.16187/j.cnki.issn1001-4918.2019.01.01 (In Chinese)
Wei, W., Xie, Q. B., Zhu, J. J., He, W., & Li, Y. (2018). Reliability analysis of the Child Executive Functioning Scale in Chinese preschool children. Chinese Journal of Clinical Psychology,26(01), 26–29. https://doi.org/10.16128/j.cnki.1005-3611.2018.01.006 (In Chinese)
Wen, P., & Chen, Y. C. (2016). Inhibitory control and working memory in 4-year-olds with attention deficit hyperactivity disorder. Chinese Journal of Special Education,09, 55–59. https://doi.org/10.3969/j.issn.1007-3728.2016.09.009 (In Chinese)
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biological psychiatry,57(11), 1336–1346. https://doi.org/10.1016/j.biopsych.2005.02.006
Xia, R. (2020). Comparison and classification of executive function and psychological theory between ADHD and ASD children (Master’s thesis). East China Normal University
Xu, W. B., Wang, M. C., Deng, J. X., Liu, H. H., Zeng, H., & Yang, W. D. (2019). Reliability probability analysis of the Chinese version of the Strengths and Difficulties Questionnaire. Chinese Journal of Clinical Psychology,27(01), 67–72. https://doi.org/10.16128/j.cnki.1005-3611.2019.01.014 (In Chinese)
Zhou, H., & Long, L. R. (2004). A statistical test and control method for common method bias. Advances in Psychological Science,12(06), 924–950. https://doi.org/10.3969/j.issn.1671-3710.2004.06.01 (In Chinese)
Funding
This work was supported by the research project of the reform of teacher education curriculum in Henan Province (No: 2015-JSJYZD-003).
Author information
Authors and Affiliations
Contributions
Conceptualization, methodology, Writing—original draft preparation: L.F.; Writing—review and editing: L.F. and Y.W.; Visualization: Y.W.; Funding acquisition: L.F. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflict of interest.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Review Board (or Ethics Committee) of Henan University (protocol code HUIRB2020-301), and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to Participate
Informed consent was obtained from all individual participants involved in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fan, L., Wang, Y. The relationship between executive functioning and attention deficit hyperactivity disorder in young children: A cross-lagged study. Curr Psychol 42, 21375–21383 (2023). https://doi.org/10.1007/s12144-022-03233-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-03233-5