
Abstract
different populations have different averages of life-space assessment scores and defining cutoff values of clinical significance by each population should take into consideration. Different cutoffs to define restricted life space have been reported. The most common is a score of 60 points. There are other cutoffs derived from receiver operating characteristic (ROC) analysis and used to classify older adults according to their ability in activities of daily living (ADLs) (52.3 points) or instrumental activities of daily living (IADLs) (56 points); other cutoffs are specialized for people with cognitive impairment (26.75 points) or people with spinal cord injury who need mobility aids (78.5 points). The aims were to identify cutoff points of Life Space Assessment (LSA) in older adults in different sites and to determine the relationship of the cutoff scores with mobility disability and depression. The study population was composed of community-dwelling adults aged 65–74 years who were not institutionalized. An ROC analysis was constructed, and the area under the curve (AUC) was calculated to identify the optimal cutoff that discriminates life-space restriction for each city. Logistic regressions were executed by site to comprehend the association among restricted LSA and mobility disability and depression. In total, 1890 participants were included in the analyses (52.38% women, 37.19% mobility disability and 21.32% had depression). Canada cities had the highest cutoff, while Tirana and Natal had the lowest cutoff (< 50). Kingston was the site with the highest association between life-space restriction and mobility disability (OR 5.4, 95% CI 2.9–10). Saint-Hyacinthe, Tirana, and Manizales had significant associations between depression and restricted life space (OR 3.25, 95% CI 1.53–6.89, OR 3.14, 95% CI 1.88–5.24, and OR 3.99, 95% CI 2.28–6.98, respectively). Different cutoffs to define restricted life-space have been identified in elderly people at different sites. The analysis of the relationship between the restricted life space and personal characteristics like depression and mobility disability supported these findings. The groupings produced by the cutoff points for each site showed notable variations. These findings emphasize the importance of population-based cutoffs to improve the general applicability of LSM criteria and take into consideration the importance of site-specific approaches.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Physical mobility affects all aspects of daily life and is a crucial part of an independent life (Satariano et al., 2012). Life-space mobility (LSM) reflects the real execution and refers to the area in which a person moves in daily life, the frequency and the need for assistance (Allman et al., 2006; Baker et al., 2003; Stalvey et al., 1999). Mobility in life-space not only measures walking ability but also includes other forms of mobility, such as using public transport or driving a car (Béland et al., 2018; Stalvey et al., 1999), and is an indicator of social participation (Sawyer & Allman, 2010). A more spacious life space provides a person with more opportunities to interact with others (Kono et al., 2004; Kuspinar et al., 2020). Conversely, restriction of life space is associated with poor physical performance, mobility limitations and disability (Curcio et al., 2013; Portegijs et al., 2015, 2016), depressive symptoms (Polku et al., 2015), cognitive impairment (James et al., 2011), limited access to social services (Rantakokko et al., 2016) and diminution of active social participation (Barnes et al., 2007; Taylor et al., 2018).
In recent decades, there has been an increasing tendency to use the University of Alabama at Birmingham (UAB) Life-Space Assessment (LSA) (Baker et al., 2003), which has been validated in different populations and translated in several languages, such as Chinese, Japanese, Spanish, Portuguese, Danish, and French (Johnson et al., 2020).
Different cutoffs to define restricted life space have been reported. The most common is a score of 60 points, which represents a level of self-sufficiency and independent mobility that is consistent with optimal and adaptive aging (Allman et al., 2006; Peel et al., 2005; Sawyer & Allman, 2010; Sheppard et al., 2013). To attain a score of 60, a person must be independent within their home environment and able to travel outside the neighborhood independently (Allman et al., 2006; Sawyer & Allman, 2010). There are other cutoffs derived from receiver operating characteristic (ROC) analysis and used to classify older adults people according to their ability in activities of daily living (ADLs) (52.3 points) (Portegijs et al., 2016) or instrumental activities of daily living (IADLs) (56 points) (Shimada et al., 2010); other cutoffs are specialized for people with cognitive impairment (26.75 points) (Ullrich et al., 2018) or people with spinal cord injury who need mobility aids (78.5 points) (Lanzino et al., 2016). If life space is to be used as an index of integration and social participation in geographically defined areas, providing a measure of how far, how often, and how independently individuals move in their environments (Sawyer & Allman, 2010), a cutoff point must be established for this purpose.
On the other hand, there is evidence that life space is explained largely by the physical ability to carry out specific activities of daily living (ADLs) and by performance on specific mobility-related tasks, that is, walking speed, timed chair stands, and standing balance (Peel et al., 2005). As suggested by Stalvey and colleagues (Stalvey et al., 1999), multiple factors other than performance may be included in determining the scope of individual life space, including environmental characteristics and socioeconomic and emotional resources. In fact, the results of the International Mobility in Aging Study (IMIAS) study showed that lower LSA was related to female sex, lower education, insufficient income, poor physical performance, mobility limitations, disability (Carmen-Lucia Curcio et al., 2013), cognitive decline (Caldas et al., 2020), restricted physical activity (Peña & Curcio, 2016) and fear of falling (Auais et al., 2017).
Beyond individual differences that influence the life-space mobility different populations may have different life space mobility patterns. The environmental, social and cultural, arrangements could be impacting this pattern. It has been shown that lower life space mobility was also relate to physical and social environmental barriers, e.g. lack of transportation, unwalkable neighborhoods (Cagney et al., 2013), living in areas where the socioeconomic conditions are unfavorable (Arms et al., 2021; Curcio et al., 2013), poverty (Curcio et al., 2013; Wong et al., 2021) environmental inequities, including disproportionate distribution of public space and green areas as well as quality of roads, (Curcio et al., 2013; Kuspinar et al., 2020; Wong et al., 2021) street violence, and feelings of insecurity (Curcio et al., 2013). Limited life space mobility is also associate with of high curbs, lighting, dangerous cross-roads, poor sidewalks, heavy traffic, inadequate lighting, lack of benches along routes and long distances to services, suggesting an important role of physical and social environments on life space mobility (Rantakokko et al., 2012, 2015).
LSA was also related to place, with lower LSA scores observed in developing countries (Portegijs et al., 2016), suggesting that different populations have different averages of LSA scores, and research aiming at defining cutoff values of clinical significance should take into consideration the importance of site-specific approaches (Ahmed et al., 2020; Curcio et al., 2013).
The purposes of this study were twofold: (1) to identify cutoff points of LSM in older adults in different sites to improve the general applicability of LSM criteria and (2) to determine the relationship of the cutoff scores with mobility disability and depression. Establishing relevant cutoff points for future health outcomes may provide evidence for the clinical relevance of life-space mobility for community-dwelling older populations.
Methods
Study Design and Participants
We used cross-sectional data from the IMIAS, a longitudinal multicenter study conducted with the aim of examining social and gender differences in mobility using a life-course perspective. The study was conducted at five sites: Tirana (Albania), Natal (Brazil), Manizales (Colombia), Kingston (Canada), and Saint-Hyacinthe (Canada). These cities are located in settings with different socioeconomic contexts, physical environments, and cultural norms. A more detailed description of the research sites and procedures has been reported previously (Gomez et al., 2018).
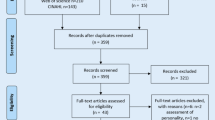
The study population was composed of community-dwelling adults aged 65–74 years who were not institutionalized. The sample was stratified by gender at the enrollment stage. The samples in Tirana, Natal and Manizales were randomly selected through registers at community health clinics and public health insurance databases. Due to contact restrictions imposed by ethics committees in Kingston and Saint-Hyacinthe, potential participants were invited by letter from their primary care physicians to contact our field coordinator to participate in the study. A sample of 1998 community-dwelling older people was recruited in 2012, of whom this study included only a sample of 1890 due to missing data on covariables. The included subjects were distributed as follows: Kingston, 385; Saint-Hyacinthe, 377; Tirana, 354; Manizales, 372; and Natal, 402. Severe cognitive decline, defined as the presence of four or more errors in the orientation domain of the Leganes Cognitive Test (LCT), was considered an exclusion criterion for participation in the study (Zunzunegui et al., 2000).
Life‑Space Assessment
LSM was measured with the LSA (Baker et al., 2003), with five levels of living space (from within the home to out of town), during the month before assessment (Peel et al., 2005); this instrument has been validated in Spanish and Portuguese during IMIAS pilot studies (Curcio et al., 2013). For each level of life space, respondents were asked about their frequency of travel (from once a week to daily) and the need for help from another person or the use of aids or equipment. Total composite LSA scores range from 0 (restriction to bed) to 120 points. Higher scores generally represent greater distance, frequency or independence of movement, including the ability to travel frequently out of town.
Mobility Disability and Depression
Mobility disability was assessed with the Nagi questionnaire (Nagi, 1976), measuring self-reported difficulty in climbing a flight of stairs without resting or in walking 400 m. The Center for Epidemiological Studies–Depression (CES-D) scale (Roadolff, 1977) was used to assess symptoms, with higher scores (≥ 16) considered suggestive of depression (Gómez et al., 2013).
Covariates
Analytical models were adjusted for sociodemographic variables (age, gender, education level), fear of falling, physical performance, and number of chronic conditions. Age and educational level were recorded in years, where educational level was defined as how many years of school the older adults had completed. Fear of falling (FoF) was assessed using the Falls Efficacy Scale International (FES-I) (Yardley et al., 2005). This test is composed of a 16-item questionnaire, with possible scores ranging from 16 (no concern about falling) to 64 (severe concern about falling).
Physical performance was assessed with the Short Physical Performance Battery (SPPB) (Guralnik et al., 1994). This test was performed using three subtests: standing balance test, gait speed, and chair stand test. The sum of 3 subtests composed the final SPPB score, which ranged from 0 to 12, with higher scores reflecting better physical function.
Cognitive function was assessed by the Leganés Cognitive Test (LCT) (Zunzunegui et al., 2000). A score less than or equal to 22 points was indicative of cognitive impairment (Del Brutto et al., 2014). Information about chronic conditions was collected using the question, “Has a doctor or nurse ever told you that you have a chronic condition?”. The question refers to hypertension, diabetes, cancer, chronic lung disease, heart disease, stroke (cerebral embolism or thrombosis), osteoarthritis (arthritis or rheumatism), osteoporosis and cataracts. The answers were categorized into two groups: up to one condition and two or more conditions. Previously, these covariates have been associated with Life-Space Assessment scores (Curcio et al., 2013; Peel et al., 2005; Polku et al., 2015).
Data Analysis
An ROC analysis was constructed, and the area under the curve (AUC) was calculated to identify the optimal cutoff that discriminates life-space restriction for each city. Discrimination of cutoff was adjusted with maximum life space, being restricted if score was between 0 and 1 and unrestricted with scores between 2 and 5. The Youden index was used to identify the ROC curve with the highest sensitivity and specificity. This analysis was executed for all 5 sites independently. The interpretation of the results was measured according to AUC as follows: moderately precise (0.7 < AUC ≤ 0.9), highly precise (0.9 < AUC < 0.1) and perfect discrimination (AUC = 1.0) (Swets, 1998). Regarding the function of site cutoffs, the existence of significant differences in descriptive variables that have been associated with LSA (demographics, physics, cognitive and emotional health variables) was analyzed (Béland et al., 2018; Peel et al., 2005; Polku et al., 2015; Portegijs et al., 2016; Snih et al., 2012). t-tests (continuous variables) and chi-square tests (dichotomous variables) were applied. A p < 0.05 was considered statistically significant.
Subsequently, logistic regressions were executed by site to comprehend the association among restricted LSA (according to the cutoff identified) and mobility disability and depression. There were 2 models, adjusting for the following sets of variables: (1) sex and chronic diseases, and (2) the previously mentioned variables plus SPPB, age, years of education and fear of falling. The confidence interval used was 95%. Statistical analyses were executed with Anaconda 3 v1.10.0 using Python and SPSS v23.
Results
Among 1890 participants in the sample (52.38% women) with mean age of 69.08 (± 2.85) years, 47.46% reported medium and high concern with fear of falling, 12.19% with poor physical performance (SPPB < 8), 37.19% mobility disability, 21.32% had depression and 57.14% had two or more chronic conditions. In the LSA, the study participants achieved an average of 68.32. More details on the differences in the survey participants according to study sites can be found in Table 1.
The optimal cutoff point, sensitivity and specificity for each site are shown in Table 2. The cutoff and AUC ROC are shown in Fig. 1 for each site. According to the curves, Canada cities had the highest cutoff, while Tirana and Natal had the lowest cutoff (< 50). The AUC ROC for all sites was considered excellent, with values ranging from 0.90 to 0.96.

Receiver operating characteristic curves for LSA by site
In accordance with the cutoff of each site, there were significant differences (p < 0.05) in sex, age, education level, depression, physical performance, chronic diseases and disability (see Table 3). Depression, number of chronic diseases, being a woman, and having difficulties walking or climbing stairs were significantly different between restricted and nonrestricted life spaces at all sites. Years of education had significant differences at 4 sites, excluding Kingston. There were only 3 sites at which SPPB and FoF had significant differences.
In the Model 1 logistic regression analysis, mobility disability was associated with life-space restriction at all sites, presenting a significant OR, as shown in Table 4. Kingston was the site with the highest association between life-space restriction and mobility disability (OR 5.4, 95% CI 2.9–10). On the other hand, only Saint-Hyacinthe, Tirana, and Manizales had significant associations between depression and restricted life space (OR 3.25, 95% CI 1.53–6.89, OR 3.14, 95% CI 1.88–5.24, and OR 3.99, 95% CI 2.28–6.98, respectively). Manizales was the site with the highest association based on depression.
In the model adjusting for SPPB, FES, years of education, and age, both depression and mobility disability had reduced ORs and sometimes lost their statistical significance. The only site that maintained a significant OR after adjusting Model 2 for depression and mobility disability was Manizales (OR 3.12, 95% CI 1.72–5.66, and OR 2.46, 95% CI 1.31–4.63, respectively). In Saint-Hyacinthe, depression and mobility disability lost their significance after adjusting Model 2.
Discussion
The present study provides data-driven cutoff points to identify restricted life space in older people in different contexts. The highest were in Canada (Kingston 69 and Saint-Hyacinthe 60 points), followed by Manizales (55.5 points); Tirana and Natal had the lowest scores, at 48.5 and 48 points, respectively. Thus, these findings add to previous evidence on the importance of defining cutoff values of clinical significance across different older adult population groups and places. In multiple logistic regression models, participants under the cut point (restricted life space) in each site showed a significantly higher OR for depression and mobility disability than participants above the cut point.
Canadian sites have the highest cutoff points for restricted life space, and these sites also have higher educational levels, fewer symptoms of depression, better observed physical performance and lower FoF. Previous studies have shown that better socioeconomical and functional conditions contribute to a higher life space (Auais et al., 2017; Curcio et al., 2013). A score ≥ 60 corresponds well with the ability to travel outside one’s own neighborhood independently (Allman et al., 2006; Peel et al., 2005). Additionally, cross-sectional and longitudinal studies showed associations with different measures, ADL and IADL limitation, lack of depression, cognition, and mortality over 4 years differed dramatically for persons scoring below and above 60 points on LSA (Sawyer & Allman, 2010). This cutoff point is widely used (Allman et al., 2006; Peel et al., 2005; Portegijs et al., 2014; Sawyer & Allman, 2010; Sheppard et al., 2013) and was found only in Saint-Hyacinthe. The cutoff for Manizales (55.5) is similar to that reported by Shimada et al. (Shimada et al., 2010) in a cross-sectional study in Japan to identify the risk of IADL limitation (56 points) and is not much different from those found in previous studies with slightly different approaches.
Other studies have shown slightly lower cutoff points for restricted life-space based on sensitivity (0.86) and specificity (0.74) analyses according to ability in ADL (52.3 points) (Portegijs et al., 2016). This cutoff point was associated with higher odds of presenting difficulty or inability in ADLs at baseline and with the development of new difficulty and inability at the 2-year follow-up, even after adjustment for factors known to be correlated with the development of ADL disability (Portegijs et al., 2016).
Tirana and Natal were the cities with the lowest cutoff point, with a value very similar to that identified by Lanzino et al. in people with spinal cord injury who require equipment to move around (49 points) (Lanzino et al., 2016). In particular, these 2 cities had the highest average of chronic diseases and the highest percentage of the population with mobility disabilities.
Possible underlying mechanisms for cutoff restricted life-space differences can be conceptualized in several ways. First, in line with previous studies, we found that LSM has been associated with social and cultural environmental aspects such as education, poverty, and exposure to social circumstances across the life course that are different in older people from places (Curcio et al., 2013). In the same way, it is not surprising that the cut-off points were lower in middle-income countries, as their populations are more affected by socio-economic problems and have poorer performance, but there are different concepts and cultural patterns of mobility and transport that justify that the population has lower performance and moves in smaller living spaces, which does not mean that they are at higher risk of functional decline over time.
Latin American cities, individuals typically do not leave their neighborhoods for daily activities, social interactions, and access to institutional resources because they have access to a variety of services and support networks in their neighborhoods, including: Access to churches, banks, grocery stores, pharmacies, cultural institutions, green spaces, and other amenities. Additionally, it is important to consider that older adults in middle-income countries are less likely to drive than older adults in high-income countries (Caldas et al., 2020), most people in low- and middle-income countries do not have a driver’s license or own a car due current economic conditions and because a few decades ago, owning a car was a sign of socioeconomic status. On the contrary, for older adults in high-income countries, including Canada, driving has been identified as the most popular and preferred means of community mobility. Having a driver’s license and access to a private automobile in older adulthood has been associated with higher LSM. According to Kuspinar et al. in the Canadian Longitudinal Study on Aging, non-drivers (7.8%) had smaller living spaces over time (Kuspinar et al., 2020). Also, in Japan the access to motorized transportation, including car ownership and rail use, was associated with higher LSM scores. Conversely, lower levels of car access, such as no car at home or only sharing a car, are factors that imply a limited (Tran et al., 2022).
Second, environmental and neighborhood characteristics and research site contexts could also explain the differences between cutoff restricted LSMs. Neighborhoods can act as either a barrier or facilitator for older adults to age well (Lu et al., 2021). Environmental factors include perceived barriers (Portegijs et al., 2017), environmental facilitators (Eronen et al., 2014), access to social services (Murayama et al., 2012), social support and social assistance (Kuspinar et al., 2020), and neighborhood green space (Gong et al., 2014). In the same way, environmental inequities, including disproportionate distribution of public space and green areas as well as quality of roads and neighborhood violence, are associated with restricted life-space mobility in older people (Curcio et al., 2013). Third, we have previously reported that individual differences between older adults in different sites, such as comorbidities, depression, FoF, physical function and functional limitations, could affect life-space mobility (Ahmed et al., 2020; Auais et al., 2017; Caldas et al., 2020; Curcio et al., 2018).
When we analyzed the association of cutoff restricted life space, depression, number of chronic diseases, and mobility disability had significant differences between the groups generated by the cutoff points for all sites. According to Model 1, the relationship between depressive symptoms and restricted life space was significant at three sites, except in Kingston and Natal. It has been established that a more restricted LSM is correlated with a higher probability of depressive symptoms (Polku et al., 2015); in addition, being homebound is a significant predictor of depression in the older adults (Choi et al., 2013).
On the other hand, the relationship between restricted life space and mobility disability was evident. In Model 1, all sites had a significant relationship, where the lowest OR was 2.85 for Tirana. This significance was held in Model 2 for three sites. This relationship was previously shown by Fristedt et al., who found a significant correlation between stair climbing and LSA (Fristedt et al., 2016). Similarly, Mardini et al. wrote that according to the National Center for Health Statistics, people with difficulties walking 400 m had a significant negative impact on LSM (Mardini et al., 2021). Conversely, a prevention intervention for disability can improve life space and fall efficacy (Liu et al., 2021).
This is an international study that includes diverse cities from middle- and high-income countries. Variability was minimized during data collection through standardized measurement tools. Relationships found in this study are free of causality due to the cross-sectional design applied. Findings on Canada sites might not be fully representative because participants were not selected randomly due to Canadian ethics committees’ requirements (Guedes et al., 2015). Although LSA registers only the information from the last month, data can be influenced by the weather at locations with high and low temperatures (Yamasaki & Someya, 2015). However, LSA has been found to be reliable across different seasons in the same sample (Portegijs et al., 2014; Yamasaki & Someya, 2015).
Conclusion
To our knowledge, this is the first international study to provide data-driven cutoff points to identify restricted life-space mobility by using older adults in different contexts. Different cutoffs to define restricted life space have been identified in older adults people at different sites. These findings emphasize the importance of population-based cutoffs to improve the general applicability of LSM criteria and take into consideration the importance of site-specific approaches. LSM is a multi-faceted concept that includes personal, physical, financial, and socio-cultural dimensions. It serves as a framework for a variety of daily behaviors and is the result of the interplay between environmental conditions and individual capabilities. Geographic, social, and cultural variables need to be considered as they influence the measurement of LSA and, consequently, the cut-off point for determining whether or not restricted life-space mobility exists. Our analysis of the relationship between the restricted life-space and personal characteristics like depression and mobility disability supported these findings. The groupings produced by the cutoff points for each site showed notable variations.
Strength and Limitations
The main strength of this study was obtaining cutoffs for five diverse cities and highlighting their differences. Additionally, we identified what relationships existed between their respective cutoffs and depression and mobility disability. Facing limitations, one of the studies was that our study analyzed only community-dwelling older adults in a narrow age range, between 65 and 74 years. Additionally, our results show interesting differences between men and women that can reflect a possible reason to calculate a new cutoff. Although in our research this cutoff was not calculated, it would be a new field to analyze LSA.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Ahmed, T., Curcio, C. L., Auais, M., Vafaei, A., Pirkle, C. M., Guerra, R. O., & Gomez, F. (2020). Falls and life-space mobility: Longitudinal analysis from the International mobility in Aging Study. Aging Clinical and Experimental Research. https://doi.org/10.1007/s40520-020-01540-0.
Allman, R. M., Sawyer, P., & Roseman, J. M. (2006). The UAB study of aging: Background and insights into life-space mobility among older americans in rural and urban settings. Aging and Health, 2(3), 417–429. https://doi.org/10.2217/1745509X.2.3.417.
Arms, T. E., Crane, P. B., McNeill, C., Horne, C., & Whited, M. C. (2021). Life-space constriction in aging adults. Geriatric Nursing, 42(2), 421–426. https://doi.org/10.1016/j.gerinurse.2021.02.001.
Auais, M., Alvarado, B., Guerra, R., Curcio, C. L., Freeman, E. E., Ylli, A., Guralnik, J., & Deshpande, N. (2017). Fear of falling and its association with life-space mobility of older adults: A cross-sectional analysis using data from five international sites. Age and Ageing, 46(3). https://doi.org/10.1093/ageing/afw239.
Baker, P. S., Bodner, E. V., & Allman, R. M. (2003). Measuring life-space mobility in Community-Dwelling older adults. Journal of the American Geriatrics Society, 51(11), 1610–1614. https://doi.org/10.1046/j.1532-5415.2003.51512.x.
Barnes, L. L., Wilson, R. S., Bienias, J. L., De Leon, M., Kim, C. F., Buchman, H. J. N., A. S., & Bennett, D. A. (2007). Correlates of life space in a volunteer cohort of older adults. Experimental Aging Research, 33(1), 77–93. https://doi.org/10.1080/03610730601006420.
Béland, F., Julien, D., Bier, N., Desrosiers, J., Kergoat, M. J., & Demers, L. (2018). Association between cognitive function and life-space mobility in older adults: Results from the FRéLE longitudinal study. BMC Geriatrics, 18(1). https://doi.org/10.1186/s12877-018-0908-y.
Cagney, K., Browning, C. R., J., Jackson, A. L. (2013). Networks, Neighborhoods, and Institutions: An Integrated Activity Space Approach for Research on Aging. In W. LJ & P. TJ (Eds.), Panel on New Directions in Social Demography, Social Epidemiology, and the Sociology of Aging (pp. 95–119). National Academies Press. https://www.ncbi.nlm.nih.gov/books/NBK184369/.
Caldas, V., Fernandes, J., Vafaei, A., Gomes, C., Costa, J., Curcio, C., & Guerra, R. O. (2020). Life-Space and Cognitive decline in older adults in different Social and Economic contexts: Longitudinal results from the IMIAS Study. Journal of Cross-Cultural Gerontology, 35, 237–250. https://doi.org/10.1007/s10823-020-09406-8.
Choi, N. G., Sirey, J. A., & Bruce, M. L. (2013). Depression in Homebound older adults: Recent advances in screening and psychosocial interventions. Curr Transl Geriatr Exp Gerontol Rep, 2(1), 16–23. https://doi.org/10.1007/s13670-012-0032-3.
Curcio, C. L., Alvarado, B., Gomez, F., Guerra, R., Guralnik, J., & Zunzunegui, M. V. (2013). Life-Space Assessment scale to assess mobility: Validation in latin American older women and men. Aging Clinical and Experimental Research, 25(5), 553–560.
Curcio, C. L., Benjumea, Á., & Gómez, F. (2018). Frailty and Life-space: results from IMIAAS Study. International Conference on Frailty & Sarcopenia Research 2017, April 2017.
Del Brutto, O. H., Mera, R. M., Zambrano, M., & Lama, J. (2014). The leganés cognitive test correlates poorly with MRI evidence of global cortical atrophy in an underserved community a population-based and nested case-control study in rural Ecuador (the atahualpa project). Dementia e Neuropsychologia, 8(4), 351–355. https://doi.org/10.1590/s1980-57642014dn84000008.
Eronen, J., von Bonsdorff, M., Rantakokko, M., & Rantanen, T. (2014). Environmental facilitators for outdoor walking and development of walking difficulty in community-dwelling older adults. European Journal of Ageing, 11(1). https://doi.org/10.1007/s10433-013-0283-7.
Fristedt, S., Kammerlind, A. S., Ernsth, M. B., & Fransson, E. I. (2016). Concurrent validity of the Swedish version of the life-space assessment questionnaire. BMC Geriatrics, 16(1). https://doi.org/10.1186/s12877-016-0357-4.
Gomez, F., Zunzunegui, M. V., Alvarado, B., Curcio, C. L., Pirkle, C. M., Guerra, R., Ylli, A., & Guralnik, J. (2018). Cohort Profile: The International Mobility in Aging Study (IMIAS). International Journal of Epidemiology, 47(5), 1303–1393h. https://doi.org/10.1093/ije/dyy074.
Gómez, J. F., Curcio, C. L., Alvarado, B., Zunzunegui, M. V. M. V., & Guralnik, J. (2013). Validity and reliability of the short physical performance Battery (SPPB): A pilot study on mobility in the Colombian Andes | validez y confiabilidad de la batería corta de desempeño físico (SPPB): Un Estudio piloto Sobre La Movilidad en Los Andes Colombi. Colombia Medica, 44(3), 165–171.
Gong, Y., Gallacher, J., Palmer, S., & Fone, D. (2014). Neighbourhood green space, physical function and participation in physical activities among elderly men: The Caerphilly prospective study. International Journal of Behavioral Nutrition and Physical Activity, 11(1). https://doi.org/10.1186/1479-5868-11-40.
Guedes, D. T., Alvarado, B. E., Phillips, S. P., Curcio, C. L., Zunzunegui, M. V., & Guerra, R. O. (2015). Socioeconomic status, social relations and Domestic Violence (DV) against elderly people in Canada, Albania, Colombia and Brazil. Archives of Gerontology and Geriatrics, 60(3), 492–500. https://doi.org/10.1016/j.archger.2015.01.010.
Guralnik, J. M., Simonsick, E. M., Ferrucci, L., Glynn, R. J., Berkman, L. F., Blazer, D. G., Scherr, P. A., & Wallace, R. B. (1994). A short physical performance Battery assessing lower extremity function: Association with Self-reported disability and prediction of mortality and nursing home admission. Journal of Gerontology, 49(2), M85–M94. https://doi.org/10.1093/geronj/49.2.M85.
James, B. D., Boyle, P. A., Buchman, A. S., Barnes, L. L., Bennett, D. A., James, Boyle, B. D., Buchman, P. A., Barnes, A. S., Bennett, L. L., & David (2011). Life Space and Risk of Alzheimer Disease, mild cognitive impairment, and Cognitive decline in Old Age. American Journal of Geriatric Psychiatry, 19(11), 961–969. https://doi.org/10.1097/JGP.0b013e318211c219.
Johnson, J., Rodriguez, M., Snih, S., & Al (2020). Life-space mobility in the Elderly: Current perspectives. Clinical Interventions in Aging, 15, 1665–1674.
Kono, A., Kai, I., Sakato, C., & Rubenstein, L. Z. (2004). Frequency of going outdoors: A predictor of Functional and Psychosocial Change among Ambulatory Frail elders Living at Home. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 59(3), M275–M280. https://doi.org/10.1093/gerona/59.3.m275.
Kuspinar, A., Verschoor, C. P., Beauchamp, M. K., Dushoff, J., Ma, J., Amster, E., Bassim, C., Bello-Haas, D., Gregory, V., Harris, M. A., Letts, J. E., Neil-Sztramko, L., Richardson, S. E., Valaitis, J., R., & Vrkljan, B. (2020). Modifiable factors related to life-space mobility in community-dwelling older adults: Results from the Canadian longitudinal study on aging. BMC Geriatrics, 20(1). https://doi.org/10.1186/s12877-020-1431-5.
Lanzino, D., Sander, E., Mansch, B., Jones, A., Gill, M., & Hollman, J. (2016). Life Space Assessment in spinal cord Injury. Topics in Spinal Cord Injury Rehabilitation, 22(3). https://doi.org/10.1310/sci2203-173.
Liu, M., Xue, Q. L., Gitlin, L. N., Wolff, J. L., Guralnik, J., Leff, B., & Szanton, S. L. (2021). Disability Prevention Program improves Life-Space and Falls Efficacy: A Randomized Controlled Trial. Journal of the American Geriatrics Society, 69(1), 85–90. https://doi.org/10.1111/jgs.16808.
Lu, S., Liu, Y., Guo, Y., Ho, H. C., Song, Y., Cheng, W., Chui, C. H. K., Chan, O. F., Webster, C., Chiu, R. L. H., & Lum, T. Y. S. (2021). Neighbourhood physical environment, intrinsic capacity, and 4-year late-life functional ability trajectories of low-income Chinese older population: A longitudinal study with the parallel process of latent growth curve modelling. EClinicalMedicine, 36. https://doi.org/10.1016/j.eclinm.2021.100927.
Mardini, M. T., Nerella, S., Kheirkhahan, M., Ranka, S., Fillingim, R. B., Hu, Y., Corbett, D. B., Cenko, E., Weber, E., Rashidi, P., & Manini, T. M. (2021). The temporal relationship between ecological pain and life-space mobility in older adults with knee osteoarthritis: A smartwatch-based demonstration study. JMIR MHealth and UHealth, 9(1), 1–14. https://doi.org/10.2196/19609.
Murayama, H., Yoshie, S., Sugawara, I., Wakui, T., & Arami, R. (2012). Contextual effect of neighborhood environment on homebound elderly in a Japanese community. Archives of Gerontology and Geriatrics, 54(1). https://doi.org/10.1016/j.archger.2011.03.016.
Nagi, S. Z. (1976). An epidemiology of disability among adults in the United States. The Milbank Memorial Fund Quarterly Health and Society, 54(4), 439. https://doi.org/10.2307/3349677.
Peel, C., Baker, P. S., Roth, D. L., Brown, C. J., Bodner, E. V., Allman, R. M., Baker, S., Roth, P., Brown, D. L., Brodner, C. J., E. V, & Allman, R. M. (2005). Assessing mobility in older adults: The UAB Study of Aging Life-Space Assessment. Physical Therapy, 85(10), 1008–1119. http://www.ncbi.nlm.nih.gov/pubmed/16180950.
Peña, Q. É. & Curcio Borrero, C. L. (2016). Espacio De vida y entorno del barrio en adultos mayores de 65 a 74 años del área urbana de Manizales, Colombia. Revista Márgenes No, 13(19), 21–31.
Polku, H., Mikkola, T. M., Portegijs, E., Rantakokko, M., Kokko, K., Kauppinen, M., Rantanen, T., & Viljanen, A. (2015). Life-space mobility and dimensions of depressive symptoms among community-dwelling older adults. Aging & Mental Health, 19(9), 781–789. https://doi.org/10.1080/13607863.2014.977768.
Portegijs, E., Iwarsson, S., Rantakokko, M., Viljanen, A., & Rantanen, T. (2014). Life-space mobility assessment in older people in Finland; measurement properties in winter and spring. BMC Research Notes, 7(1), 323. https://doi.org/10.1186/1756-0500-7-323.
Portegijs, E., Tsai, L. T., Rantanen, T., & Rantakokko, M. (2015). Moving through Life-Space areas and objectively measured physical activity of older people. PLOS ONE, 10(8), e0135308. https://doi.org/10.1371/journal.pone.0135308.
Portegijs, E., Rantakokko, M., Viljanen, A., Sipilä, S., & Rantanen, T. (2016). Identification of older people at risk of ADL disability using the Life-Space Assessment: A longitudinal cohort study. Journal of the American Medical Directors Association. https://doi.org/10.1016/j.jamda.2015.12.010.
Portegijs, E., Rantakokko, M., Viljanen, A., Rantanen, T., & Iwarsson, S. (2017). Perceived and objective entrance-related environmental barriers and daily out-of-home mobility in community-dwelling older people. Archives of Gerontology and Geriatrics, 69, 69–76. https://doi.org/10.1016/j.archger.2016.11.011.
Rantakokko, M., Iwarsson, S., Manty, M., Leinonen, R., & Rantanen, T. (2012). Perceived barriers in the outdoor environment and development of walking difficulties in older people. Age and Ageing, 41(1), 118–121. https://doi.org/10.1093/ageing/afr136.
Rantakokko, M., Iwarsson, S., Portegijs, E., Viljanen, A., & Rantanen, T. (2015). Associations between Environmental characteristics and life-space mobility in Community-Dwelling Older people. Journal of Aging and Health, 27(4), 606–621. https://doi.org/10.1177/0898264314555328.
Rantakokko, M., Portegijs, E., Viljanen, A., Iwarsson, S., Kauppinen, M., & Rantanen, T. (2016). Changes in life-space mobility and quality of life among community-dwelling older people: A 2-year follow-up study. Quality of Life Research, 25(5). https://doi.org/10.1007/s11136-015-1137-x.
Roadolff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
Satariano, W. A., Guralnik, J. M., Jackson, R. J., Marottoli, R. A., Phelan, E. A., & Prohaska, T. R. (2012). Mobility and aging: New directions for public health action. American Journal of Public Health. https://doi.org/10.2105/AJPH.2011.300631.
Sawyer, P., & Allman, R. M. (2010). Resilience in mobility in the context of chronic disease and aging: Cross-sectional and prospective findings from the University of Alabama at Birmingham (UAB) study of aging. In New Frontiers in Resilient Aging: Life-Strengths and Well-Being in Late Life (pp. 310–339). https://doi.org/10.1017/CBO9780511763151.014.
Sheppard, K. D., Sawyer, P., Ritchie, C. S., Allman, R. M., & Brown, C. J. (2013). Life-space mobility predicts nursing home admission over 6 years. Journal of Aging and Health. https://doi.org/10.1177/0898264313497507.
Shimada, H., Sawyer, P., Harada, K., Kaneya, S., Nihei, K., Asakawa, Y., Yoshii, C., Hagiwara, A., Furuna, T., & Ishizaki, T. (2010). Predictive validity of the classification Schema for Functional mobility tests in Instrumental activities of Daily Living decline among older adults. Archives of Physical Medicine and Rehabilitation. https://doi.org/10.1016/j.apmr.2009.10.027.
Snih, S., Al, Peek, K. M., Sawyer, P., Markides, K. S., Allman, R. M., & Ottenbacher, K. J. (2012). Life-space mobility in Mexican americans aged 75 and older. Journal of the American Geriatrics Society. https://doi.org/10.1111/j.1532-5415.2011.03822.x.
Stalvey, B. T., Owsley, C., Sloane, M. E., & Ball, K. (1999). The Life Space Questionnaire: A measure of the extent of mobility of older adults. Journal of Applied Gerontology. https://doi.org/10.1177/073346489901800404.
Swets, J. A. (1998). Measuring the Accuracy of Diagnostic Information. Science, 40, 1285–1293. https://doi.org/10.1002/9781118341544.ch5.
Taylor, J. K., Buchan, I. E., & van der Veer, S. N. (2018). Assessing life-space mobility for a more holistic view on wellbeing in geriatric research and clinical practice. Aging Clinical and Experimental Research. https://doi.org/10.1007/s40520-018-0999-5.
Tran, Y., Hashimoto, N., Ando, T., Sato, T., Konishi, N., Takeda, Y., & Akamatsu, M. (2022). Associations between motorized transport access, out-of-home activities, and life-space mobility in older adults in Japan. Bmc Public Health, 22(1), 1–11. https://doi.org/10.1186/s12889-022-13033-y.
Ullrich, P., Werner, C., Eckert, T., Bongartz, M., Kiss, R., Feißt, M., Delbaere, K., Bauer, J. M., & Hauer, K. (2018). Cut-off for the Life-Space Assessment in persons with cognitive impairment. Aging Clinical and Experimental Research. https://doi.org/10.1007/s40520-018-1062-2.
Wong, P. H., Kourtit, K., & Nijkamp, P. (2021). The ideal neighbourhoods of successful ageing: A machine learning approach. Health and Place, 72(September), 102704. https://doi.org/10.1016/j.healthplace.2021.102704.
Yamasaki, M., & Someya, F. (2015). Seasonal changes in activity levels among nursing care insurance service users in areas with different climates. Journal of Physical Therapy Science, 27(3), 929–932. https://doi.org/10.1589/jpts.27.929.
Yardley, L., Beyer, N., Hauer, K., Kempen, G., Piot-Ziegler, C., & Todd, C. (2005). Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age and Ageing, 34(6), 614–619. https://doi.org/10.1093/ageing/afi196.
Zunzunegui, M. V., Cuadra, P. G., Béland, F., Del Ser, T., & Wolfson, C. (2000). Development of simple cognitive function measures in a community dwelling population of elderly in Spain. International Journal of Geriatric Psychiatry, 15(2), 130–140. https://doi.org/10.1002/(SICI)1099-1166(200002)15:2%3C130::AID-GPS91%3E3.0.CO;2-C.
Funding
Open Access funding provided by Colombia Consortium
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This study was approved by the ethics committees of each site. Informed consent Written informed consent was obtained from all subjects before their participation.
Conflict of Interest
The authors declare that there are no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Curcio, CL., Pérez-Trujillo, M., Gomes, C. et al. Cutoffs to Identify Restricted Life-space Mobility in Older Adults Across Different Contexts: The International Mobility in Aging Study. Ageing Int 49, 374–389 (2024). https://doi.org/10.1007/s12126-023-09553-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12126-023-09553-6