
Abstract
We investigated if cultural activities are associated with improved quality of life experiences of older people. In 2012, older people in five care units were invited to participate more cultural activities (study group) than usual. Each person in the study group had a tailored cultural plan integrated into the care plan. Older people in traditional care units (control group) did not have such cultural plans.
One hundred sixty-one persons from care units in two cities in Finland participated in 2012 and 161 persons in 2014 in a cross-sectional study. Their quality of life was assessed with the World Health Organization’s Quality of Life WHOQOL-BREF (Field Tríal Version) enquiry. The quality of life variable contained four domains: physical, psychosocial, social and environment. The values of these domains underwent multivariate analysis of variance of the following explanatory variables: intervention group, age (</= to 80 compared to >80 years old), education background, marital status, gender and comorbidities. The domains of the participants’ self-rated experience were also assessed.
The quality of life experience was similar at baseline in 2012 in both study groups. In 2014 the study group rated the quality of life (p<0.0001 respectively) and satisfaction with health (p=0.001 respectively) higher than the control group.
Older people in care units need cultural activities as a necessary part of their care. The care provided in the care units does not put enough emphasis on this need. With individually tailored cultural activities set down in a cultural plan, care providers can ensure a better quality of life for older people.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
People over 65 years old are the growing age group in the decades to come in Finland. In 2010 people above age 64 constituted 17,5% of the population and in 2020 no less than 23,7%. This proportion will increase until 2070 (Official Statistics of Finland 2018). Aging can be considered to be a process of adaptation of the human being to individual changes rather than only changes in physical activity, psychological function and social function (Nosraty et al. 2015; Faber et al. 2001). Aging maybe be defined as referring to persons older than 71 to 80 years, 75 years or 85 years (Cohen-Mansfield et al. 2013). We use term older people as defined under Data and methods below.
Well-being, life satisfaction, empowerment and quality of life (QOL) are often used terms in studies on cultural activities and arts. (Hallam et al. 2014) “QOL in old age” is a term often used in studies among older people and QOL. QOL in old age as regards general well-being may be defined as a subjective state characterized by the attributes life satisfaction and emotional balance. These attributes mirror the degree satisfaction of fulfilled underlying needs and are remain stable by the individual’s adaptation to gradually deteriorating life conditions (Boggatz, 2014). Ettema et al. (2005) conceptualized QOL in terms of dementia (according to Lawson): “quality of life is defined in so many ways by so many people and, regrettably, often is not defined.” In our study we use The World Health Organization’s (WHO) definition of quality of life. WHO (1996) defines quality of life as an individual’s perception of his or her position in life in the context of the culture and value systems in which he or she lives and in relation to goals, expectations, standards and concerns. The definition is comprehensive and it encompasses a person’s physical health, psychological state, social relationships and their relationship as a salient feature of his or her environment in a complex way (WHO 1996). Regardless of the state of living or health, an individual’s right to enjoy art and to be part of the community’s cultural life is emphasized in several declarations and programs (United Nations Educational, Scientific and Cultural Organization (UNESCO) 1966, 1982, 1996; in Finland Liikanen 2010; Koponen et al. 2017). Creating possibilities for older people to be engaged one’s meaningful activities is ensured in Finland by law (Finlex, 2012).
In WHO’s review the role of arts lies in improving health and well-being (2019) and in producing emotional, imaginative and creative experiences for the actors, the artists and the audience. According to the study of Nenonen et al. (2014) the cultural activities were associated with self-rated health and quality of life. In several studies cultural activities enhance the quality of life or well-being (Gelo et al. 2015, Hannemann 2006). In the study of Davies et al. (2012) engagement in arts is described as engagement in five categories of art practices: performing arts; visual arts, design and craft; literature; culture; and digital and electronic arts. A person can participate actively or non-actively (by looking and listening) in arts, depending on his or her state of health. Due to the wide variety of arts we defined here, as we have done previously (Koponen et al. 2017), art as being engaged with different cultural activities, based on the older adult’s own choices in harmony with the specific cultural plan of the care unit. Cultural activities in our study include a range of art forms from performing arts to non-performing arts (theatre visits, concerts, poetry, music, literature etc.). These art services are provided to the older adult with consideration of his or her ability to function and experience. The participants included the oldest of the older adults who still enjoyed engagement with cultural activities despite deteriorating cognition and physique. The main result of our previous study (Koponen et al. 2017) was that by attending cultural events older people are able to influence their quality of life and are distanced from just being an object of care. Their feeling of well-being increases and their feeling of loneliness decreases.
In this and in our previous study (Koponen et al. 2017) we defined art as being engaged with different cultural activities of older adult’s own choice based to the individual cultural plan. Cultural activities include various art forms from performing arts to non-performing arts. The participants of our study group are the older adults who still enjoy engagement to cultural activities if activities are provided in the care units despite their deteriorating cognition and physical condition.
Being old does not necessarily mean poor physical activity, but it may mean being active and achieving the goals in late life, as well (Yeung and Breheny 2016; Persson et al. 2001). Poor health can restrict being engaged in activities, but it does not necessarily affect the experience of well-being (Yeung and Breheny 2016). For older people, good health means being active and being able to function.
Psychological health influences quality of life. Supportive activity within social networks, such as meeting friends and participating in cultural activities, are positively associated with life satisfaction and longevity (Koponen et al. 2017; Helvik et al. 2011; Forssén, 2007; Koonlaan et al. 2000, 1996). Older people in hospital care have an increased risk of dissatisfaction when social connections and participation in activities are reduced (Helvik et al. 2011).
In our previous study, we have reported our results of the cultural activities in culture study groups started in 2011 by a project called Cultural plans for senior citizens (Koponen et al. 2017). The results of the experienced quality of life were modest in the group that enjoyed cultural activities (study group) because of the short time of cultural endeavors, since the observation period ended already in 2012. Changes in the study group’s organizational culture, attitudes and implementation of the cultural plan in care took time and the results in quality of life experiences were clearly emerging in three years by 2014, as we report in this paper. The objective of this study was to examine if cultural activities in the everyday life of older people living in care units result better quality of life than if such activities are not provided.
Data and Methods
The data were collected from 15 care units for older people of two healthcare-providing organizations in two different cities (Oulu and Turku) in Finland in 2012 and 2014. The care units were managed by the municipal, public health. The two participating cities are located 600 km apart in Finland; their demographic structure and care provision is similar. Both cities rank among the six biggest cities in Finland (Finnish institute for health and welfare (THL) 2017). During the study time, the criteria for acquiring municipal long-term care (LTC) service were tightened in both cities. The units used uniform criteria for approving tenants and the care provided was based on nationally approved principals for old people care. The older people who entered the study were more frail and had a higher number of illnesses than before as a consequence of the tightened criteria. They had an increased need of help in their daily activities or were not able to live at home with the care provided. This change in patient allocation meant that shorter times were spent in the care units at the end of the life than before; these units were the last homes for the participants who required 24-hour care. Our study focused on the differences in the experienced quality of life between the group of older people who were provided with cultural activities (study group) compared to who were not (control group).
Age was not the primary variable, but study participants were recruited by the following criteria: the participant was orientated in time and location, was able to communicate and understood the purpose of the study. The exclusion criteria were: the person was not orientated in time and location and could not understand the purpose of the study due to the health condition. In the study group and the control group, participants aged 80 years or more formed more than half of the study population (Table 1). Poor health was the main reason for the need for institutional 24-hour care. In the control group, the staff had no systematic way of documenting individual wishes of cultural or personal activities into the care plan, while each participant in the study group had an individually tailored cultural plan attached into the care plan. The cultural plan is a document that defines the cultural activities (e.g., theatre visits, concerts, poetry and other art forms) that are considered important by the study participant (intervention) and which he or she wanted experience in the daily life of the care unit (Koponen et al. 2017).
At baseline in 2012 and 2 years later, the study population was interviewed by using the WHOQLY-BREF (Field trial Version) questionnaire. At baseline, 19 participants out of 78 (24%) in the study (culture) group had one year of experience of systematically planned and arranged cultural activities provided by the developmental project of the European Culture Capital year 2011 program (Koponen et al. 2017). The participants of the control group were provided with a regular level of care which included social and diversional activities suited for older people.
Assessment of Quality of Life
We used the WHO WHOQOL-BREF (Field Trial Version) quality of life questionnaire (WHO 1996), which is internationally used in life quality studies. The WHOQOL-BREF is an abbreviated version of the WHOQOL-100 developed by the WHO WHOQOL Group. WHOQOL-BREF consists of 26 questions in four domains: physical health (7 questions), psychological health (6), social relationships (3) and living environment (8) (WHO 1996). The two first questions measure the respondent’s own evaluation of his or her general health status and quality of life. The question of the WHOQOL rely on quality of life as a multidimensional concept with both positive and negative aspects (Sapouna and Orley 1997). The questions are answered on a Likert scale from 1 to 5.
The WHOQLY-BREF questionnaire’s four domains give a reliable description of how the study population experience their present quality of life in care units. The experience of having the opportunity to enjoy activities is significant in our study. In the physical domain, a feeling of energy for daily life, the quality of sleep and the degree of satisfaction with one’s ability to perform daily activities give answer to the quality of life experience. The psychosocial domains concern enjoying life, meaningful life experience, satisfaction with oneself and having negative feelings like depression, despair, blue mood and anxiety. The social domains questions concern personal relationships, social support and sexual activity. Environment domain relates to the living environment.
The WHOQOL-BREF (Field Trial Version) has been validated in Finland by the National Research and Development Centre for Welfare and Health (2019). The WHOQOL-BREF (Field Trial Version) questionnaire can be filled in either by the respondent alone or by an interviewer. In this study we used the latter way in 2012 and 2014 due to the high age, multiple chronic diseases and the weakened hearing or sight of the respondents.
In Finland, the average time spent in LTC units before death was less than one month in 2012 and 2014 (THL2017). Due to the advanced age, multiple chronic diseases and high mortality of our study subjects, the study population varied during the research process. Two years can be considered a long follow-up time in this study group (Koponen et al. 2017). Most interviews were carried out by one of the authors (TK). The participants’ background information was collected from the medical records by the nursing personnel and by TK.
The data are summarized as counts and percentages or as means and standard deviations (SD) added by median for WHOQOL-BREF, questions 1 and 2. Fisher’s exact test was used to compare categorical background variables of the groups (Table 1). All comparisons were made separately for 2012 and 2014, because most of study participants were different at 2012 and 2014. Self-rated experience WHOQOL-BREF, questions 1 and 2 in, Likert scale 1–5 were analyzed separately for 2012 and 2014 with Wilcoxon rank sum test (Table 2).
The WHOQOL-BREF dimensions were analyzed separately for 2012 and 2014 with multi-way analysis of variance, which included the following explanatory variables: intervention group, age class (</= to 80 compared to >80 years old), education background, marital status, gender and diagnoses (Table 3 and supplementary table). All statistical tests were performed 2-tailed, with a significance level set at 0.05. The analyses were performed using the SAS System, version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA).
Ethical Considerations
The involved organizations granted research permissions: The University of Turku ethical permission 20/2011, the city of Turku 16/10 (25.11.2011) and the city of Oulu city §32 (29.2.2012). All participants were informed of the study before the interview and written consent was obtained. The participants were also informed of the option to withdraw from the study at any time during the interview. All information was handled confidentially.
Results
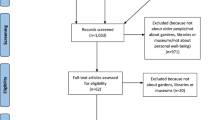
One hundred sixty-one subjects participated in the study in 2012 and 161 subjects in 2014. Some individuals participated on both occasions, but due to high mortality in this age group 37 (23%) of the participants were the same in 2012 and in 2014. In 2012, the mean age of the participants was 83 years and in 2014 it was 85. Of the participants in 2012, 70% were 80 years or older, in 2014 the figure was 76%. In 2012 the proportion of participants over 80 years in the control group was 76% and in intervention group 64%; in 2014 the figures were 76% and 77%. Most participants were female in both groups, married or widows. The prevalent education level was primary school or less. Most participants had at least three chronic diseases (Table 1).
In 2012, more participants in the control group than in the study (culture) group had at least 3 chronic diseases (p=0.010), which was associated with a more severe feeling of morbidity (p<0.001). In 2014, but not in 2012, the participants in culture group were more educated than in the control group (p<0.001). Otherwise the background factors did not differ significantly between the groups.
The study population was homogeneous regarding overall morbidity (Appendix I). Most participants in both groups had diseases of the circulatory and nervous system. The frequency of mental and behavioral diseases, including Alzheimer’s disease and other memory diseases, was similar in 2012 in both groups (28% in the control group and 31% in the culture group), but in 2014 there was a significant difference of p=0.016 (39% in the control group and 21% in the culture group) (Appendix I).
The question “Do you feel that you are ill?” was answered “yes” by 41% in the control group and by 73% in the culture group in 2012. The corresponding figures were 52% and 67%. in 2014. Less participants in the culture group felt ill in 2014 than in 2012 (27% and 33%, respectively), i.e., after some two years of access to cultural activities in their daily life, as stated in the cultural plan (Table 1).
In 2012 the mean quality of life score was 3.2 (SD 0.8) in the control group and 3.3 (SD 0.8) in the study group (on the Likert scale 1–5 in WHOQOL-BREF) (p=0.23). In 2014, the study group rated the quality of life higher than the control group: 3.7 (SD 0.9) and 3.0 (SD 0.8), respectively (p<0.001). In 2012, the mean score for how satisfied participants were with their health was 3.5 (SD 1.0) in the study group and 3.1 (SD 1.1) in the control group (p=0.006).
In 2014, the study group rated satisfaction with health significantly higher than the control group 3.8 (SD1.1) vs. 3.2 (SD1.2), respectively (p<0.001) (Table 2).
Based on the domains on the WHOQOL-BREF interview the overall experience of the respondents’ quality of life was similar at baseline in the study and control group in 2012. There were, however, significant differences in the psychological, social and environmental domains in 2012 (p=0.0062, p<0.001, p<0.001 respectively): the culture group had a higher mean in all these domains, but not in the physical domain (p=0.33). In 2014, the experience of the quality of life differed between the groups in all four dimensions. Looking at the domains, the study group experienced better quality of life in all the domains -physical (p <0.001), psychosocial (p <0.001), social (p=0.033) and environment (p <0.001) domains (Table 3).
Discussion
We studied older people in poor health. The most significant result is that the experienced quality of life and health satisfaction were significantly better in the study group than in the control group in 2014 but not in 2012. Participants in the study group followed an individually tailored culture plan, which included cultural activities, hobbies and other elements which the subjects themselves perceived as being important for them in their lives. Caspari et al. (2018) point out that older people feel loosing their autonomy in nursing homes when are not able to maintain important hobbies or habits in the care unit. When personal wishes and needs are fulfilled through individually planned activities, the quality of life improves as the sense of meaning and purpose in life is strengthened (Drageset et al. 2017; Frändin et al. 2016). Kontos (2003) points out that, in Alzheimer’s disease, some agency is retained although memory fails gradually. Unruh (1983) emphasizes the importance of the social environment for old people. Social activities, like dancing, biking and arts, are strongly influenced by the institutional level and the variation of human interaction. In a previous study, we have showed that older people living in care units are active actors and participate in the interactions of the unit where they are live. The personnel and other people at the unit create a characteristic social world with its daily routines involving care, meals and scheduled leisure time activities. Meaningful activities and a tailored cultural plan ensure that the individual can experience his or her last years, months or weeks of life as satisfying and significant (Koponen et al. 2017).
The number of chronic diseases did not affect significantly the experienced quality of life (Table 1). The study group felt less ill after two years, but the opposite was true for the control group. In the study group fewer participants felt ill in 2014 after having participated in cultural activities and more felt satisfied with their health. This was the case despite the fact they were older and had more diseases than the groups in 2012.
The WHOQOL-BREF questionnaire evaluates also self-rated health by asking “How would you rate your quality of life” and “How satisfied are you with your health”. Our results demonstrate the importance of having cultural activities as part of the daily life of older people in care units. According to the study of Yeung and Thang LTC units are encouraged to emphasize on enabling activities to meet older people’s personal choices and function ability (Yeung and Thang, 2018). The WHOQOL-BREF is cross-culturally validated questionnaire with the domains physical, psychological, social and environment (Skevington et al 2004).
In the classical study of Matarasso (2009) participants attending arts projects experienced increased quality of life. Compared to several earlier, our study had a unique setup, since of older people participated in the study, carried out a self-evaluation of their quality of life in the care unit. This evaluation is valuable and adds to existing data, because it conveys the personal, subjective experience of each respondent.
We compared the differences in the experienced quality of life between a group of older people with cultural activities integrated into the care plan with a control group of older people with no planned cultural activities. One of the strengths of this study is that it involved the oldest of older people in care unit setting, and they had similar chronic diseases and age range as Finnish older people in care units overall. Interobserver variably was minimized by interviews having been made mostly by one and the same person, one of the authors.
Limitations
The study population changed from 2012 to 2014 due to the mortality and morbidity characteristic for this age group. Follow-up for two years of the same individuals was not possible. Instead, the study data was managed cross-sectionally and data from 2012 to 2014 was analyzed separately. During the study, the criteria for older people care in both cities started to focus on older people in a poor medical condition. Due to this change, the tenants lived for shorter times in the care units than before the change of criteria. Nor did everyone in the study group have the opportunity to participate in the cultural activities of their liking due to the rapidly changing study population. But most participants in the study group did have the possibility to participate, at least partly, in some of the several cultural activities offered. We did not record the quantity of culture and leisure activities the participants had been involved in during the study. Thus, it was not possible to evaluate the amount of cultural activities required for a person to experience a better quality of life.
Conclusions
The results of this study show how important it is to understand older people’s ability to enjoy various cultural activities even at the very end of life. Being able to participate in cultural activities by one’s own choice has connections to the quality of life experience. Older people value their quality of life better when they can decide whether and which cultural activities are introduced into their daily lives. Individual care with a cultural plan ensures that important and appealing cultural activities can be introduced into the care of older people. The number of chronic diseases does not significantly influence the quality of life.
This study establishes the value of cultural activities for inhabitants in older people’s care institutions. The question of cultural activities and experiences of quality of life should next be broadened to older people living at home with assisted care.
References
Boggatz, T. (2014). Quality of life in old age – a concept analysis. International Journal of Older People Nursing, 11, 55–69. DOI: https://doi.org/10.1111/opn.12089. https://pubmed-ncbi-nlm-nih-gov.ezproxy.utu.fi/26118350/
Bygren, L. O., Koonlaan, B. B., & Johansson, S. E. (1996). Attendance at cultural events, reading books or periodicals, and making music or singing in a choir as determinants for survival: Swedish interview survey of living conditions. British Medical Journal, 313, 1577–1580. https://doi.org/10.1136/bmj.313.7072.1577
Caspari, S., Råholm, M. B., Sætere, B., et al. (2018). Tension between freedom and dependence—A challenge for residents who live in nursing homes. Journal of Clinical Nursing, 27, 4119–4127. https://doi.org/org.ezproxy.utu.fi/10.1111/jocn.14561
Cohen-Mansfield, J., Shmotkin, D., Blumstein, Z., Shorek, A., Eyal, N., & Hazan, H. (2013). The old, old-old, and the oldest old: continuation or distinct categories? An examination of the relationship between age and changes in health, function, and wellbeing. International Journal of Aging and Human Development, 77, 37–57. http://org.ezproxy.utu.fi/10.2190%2FAG.77.1.c
Davies, C. R., Rosenberg, M., Knuiman, M., Ferguson, R., Pikora, T., & Slatter, N. (2012). Defining arts engagement for population-based health research: Art forms activities and level of engagement. Arts & Health, 4(3), 203–216. https://doi.org/10.1080/17533015.2012.656201
Drageset, J., Haugan, G., & Tranvåg, O. (2017). Crucial aspects promoting meaning and purpose in life: perceptions of nursing home residents. BMC Geriatrics, 17, 254–263. https://doi.org/10.1186/s12877-017-0650-x. https://bmcgeriatr.biomedcentral.com/articles/
Ettema, T. P., Dröes, R. M., de Lange, J., Ooms, M. E., Mellenbergh, G. J., & Ribbe, M. W. (2005). The concept of quality of life in dementia in the different stages of the disease. International Psychogeriatrics, 17(3), 353–370
Faber, M., Gussekloo, J., & Knook, D. L. (2001). Successful aging in the oldest olds. Who can be characterized as successfully aged? Internal Medicine, 161, 2694–2700. https://jamanetwork-com.ezproxy.utu.fi/journals/jamainternalmedicine/fullarticle/752299
Ministry of Justice (2012). Act on supporting the functional capacity of the older population and on social and health services for older persons. Retrieved September 11, 2020, from http://www.finlex.fi/en/laki/kaannokset/2012/en20120980
Finnish institute for health and welfare (THL) (2019). The WHOQLY-BREF (Field Version) questionnaire. Retrieved June 24, 2019, from https://thl.fi/en/web/functioning/toimia-functioning-measures-database
Finnish institute for health and welfare (THL) (2017). The statistical facts on the elderly care and population in Finland. Retrieved June 27, 2017, from https://sotkanet.fi/sotkanet/en/index
Forssén, A. K. (2007). Humour, beauty, and culture as personal health resources: Experiences of elderly Swedish women. Scandinavian Journal of Public Health, 35, 228–234. https://journals-sagepub-com.ezproxy.utu.fi/doi/pdf/10.1080/1403494060116068
Frändin, K., Grönstedt, H., Helbostad, J. L., et al. (2016). Long-Term Effects of Individually Tailored Physical Training and Activity on Physical Function, Well-Being and Cognition in Scandinavian Nursing Home Residents: A Randomized Controlled Trial. Gerontology, 62, 571–580. https://doi.org/10.1159/000443611
Gelo, F., Klassen, A. C., & Gracely, E. (2015). Patient use of images of artworks to promote conversation and enhance coping with hospitalization, Arts & Health, 7(1),42–53. https://doi.org/10.1080/17533015.2014.961492
Hallam, S., Creech, A., Varvarigou, M., McQueen, H., & Gaunt, H. (2014). Does active engagement in community music support the well-being of older people? Arts&Health, 6, 101–106. https://doi.org/10.1080/17533015.2013.809369
Hannemann, B. T. (2006). Creativity with Dementia Patients Can Creativity and Art Stimulate Dementia patients Positively? Gerontology, 52:59–65. https://www-proquest-com.ezproxy.utu.fi/docview/70703662?pq-origsite=primo
Helvik, A. S., Engedal, K., Krokstad, S., & Selbaek, G. (2011). A comparison of life satisfaction in elderly medical inpatients and the elderly in a population-based study: Nord-Tro/ndelag Health Study 3. Scandinavian Journal of Public Health, 39, 337–344. https://journals-sagepub-com.ezproxy.utu.fi/doi/pdf/10.1177/1403494811405093
Kontos, P. (2003). ‘‘The painterly hand’’: embodied consciousness and Alzheimer’s disease. Journal of Aging Studies, 2, 151–170. https://doi.org/10.1016/S0890-4065(03)00006-9
Koonlaan, B. B., Bygren, L. O., & Johansson, S. E. (2000). Visiting the cinema, concerts, museums or art exhibitions as determinant of survival: a Swedish fourteen-year cohort follow-up. Scandinavian Journal of Public Health, 28, 174–178. https://journals-sagepub-com.ezproxy.utu.fi/doi/pdf/10.1177/14034948000280030501
Koponen, T., Honkasalo, M. L., & Rautava, P. (2017). Cultural plan model: Integrating cultural and creative activities into care units for the elderly. Arts&Health, 10, 65–71. https://doi.org/10.1080/17533015.2017.1315436
Liikanen, H. L. (2010). Art and Culture for Well-being: Proposal for an action programme 2010–2014. Retrieved April 14, 2018, from https://urn.fi/URN:ISBN:978-952-485-918-9
Matarasso, F. (2009). Use or ornament? The social impact of participation in the Arts. Retrieved July 20, 2011, from https://www.disseminate.net.au/files/webfiles/OrnamentMatarasso.pdf
Nenonen, T., Kaikkonen, R., Murto, J., & Luoma, M. L. (2014). Cultural services and activities: The association with self-rated health and quality of life. Arts & Health, 6(3), 235–253. https://doi.org/10.1080/17533015.2014.897958
Nosraty, L., Jylhä, M., Raittila, T., & Lumme-Sand, K. (2015). Perceptions by the oldest old of successful aging, Vitality 90+ Study. Journal of Aging Studies, 32, 50–58. https://doi.org/10.1016/j.jaging.2015.01.002
Official Statistics of Finland (OSF) (2018). Population projection. Retrieved November 28, 2019, from https://www.stat.fi/til/vaenn/2018/vaenn_2018_2018-11-16_tau_001_fi.html
Persson, G., Boström, G., Allebeck, P., et al. (2001). Elderly People’s Health – 65 and After. Scandinavian Journal of Public Health 2001; Supplement 58: 117–131. https://journals-sagepub-com.ezproxy.utu.fi/doi/pdf/10.1177/14034948010290032901
Sapouna, S., & Orley, J. (1997). Quality of life assessment: the World Health Organization perspective. Eur Psychiatry, 12(S3), 263s–266s. https://doi.org/10.1016/S0924-9338(97)89095-5
Skevington, S. M., Lotfy, M., & O’Connell, K. A. (2004). The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial A Report from the WHOQOL Group. Quality of Life Research, 13, 299–310. https://link-springer-com.ezproxy.utu.fi/article/10.1023/B%3AQURE.0000018486.91360.00
United Nations Educational, Scientific and Cultural Organization (UNESCO) (1982). World Conference on Cultural Policies. Final Report. Retrieved September 9, 2020, from https://unesdoc.unesco.org/ark:/48223/pf0000052505
United Nations Educational, Scientific and Cultural Organization (UNESCO) (1966). Universal Declaration on Cultural Diversity. Retrieved August 17, 2018, from https://unesdoc.unesco.org/images/0010/001035/103546Eb.pdf
United Nations Educational, Scientific and Cultural Organization (UNESCO) (1996). Culture and Health Orientation Texts on the 1996 theme. Retrieved August 17, 2018, from https://unesdoc.unesco.org/search/28a33765-e1d0-4b65-9bf8-e20851d460c8
Unruh, D. (1983). Invisible lives. Social Worlds of the Aged. Sage Publications
World Health Organization (WHO). (1996). WHOQOL-BREF Introduction, Administration, Scoring and Generic version of the Assessment. Field trial Version, December 1996. Programme on Mental Health Retrieved February 24, 2016, from https://www.who.int/mental_health/publications/whoqol/en/
World Health Organization (WHO) (2019). Health Evidence Network synthesis report 67. Retrieved August 26, 2020, from https://www.euro.who.int/en/data-and-evidence/evidence-informed-policy-making/publications/2019/what-is-the-evidence-on-the-role-of-the-arts-in-improving-health-and-well-being-a-scoping-review-2019
Yeung, P., & Breheny, M. (2016). Using the capability approach to understand the determinants of subjective well-being among community-dwelling older people in New Zealand. Age and Ageing, 45, 292–298. https://doi-org.ezproxy.utu.fi/10.1093/ageing/afw002
Yeung, W. J. J., & Thang, L. L. (2018). Long-Term Care for Older Adults in ASEAN Plus Three: The Roles of Family, Community, and the State in Addressing Unmet Eldercare Needs. Journal of Aging and health, 30(10), 1499–1515. https://oce-ovid-com.ezproxy.utu.fi/article/01220459-201830100-00001/HTML
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Open Access funding provided by University of Turku (UTU) including Turku University Central Hospital.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Tuulia Koponen, Eliisa Löyttyniemi, Marja-Liisa Honkasalo and Päivi Rautava. The first draft of the manuscript was written by Tuulia Koponen and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no potential conflict of interest.
Ethical treatment of subjects
Informed consent was obtained from participants and the study complies with all ethical requirements.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Appendix I
Appendix I
The top five ICD 10 classification (International Statistical Classification of Diseases and Related Health Problem) of diagnosis described with number of subject with diagnosis group and proportion in 2012 and 2014.
ICD 10 | Culture group 2012 (n=78) n (%) | Control group 2012 (n=83) n (%) | p-value | Culture group 2014 (n=81) n (%) | Control group 2014 (n=80) n (%) | p-value |
|---|---|---|---|---|---|---|
Endocrine, nutritional and metabolic diseases. Code range E00-E90 | 21 (27) | 17 (20) | 0.36 | 23 (28) | 28 (35) | 0.40 |
Mental and behavioral diseases. Code range F00-F99 | 24 (31) | 23 (28) | 0.73 | 17 (21) | 31 (39) | 0.016 |
Diseases of nervous system. Code range G00-G99 | 37 (47) | 35 (42) | 0.53 | 31 (38) | 38 (48) | 0.27 |
Diseases of circulatory system. Code range I00-I99 | 54 (69) | 66 (80) | 0.15 | 62 (77) | 59 (74) | 0.72 |
Diseases of musculoskeletal system and connective tissue. Code range M00-M99 | 14 (18) | 25 (30) | 0.097 | 18 (22) | 21 (26) | 0.59 |
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koponen, T., Löyttyniemi, E., Arve, S. et al. Experienced Quality of Life and Cultural Activities in Elderly Care. Ageing Int 48, 452–464 (2023). https://doi.org/10.1007/s12126-022-09483-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12126-022-09483-9