
Abstract
Purpose
Colorectal cancer (CRC) is one of the most common malignancies, with a high incidence and mortality worldwide. Methylated Septin 9 (mSEPT9) has been used clinically as an auxiliary tool for CRC screening. The aim of the present study was to investigate the association of the methylenetetrahydrofolate reductase (MTHFR) rs1801133 polymorphism with the risk of CRC and the methylation status of Septin 9 in CRC.
Methods
Information of 540 patients with a confirmed diagnosis of CRC and with a physical examination were utilized to assess the association of the MTHFR rs1801133 polymorphism with CRC and the methylation of SEPT9. MTHFR rs1801133 polymorphism was genotyped using polymerase chain reaction (PCR). The commercial Septin 9 Gene Methylation(mSEPT9) Detection Kit was used for plasma SEPT9 methylation analysis.
Results
Among 540 patients, 61.48% were men and the median age was 54.47 ± 13.14. 65.37% of all colorectal tumors developed in the rectum. 195 patients had negative mSEPT9 methylation, while 345 had positive results. 87 individuals with stage I, 90 with stage II, 287 with stage III, and 76 with stage IV colorectal cancer were included in the sample. The results demonstrated that the positivity rate and degree of methylation of mSEPT9 were remarkably higher in patients with more advanced TNM stages than in those with less advanced stages. The frequencies of the MTHFR rs1801133 CC genotype and allele C carriers in patients with CRC were significantly higher than those in healthy individuals (P = 0.006 and P = 0.001, respectively). The positivity rate of the mSEPT9 assay was significantly higher among the MTHFR rs1801133 TT genotype and allele T carriers than among the CC and allele C carriers respectively. The MTHFR rs1801133 TT genotype and allele T carriers were positively associated with the methylation of SEPT9 (OR = 3.320, 95% CI 1.485–7.424, P = 0.003 and OR = 1.783, 95% CI 1.056–3.010, P = 0.030, respectively).
Conclusion
In conclusion, individuals harboring the MTHFR rs1801133 CC genotype had a higher risk of CRC and the MTHFR rs1801133 TT carriers were more susceptible to Septin 9 gene methylation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is one of the most common cancers of the gastrointestinal tract. In 2020, there were more than 1.9 million estimated new cases of CRC, with approximately 935,000 deaths due to CRC [1], and its incidence and mortality rates are rising in Asian countries, posing a serious health threat [2].
Single nucleotide polymorphisms (SNPs) are found in a large number of genes linked to different forms of cancer [3]. Risk-associated SNPs for cancer are often found in the genes that control the cell cycle, DNA repair, immunity, and cellular metabolism [4]. SNPs in the promoter region affect DNA methylation, histone modification, transcription factor binding, and promoter activity, such as MMP-1 rs1799750 [5]. SNPs in the intron region frequently influence mRNA splicing, genomic imprinting and chromatin looping, such as IRF4 rs12203592 [6], H19 rs2839698 [7]. SNPs in the 3’UTR region typically impact target gene post-transcriptional levels by changing binding to miRNAs; and exon SNPs on exons may impact protein-protein interactions through changing amino acid sequences, such as MTHFR rs1801133 [8]. It may be possible to establish potential biomarkers for determining the long-term risk of CRC by identifying the genetic components that raise an individual’s risk of developing CRC.
The rs1801133 polymorphism of MTHFR is the most common mutation that decreases the enzymatic activity of MTHFR in folate metabolism. MTHFR rs1801133 polymorphisms can affect its activity, resulting in a reduction in 5-methyltetrahydrofolate production. 5-methyltetrahydrofolate acts as a methyl donor and participates in homocysteine regulation, methylation reactions, nucleotide synthesis, DNA synthesis, and repair [9]. This polymorphism results in hyperhomocysteinemia, reduced folate levels, several cardiovascular diseases, cancer, neural tube defects, pregnancy complications, and psychiatric diseases [10, 11]. In contrast, 5-methyltetrahydrofolate affects carcinogenesis by regulating the methylation of CpG sites in the promoter regions of specific genes [12]. A study on a Chinese population [13] and Iranian women [14] found that MTHFR rs1801133 TT and CT genotypes were associated with a higher incidence of breast cancer than the CC genotype. While, MTHFR rs1801133 TT has been associated with a lower risk of CRC [15].The MTHFR rs1801133 TT genotype has been proven to be associated with global DNA hypomethylation and hypermethylation of tumor suppressor genes [16, 17]. Study on CRC showed decreased LINE-1 methylation in individuals with MTHFR rs1801133 CC/ rs1801131 AA [18]. However, the evidence regarding the role of MTHFR rs1801133 polymorphism in gene methylation is conflicting. Meanwhile MTHFR rs1801133 polymorphism shows marked heterogeneity among different populations and areas. Further studies on the effect of MTHFR rs1801133 on the risk of CRC and DNA methylation are needed to be clarified in the local areas.
Chaotic gene-specific DNA methylation is a risk factor for CRC and a promising candidate for biomarker development [19]. The Septin 9 (SEPT9) gene methylation test was approved by the US Food and Drug Administration (FDA) as a screening test for CRC [20]. The SEPT9 gene is located on human chromosome 17q25.3 and contains 17 exons that are involved in cell chromosome separation, DNA migration, apoptosis, and regulation of cell growth. In the early stages of CRC, SEPT9 is methylated and released into the peripheral blood when cancer cells undergo necrosis or apoptosis. By detecting the level of plasma methylated Septin 9 (mSEPT9) in peripheral blood, the risk of CRC in patients can be preliminarily evaluated. A plasma mSEPT9 assay was developed for the early screening and diagnosis of CRC. At present, the sensitivity range of mSEPT9 for CRC diagnosis is 48.2–95.6%, and the specificity range is 79.1–99.1% [20,21,22,23]. The sensitivity of the mSEPT9 assay increases with tumor progression from stage I to IV [24]. The mSEPT9 assay also plays a role in monitoring treatment effectiveness and predicting recurrence and survival rates [25]. However, whether related factors affect the methylation of SEPT9 is unclear.
Despite a great deal of research, the processes behind SNPs’ involvement in the genetic susceptibility of cancer are still unclear. Furthermore, variations in epigenetic regulation brought on by gene polymorphisms add to the complexity of SNP-related cancer susceptibility. It is uncertain whether MTHFR rs1801133 influences SEPT9 methylation in CRC. The aim of the present study was to investigate the association of the MTHFR rs1801133 polymorphism with the risk of CRC and the methylation status of SEPT9 in CRC patients in Yunnan Province in southwestern China.
Subjects and Methods
Study Population
To assess the overall prevalence of the MTHFR rs1801133 polymorphism, data were obtained from the routine testing of 2,999 patients who underwent MTHFR rs1801133 polymorphism testing at the physical examination center of the First People’s Hospital of Yunnan Province from January 2021 to June 2023. The results of MTHFR rs1801133 polymorphism and serum homocysteine tests were analyzed.
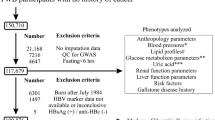
To evaluate the effect of the MTHFR rs1801133 polymorphism on CRC and the methylation of SEPT9, clinical medical information of 540 patients with a definite diagnosis of CRC were collected for the present study from May 2020 to June 2023. And 567 patients from January 2022 to June 2023 who were healthy and just underwent a physical examination for SEPT9 methylation were enrolled. All patients underwent simultaneous examinations of mSEPT9, CEA, CA199, and CA724. Patients with CRC were diagnosed based on pathological results obtained through colonoscopy. Among these 540 patients with CRC and 567 healthy individuals, 140 patients with CRC and 205 healthy individuals were genotyped for MTHFR rs1801133. The tumor, node, and metastasis staging (TNM) were defined based on the 8th edition of the Cancer Staging Manual of the American Joint Committee on Cancer [26]. The clinicopathological information of the patients, including age, sex, TNM stage, and tumor location, was collected for analysis. This study was approved by the Institutional Review Board of the First People’s Hospital of Yunnan Province(No. KHLL2023-KY177).
SEPT9 Methylation Assay
A 10 mL peripheral-elbow venous blood sample was collected using a K2EDTA anticoagulant tube. Whole blood was centrifuged (1200 g, 12 min) to separate the plasma within 2 h. After obtaining the plasma, it was centrifuged again for 12 min with the centrifugal force used previously. Then the separated plasma was stored at -20℃, and the test was performed within 4 days. The Septin9 Gene Methylation Detection Kit (Beijing BioChain Co., Ltd.; China) was used to perform the mSEPT9 assay. The experiments were performed in accordance with the manufacturer’s instructions. Real-time polymerase chain reaction (RT-PCR) was performed for 45 cycles to detect both mSEPT9 and the internal control, β-actin (ACTB). A cycle threshold (Ct) ACTB value ≤32, signaled the presence of sufficient DNA and experimental validity. Samples with mSEPT9 Ct values ≤41 were considered positive for mSEPT9.
MTHFR rs1801133 polymorphism Analysis
Genomic DNA from the buffy coat of the K2EDTA anticoagulant tube was extracted using a commercial DNA extraction kit (HEALTH Gene Technologies Co., Ltd.; Ningbo, China). Experiments were performed according to the manufacturer’s instructions. Genotyping for MTHFR rs1801133 was performed using a mutagenically separated polymerase chain reaction and running on a 3% agarose gel to determine the size, as described by Mokarram [27]. PCR reactions were carried out in a volume of 20 µL using GoTaq Master Mixes (Promega, Madison, USA). The cycling parameters were 5 min at 95℃ followed by 35 cycles of 45 s at 95℃, 1 min at 55℃, and 45 s at 72℃, followed by a single 10-min extension at 72℃. Using a 3% agarose gel,10 µL of each reaction mixture were separated, stained with ethidium bromide, and visualized under UV illumination.
Statistical Analysis
Data analysis was performed using SPSS software (V.26.0, IBM Inc.; Chicago, Illinois, USA) or GraphPad Prism software (V.9.0; GraphPad Software, Inc.; San Diego, CA, USA). Categorical variables were analyzed using the chi-square test. Numerical data are expressed as mean ± standard deviation and were analyzed using the Student’s t-test. Logistic regression analysis was applied for the risk assessment of CRC and methylation of SEPT9, and the risk of association was estimated using odds ratios (OR) with 95% confidence intervals (95%CI). Statistical significance was set at P < 0.05.
Results
Frequencies of MTHFR rs1801133 Genotypes and Alleles in Yunnan Province
Of the 2,999 patients enrolled, the average age was 46.87 ± 9.78 years. In total, 1,110 (37.0%) patients were homozygous for the wild-type allele (CC) genotype of MTHFR rs1801133, 1,435 (47.8%) carried one mutant allele (CT), and 454 (15.1%) were homozygous for the mutant allele (TT). The overall frequencies of the MTHFR rs1801133 C and T alleles were 60.9% and 39.1%, respectively. The frequencies of the MTHFR rs1801133 polymorphism among the enrolled patients were in Hardy–Weinberg equilibrium. The distribution of the MTHFR rs1801133 polymorphism between males and females is shown in Table 1; the frequencies of the T allele and TT genotype among males were significantly different from those of females. The serum homocysteine (Hcy) levels of 2,960 participants were tested. The median Hcy level in patients with the MTHFR rs1801133 CC genotype (n = 1,096) was 11.80 (9.80–13.97) µmol/L. Patients with MTHFR rs1801133 CT (n = 1,415) and TT (n = 449) genotypes had elevated Hcy levels of 12.3 (9.90–14.40) and 13.2 (10.20–17.80) µmol/L, respectively (Fig. 1A). Considering the relationship between Hcy levels and age, we categorized the enrolled patients into five age groups (Fig. 1B). With increasing age, the Hcy level among people with the MTHFR rs1801133 TT genotype was significantly higher, especially in the age group of 41–50 years (Fig. 1B).

Plasma homocysteine levels. (A) Plasma homocysteine levels in MTHFR rs1801133 genotypes. (B) Plasma homocysteine levels in MTHFR rs1801133 genotypes among different age groups. Values are expressed as mean ± SD, *significantly different from CC genotype, *P<0.05, **P<0.01, ***P<0.001
Value of mSEPT9 Assay in the Diagnosis of CRC in Yunnan Province
To assess the diagnostic value of the mSEPT9 assay for CRC, 540 patients with a definite diagnosis of CRC were recruited. Table 2 shows the clinicopathological characteristics of the enrolled patients. Among 540 patients, 61.48% were men and the median age was 54.47 ± 13.14. 65.37% of all colorectal tumors developed in the rectum. 195 patients had negative mSEPT9 methylation, while 345 had positive results. 87 individuals with stage I, 90 with stage II, 287 with stage III, and 76 with stage IV colorectal cancer were included in the sample. The positivity rate of mSEPT9 between male and female patients with CRC was not significantly different (P > 0.05). mSEPT9-positive and -negative patients showed no significant differences in age or cancer location (P > 0.05). The positivity rate for mSEPT9 was markedly higher in patients with more advanced TNM stages than in those with less advanced stages. The mean Ct values of mSEPT9 in patients with more advanced TNM stages were much lower (Fig. 2A– C), indicating a higher degree of methylation. With respect to other peripheral blood biomarkers, mSEPT9-positive patients had higher levels of CEA, CA199, and CA724 than mSEPT9-negative patients.

Association Between Septin9 methylation and CRC. (A) Ct value of plasma mSEPT9 in each primary tumor (T) category. (B) Ct value of plasma mSEPT9 in each primary tumor (N) category. (C) Ct value of plasma mSEPT9 in each primary tumor (M) category. (D) ROC curves of mSEPT9, CEA, CA19-9, and CA724 in discriminating patients with CRC from healthy participants. Values are expressed as mean ± SD, *significantly different from CC genotype, *P<0.05, ***P<0.001
To further understand the performance of the mSEPT9 assay in the diagnosis of CRC, 540 subjects with a definite diagnosis of CRC and 567 subjects who underwent a physical examination for SEPT9 methylation were recruited. The areas under the ROC curve (AUC) for mSEPT9, CEA, CA19-9, and CA724 were 0.865, 0.829, 0.522, and 0.564, respectively (Fig. 2D). The sensitivity and specificity of the mSEPT9 assay (73.89% and 97.88%, respectively) were higher than those of the CEA (79.22% and 70.02%, respectively), CA19-9 (18.40% and 83.90%, respectively), and CA724 (27.00% and 76.68%, respectively) assays.
Association Between the Risk of CRC and MTHFR rs1801133 in Yunnan Province
To investigate the association between the risk of CRC and MTHFR rs1801133 in Yunnan Province, among 540 patients with CRC and 546 healthy individuals, 140 patients with CRC and 205 healthy individuals were genotyped for MTHFR rs1801133. The frequencies of MTHFR rs1801133 CC, CT, and TT in patients with CRC were 50.00%, 38.57%, and 11.43%, respectively. For healthy individuals, the frequencies were 37.80%, 44.86%, and 17.84%, respectively (Table 3), which were similar to the overall prevalence described previously (Table 1). The distribution of MTHFR genotypes in these individuals agreed with the Hardy-Weinberg equilibrium. The frequencies of the MTHFR CC genotype and allele C carriers in patients with CRC were significantly higher than those in healthy individuals (P = 0.006 and P = 0.001, respectively). Moreover, Table 3 indicates that CC genotype carriers were associated with a higher risk of CRC before and after adjusting for sex and age.
Association Between SEPT9 Methylation and MTHFR rs1801133 in Yunnan Province
To further analyze the association between SEPT9 methylation and the MTHFR rs1801133 polymorphism, 135 patients with CRC were analyzed. Among them, 65 patients were negative for the mSEPT9 assay, and 70 patients were positive for the methylation of SEPT9. The positivity rate of the mSEPT9 assay was significantly higher among the MTHFR rs1801133 TT genotype and allele T carriers than among the CC and allele C carriers respectively (P = 0.040 and P = 0.028, respectively) (Table 4). The MTHFR rs1801133 TT genotype and allele T carriers had a positive correlation with the methylation of SEPT9 (OR = 3.320, 95% CI 1.485–7.424, P = 0.003 and OR = 1.783, 95% CI 1.056–3.010, P = 0.030, respectively) (Table 4).
Discussion
Both genetic and epigenetic changes are important in CRC pathogenesis. In the present study, the association of the MTHFR rs1801133 genotype with CRC risk and SEPT9 methylation in individuals with CRC in the Yunnan Province was reported.
Our study showed that the prevalence of the MTHFR rs1801133 CC, CT, and TT genotypes was 37.0%, 47.8%, and 15.1%, respectively. Meanwhile, the mutant T allele carriers had a higher level of serum Hcy, especially among individuals aged 41–50 years. This finding implies that individuals with the mutation in this age range should be cautious of hyperhomocysteine-related disorders. The frequency of the MTHFR rs1801133 polymorphism varies among different regions and ethnic groups. The frequency of the mutant T allele is much higher in South America and Asia and less common in Europe and North America. The prevalence of the MTHFR rs1801133 TT genotype is 32.2% in Mexico, while in North America, the prevalence ranges from 2.7–10.7% [28]. A study conducted in the United Kingdom showed that the frequencies of the CC, CT, and TT genotypes are 55%, 35%, and 10%, respectively [29]. China is a vast land comprised of multiethnic groups, and the frequency of the MTHFR rs1801133 TT genotype varies from 6.4 to 40.8% from south to north [30]. Using larger sample sizes, the frequency of the mutant T allele in Yunnan Province in our study was slightly higher than that reported by Ni et al. [31], and may provide more accurate information on the prevalence of MTHFR polymorphisms in Yunnan Province.
We investigated the association of MTHFR rs1801133 polymorphisms with CRC in the local region. Our results showed that the frequencies of the MTHFR rs1801133 CC genotype and allele C carriers were significantly higher in patients with CRC and were associated with a higher risk of CRC. Previous studies investigating the association of MTHFR rs1801133 and CRC have yielded conflicting results. Three studies conducted in Iran found that the MTHFR rs1801133 TT genotypes demonstrated a higher risk of CRC [32,33,34]. Baghad et al. [35], Slattery et al. [36], Ma et al. [37], and Le Marchand et al [38]. observed similar phenomena. Lin et al. [39] reported that the mutant T allele serves as a predictive factor for CRC in Taiwan. Meta-analyses by Guo et al. [40] and Yang et al. [41] also suggests that the MTHFR mutant T allele is associated with a low risk of CRC in Asians. This disparity may be due to differences in the ethnicity or other factors. To the best of our knowledge, this is the first study to investigate the association of MTHFR rs1801133 and CRC susceptibility in the Yunnan Province, China. This finding could help to partially explain why CC carriers have a higher risk of CRC.
In the present study, we demonstrated the diagnostic value of the mSEPT9 assay in the Yunnan Province, with an AUC of 0.865, a sensitivity of 73.89%, and a specificity of 97.88%. The positivity rate and degree of mSEPT9 methylation were remarkably higher in patients with more advanced TNM stages than in those with less advanced stages. These findings are in accordance with those of Sun et al. [42] and Lu et al. [43], who reported that the sensitivity and specificity of the mSEPT9 assay for CRC detection were 73.0% and 94.5%, respectively. Furthermore, we assessed the association of the MTHFR rs1801133 polymorphism with the methylation status of SEPT9 in CRC. Our data showed that the MTHFR rs1801133 TT genotype and allele T carriers were positively correlated with the methylation of SEPT9. The MTHFR mutant T allele has been associated with genomic DNA hypomethylation [44], especially when accompanied by a low folate intake [45]. Supic et al. [46] suggested that the MTHFR rs1801133 TT genotype is a risk factor for methylation of the RASSF1A gene in oral squamous cell carcinoma patients. Cheng et al. [47] found a significant association between the MTHFR rs1801133 CC genotype and hypomethylation of the IGF-2 gene in transitional cell carcinoma of the bladder. The methylation status of the WIF-1 gene in CRC has also been associated with the MTHFR rs1801133 polymorphism [48]. Our study is the first to report that the MTHFR C677T polymorphism contributes to the methylation of the SEPT9 gene in CRC. This finding raises the possibility that SEPT9 gene methylation influences disease severity and may influence treatment and prognosis in people with colorectal cancer. MTHFR rs1801133 gene polymorphism also influences the methylation of SEPT9. Our study had some limitations. First, the effects of MTHFR polymorphisms are significantly related to the daily folate intake [49]. When analyzing the impact of the MTHFR rs1801133 polymorphism on CRC and the methylation of SEPT9, we did not consider the folate intake of the enrolled patients. Second, the sample size of patients with CRC remains small, and further studies with larger sample sizes are required to verify our results. Yunnan is a multiethnic province, and research involving multiple centers and ethnic groups can provide more accurate information. Third, because of the limited availability of colonic tissue biopsies, we only evaluated the impact of the MTHFR rs1801133 polymorphism on serum cell-free circulating methylated SEPT9. Further research is warranted to investigate the effect of the MTHFR polymorphism on the methylation of SEPT9 in tumor tissues.
In conclusion, our results suggest that the positivity rate and degree of methylation of mSEPT9 are significantly associated with the TNM stage in CRC patients. Individuals in Yunnan Province with the MTHFR rs1801133 CC genotype have a higher risk of CRC and the MTHFR rs1801133 TT carriers are more susceptible to SEPT9 gene methylation. Further well-designed, prospective, multicenter, and multiethnic studies are required to examine the influence of MTHFR polymorphisms in gene methylation and CRC pathogenesis.
Data Availability
Data can be requested by the corresponding author.
References
Sung H, Ferlay J, Siegel RL, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Sung JJ, Ng SC, Chan FK, et al. An updated Asia Pacific Consensus recommendations on colorectal cancer screening. Gut. 2015;64(1):121–32.
Yu S, Cheng J, Li P, et al. Association study for the role of MMP8 gene polymorphisms in colorectal cancer susceptibility. BMC Cancer. 2023;23(1):1169.
Shridhar K, Aggarwal A, Walia GK, et al. Single nucleotide polymorphisms as markers of genetic susceptibility for oral potentially malignant disorders risk: review of evidence to date. Oral Oncol. 2016;61:146–51.
Tower GB, Coon CI, Belguise K, et al. Fra-1 targets the AP-1 site/2G single nucleotide polymorphism (ETS site) in the MMP-1 promoter. Eur J Biochem. 2003;270(20):4216–25.
Do TN, Ucisik-Akkaya E, Davis CF, et al. An intronic polymorphism of IRF4 gene influences gene transcription in vitro and shows a risk association with childhood acute lymphoblastic leukemia in males. Biochim Biophys Acta. 2010;1802(2):292–300.
Verhaegh GW, Verkleij L, Vermeulen SH, et al. Polymorphisms in the H19 gene and the risk of bladder cancer. Eur Urol. 2008;54(5):1118–26.
Biselli PM, Guerzoni AR, de Godoy MF, et al. Genetic polymorphisms involved in folate metabolism and concentrations of methylmalonic acid and folate on plasma homocysteine and risk of coronary artery disease. J Thromb Thrombolysis. 2010;29(1):32–40.
Bae S, Ulrich CM, Bailey LB, et al. Impact of folic acid fortification on global DNA methylation and one-carbon biomarkers in the women’s Health Initiative Observational Study cohort. Epigenetics. 2014;9(3):396–403.
Raghubeer S, Matsha TE. Methylenetetrahydrofolate (MTHFR), the one-Carbon cycle, and Cardiovascular risks. Nutrients. 2021;13(12).
Levin BL, Varga E. MTHFR: addressing genetic counseling dilemmas using evidence-based literature. J Genet Couns. 2016;25(5):901–11.
Duthie SJ, Narayanan S, Brand GM, et al. Impact of folate deficiency on DNA stability. J Nutr. 2002;132(8 Suppl):2444S–9S.
Lu Q, Jiang K, Li Q, et al. Polymorphisms in the MTHFR gene are associated with breast cancer risk and prognosis in a Chinese population. Tumour Biol. 2015;36(5):3757–62.
Hesari A, Maleksabet A, Tirkani AN, et al. Evaluation of the two polymorphisms rs1801133 in MTHFR and rs10811661 in CDKN2A/B in breast cancer. J Cell Biochem. 2019;120(2):2090–7.
Castro R, Rivera I, Blom HJ, et al. Homocysteine metabolism, hyperhomocysteinaemia and vascular disease: an overview. J Inherit Metab Dis. 2006;29(1):3–20.
Friso S, Choi SW, Girelli D, et al. A common mutation in the 5,10-methylenetetrahydrofolate reductase gene affects genomic DNA methylation through an interaction with folate status. Proc Natl Acad Sci U S A. 2002;99(8):5606–11.
Stern LL, Mason JB, Selhub J, et al. Genomic DNA hypomethylation, a characteristic of most cancers, is present in peripheral leukocytes of individuals who are homozygous for the C677T polymorphism in the methylenetetrahydrofolate reductase gene. Cancer Epidemiol Biomarkers Prev. 2000;9(8):849–53.
Iacopetta B, Grieu F, Phillips M, et al. Methylation levels of LINE-1 repeats and CpG island loci are inversely related in normal colonic mucosa. Cancer Sci. 2007;98(9):1454–60.
Ebert MP, Mooney SH, Tonnes-Priddy L, et al. Hypermethylation of the TPEF/HPP1 gene in primary and metastatic colorectal cancers. Neoplasia. 2005;7(8):771–8.
Church TR, Wandell M, Lofton-Day C, et al. Prospective evaluation of methylated SEPT9 in plasma for detection of asymptomatic colorectal cancer. Gut. 2014;63(2):317–25.
Tham C, Chew M, Soong R, et al. Postoperative serum methylation levels of TAC1 and SEPT9 are independent predictors of recurrence and survival of patients with colorectal cancer. Cancer. 2014;120(20):3131–41.
Grutzmann R, Molnar B, Pilarsky C, et al. Sensitive detection of colorectal cancer in peripheral blood by septin 9 DNA methylation assay. PLoS ONE. 2008;3(11):e3759.
Song L, Jia J, Peng X, et al. The performance of the SEPT9 gene methylation assay and a comparison with other CRC screening tests: a meta-analysis. Sci Rep. 2017;7(1):3032.
Ma ZY, Law WL, Ng EKO, et al. Methylated septin 9 and Carcinoembryonic Antigen for Serological Diagnosis and monitoring of patients with colorectal Cancer after surgery. Sci Rep. 2019;9(1):10326.
Song L, Yu H, Jia J, et al. A systematic review of the performance of the SEPT9 gene methylation assay in colorectal cancer screening, monitoring, diagnosis and prognosis. Cancer Biomark. 2017;18(4):425–32.
Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer staging Manual: continuing to build a bridge from a population-based to a more personalized approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–9.
Mokarram P, Naghibalhossaini F, Saberi Firoozi M, et al. Methylenetetrahydrofolate reductase C677T genotype affects promoter methylation of tumor-specific genes in sporadic colorectal cancer through an interaction with folate/vitamin B12 status. World J Gastroenterol. 2008;14(23):3662–71.
Wilcken B, Bamforth F, Li Z, et al. Geographical and ethnic variation of the 677C > T allele of 5,10 methylenetetrahydrofolate reductase (MTHFR): findings from over 7000 newborns from 16 areas world wide. J Med Genet. 2003;40(8):619–25.
Hanks J, Ayed I, Kukreja N, et al. The association between MTHFR 677C > T genotype and folate status and genomic and gene-specific DNA methylation in the colon of individuals without colorectal neoplasia. Am J Clin Nutr. 2013;98(6):1564–74.
Yang B, Liu Y, Li Y, et al. Geographical distribution of MTHFR C677T, A1298C and MTRR A66G gene polymorphisms in China: findings from 15357 adults of Han nationality. PLoS ONE. 2013;8(3):e57917.
Ni J, Zhang L, Zhou T, et al. Association between the MTHFR C677T polymorphism, blood folate and vitamin B12 deficiency, and elevated serum total homocysteine in healthy individuals in Yunnan Province, China. J Chin Med Assoc. 2017;80(3):147–53.
Ghorbani M, Azghandi M, Khayami R, et al. Association of MTHFR C677T variant genotype with serum folate and vit B12 in Iranian patients with colorectal cancer or adenomatous polyps. BMC Med Genomics. 2021;14(1):246.
Naghibalhossaini F, Mokarram P, Khalili I, et al. MTHFR C677T and A1298C variant genotypes and the risk of microsatellite instability among Iranian colorectal cancer patients. Cancer Genet Cytogenet. 2010;197(2):142–51.
Haghighi MM, Radpour R, Mahmoudi T, et al. Association between MTHFR polymorphism (C677T) with nonfamilial colorectal cancer. Oncol Res. 2009;18(2–3):57–63.
Baghad I, Erreguibi D, Boufettal R, et al. [Association of methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism and the risk of sporadic colorectal cancer]. Pan Afr Med J. 2021;38:287.
Slattery ML, Potter JD, Samowitz W, et al. Methylenetetrahydrofolate reductase, diet, and risk of colon cancer. Cancer Epidemiol Biomarkers Prev. 1999;8(6):513–8.
Ma J, Stampfer MJ, Giovannucci E, et al. Methylenetetrahydrofolate reductase polymorphism, dietary interactions, and risk of colorectal cancer. Cancer Res. 1997;57(6):1098–102.
Le Marchand L, White KK, Nomura AM, et al. Plasma levels of B vitamins and colorectal cancer risk: the multiethnic cohort study. Cancer Epidemiol Biomarkers Prev. 2009;18(8):2195–201.
Lin KM, Yang MD, Tsai CW, et al. The role of MTHFR genotype in Colorectal Cancer susceptibility in Taiwan. Anticancer Res. 2018;38(4):2001–6.
Guo XP, Wang Y, Zhao H, et al. Association of MTHFR C677T polymorphisms and colorectal cancer risk in asians: evidence of 12,255 subjects. Clin Transl Oncol. 2014;16(7):623–9.
Yang Z, Zhang XF, Liu HX, et al. MTHFR C677T polymorphism and colorectal cancer risk in asians, a meta-analysis of 21 studies. Asian Pac J Cancer Prev. 2012;13(4):1203–8.
Sun J, Fei F, Zhang M, et al. The role of (m)SEPT9 in screening, diagnosis, and recurrence monitoring of colorectal cancer. BMC Cancer. 2019;19(1):450.
Lu P, Zhu X, Song Y, et al. Methylated septin 9 as a Promising Biomarker in the diagnosis and recurrence monitoring of Colorectal Cancer. Dis Markers. 2022;2022:7087885.
Mao N, Chen J, Wang J, et al. [Correlations of Methylenetetrahydrofolate Reductase Gene Polymorphism and genomic DNA hypomethylation level with Ankylosing Spondylitis]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2020;42(3):307–12.
Bozovic IB, Stankovic A, Zivkovic M, et al. Altered LINE-1 methylation in mothers of children with Down Syndrome. PLoS ONE. 2015;10(5):e0127423.
Supic G, Jovic N, Kozomara R, et al. Interaction between the MTHFR C677T polymorphism and alcohol–impact on oral cancer risk and multiple DNA methylation of tumor-related genes. J Dent Res. 2011;90(1):65–70.
Cheng H, Deng Z, Wang Z, et al. MTHFR C677T polymorphisms are associated with aberrant methylation of the IGF-2 gene in transitional cell carcinoma of the bladder. J Biomed Res. 2012;26(2):77–83.
Jalilvand A, Soltanpour MS. Promoter hypermethylation of Wnt/beta-catenin signaling pathway inhibitor WIF-1 gene and its Association with MTHFR C677T polymorphism in patients with colorectal Cancer. Oman Med J. 2020;35(3):e131.
Levine AJ, Figueiredo JC, Lee W, et al. Genetic variability in the MTHFR gene and colorectal cancer risk using the colorectal cancer family registry. Cancer Epidemiol Biomarkers Prev. 2010;19(1):89–100.
Funding
This project was supported by Yunnan Provincial Key Laboratory of Clinical Virology(grant No. 202002AG070062), Research Fund for the Doctoral Program of the First People Hospital of Yunnan Province(grant No. KHBS-2020-009) and the National Natural Science Foundation of China (grant No.82060664 and 81960606).
Author information
Authors and Affiliations
Contributions
Ya Xu and Tao Zhou designed the experiments and analyzed the data. Yafei Huang, Ting Su and Qiuting Duan performed the experiments. Xin Fan, Luping Liu, Jinxiu Wan and Xiangcong Wei collected the clinical information. Ziqin Dian, Guiqian Zhang and Yi Sun wrote the main manuscript text. All authors reviewed the manuscript and approved the manuscript and agree to be accountable for all aspects of the research in ensuring that the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, Y., Su, T., Duan, Q. et al. Association of Methylenetetrahydrofolate Reductase rs1801133 Gene Polymorphism with Cancer Risk and Septin 9 Methylation in Patients with Colorectal Cancer. J Gastrointest Canc 55, 778–786 (2024). https://doi.org/10.1007/s12029-024-01020-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-024-01020-y