
Abstract
Portal vein embolization with stem cell augmentation (PVESA) is an emerging approach for enhancing the growth of the liver segment that will remain after surgery (i.e., future liver remnant, FLR) in patients with liver cancer. Conventional portal vein embolization (PVE) aims to induce preoperative FLR growth, but it has a risk of failure in patients with underlying liver dysfunction and comorbid illnesses. PVESA combines PVE with stem cell therapy to potentially improve FLR size and function more effectively and efficiently. Various types of stem cells can help improve liver growth by secreting paracrine signals for hepatocyte growth or by transforming into hepatocytes. Mesenchymal stem cells (MSCs), unrestricted somatic stem cells, and small hepatocyte-like progenitor cells have been used to augment liver growth in preclinical animal models, while clinical studies have demonstrated the benefit of CD133 + bone marrow–derived MSCs and hematopoietic stem cells. These investigations have shown that PVESA is generally safe and enhances liver growth after PVE. However, optimizing the selection, collection, and application of stem cells remains crucial to maximize benefits and minimize risks. Additionally, advanced stem cell technologies, such as priming, genetic modification, and extracellular vesicle-based therapy, that could further enhance efficacy outcomes should be evaluated. Despite its potential, PVESA requires more investigations, particularly mechanistic studies that involve orthotopic animal models of liver cancer with concomitant liver injury as well as larger human trials.
Similar content being viewed by others


Background
Liver cancers represent the third leading cause of cancer death worldwide, and their aggressive nature and late detection often result in a poor prognosis [1]. For many individuals with primary and secondary liver cancers, liver resection offers a potential cure. However, many patients who would otherwise undergo curative liver resection do not have enough remaining functional liver to safely carry out major resection. This situation places patients at a high risk of life-threatening hepatic insufficiency due to minimal postoperative functional liver volume.
Portal vein ligation (PVL) and portal vein embolization (PVE) are methods developed in the mid-1980s to increase the future liver remnant (FLR) volume prior to resection by obstructing portal blood flow to the liver segments slated for removal [2]. PVL is typically performed by a surgeon either during open surgery or laparoscopy, while PVE is performed percutaneously by an interventional radiologist. Our group favors PVE over PVL because it tends to induce less inflammation in the porta hepatis, potentially enhancing the safety of subsequent major hepatectomies. Makuuchi et al. first described PVE in 1984, building on early 20th-century animal studies that demonstrated the growth of non-ligated liver segments following portal vein branch ligation [2]. Notably, about 70% of patients undergoing PVE can proceed to resection within six weeks of the procedure [3, 4].
Despite the use of portal vein occlusion strategies, post-hepatectomy liver failure remains the leading cause of morbidity and mortality after resection [3, 5]. To further augment FLR growth following PVL or PVE, adjunctive procedures, such as associated liver partition and PVL for staged hepatectomy (ALPPS) and liver venous deprivation (LVD), have been developed [6]. ALPPS is a two-pronged approach that combines complete transection of the liver along the falciform ligament and right PVL. However, it has been associated with significantly higher morbidity and mortality [7]. On the other hand, LVD, which combines PVE and hepatic venous embolization, has shown comparable intra-operative and post-operative complication rates with standalone PVE [8]. While these procedures may provide improvements in FLR growth, the outcomes for many patients with liver cancer remain severely limited by underlying chronic liver injury. In this clinical scenario, adjunctive intrahepatic administration of stem cells, in combination with PVE is a promising solution. In this review, we discuss the challenges of increasing the volume and quality of the FLR using PVE as a standalone procedure and the potential of PVE with stem cell augmentation (PVESA) to enhance the benefits seen with PVE. Various stem cell types have been utilized in preclinical and clinical research (Fig. 1), and the most recent data and outlook for each are also discussed.

Schematic diagram of factors and mechanisms involved in PVE and PVESA. The growth of hepatocytes following PVE is mediated by several cytokines, growth factors, vasoactive substances, and hormones. On the other hand, PVESA enhances the FLR growth achieved with PVE through additional paracrine effects and differentiation. The differentiation of HSCs and SHPCs to hepatocytes has been suggested, but it requires further investigation. Abbreviations: 5-HT, serotonin; EGF, epidermal growth factor; FLR, future liver remnant; HGF, hepatocyte growth factor; HSC, hematopoietic stem cell; IGF-1, insulin-like growth factor 1; IL, interleukin; MMP-9, matrix metalloproteinase 9; MSC, mesenchymal stem cell; NE, norepinephrine; NO, nitric oxide; PGE2, prostaglandin E2; PVE, portal vein embolization; PVESA, portal vein embolization with stem cell augmentation; SHPC, small hepatocyte-like progenitor cell; TGF-α, transforming growth factor alpha; TNF-α, tumor necrosis factor alpha; USSC, unrestricted somatic stem cell; VEGF, vascular endothelial growth factor. The figure has been created using Biorender.com
Current Clinical Use of Preoperative PVE or PVL
PVE is currently the standard method for increasing FLR volume prior to liver resection [5]. By directing portal blood flow away from the part of the liver that will be resected, FLR growth may be induced. PVE is generally associated with minimal procedure-related mortality and is well-tolerated by patients [9, 10]. Unfortunately, up to 30% of patients who receive PVE will experience insufficient liver growth to allow for major liver resection [3, 4]. The degree of liver growth achieved with PVE depends on the degree of liver disease present in the patient, as well as the technical aspects of the PVE procedure.
Clinical Utility of PVE
For patients with liver malignancy, surgical resection or liver transplantation remain the best treatment options. However, liver transplantation is unavailable to many because of a scarcity of liver donors, while the presence of chronic liver damage in a large percentage of patients with liver cancer precludes surgical resection. FLR volume is an important determinant of resectability as it can predict post-hepatectomy liver failure and may constitute the difference between curative treatment and malignant progression. Maximizing the capacity to enhance FLR volume directly results in an increase in the number of lives saved from liver malignancy by expanding the cohort of patients who can undergo safe liver resection. For patients with normal healthy liver parenchyma, an FLR volume standardized to the patient’s body surface area of ≥ 20% is required. A higher FLR volume (30–40%) is recommended if chronic liver injury is present (e.g., chemotherapy-associated liver damage, liver fibrosis, or cirrhosis) [3, 11, 12]. For those with insufficient FLR volume or limited functional capacity because of concurrent liver dysfunction, PVE is the gold standard for inducing an increase in FLR. Hence, PVE allows some patients with liver malignancies to undergo curative resection. The most common malignancies for which PVE is indicated prior to resection are hepatocellular carcinoma (HCC), cholangiocarcinoma (CCA), and metastatic colorectal cancer (mCRC). For patients with intrahepatic colorectal metastasis, resection can offer significantly prolonged survival and a superior prognosis with regard to further disease progression [13, 14].
Mechanism of Liver Growth from PVE
The liver has long been known to have significant regenerative capacity. The first published instance of liver regeneration following PVE was a 1920 paper describing the compensatory growth of the non-embolized sections of the liver in rabbits following occlusion of the other portal veins [15]. The mechanisms of hepatic growth after PVE appear to be similar to those seen in partial hepatectomy (PH). However, the more sudden change in hemodynamics observed in PH contributes to more rapid activation of liver proliferation compared to PVE. The rapid increase in hepatic portal venous blood flow into the non-embolized lobe increases shear and circumferential stress on sinusoidal endothelial cells, hepatocytes, and Kupffer cells, initiating a cascade of signaling events that leads to an increase in pro-proliferative cytokines (e.g., interleukin-6 and tumor necrosis factor alpha), growth factors (e.g., hepatocyte growth factor [HGF], epidermal growth factor [EGF], transforming growth factor alpha, and vascular endothelial growth factor [VEGF]), vasoactive factors (e.g., nitric oxide [NO] and prostaglandin E2 [PGE2]), and hormones (e.g., insulin, insulin-like growth factor 1, estrogen, norepinephrine, and serotonin) (Fig. 1) [16,17,18,19]. The majority of studies on liver growth focus on clinically measurable endpoints, such as liver volume or weight, and the increase in these measures seen after PH or PVE is generally referred to as liver hypertrophy. However, preclinical studies on rodents have shown that the overall growth of the liver following PH or PVE depends not only on hepatocyte hypertrophy but also on hepatocyte hyperplasia [18, 20,21,22]. It has been shown in rats that the hepatocytes in the FLR proliferate in both PH and PVE, and the proliferating cell nuclear antigen index peaks in the FLR after PH and PVE at 24 and 48 h, respectively [23, 24]. After which, biliary epithelial cells, Kupffer cells, stellate cells, and sinusoidal endothelial cells also proliferate to restore the typical lobular architecture [25].
Technique
Prior to PVE, the FLR must be calculated to determine whether PVE is a necessary and appropriate treatment. A number of methods for calculating FLR may be used, including both volumetric and functional tests. A method to estimate the total required liver volume as a function of the patient’s size is provided by the following validated calculation based on a linear correlation between total liver volume (TLV) and body surface area (BSA): TLV = − 794.41 + 1267.28 × BSA (m2) [26]. Axial images from computed tomography and magnetic resonance imaging are the primary methods for volumetric assessment of the liver, both before and after resection (Fig. 2).

Imaging before and after PVE. (a) CT with contrast before PVE in a 67-year-old woman with metastatic colorectal cancer (arrowhead, right liver lobe). (b) Direct portography showing normal portal vein anatomy (arrowhead, portal vein). (c) Glue cast in the right portal vein branches demonstrating adequate embolization using an N-butyl-cyanoacrylate-lipiodol mixture. (d) CT imaging 30 days after right PVE showing growth of the left liver (arrowhead, left liver lobe). (e, f) CT volumetry after PVE illustrates an increase in FLR (red, right liver lobe; green, left liver lobe). Abbreviations: CT, computed tomography; FLR, future liver remnant; PVE, portal vein embolization. Images have been adapted from Luz et al., 2017 [30]. The figure has been created using Biorender.com
There are several techniques for accessing the portal vein for PVE. The less invasive methods include percutaneous approaches, where transhepatic puncture of the portal vein is executed using ultrasound and fluoroscopic guidance. The cutaneous approach is generally performed via an ipsilateral (i.e., same side as the PVE) or contralateral approach (i.e., opposite side from the PVE) [27]. An older surgical technique, often referred to as the transileocolic approach, may also be used, whereby direct puncture of the ileocolic venous branch is conducted through a lower right quadrant incision. No literature suggests that any of these techniques are contraindicated in the case of concurrent stem cell administration.
There are several embolic agents available for use in PVE. These include gelatin sponges, N-butyl-cyanoacrylate (NBCA), nitinol vascular plug, occlusion coils, polyvinyl alcohol, sodium tetradecyl sulfate, and trisacryl microspheres [28]. The two most commonly used agents are trisacryl microspheres and coils as well as a mixture of NBCA and lipiodol. Most agents are considered safe and have demonstrated low complication rates. Considerations taken into account when choosing an agent should include its safety profile, cost, ease of use, efficacy, and required fluoroscopy time [29].
Clinical Challenges in Preoperative PVE
Increased resectability and decreased post-hepatectomy liver failure rates after PVE have been observed in appropriately selected patients. However, PVE is still limited by inadequate and protracted growth, especially in patients with specific risk factors. Several risk factors have been reported in the literature, such as a history of chemotherapy, underlying liver dysfunction, advanced age, and sarcopenia [31]. It is postulated that these factors contribute to a diminished functional capacity per unit volume of the liver. However, a recent meta-analysis by Soykan et al. revealed that there was no significant difference in the extent of hypertrophy following PVE between patients who did not undergo pre-procedural systemic therapy and those who received neo-adjuvant chemotherapy [31]. The pooled data, though, showed a high degree of heterogeneity. Patients with background liver fibrosis have also been reported to exhibit delayed or insufficient FLR growth after PVE [32]. Paradoxically, however, some studies have reported that background cirrhosis, which is the late stage of progressive hepatic fibrosis, does not significantly affect the extent of FLR growth [33, 34]. Importantly, regardless of the degree of FLR hypertrophy following PVE, patients with evidence of liver injury require a larger quantity of FLR following right or extended right hepatectomy, underscoring the need for improved hypertrophy techniques in this patient population [35].
Similarly, conflicting findings have been reported on the relationship between advanced age and FLR growth, with the majority of research revealing no correlation [31]. Overall, liver function seems to be uniquely protected in aging humans. While many other organs exhibit a significant age-related decline in structure and function, the liver exhibits relatively modest changes related directly to aging [36]. A 2015 case-control study found that patients 70 years and older did not have impaired liver growth after portal vein occlusion compared to patients under 70 years of age [37]. In the same study, however, age was associated with greater postoperative liver failure, which underscores the importance of liver quality and function and suggests that the magnitude of FLR growth in older patients needed to prevent postoperative failure may be greater compared to that in younger patients. Sarcopenia is a condition of low muscularity and low muscular strength that occurs most often in old age [38]. As opposed to advanced age, it has been consistently linked to inadequate FLR growth [39,40,41,42]. The relationship between sarcopenia and poor FLR growth following PVE is correlative [39,40,41,42], and further studies are needed to uncover the mechanisms underlying this association.
To date, advancements to PVE to further maximize liver growth have been largely mechanical in nature (i.e., right PVE extended to segment 4 branches [43], ALPPS [44, 45], and LVD [6]). The advantage of PVESA over these other techniques is that it may specifically address the critical need to improve FLR growth in a large number of patients with underlying liver fibrosis and comorbidities. Nonetheless, further investigations on the mechanisms underlying the relationship between the aforementioned risk factors and suboptimal liver growth following PVE are necessary to help inform clinicians in making decisions regarding which patients may most benefit from an enhanced PVE procedure, such as PVESA.
Role of Stem Cells in Augmenting PVE
Although hepatocyte repopulation following resection of a healthy liver is mainly conducted by fully differentiated hepatocytes, which have a sufficient regenerative capacity to reconstruct the full volume of the liver, stem cells may play a bigger role in the context of massive acute liver injury or chronic liver disease [17, 21]. Typical regeneration in healthy livers involves hepatocyte hypertrophy and hyperplasia [18, 20,21,22]. Hepatocyte hypertrophy may sufficiently compensate for the loss of function because of small resections, but hepatocyte hyperplasia is necessary for resections involving more than 2/3 of the total liver volume. In the context of massive acute liver injury (≥ 80% loss of total liver volume) or chronic liver disease, the regenerative reserve of parenchymal hepatocytes becomes exhausted to the point that hepatic progenitor cells (HPCs)—the primary resident stem cells of the liver found in the canals of Hering—are activated [17, 21]. HPCs have the capacity to differentiate into hepatocytes and biliary epithelial cells, but their role in the reconstruction of hepatic architecture is not well established [21, 46]. Hence, the use of other stem cell types, which have the potential to not only differentiate into hepatocytes but also enhance hepatocyte proliferation through pro-proliferative signaling, has been explored in the last decades. Since up to 30% of patients undergoing PVE do not ultimately qualify for major resection because of malignant progression and/or inadequate liver growth, the use of stem cells to augment liver growth in a potentially shorter period could benefit a significant proportion of patients with liver malignancies.
Stem Cell Types and Potential Mechanisms of Augmented Liver Growth
Stem cells can augment FLR growth achieved by PVE through their paracrine effects and by increasing the pool of cells that can differentiate into hepatocytes [47,48,49,50,51]. Stem cell types that have been used to augment FLR growth following PVE or PVL in animal studies include adipose tissue-derived mesenchymal stem/stromal cells (AMSCs), bone marrow-derived mesenchymal stem/stromal cells (BMSCs), unrestricted somatic stem cells (USSCs), and small hepatocyte-like progenitor cells (SHPCs). On the other hand, clinical studies of PVESA have utilized CD133 + BMSCs and hematopoietic stem cells (HSCs).
MSCs have immunomodulatory and multi-lineage differentiation capacities, making them an ideal candidate for various clinical applications. These cells are characterized by the expression of markers such as CD105, CD73, and CD90 [52]. MSCs can be isolated from a wide variety of tissue types, expanded in vitro without significant changes in their properties, and delivered via autologous or allogeneic transplantation because of their low immunogenicity [53]. In the context of PVESA, preclinical studies have utilized AMSCs and BMSCs, while clinical studies have only utilized autologous BMSCs. The ability of AMSCs and BMSCs to differentiate into hepatocyte-like cells has been demonstrated in several preclinical in vivo studies [54, 55]. Umbilical cord-derived MSCs (UMSCs) have also been implanted in rats with fibrotic livers and have been shown to differentiate into cells that express hepatocyte-specific markers, such as albumin, α-fetoprotein, and cytokeratin 18 [56, 57]. With the support of specific growth factors, such as EGF, fibroblast growth factor, HGF, oncostatin M, and trichostatin A, MSCs from different tissues can also be induced in vitro to differentiate into cells with liver-specific morphology and function [58,59,60]. However, in some studies, only a small proportion of transplanted MSCs differentiate into hepatocyte-like cells, suggesting that they primarily promote liver regeneration through mechanisms other than direct differentiation into hepatocytes [61, 62]. Indeed, MSCs can also enhance the repair of injured liver tissue by exerting paracrine effects, which involve the secretion of soluble factors and modulation of inflammation [63].
MSCs have been shown to stimulate hepatocyte proliferation and inhibit hepatocyte apoptosis in rodent models of acute liver injury [64,65,66,67,68]. Secretory products of various MSCs that have been implicated in hepatocyte proliferation include HGF, VEGF, interleukin-10 (IL-10), and PGE2 [66, 69, 70]. HGF is a growth factor that stimulates the proliferation of hepatocytes and several other cell types by activating the c-Met receptor [71], and it has been shown that UMSCs can promote liver regeneration in rats with acute-on-chronic liver failure through an increase in HGF expression [69]. VEGF is a growth factor that promotes hepatocyte proliferation by stimulating the regeneration of endothelial cells, and consequently, the liver sinusoids [72, 73]. It has been shown to support hepatocyte proliferation in rodent models of acute liver injury [67] and PH [72, 73]. IL-10 is an anti-inflammatory cytokine that has been implicated in mediating the immunomodulatory and regenerative effects of AMSCs in the context of acute kidney injury [66], while PGE2 is a vasoactive factor that has been shown to mediate the anti-apoptotic and pro-proliferative effects of BMSCs towards hepatocytes in a mouse model of acute liver failure [70].
The capacity of MSCs to attenuate liver fibrosis and inflammation has also been reported in several studies [74, 75]. BMSCs can modulate the proliferation of hepatic stellate cells [74], which are responsible for the production of collagen-rich extracellular matrix (ECM) in the liver in response to injury, and regulate the expression of matrix metalloproteinases (MMPs) [75], which mediate the degradation and remodeling of ECM in fibrotic livers. MSCs also exert immunomodulatory activity that affects both the innate and adaptive arms of the immune system. In animal models of liver disease, BMSCs promoted the polarization of macrophages to the immunomodulatory M2 phenotype through the secretion of anti-inflammatory cytokines, such as chemokine ligand 1 and IL-10 [76, 77]. Various MSC types have also been shown to promote the generation of regulatory T-cells and suppress the activation of effector T-cells through the secretion of several molecules, such as inducible NO synthase, HGF, MMPs, PGE2, and transforming growth factor beta (TGF-β) [53].
HSCs represent a small population of self-renewing, multipotent cells that lie at the apex of the hematopoietic system. These cells are characterized by the expression of CD34 and CD133, and they have been used in several clinical studies of liver regeneration because of their plasticity [78]. HSCs are hypothesized to aid in liver regeneration primarily through hepatocyte differentiation and hepatocyte fusion [79]. HSCs are isolated from the patient prior to PVE via leukapheresis of the peripheral blood or directly from bone marrow. Given that many HSC investigations employ granulocyte colony–stimulating factor for mobilization into the peripheral blood, it is important to understand how the administration of this growth factor affects liver regeneration. Granulocyte colony–stimulating factor infusion in patients is often accompanied by an increase in the serum levels of growth factors that play a role in liver regeneration, such as HGF and VEGF [80]. Hence, this may be a confounding factor in understanding the mechanism of PVESA involving HSCs.
USSCs, also known as MSC progenitors, are stem cells that can be isolated from cord blood and display a broad differentiation potential for ectodermal, mesodermal, and endodermal cell types. Similar to MSCs, these cells also have relatively low immunogenicity, which allows allogeneic transplantation [81]. USSCs have been shown to differentiate into hepatocytes [50], although it is unclear whether they can generate secretory products that can support hepatocyte growth.
SHPCs, also known as small hepatocytes, are a special subset of hepatic progenitor cells that emerge in rat livers treated with retrorsine and a 70% PH. Retrorsine is a pyrrolizidine alkaloid that binds DNA and inhibits hepatocyte proliferation. In livers treated with retrorsine, SHPCs can be distinguished from surrounding hepatocytes through their smaller and darker-staining nuclei, as well as fine fat droplets in the cytoplasm [82]. These cells represent a less differentiated population and have been reported to be more resistant to several forms of toxic injury [83]. Similar to HSCs, these stem cells are hypothesized to aid in liver regeneration primarily through hepatocyte differentiation.
Preclinical in Vivo Studies of PVESA
The efficacy of PVESA has been explored in several preclinical in vivo studies using murine, swine, and ovine models, as shown in Table 1.
The first animal studies focused on the effect of PVESA in the context of regenerating healthy livers. Liska et al. first evaluated the intraportal injection of allogeneic BMSCs stained with 5-bromo-2-deoxyuridine following PVE in 6-week-old piglets and found that the BMSC group demonstrated a significantly larger non-ligated lobe than did the control group on the third and seventh days after surgery. Although the BMSC group had 30% larger non-ligated lobes on average at the end of the experiment, the difference between the groups lost statistical significance on the 10th and 14th days, suggesting that the added benefit of BMSC augmentation to liver growth is more pronounced early during hepatic regeneration. Both groups followed similar patterns of serum aspartate transaminase, alanine transaminase, alkaline phosphatase, bilirubin, and gamma-glutamyltransferase. At the end of the experiment, the Ki-67 proliferative index was practically the same between the two groups and equal to levels found in a normal liver. Few 5-bromo-2-deoxyuridine-stained cells were found in the liver, which is why the authors concluded that the injected BMSCs enhanced liver regeneration mainly through the establishment of a supportive micromilieu for pre-existing liver hepatocytes instead of repopulating the liver through differentiation into hepatocytes [47].
In another study using a swine model, the intraarterial injection of human adipose tissue–derived stromal vascular fraction—a heterogeneous mix of various cell populations, including AMSCs, endothelial progenitor cells, and vascular smooth muscle cells—normalized the transcriptomic profile of the regenerating liver after 9 days, while the control group had 39 differentially expressed genes related to fibrosis and inflammation. However, the intravenous administration of hydrocortisone in the adipose tissue–derived stromal vascular fraction group to prevent immune rejection could be a confounder in the observed reduction in fibrosis and inflammation. The research is also constrained by a small sample size, and the authors suggested increasing the number of biological replicates and including additional time points for succeeding studies [84].
Ghodsizad et al. reported that human USSCs can support hepatic regeneration in an ovine model by differentiating into hepatocytes within 4 weeks. However, liver tests and volumetry were not reported, which limits the assessment of the treatment’s impact on hepatic regeneration [50].
Given that many liver cancer patients have varying degrees of chronic liver damage, it is imperative to evaluate PVESA in the context of chronic liver disease. Li et al. investigated the intraportal injection of autologous PKH26-labeled BMSCs in cirrhotic Sprague-Dawley rats and found that the BMSC group had a significantly higher FLR to total liver weight ratio (Fig. 3), Ki-67 proliferation index, and serum albumin level than did the control group at 14 and 28 days after PVE. The BMSC group also had a decreased level of total bilirubin as well as hydroxyproline and collagen content in the liver. Gene expression studies revealed the FLR of the BMSC-treated group had a significantly higher expression of VEGF, HGF, IL-10, and MMP-9. The PKH26-labeled BMSCs differentiated into functional hepatocytes and expressed hepatocyte-specific markers, such as α-fetoprotein, cytokeratin 18, and albumin. Overall, this study supports the dual role of MSCs in augmenting liver growth after PVE, as it has been shown that they differentiate into hepatocytes and improve the local microenvironment by reducing fibrosis in a liver fibrosis model [48]. Nonetheless, it is important to note that on days 14 and 28, the BMSC group had significantly higher aspartate transaminase and alanine transaminase than the control group. Although cell emboli were not detected in this study, the observed elevation in liver enzymes may be attributed to the presence of these masses, since they can cause significant ischemia and elevate serum aminotransferases once they reach the hepatic sinusoids [85].

Liver growth after PVESA in cirrhotic rats. (a) Ratios of FLR versus total liver weight as well as (b) Ki-67-positive cells among the three groups were significantly different (p < 0.001), with the BMSC-treated group showing the highest values at days 14 and 28 after surgery (*, p < 0.001; BMSCs, bone marrow-derived mesenchymal stem cells; FLR, future liver remnant; LI, labeling index; SO, sham operation). (c/d) Representative immunohistochemistry slides for the BMSC-treated (c) and PVE-only control (d) groups show higher expression of Ki-67 (brown nuclear stains) in the BMSC-treated liver. Images have been adapted from Li et al., 2013 [48]. The figure has been created using Biorender.com
Lastly, Miyazaki et al. evaluated the splenic implantation of AMSCs and SHPCs after liver irradiation and PVL and found that both cell types had successfully migrated and engrafted into the irradiated liver after 8 weeks [51]. Notably, SHPCs showed more significant hepatic proliferation, but AMSCs did not, suggesting that the activity of MSCs may differ in the context of the regeneration of an irradiated liver.
Clinical Studies on PVESA
The efficacy of PVESA has been tested in several clinical studies in patients with liver tumors, such as CCA, HCC, mCRC, and metastatic neuroendocrine tumors, as shown in Table 2.
The benefit of PVESA in patients with liver malignancy was first reported by am Esch et al. in a small study involving three cases treated with intraportal injection of autologous CD133 + BMSCs after PVE and three controls who underwent PVE alone. The BMSC-treated group had a 2.5-fold higher mean daily gain in FLR volume compared to the control group (p < 0.01), and all BMSC-treated patients had sufficient FLR for liver resection. Two control patients did not undergo resection due to disease progression in the FLR [86].
Furst et al. expanded on the first study by increasing the number of patients to 6 BMSC-treated cases and 7 PVE-only controls. Similarly, the BMSC-treated group had a 2.3-fold higher mean daily gain in FLR volume compared to the control group (p = 0.03). All BMSC-treated patients had sufficient FLR and underwent extended hepatectomy. Six PVE-only controls underwent extended hemihepatectomy, but their time to surgery was 1.7x longer for the control group versus the treated group (p = 0.057), which supports the hypothesis that PVESA can accelerate the growth of the FLR. One treated and one control patient had minimal dislocation of the embolic agent [87].
To evaluate the functional and survival outcomes after extended right hepatectomy, am Esch et al. conducted a retrospective study involving 11 BMSC-treated cases, 11 PVE-only cases, and 18 controls with no presurgical FLR expansion. They found no significant differences among the groups in terms of functional parameters on postoperative day 7, but FLR expansion was found to be positively associated with overall survival. A post hoc analysis revealed that the BMSC group (p = 0.028) had significantly longer survival compared with controls. The median overall survival durations were 27, 20, and 6 months in the PVESA, PVE, and control groups, respectively. There were no complications associated with PVE, alone or with PVESA, before the extended right hepatectomy. Two PVESA and three PVE-alone patients were not able to undergo extended right hepatectomy because of unresectable disease or physical impairment [88].
Aside from CD133 + BMSCs, HSCs have also been utilized in clinical investigations of PVESA. Treska et al. reported the benefit of autologous CD133 + HSCs after PVE in 5 cases of HCC or mCRC. Increases in FLR volume (> 30%) occurred in all cases 2–4 weeks following PVESA. Three patients had sufficient FLR and underwent resection. One patient had severe intra-abdominal adhesions, while the last patient experienced tumor progression, which hampered resection [49]. Similarly, Canepa et al. reported that the intraportal injection of autologous CD133 + HSCs after PVE results in a higher FLR volume gain compared to that in PVE-only patients [89].
Lastly, Han et al. evaluated the intraportal injection of HSCs after PVE in a randomized trial and found that the daily hepatic volume growth in the HSC-treated group was significantly higher than that in the PVE-only group [90].
Overall, clinical studies demonstrate that stem cell augmentation is a generally safe procedure that enhances liver growth after PVE. However, larger trials are needed to validate the clinical benefit seen in the aforementioned studies. Moreover, none of the clinical investigations have evaluated the behavior of the delivered stem cells and the expression of relevant signaling pathways in the FLRs. Hence, more extensive biological studies must be conducted in further clinical studies to better shape our understanding of the underlying mechanisms of liver regeneration in the context of PVESA, especially in humans(Fig. 4).

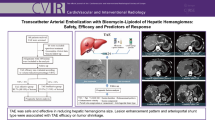
Liver growth after PVESA in a patient with HCC. (a) Axial helical computed tomography scans before and (b) 14 days after PVE and intraportal autologous CD133 + BMSC application revealed marked growth of segments II and III, marked by white arrows (black arrowhead, dislocated cyanoacrylate-to-iodinized oil particle; black arrow, hepatocellular carcinoma). Images have been adapted with permission from Fürst et al. 2007 [87]. The figure has been created using Biorender.com
Future Directions
PVESA has been shown to enhance the degree and rapidity of FLR growth in various studies, but this technique has not yet seen widespread adoption. To facilitate the clinical translation of PVESA, several issues must be addressed. These include the identification of optimal stem cell types, refinement of stem cell collection and administration, appraisal of novel stem cell technologies for potential integration, and evaluation of underlying mechanisms to maximize FLR growth and minimize tumor progression.
Stem Cell Selection
The stem cell types utilized in clinical studies of PVESA have been limited to BMSCs and HSCs. However, there is still no definitive standard regarding which type of stem cells should be utilized for liver regeneration in the context of PVE. BMSCs are highly suitable for autologous transplantation, but the isolation method is invasive and may cause adverse effects, such as injury and site inflammation. Moreover, it should be noted that although the research surrounding adult stem cells for FLR growth is promising, adult stem cells may not be versatile and durable, especially in older patients. Alternatively, UMSCs, which may be obtained from tissue that might otherwise have been disposed, have been shown to have a lower immunogenicity and higher self-renewal and differentiation capacity than BMSCs. In addition, because these cells originated from early-phase tissue, they do not experience an age-related decline in proliferation that weakens the therapeutic effect of MSCs. AMSCs are also easier to obtain than BMSCs, but they have been shown to have lower proliferative and immunomodulatory capacity [53]. On the other hand, HSCs may also be mobilized from the bone marrow to the peripheral blood to facilitate a less invasive isolation process. However, mobilization typically involves the administration of granulocyte colony–stimulating factor, which may be a confounding factor in stimulating liver growth. Comparative studies are necessary to evaluate the performance of various stem cell types.
Stem Cell Collection and Administration
Although all clinical studies on PVESA have used autologous stem cell transplantation, allogeneic transplantation is emerging as an attractive alternative because of the low immunogenicity of several stem cell types. In many patients with co-morbid conditions, the type and amount of stem cells may be compromised, and the time it could take to obtain a sufficient number of stem cells could cause physicians to miss the window of treatment for patients with liver malignancies and chronic liver disease [53]. Although most research studies have administered stem cells into the main portal vein following PVE, the optimal dosage and route of stem cell administration remain unknown. At present, it is unclear whether systemic administration is sufficient. The timing of administration, potentially at multiple time points, may improve stem cell engraftment into the liver since a major limitation of PVESA is the rapid washout of the stem cells from the delivery site. In the case of MSCs, most studies have shown that less than 5% of administered cells are present in the target tissue a few hours after transplantation [91]. Hence, different techniques for stem cell collection and administration should be investigated thoroughly to determine which approach produces the greatest benefit with the least risk to the patient.
Novel Stem Cell Technologies
Novel stem cell technologies are currently being developed to improve the efficacy of stem cells for liver regeneration. Advancements in this area are mostly focused on MSCs and include techniques such as priming, genetic manipulation, and extracellular vesicle (EV)-based therapy [92, 93]. Priming is a pre-conditioning process that involves the exposure of cells to cytokines, growth factors, and selected microenvironments to enhance their survival and augment their valuable properties. In the case of MSCs, studies have demonstrated that various priming strategies can promote their survival and amplify their immunomodulatory secretions. These strategies include the use of cytokines, growth factors, hypoxia, and three-dimensional culture conditions [94]. In the context of liver regeneration, it has been shown that the exposure of AMSCs to low-dose lipopolysaccharide (LPS)—a potent endotoxin that induces the release of proinflammatory cytokines—for 24 h can increase their expression of IL-6, TNF-α, HGF, and VEGF, and the infusion of LPS-conditioned media can significantly enhance liver regeneration following PH in mice [95]. Priming of BMSCs with TGF-β—a major fibrogenic cytokine—has been shown to enhance their ability to engraft into the liver and to reduce inflammation and necrosis in mice with liver injury [96]. Similarly, priming of BMSCs with melatonin has been shown to enhance their ability to home and to reduce lipid accumulation, fibrosis, and hepatocyte apoptosis in rats with induced liver fibrosis [97].
Another emerging strategy is the genetic modification of MSCs through the use of viral vectors. Studies have shown the overexpression of HGF in BMSCs enhanced the BMSCs’ ability to prevent liver failure and reduce mortality in rats with small-for-size liver grafts [98] as well as enhance their ability to attenuate liver injury in rats with induced liver fibrosis [99]. The overexpression of hepatic nuclear factor 4 alpha—a transcription factor that plays an important role in hepatocyte maturation—has been shown to enhance the ability of BMSCs to reduce inflammation and attenuate liver injury in mice with induced liver fibrosis [100]. In another study, overexpression of CC motif chemokine receptor 2—the receptor for monocyte chemoattractant protein-1—enhanced the ability of UMSCs to localize to the liver, reduce inflammation, and promote recovery in mice with acute liver failure [101]. While the aforementioned studies did not report major adverse effects associated with the use of viral vectors, it is still important to remain vigilant regarding potential risks, such as immunogenicity and vector-related toxicity.
EVs refer to lipid membrane vesicles that contain bioactive cargoes (e.g., proteins, lipids, nucleic acids) and are released by cells into the extracellular space to mediate intercellular communication and elicit diverse biological responses in recipient cells [102]. Exosomes refer to a subset of vesicles that are smaller than 200 nm. Although numerous cell types have been documented to secrete therapeutically active EVs, MSC-derived EVs are the most advanced in preclinical and clinical studies due to the well-established therapeutic benefits of MSC [102]. EVs derived from different MSC types have been shown to promote liver regeneration in preclinical models of liver injury via modulation of inflammation and attenuation of oxidative stress [103,104,105]. UMSC-derived EVs have been shown to modulate the expression of CD154—a member of the TNF superfamily and a stimulant of immune response—in intrahepatic CD4 + T-cells in mice with liver ischemia/reperfusion injury [103]. BMSCs have also been shown to regulate the miRNA content of the exosomes within the hepatic microenvironment and down-regulate the expression of CXC motif chemokine ligand 8—a pro-inflammatory cytokine elevated in patients with acute liver failure [104]. Glutathione peroxidase 1-containing exosomes from UMSCs have also rescued mice from induced liver failure by reducing oxidative stress and hepatocyte apoptosis [105]. Similarly, EVs have also been shown to promote liver regeneration following PH. Exosomes derived from UMSCs contain miRNAs that can promote liver regeneration after PH in rats [106]. EVs are an attractive alternative for MSCs due to their simpler storage and administration compared to MSCs. Nevertheless, further research is needed to resolve issues surrounding EVs, such as biodistribution, pharmacodynamics, and cellular fate post-uptake.
Mechanistic Studies and Larger Trials
Despite the potential of PVESA, obstacles such as limited understanding of its mechanisms and the lack of standardized protocols hinder its adoption in interventional radiology. The exact mechanisms by which each stem cell type enhances FLR growth following PVE are not completely understood. Moreover, although current studies do not show an increased risk of cancer progression with PVESA, more investigations are needed to thoroughly understand this process. Most animal studies on PVESA have used models without liver tumors, which prevents an expansive evaluation of the effects of PVESA on tumor biology. The establishment of orthotopic models for PVESA could provide baseline information and mechanistic insights that can address the concerns surrounding PVESA’s safety and efficacy. Additionally, further insight into the specific factors that could support stem cell–induced FLR growth and inhibit tumor progression could give rise to novel approaches, such as the use of biologics and combination therapies. Nine years have elapsed since the last publication of the results of a randomized trial on PVESA. A clinical investigation of the efficacy of autologous CD133 + HSCs in augmenting liver growth after PVE patients with mCRC was recently completed in 2021 (NCT03803241); the results are still pending. Ultimately, randomized-controlled clinical trials with greater numbers of participants and more in-depth biological studies of human tissue samples must eventually be performed to validate the safety and efficacy of PVESA, especially within the context of alternative FLR techniques, such as LVD and ALPPS.
Conclusion
PVESA is an exciting method for enhancing FLR growth before resection. Any technique that enhances the magnitude and rate of FLR hypertrophy will necessarily translate into an increased number of patients with liver cancer who may undergo curative resection while minimizing the risk of post-operative liver insufficiency and death. Much remains unknown regarding the mechanism by which stem cells enhance growth following PVE, yet this procedure has been shown repeatedly to increase FLR size compared to traditional PVE. The utility of PVESA within the context of newer techniques used to induce greater degrees of FLR hypertrophy (i.e., LVD and ALPPS) needs to be elucidated. An advantage of MSCs is their ability to attenuate liver inflammation and fibrosis. Many patients with liver malignancy will have underlying chronic liver disease. While there are multiple techniques capable of inducing FLR hypertrophy prior to major liver surgery, PVESA may also address the underlying quality of the FLR. Thus, further elucidation of the driving mechanisms of PVESA may unlock even more advanced and practical treatments to enhance FLR volume and perhaps address underlying liver disease.
Data Availability
Not applicable.
Code Availability
Not applicable.
Abbreviations
- AMSC:
-
Adipose tissue-derived mesenchymal stem/stromal cell
- ASVF:
-
Adipose tissue–derived stromal vascular fraction
- BMSC:
-
Bone marrow–derived mesenchymal stem/stromal cell
- CCA:
-
Cholangiocarcinoma
- ECM:
-
Extracellular matrix
- EGF:
-
Epidermal growth factor
- EV:
-
Extracellular vesicle
- FLR:
-
Future liver remnant
- HCC:
-
Hepatocellular carcinoma
- HGF:
-
Hepatocyte growth factor
- HPC:
-
Hepatic progenitor cells
- HSC:
-
Hematopoietic stem cell
- IL:
-
Interleukin
- LPS:
-
Lipopolysaccharide
- mCRC:
-
Metastatic colorectal cancer
- MMP:
-
Matrix metalloproteinase
- mNET:
-
Metastatic neuroendocrine tumor
- MSC:
-
Mesenchymal stem/stromal cell
- NBCA:
-
N-butyl-cyanoacrylate
- NO:
-
Nitric oxide
- PGE2 :
-
Prostaglandin E2
- PH:
-
Partial hepatectomy
- PVE:
-
Portal vein embolization
- PVESA:
-
PVE with stem cell augmentation
- SHPC:
-
Small hepatocyte-like progenitor cell
- TGF:
-
Transforming growth factor
- TLV:
-
Total liver volume
- UMSC:
-
Umbilical cord-derived mesenchymal stem/stromal cell
- USSC:
-
Unrestricted somatic stem cell
- VEGF:
-
Vascular endothelial growth factor
References
Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., & Bray, F. (2021). Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. C Ca: A Cancer Journal for Clinicians, 71(3), 209–249.
Makuuchi, M., Takayasu, K., Takuma, T., Yamazaki, S., Hasegawa, H., Nishiura, S., & Shimamura, Y. (1984). Preoperative transcatheter embolization of the portal venous branch for patients receiving extended lobectomy due to the bile duct carcinoma. Nihon Rinsho Geka Gakkai Zasshi (Journal of Japan Surgical Association), 45, 1558–1564.
Shindoh, J., Vauthey, J. N., Zimmitti, G., Curley, S. A., Huang, S. Y., Mahvash, A., Gupta, S., Wallace, M. J., & Aloia, T. A. (2013). Analysis of the efficacy of portal vein embolization for patients with extensive liver malignancy and very low future liver remnant volume, including a comparison with the associating liver partition with portal vein ligation for staged hepatectomy approach. American Journal of Surgery, 217(1), 126–133.
Siriwardana, R. C., Lo, C. M., Chan, S. C., & Fan, S. T. (2012). Role of portal vein embolization in hepatocellular carcinoma management and its effect on recurrence: A case-control study. World Journal of Surgery, 36(7), 1640–1646.
Cassese, G., Han, H. S., Lee, B., Cho, J. Y., Lee, H. W., Guiu, B., & Panaro, F. (2022). Troisi R. I. Portal vein embolization failure: Current strategies and future perspectives to improve liver hypertrophy before major oncological liver resection. World Journal of Gastrointestinal Oncology, 14(11), 2088–2096.
Guiu, B., Quenet, F., Escal, L., Bibeau, F., Piron, L., Rouanet, P., Fabre, J. M., Jacquet, E., Denys, A., Kotzki, P. O., Verzilli, D., & Deshayes, E. (2017). Extended liver venous deprivation before major hepatectomy induces marked and very rapid increase in future liver remnant function. European Radiology, 27(8), 3343–3352.
Schnitzbauer, A. A., Lang, S. A., Goessmann, H., Nadalin, S., Baumgart, J., Farkas, S. A., Fichtner-Feigl, S., Lorf, T., Goralcyk, A., Hörbelt, R., Kroemer, A., Loss, M., Rümmele, P., Scherer, M. N., Padberg, W., Königsrainer, A., Lang, H., & Obed, A. (2012). Schlitt H. J. Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Annals of Surgery, 255(3), 405–414.
Cassese, G., Troisi, R. I., Khayat, S., Benoudifa, B., Quenet, F., Guiu, B., & Panaro, F. (2023). Liver venous deprivation versus portal vein embolization before major hepatectomy for colorectal liver metastases: A retrospective comparison of short- and medium-term outcomes. Journal of Gastrointestinal Surgery, 27(2), 296–305.
Abulkhir, A., Limongelli, P., Healey, A. J., Damrah, O., Tait, P., Jackson, J., & Habib, N. (2008). Jiao L. R. Preoperative portal vein embolization for major liver resection: A meta-analysis. Annals of Surgery, 247(1), 49–57.
May, B. J., & Madoff, D. C. (2012). Portal vein embolization: Rationale, technique, and current application. Semin Intervent Radiol, 29(2), 81–89.
Aussilhou, B., Lesurtel, M., Sauvanet, A., Farges, O., Dokmak, S., Goasguen, N., Sibert, A., Vilgrain, V., & Belghiti, J. (2008). Right portal vein ligation is as efficient as portal vein embolization to induce hypertrophy of the left liver remnant. Journal of Gastrointestinal Surgery : Official Journal of the Society for Surgery of the Alimentary Tract, 12(2), 297–303.
Schnitzbauer, A. A., Lang, S. A., Goessmann, H., Nadalin, S., Baumgart, J., Farkas, S. A., Fichtner-Feigl, S., Lorf, T., Goralcyk, A., Horbelt, R., Kroemer, A., Loss, M., Rummele, P., Scherer, M. N., Padberg, W., Konigsrainer, A., Obed, L. H. K., & Schlitt, A. (2012). Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Annals of Surgery, 255(3), 405–414.
Jones, R. P., Jackson, R., Dunne, D. F., Malik, H. Z., Fenwick, S. W., Poston, G. J., & Ghaneh, P. (2012). Systematic review and meta-analysis of follow-up after hepatectomy for colorectal liver metastases. British Journal of Surgery, 99(4), 477–486.
Kawaguchi, Y., Kopetz, S., Panettieri, E., Hwang, H., Wang, X., Cao, H. S. T., Tzeng, C. D., Chun, Y. S., Aloia, T. A., & Vauthey, J. (2022). N. Improved survival over time after resection of colorectal liver metastases and clinical impact of multigene alteration testing in patients with metastatic colorectal cancer. Journal of Gastrointestinal Surgery : Official Journal of the Society for Surgery of the Alimentary Tract, 26(3), 583–593.
Rous, P., & Larimore, L. D. (1920). Relation of the portal blood to liver maintenance: A demonstration of liver atrophy conditional on compensation. Journal of Experimental Medicine, 31(5), 609–632.
Yokoyama, Y., Nagino, M., & Nimura, Y. (2007). Mechanisms of hepatic regeneration following portal vein embolization and partial hepatectomy: A review. World Journal of Surgery, 31(2), 367–374.
Kiseleva, Y. V., Antonyan, S. Z., Zharikova, T. S., Tupikin, K. A., Kalinin, D. V., & Zharikov, Y. O. (2021). Molecular pathways of liver regeneration: A comprehensive review. World Journal of Hepatology, 13(3), 270–290.
Szijártó, A., & Fülöp, A. (2015). Triggered liver regeneration: From experimental model to clinical implications. European Surgical Research, 54(3–4), 148–161.
Tao, Y., Wang, M., Chen, E., & Tang, H. (2017). Liver regeneration: Analysis of the main relevant signaling molecules. Mediators Inflamm, 2017, 4256352.
Takeuchi, E., Nimura, Y., Mizuno, S., Nagino, M., Shoji-Kawaguchi, M., Izuta, S., & Yoshida, S. (1996). Ligation of portal vein branch induces DNA polymerases alpha, delta, and epsilon in nonligated lobes. Journal of Surgical Research, 65(1), 15–24.
Gilgenkrantz, H., & Collin de l’Hortet, A. (2018). Understanding liver regeneration: From mechanisms to regenerative medicine. American Journal of Pathology, 188(6), 1316–1327.
Le Roy, B., Dupré, A., Gallon, A., Chabrot, P., Gagnière, J., & Buc, E. (2018). Liver hypertrophy: Underlying mechanisms and promoting procedures before major hepatectomy. Journal of Visceral Surgery, 155(5), 393–401.
Takamura, K., Tsuchida, K., Miyake, H., Tashiro, S., & Sugino, H. (2005). Activin and activin receptor expression changes in liver regeneration in rat. Journal of Surgical Research, 126(1), 3–11.
Lambotte, L., Li, B., Leclercq, I., Sempoux, C., Saliez, A., & Horsmans, Y. (2000). The compensatory hyperplasia (liver regeneration) following ligation of a portal branch is initiated before the atrophy of the deprived lobes. Journal of Hepatology, 32(6), 940–945.
Kim, R. D., Kim, J. S., Watanabe, G., & Mohuczy, D. (2008). Behrns K. E. Liver regeneration and the atrophy-hypertrophy complex. Semin Intervent Radiol, 25(2), 92–103.
Vauthey, J. N., Abdalla, E. K., Doherty, D. A., Gertsch, P., Fenstermacher, M. J., Loyer, E. M., Lerut, J., Materne, R., Wang, X., Encarnacion, A., Herron, D., Mathey, C., Ferrari, G., Charnsangavej, C., Do, K. A., & Denys, A. (2002). Body surface area and body weight predict total liver volume in western adults. Liver Transplantation, 8(3), 233–240.
May, B. J., Talenfeld, A. D., & Madoff, D. C. (2013). Update on portal vein embolization: Evidence-based outcomes, controversies, and novel strategies. Journal of Vascular and Interventional Radiology, 24(2), 241–254.
Chansangrat, J., & Keeratibharat, N. (2021). Portal vein embolization: Rationale, techniques, outcomes and novel strategies. Hepat Oncol, 8(4), Hep42.
Luz, J. H. M., Gomes, F. V., Coimbra, E., Costa, N. V., & Bilhim, T. (2020). Preoperative portal vein embolization in hepatic surgery: A review about the embolic materials and their effects on liver regeneration and outcome. Radiol Res Pract, 2020, 9295852.
Luz, J. H. M., Luz, P. M., Bilhim, T., Martin, H. S., Gouveia, H. R., Coimbra, É., Gomes, F. V., Souza, R. R., Faria, I. M., & de Miranda, T. (2017). N. Portal vein embolization with n-butyl-cyanoacrylate through an ipsilateral approach before major hepatectomy: Single center analysis of 50 consecutive patients. Cancer Imaging, 17(1), 25.
Soykan, E. A., Aarts, B. M., Lopez-Yurda, M., Kuhlmann, K. F. D., Erdmann, J. I., Kok, N., van Lienden, K. P., Wilthagen, E. A., Beets-Tan, R. G. H., van Delden, O. M., Gomez, F. M., & Klompenhouwer, E. (2021). G. predictive factors for hypertrophy of the future liver remnant after portal vein embolization: A systematic review. Cardiovasc Intervent Radiol, 44(9), 1355–1366.
Denys, A., Lacombe, C., Schneider, F., Madoff, D. C., Doenz, F., Qanadli, S. D., Halkic, N., Sauvanet, A., Vilgrain, V., & Schnyder, P. (2005). Portal vein embolization with n-butyl cyanoacrylate before partial hepatectomy in patients with hepatocellular carcinoma and underlying cirrhosis or advanced fibrosis. Journal of Vascular and Interventional Radiology, 16(12), 1667–1674.
Jaberi, A., Toor, S. S., Rajan, D. K., Mironov, O., Kachura, J. R., Cleary, S. P., Smoot, R., St-Germain, T., & Tan, A. (2016). Comparison of clinical outcomes following glue versus polyvinyl alcohol portal vein embolization for hypertrophy of the future liver remnant prior to right hepatectomy. Journal of Vascular and Interventional Radiology, 27(12), 1897–1905e1891.
Sun, J. H., Zhang, Y. L., Nie, C. H., Li, J., Zhou, T. Y., Zhou, G. H., Zhu, T. Y., Chen, L. M., Wang, W. L., & Zheng, S. S. (2018). Effects of liver cirrhosis on portal vein embolization prior to right hepatectomy in patients with primary liver cancer. Oncol Lett, 15(2), 1411–1416.
Breitenstein, S., Apestegui, C., Petrowsky, H., & Clavien, P. A. (2009). State of the art in liver resection and living donor liver transplantation: A worldwide survey of 100 liver centers. World Journal of Surgery, 33(4), 797–803.
Schmucker, D. L. (1998). Aging and the liver: An update. Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, 53(5), B315–320.
Russolillo, N., Ratti, F., Viganò, L., Langella, S., Cipriani, F., Aldrighetti, L., & Ferrero, A. (2015). The influence of aging on hepatic regeneration and early outcome after portal vein occlusion: A case-control study. Annals of Surgical Oncology, 22(12), 4046–4051.
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., Cooper, C., Landi, F., Rolland, Y., Sayer, A. A., Schneider, S. M., Sieber, C. C., Topinkova, E., Vandewoude, M., Visser, M., Zamboni, M., & Sarcopenia (2019). Revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31.
Wang, Q., Wang, A., Li, Z., Sparrelid, E., & Brismar, T. B. (2022). Impact of Sarcopenia on the future liver remnant growth after portal vein embolization and associating liver partition and portal vein ligation for staged hepatectomy in patients with liver cancer: A systematic review. Frontiers in Oncology, 12, 1064785.
Schulze-Hagen, M., Truhn, D., Duong, F., Keil, S., Pedersoli, F., Kuhl, C. K., Lurje, G., Neumann, U., Isfort, P., Bruners, P., & Zimmermann, M. (2020). Correlation between Sarcopenia and growth rate of the future liver remnant after portal vein embolization in patients with colorectal liver metastases. Cardiovasc Intervent Radiol, 43(6), 875–881.
Denbo, J. W., Kim, B. J., Vauthey, J. N., Tzeng, C. W., Ma, J., Huang, S. Y., Chun, Y. S., & Katz, M. H. G. (2021). Aloia T. A. Overall body composition and sarcopenia are associated with poor liver hypertrophy following portal vein embolization. Journal of Gastrointestinal Surgery : Official Journal of the Society for Surgery of the Alimentary Tract, 25(2), 405–410.
Yao, S., Kamo, N., Taura, K., Miyachi, Y., Iwamura, S., Hirata, M., Kaido, T., & Uemoto, S. (2022). Muscularity defined by the combination of muscle quantity and quality is closely related to both liver hypertrophy and postoperative outcomes following portal vein embolization in cancer patients. Annals of Surgical Oncology, 29(1), 301–312.
Mise, Y., Passot, G., Wang, X., Chen, H. C., Wei, S., Brudvik, K. W., Aloia, T. A., Conrad, C., Huang, S. Y., & Vauthey, J. (2016). N. A nomogram to predict hypertrophy of liver segments 2 and 3 after right portal vein embolization. Journal of Gastrointestinal Surgery : Official Journal of the Society for Surgery of the Alimentary Tract, 20(7), 1317–1323.
Niekamp, A. S., Huang, S. Y., Mahvash, A., Odisio, B. C., Ahrar, K., Tzeng, C. D., & Vauthey, J. (2020). N. Hepatic vein embolization after portal vein embolization to induce additional liver hypertrophy in patients with metastatic colorectal carcinoma. European Radiology, 30(7), 3862–3868.
Melandro, F., Giovanardi, F., Hassan, R., Larghi Laureiro, Z., Ferri, F., Rossi, M., Mennini, G., Pawlik, T. M., & Lai, Q. (2019). Minimally invasive approach in the setting of alpps procedure: A systematic review of the literature. Journal of Gastrointestinal Surgery : Official Journal of the Society for Surgery of the Alimentary Tract, 23(9), 1917–1924.
Gouw, A. S., Clouston, A. D., & Theise, N. D. (2011). Ductular reactions in human liver: Diversity at the interface. Hepatology, 54(5), 1853–1863.
Liska, V., Slowik, P., Eggenhofer, E., Treska, V., Renner, P., Popp, F. C., Mirka, H., Kobr, J., Sykora, R., Schlitt, H. J., Holubec, L., Chlumska, A., Skalicky, T., Matejovic, M., & Dahlke, M. H. (2009). Intraportal injection of porcine multipotent mesenchymal stromal cells augments liver regeneration after portal vein embolization. In Vivo, 23(2), 229–235.
Li, T., Zhu, J., Ma, K., Liu, N., Feng, K., Li, X., Wang, S., & Bie, P. (2013). Autologous bone marrow-derived mesenchymal stem cell transplantation promotes liver regeneration after portal vein embolization in cirrhotic rats. Journal of Surgical Research, 184(2), 1161–1173.
Treska, V., Koza, V., Lysak, D., Slauf, F., Mirka, H., Sutnar, A., Skalicky, T., Fichtl, J., & Ferda, J. (2013). Portal vein embolization and application of autologous stem cells in patients with primary unresectable liver tumours. Bratislavske Lekarske Listy, 114(7), 389–393.
Ghodsizad, A., Fahy, B. N., Waclawczyk, S., Liedtke, S., Gonzalez Berjon, J. M., Barrios, R., Mehrabi, A., Karck, M., Ruhparwar, A., & Kögler, G. (2012). Portal application of human unrestricted somatic stem cells to support hepatic regeneration after portal embolization and tumor surgery. Asaio j, 58(3), 255–261.
Miyazaki, K., Yamanouchi, K., Sakai, Y., Yamaguchi, I., Takatsuki, M., Kuroki, T., Guha, C., & Eguchi, S. (2013). Construction of liver tissue in vivo with preparative partial hepatic irradiation and growth stimulus: Investigations of less invasive techniques and progenitor cells. Journal of Surgical Research, 185(2), 889–895.
Dominici, M., Le Blanc, K., Mueller, I., Slaper-Cortenbach, I., Marini, F. C., Krause, D. S., Deans, R. J., Keating, A., Prockop, D. J., & Horwitz, E. (2006). M. minimal criteria for defining multipotent mesenchymal stromal cells. The international society for cellular therapy position statement. Cytotherapy, 8(4), 315–317.
Yang, X., Meng, Y., Han, Z., Ye, F., Wei, L., & Zong, C. (2020). Mesenchymal stem cell therapy for liver disease: Full of chances and challenges. Cell & Bioscience, 10(1), 123.
Yin, L., Zhu, Y., Yang, J., Ni, Y., Zhou, Z., Chen, Y., & Wen, L. (2015). Adipose tissue-derived mesenchymal stem cells differentiated into hepatocyte-like cells in vivo and in vitro. Molecular Medicine Reports, 11(3), 1722–1732.
Ju, S., Teng, G. J., Lu, H., Jin, J., Zhang, Y., Zhang, A., & Ni, Y. (2010). In vivo differentiation of magnetically labeled mesenchymal stem cells into hepatocytes for cell therapy to repair damaged liver. Investigative Radiology. ;45(10).
Zhang, G. Z., Sun, H. C., Zheng, L. B., Guo, J. B., & Zhang, X. L. (2017). In vivo hepatic differentiation potential of human umbilical cord-derived mesenchymal stem cells: Therapeutic effect on liver fibrosis/cirrhosis. World Journal of Gastroenterology, 23(46), 8152–8168.
Lin, S. Z., Chang, Y. J., Liu, J. W., Chang, L. F., Sun, L. Y., Li, Y. S., Luo, G. H., Liao, C. H., Chen, P. H., Chen, T. M., Lee, R. P., Yang, K. L., Harn, H. J., & Chiou, T. W. (2010). Transplantation of human wharton’s jelly-derived stem cells alleviates chemically induced liver fibrosis in rats. Cell Transplantation, 19(11), 1451–1463.
Zhao, Q., Ren, H., Li, X., Chen, Z., Zhang, X., Gong, W., Liu, Y., Pang, T., & Han, Z. C. (2009). Differentiation of human umbilical cord mesenchymal stromal cells into low immunogenic hepatocyte-like cells. Cytotherapy, 11(4), 414–426.
Xu, F., Liu, J., Deng, J., Chen, X., Wang, Y., Xu, P., Cheng, L., Fu, Y., Cheng, F., Yao, Y., Zhang, Y., Huang, M., Yu, D., Wei, Y., & Deng, H. (2015). Rapid and high-efficiency generation of mature functional hepatocyte-like cells from adipose-derived stem cells by a three-step protocol. Stem Cell Research & Therapy, 6(1), 193.
Afshari, A., Shamdani, S., Uzan, G., Naserian, S., & Azarpira, N. (2020). Different approaches for transformation of mesenchymal stem cells into hepatocyte-like cells. Stem Cell Research & Therapy, 11(1), 54.
Chen, L., Zhang, C., Chen, L., Wang, X., Xiang, B., Wu, X., Guo, Y., Mou, X., Yuan, L., Chen, B., Wang, J., & Xiang, C. (2016). Human menstrual blood-derived stem cells ameliorate liver fibrosis in mice by targeting hepatic stellate cells via paracrine mediators. Stem Cells Translational Medicine, 6(1), 272–284.
Shi, D., Zhang, J., Zhou, Q., Xin, J., Jiang, J., Jiang, L., Wu, T., Li, J., Ding, W., Li, J., Sun, S., Li, J., Zhou, N., Zhang, L., Jin, L., Hao, S., Chen, P., Cao, H., Li, M., et al. (2017). Quantitative evaluation of human bone mesenchymal stem cells rescuing fulminant hepatic failure in pigs. Gut, 66(5), 955–964.
Pittenger, M. F., Discher, D. E., Péault, B. M., Phinney, D. G., & Hare, J. M. (2019). Caplan A. I. Mesenchymal stem cell perspective: Cell biology to clinical progress. Npj Regenerative Medicine, 4(1), 22.
van Poll, D., Parekkadan, B., Cho, C. H., Berthiaume, F., Nahmias, Y., & Tilles, A. W. (2008). Yarmush M. L. Mesenchymal stem cell-derived molecules directly modulate hepatocellular death and regeneration in vitro and in vivo. Hepatology, 47(5), 1634–1643.
Feng, J., Yao, W., Zhang, Y., Xiang, A. P., Yuan, D., & Hei, Z. (2018). Intravenous anesthetics enhance the ability of human bone marrow-derived mesenchymal stem cells to alleviate hepatic ischemia-reperfusion injury in a receptor-dependent manner. Cellular Physiology and Biochemistry, 47(2), 556–566.
Zhang, S., Zhu, Z., Wang, Y., Liu, S., Zhao, C., Guan, W., & Zhao, Y. (2018). Therapeutic potential of bama miniature pig adipose stem cells induced hepatocytes in a mouse model with acute liver failure. Cytotechnology, 70(4), 1131–1141.
Lotfinia, M., Kadivar, M., Piryaei, A., Pournasr, B., Sardari, S., Sodeifi, N., Sayahpour, F. A., & Baharvand, H. (2016). Effect of secreted molecules of human embryonic stem cell-derived mesenchymal stem cells on acute hepatic failure model. Stem Cells and Development, 25(24), 1898–1908.
Chen, L., Xiang, B., Wang, X., & Xiang, C. (2017). Exosomes derived from human menstrual blood-derived stem cells alleviate fulminant hepatic failure. Stem Cell Research & Therapy, 8(1), 9.
He, Y., Guo, X., Lan, T., Xia, J., Wang, J., Li, B., Peng, C., Chen, Y., Hu, X., & Meng, Z. (2021). Human umbilical cord-derived mesenchymal stem cells improve the function of liver in rats with acute-on-chronic liver failure via downregulating notch and stat1/stat3 signaling. Stem Cell Research & Therapy, 12(1), 396.
Liu, Y., Ren, H., Wang, J., Yang, F., Li, J., Zhou, Y., Yuan, X., Zhu, W., & Shi, X. (2019). Prostaglandin e2 secreted by mesenchymal stem cells protects against acute liver failure via enhancing hepatocyte proliferation. The FASEB Journal, 33(2), 2514–2525.
Araújo, T. G., de Oliveira, A. G., Tobar, N., Saad, M. J., Moreira, L. R., Reis, E. R., Nicola, E. M., de Jorge, G. L., dos Tártaro, R. R., Boin, I. F., & Teixeira, A. R. (2013). Liver regeneration following partial hepatectomy is improved by enhancing the hgf/met axis and akt and erk pathways after low-power laser irradiation in rats. Lasers in Medical Science, 28(6), 1511–1517.
Taniguchi, E., Sakisaka, S., Matsuo, K., Tanikawa, K., & Sata, M. (2001). Expression and role of vascular endothelial growth factor in liver regeneration after partial hepatectomy in rats. Journal of Histochemistry and Cytochemistry, 49(1), 121–130.
Bockhorn, M., Goralski, M., Prokofiev, D., Dammann, P., Grünewald, P., Trippler, M., Biglarnia, A., Kamler, M., Niehues, E. M., Frilling, A., & Broelsch, C. E. (2007). Schlaak J. F. Vegf is important for early liver regeneration after partial hepatectomy. Journal of Surgical Research, 138(2), 291–299.
Parekkadan, B., van Poll, D., Megeed, Z., Kobayashi, N., Tilles, A. W., Berthiaume, F., & Yarmush, M. L. (2007). Immunomodulation of activated hepatic stellate cells by mesenchymal stem cells. Biochemical and Biophysical Research Communications, 363(2), 247–252.
Rabani, V., Shahsavani, M., Gharavi, M., Piryaei, A., Azhdari, Z., & Baharvand, H. (2010). Mesenchymal stem cell infusion therapy in a carbon tetrachloride-induced liver fibrosis model affects matrix metalloproteinase expression. Cell Biology International, 34(6), 601–605.
Watanabe, Y., Tsuchiya, A., Seino, S., Kawata, Y., Kojima, Y., Ikarashi, S., Starkey Lewis, P. J., Lu, W. Y., Kikuta, J., Kawai, H., Yamagiwa, S., Forbes, S. J., Ishii, M., & Terai, S. (2018). Mesenchymal stem cells and induced bone marrow-derived macrophages synergistically improve liver fibrosis in mice. Stem Cells Translational Medicine, 8(3), 271–284.
Li, C., Jin, Y., Wei, S., Sun, Y., Jiang, L., Zhu, Q., Farmer, D. G., Busuttil, R. W., Kupiec-Weglinski, J. W., & Ke, B. (2019). Hippo signaling controls nlr family pyrin domain containing 3 activation and governs immunoregulation of mesenchymal stem cells in mouse liver injury. Hepatology, 70(5), 1714–1731.
Siapati, E. K., Roubelakis, M. G., & Vassilopoulos, G. (2022). Liver regeneration by hematopoietic stem cells: Have we reached the end of the road? Cells, 11, 15.
Soares-da-Silva, F., Peixoto, M., & Cumano, A. (2020). Pinto-do-Ó P. Crosstalk between the hepatic and hematopoietic systems during embryonic development. Front Cell Dev Biol, 8, 612.
Fujii, K., Ishimaru, F., Kozuka, T., Matsuo, K., Nakase, K., Kataoka, I., Tabayashi, T., Shinagawa, K., Ikeda, K., Harada, M., & Tanimoto, M. (2004). Elevation of serum hepatocyte growth factor during granulocyte colony-stimulating factor-induced peripheral blood stem cell mobilization. British Journal of Haematology, 124(2), 190–194.
Akhavan Rahnama, M., Soufi Zomorrod, M., Abroun, S., & Atashi, A. (2023). The effect of exosomes derived from unrestricted somatic stem cells on murine model of sepsis. Cells Tissues Organs, 212(2), 164–175.
Ichinohe, N., Tanimizu, N., & Mitaka, T. (2022). Isolation of small hepatocyte-like progenitor cells from retrorsine/partial hepatectomy rat livers by laser microdissection. In N. Tanimizu (Ed.), Hepatocytes: Methods and protocols (pp. 183–193). Springer US.
Fausto, N., & Campbell, J. S. (2003). The role of hepatocytes and oval cells in liver regeneration and repopulation. Mechanisms of Development, 120(1), 117–130.
Bartas, M., Červeň, J., Oppelt, J., Peteja, M., Vávra, P., Zonča, P., Procházka, V., Brázda, V., & Pečinka, P. (2018). Liver regeneration during the associating liver partition and portal vein ligation for staged hepatectomy procedure in sus scrofa is positively modulated by stem cells. Oncol Lett, 15(5), 6309–6321.
Pastor, C. M. (2005). Tracking mesenchymal stem cells in the liver by magnetic resonance imaging. Journal of Hepatology, 43(5), 915–916.
am Esch, J. S., Knoefel, I. I., Klein, W. T., Ghodsizad, M., Fuerst, A., Poll, G., Piechaczek, L. W., Burchardt, C., Feifel, E. R., Stoldt, N., Stockschläder, V., Stoecklein, M., Tustas, N., Eisenberger, R. Y., Peiper, C. F., & Häussinger, M. (2005). Hosch S. B. Portal application of autologous cd133 + bone marrow cells to the liver: A novel concept to support hepatic regeneration. Stem Cells, 23(4), 463–470.
Fürst, G., Esch, J. S., a., Poll, L. W., Hosch, S. B., Fritz, L. B., Klein, M., Godehardt, E., Krieg, A., Wecker, B., Stoldt, V., Stockschläder, M., Eisenberger, C. F., & Mödder, U. (2007). Knoefel W. T. Portal vein embolization and autologous cd133 + bone marrow stem cells for liver regeneration: Initial experience. Radiology, 243(1), 171–179.
am Esch, J. S., Schmelzle, M., Fürst, G., Robson, S. C., Krieg, A., Duhme, C., Tustas, R. Y., Alexander, A., Klein, H. M., Topp, S. A., Bode, J. G., Häussinger, D., Eisenberger, C. F., & Knoefel, W. T. (2012). Infusion of cd133 + bone marrow–derived stem cells after selective portal vein embolization enhances functional hepatic reserves after extended right hepatectomy: A retrospective single-center study. Annals of Surgery, 255(1), 79–85.
Canepa, M. C., Quaretti, P., Perotti, C., Vercelli, A., Rademacher, J., Peloso, A., Barbieri, L., Franchi, E., Briani, L., Gaspari, A., Brugnatelli, S., Pedrazzoli, P., Dionigi, P., & Maestri, M. (2013). Autologous cd133 + cells augment the effect of portal embolization. Minerva Chir, 68(2), 163–168.
Han, H. S., Ahn, K. S., Cho, J. Y., Yoon, Y. S., Yoon, C. J., Park, K. U., Min, S. K., & Lee, H. K. (2014). Ryu K. H. Autologous stem cell transplantation for expansion of remnant liver volume with extensive hepatectomy. Hepato-Gastroenterology, 61(129), 156–161.
Levit, R. D., Landázuri, N., Phelps, E. A., Brown, M. E., García, A. J., Davis, M. E., Joseph, G., Long, R., Safley, S. A., Suever, J. D., Lyle, A. N., & Weber, C. J. (2013). Taylor W. R. Cellular encapsulation enhances cardiac repair. J Am Heart Assoc, 2(5), e000367.
Shokravi, S., Borisov, V., Zaman, B. A., Niazvand, F., Hazrati, R., Khah, M. M., Thangavelu, L., Marzban, S., Sohrabi, A., & Zamani, A. (2022). Mesenchymal stromal cells (mscs) and their exosome in acute liver failure (alf): A comprehensive review. Stem Cell Research & Therapy, 13(1), 192.
Eom, Y. W., Kang, S. H., Kim, M. Y., Lee, J. I., & Baik, S. (2020). K. Mesenchymal stem cells to treat liver diseases. Ann Transl Med, 8(8), 563.
Noronha, N. C., Mizukami, A., Caliári-Oliveira, C., Cominal, J. G., Rocha, J. L. M., Covas, D. T., Swiech, K., & Malmegrim, K. (2019). C. R. Priming approaches to improve the efficacy of mesenchymal stromal cell-based therapies. Stem Cell Research & Therapy, 10(1), 131.
Lee, S. C., Jeong, H. J., Lee, S. K., & Kim, S. J. (2015). Lipopolysaccharide preconditioning of adipose-derived stem cells improves liver-regenerating activity of the secretome. Stem Cell Research & Therapy, 6(1), 75.
Garg, A., Khan, S., Luu, N., Nicholas, D. J., Day, V., King, A. L., Fear, J., Lalor, P. F., & Newsome, P. N. (2023). Tgfβ(1) priming enhances cxcr3-mediated mesenchymal stromal cell engraftment to the liver and enhances anti-inflammatory efficacy. Journal of Cellular and Molecular Medicine, 27(6), 864–878.
Mortezaee, K., Khanlarkhani, N., Sabbaghziarani, F., Nekoonam, S., Majidpoor, J., Hosseini, A., Pasbakhsh, P., Kashani, I. R., & Zendedel, A. (2017). Preconditioning with melatonin improves therapeutic outcomes of bone marrow-derived mesenchymal stem cells in targeting liver fibrosis induced by ccl4. Cell and Tissue Research, 369(2), 303–312.
Yu, Y., Yao, A. H., Chen, N., Pu, L. Y., Fan, Y., Lv, L., Sun, B. C., Li, G. Q., & Wang, X. H. (2007). Mesenchymal stem cells over-expressing hepatocyte growth factor improve small-for-size liver grafts regeneration. Molecular Therapy, 15(7), 1382–1389.
Zhang, Y., Li, R., Rong, W., Han, M., Cui, C., Feng, Z., Sun, X., & Jin, S. (2018). Therapeutic effect of hepatocyte growth factor-overexpressing bone marrow-derived mesenchymal stem cells on ccl(4)-induced hepatocirrhosis. Cell Death and Disease, 9(12), 1186.
Ye, Z., Lu, W., Liang, L., Tang, M., Wang, Y., Li, Z., Zeng, H., Wang, A., Lin, M., Huang, L., Wang, H., & Hu, H. (2019). Mesenchymal stem cells overexpressing hepatocyte nuclear factor-4 alpha alleviate liver injury by modulating anti-inflammatory functions in mice. Stem Cell Research & Therapy, 10(1), 149.
Xu, R., Ni, B., Wang, L., Shan, J., Pan, L., He, Y., Lv, G., Lin, H., Chen, W., & Zhang, Q. (2022). Ccr2-overexpressing mesenchymal stem cells targeting damaged liver enhance recovery of acute liver failure. Stem Cell Research & Therapy, 13(1), 55.
Toh, W. S., Yarani, R., El Andaloussi, S., Cho, B. S., Choi, C., Corteling, R., De Fougerolles, A., Gimona, M., Herz, J., Khoury, M., Robbins, P. D., Williams, D., Weiss, D. J., Rohde, E., Giebel, B., & Lim, S. (2023). K. A report on the international society for cell & gene therapy 2022 scientific signature series, therapeutic advances with native and engineered human extracellular vesicles. Cytotherapy, 25(8), 810–814.
Zheng, J., Lu, T., Zhou, C., Cai, J., Zhang, X., Liang, J., Sui, X., Chen, X., Chen, L., Sun, Y., Zhang, J., Chen, W., Zhang, Y., Yao, J., Chen, G., & Yang, Y. (2020). Extracellular vesicles derived from human umbilical cord mesenchymal stem cells protect liver ischemia/reperfusion injury by reducing cd154 expression on cd4 + t cells via cct2. Advanced Science, 7(18), 1903746.
Zhang, J., Gao, J., Lin, D., Xiong, J., Wang, J., Chen, J., Lin, B., & Gao, Z. (2021). Potential networks regulated by mscs in acute-on-chronic liver failure: Exosomal mirnas and intracellular target genes. Frontiers in Genetics, 12, 650536.
Yan, Y., Jiang, W., Tan, Y., Zou, S., Zhang, H., Mao, F., Gong, A., Qian, H., & Xu, W. (2017). Hucmsc exosome-derived gpx1 is required for the recovery of hepatic oxidant injury. Molecular Therapy, 25(2), 465–479.
Song, X. J., Zhang, L., Li, Q., Li, Y., Ding, F. H., & Li, X. (2021). Hucb-Msc derived exosomal mir-124 promotes rat liver regeneration after partial hepatectomy via downregulating foxg1. Life Sciences, 265, 118821.
Acknowledgements
The authors would also like to acknowledge Ann Sutton from Editing Services of MD Anderson’s Research Medical Library for editing the manuscript.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization, A.J.R.B., T.C.O., S.M., I.W., H.S.T., J.V., S.Y.H.; data curation, A.J.R.B., T.C.O., S.M., I.W.; writing—original draft preparation, A.J.R.B., T.C.O., S.M., I.W.; writing—review and editing, A.J.R.B., T.C.O., S.M., I.W., H.S.T., J.V., S.Y.H.; supervision, S.Y.H.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors have read and agreed to the published version of the manuscript.
Competing Interests
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Barcena, A.J.R., Owens, T.C., Melancon, S. et al. Current Perspectives and Progress in Preoperative Portal Vein Embolization with Stem Cell Augmentation (PVESA). Stem Cell Rev and Rep (2024). https://doi.org/10.1007/s12015-024-10719-1
Accepted:
Published:
DOI: https://doi.org/10.1007/s12015-024-10719-1