
Abstract
Purpose of review
Type 2 diabetes mellitus (T2DM) is a chronic disease that may lead to severe complications. The main methods of preventing or delaying the onset of T2DM include lifestyle changes. The purpose of this study is to identify and evaluate the effectiveness of workplace interventions aimed at preventing type 2 diabetes. An umbrella review was conducted in accordance with the Cochrane Collaboration guidelines. Searches were performed in Medline (via PubMed), Embase (via OVID), and Cochrane Library databases. The quality assessment of the included studies was performed using the AMSTAR2 tool.
Recent findings
The final analysis included 7 studies. The majority (4 of 7) of the studies included in the review focused on workplace interventions based on the guidelines of the US Diabetes Prevention Program (DPP) or other similar programs. The method of decreasing the risk of type 2 diabetes among employees are programs consisting of multiple approaches aimed at improving parameters associated with diabetes, i.e., body weight, and therefore BMI, reduction, and reducing blood glucose levels, as well as HbA1c levels through educational approach and lifestyle changes. The results of those studies point to multicomponent interventions as more effective than single-component interventions.
Summary
An effective workplace intervention aimed to reduce the risk of type 2 diabetes among employees is a multicomponent program consisting of elements such as educational activities, interventions targeting dietary changes and increased physical activity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The International Diabetes Federation estimated in its 2021 report that 537 million adults aged 20–79 were diagnosed with diabetes worldwide, and forecasted the increase to 643 million in 2030, and to 743 million in 2045. The most common type of diabetes is type 2 diabetes, which accounts for more than 90% of all cases of the disease worldwide. In type 2 diabetes, the increase in blood glucose initially results from insulin-resistance, or the inability of the body cells to respond fully to insulin. This type of impairment results in an increase of insulin production, and over time, due to the inability of pancreatic beta cells to keep up with the demand, insulin production becomes insufficient [1].
Appropriate lifestyle modification has been proven effective in preventing or delaying the onset of type 2 diabetes. The main preventive goals should include achieving and maintaining a appropriate body weight, engaging in physical activity for at least 30 min most days of the week, avoiding intake of sugar and saturated fat, and quitting smoking [2].
One of the most well-known programs aimed at preventing type 2 diabetes is the US-led National Diabetes Prevention Program (DPP). This program was initially a multicenter clinical trial. The researched intervention included lifestyle changes in the form of calorie intake reduction and increased physical activity to at least 150 min per week. The results of this study showed that the structured lifestyle change program contributed to weight loss of participants between 5 and 7% of body weight and reduced the risk of developing type 2 diabetes in high-risk adults by 58% [3•]. Currently, the DPP program indicates a framework for diabetes prevention activities, bringing together both public and private sectors. The program partners include federal agencies, state and local health departments, national and community organizations, employers, public and private insurers, health care professionals, academic community education programs and companies that focus on health [4]. An increasing number of employers and insurers in the USA are offering lifestyle change programs for the prevention of type 2 diabetes as health-insuranc-covered benefit [5].
The purpose of this study is to identify and evaluate the effectiveness of interventions aimed at preventing type 2 diabetes that can be implemented in the workplace.
Given the plethora of systematic reviews in the field of diabetes prevention, the authors have decided to conduct an umbrella review for pooled analysis of the available scientific evidence in the field. The methodology utilized in this study allowed for the identification of the highest-level studies in the hierarchy of scientific evidence.
Material and Method
For this paper, the search of systematic reviews with or without meta-analysis was conducted through Medline (via PubMed), Embase (via OVID) and Cochrane Library databases in accordance to previously prepared strategy (supplementary material). Websites of scientific societies, google scholar, TripDatabase and gray literature were also searched for additional studies or clinical recommendations.
An umbrella review was conducted according to the Cochrane Collaboration guidelines [6]. The search of studies was based on a protocol developed before the work began. It included the criteria for including studies in the review, the search strategy, how studies were selected, and the planned methodology for conducting the analysis and data synthesis. The inclusion criteria for this analysis are cited in the following table (Table 1).
At every step of the review process studies were selected by two independent analysts (J.Ś., K.W.). All discrepancies were solved by means of consensus together with third author (T.T.).
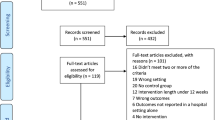
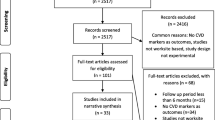
Out of 603 initially included abstracts, 24 studies were chosen for full-text assessment. The study inclusion criteria were met in 7 studies.
The authors have also found an umbrella review by Proper from 2019 [7], where workplace health-promoting intervention had been assessed. Studies included in this review were aimed at assessment of intervention effectiveness in overweight/obese population and reduction of body-weight (14 studies), psychologically healthy (6 studies), musculoskeletal prophylactics (6 studies) and interventions aimed at metabolic risk factors prophylactics (5 studies). This umbrella study yielded an additional study for our analysis—a 2017 narrative systematic review by Hafez [8] referring to workplace intervention for type 2 diabetes prevention. The 2019 umbrella review by Proper also analyzed the 2009 Conn meta-analysis [9], however, that study had already been included for final assessment based on the full-text assessment.
The most common exclusion reasons were intervention issues (lack of information about intervention being conducted at a workplace) and methodology (lack of properly described materials, as well as inconsistencies in results description). Figure 1 depicts each step of the selection process. Lists of included and excluded studies are available in the supplementary material.

PRISMA flow diagram
The quality of the included in the analysis studies was assessed with AMSTAR2 tool [10]. This tool allows for indicating studies of the highest quality; however, it is not including or excluding studies as it is merely a guideline for measuring potential value of results. The highest grade can be awarded to a study in which every questions of the tool yielded positive answers (partial positive is also permissible). A single “no” answer in the critical domain yields study value as “low.” Two or more “no” answers lower the score to “critically low.” The scoring process had been independently performer by two authors (K.W. and J.Ś.). All discrepancies were solved by means of consensus together with third author (T.T.).
Results
The inclusion criteria for umbrella review encompassing intervention analysis aimed at diabetes prevention at the workplace were met by the following studies (n = 7; Fitzpatrick-Lewis 2022, Peñalvo 2021, Inolopú 2019, Brown 2018, Shrestha 2018, Hafez 2017, Conn 2009).
None of the included studies scored high at AMSTAR-2 scale. Most included studies scored a critically low (n = 4). Due to the nature of the 2019 Proper study (an umbrella review), the study has been scored according to AMSTAR-2. Detailed analysis results regarding the quality assessment and risk of error analysis have been included in the supplementary material.
Programs Based on Multicomponent Interventions
According to the results of the 2022 Fitzpatrick-Lewis meta-analysis 2022 conducting in a workplace a structured programs based on US DPP with at least 3 components (health education, diet changes, and increase in physical activity) statistically significantly increases probability body-weight reduction by ≥ 5% (RR = 3.85 [95% CI: (1.58; 9.38)]) and by ≥ 7% (RR = 9.36 [95% CI: (2.31; 37.97)]) in comparison to baseline body-weight among participating employees. Moreover, implementing a DPP-like program statistically significantly influences the decrease of BMI by 0.86 kg/m2 (MD = −0.86 [95% CI: (−1.37; −0.34)]) on average. The 4 RCTs analysis also showed statistically significant increase in physical activity among participants—SMD = 0.38 [95% CI: (0.21; 0.55)] [11•].
In the 2021 Peñalvo meta-analysis an influence of multicomponent wellness programs at workplace on anthropometric measurements and blood glucose levels had been assessed. The authors indicated 9 component groups in those programs: screening (A), individual education (B), group education (C), food environment (D), labeling (E); financial incentives (F), physical Activity (G), self-awareness (H), and others (I). The median time of the intervention was 9 months. According to the meta-analysis results the wellness programs consisting of at least single component from A to I statistically significantly influences lowering of the BMI (kg/m2) (ES = −0.22 [95% CI: (−0.28; −0.17)]), body-weight (kg) (ES = −0.92 [95% CI: (−1.11; −0.72)]), and waist girth (cm) (ES = −1.47 [95% CI: (−1.96; −0.98)]) in participating in the program employees. For the blood glucose level (mg/dl) outcome the wellness programs (A-I components) the parameter had been statistically significantly lowered—ES = −1.81 [95% CI: (−3.33; −0.28)]. The remaining results of the utilized intervention for percentage body fat reducing (%) (ES = −0.80 [95% CI: (−1.80; 0.21)]; A, B, C, D, F, G, H, I components), decreasing the waist-hip ratio (ES = 0.00 [95% CI: (−0.01; 0.00)]; A, B, C, D, F, G components), as well as increase in fat-free body mass (kg) (ES = 1.01 [95% CI: (−0.82; 2.83)]; B, C, G, I components) were not statistically significant [12•].
In the 2019 Inolopú systematic review, the inclusion criteria were met by 10 studies analyzing interventions aimed at preventing the risk factors and type 2 diabetes at workplace. The studies included 7 analyzed conventional lifestyle changes, 2 analyzed online lifestyle coaching, and 1 analyzed dietary coaching. In 8 studies the interventions were based on the DPP (Diabetes Prevention Program), FDPS (Finnish Diabetes Prevention Study), LiSM10! (Life Style Modification Program for Physical Activity and Nutrition program), and NICE guidelines (National Institute for Health and Care Excellence), as well as JDS/ADA (Japan Diabetes Society and the American Diabetes Association). For outcomes, reduction in body-weight, calorie intake, and 2-h post-prandial blood glucose were chosen. According to 6 included studies utilizing at workplace structured programs based on DPP, FDPS, LiSM10!, and NICE guidelines influenced body-weight reduction among employees. Moreover, the dietary interventions based on JDS/ADA guidelines influenced calorie intake and lowering of the 2-h postprandial blood glucose among the employees (1 study). Two of the included studies were aimed at management and treatment of the previously diagnosed diabetes had not shown influence on the analyzed outcomes [13•].
Contrary, in the 2018 Brown systematic review analyzing the influence of prophylactics programs at workplace aimed at diabetes prevention 8 studies were based on DPP (lifestyle parts) and 14 included other prophylactics programs aimed at improvement of nutritional habits, increasing physical activity and/or management diabetes/cardiovascular disease risk factors. The analyzed studies had shown influence on body-weight and BMI reduction among employees (15 out of 20 studies). Additionally, in 6 out of 10 included in the review studies the influence on HbA1c lowering had been shown [14].
The narrative 2017 Hafez systematic review assessed the efficacy of conducting of prophylactics programs aimed at preventing diabetes at workplace included 10 DPP-based studies and 3 with lower than DPP intensity level aimed at life-style changes support through educational sessions, individual consultations, and websites. The results showed DPP-based programs to influence the reduction of body-weight among employees during 3–6 months (range from −0.4 to −5.1 kg; 8 studies), and 7–12 months (range from −1.43 to −4.9 kg; 6 studies). Moreover, the DPP-based interventions influenced HbA1c lowering (2 studies) and fasting blood glucose level (1 study). The authors had shown only slight influence of the non-DPP-based programs on the body-weight reduction after 6–12 months, as well as on the HbA1c level (2 studies). Conversely, a study showed the ineffectiveness of non-DPP-based program with an observed increase of blood glucose levels 2.5 years after the intervention [8].
Programs Based on Single-Component Interventions
In the 2018 Shrestha meta-analysis, the influence of the dietary interventions conducted on employees at the workplace on the levels of HbA1c and fasting blood glucose was assessed. The dietary interventions were conducted in small group sessions (8 studies), individual coaching (9 studies) and through setting short-term and long-term heath goals. The results of the meta-analysis of 10 studies showed statistically significant influence of dietary intervention on lowering of the HbA1c (%)—mean change = −0.18% [95% CI: (−0.29; −0.06)]. Conversely, meta-analysis of 12 studies showed no statistically significant difference in fasting blood glucose levels in employees—mean change = −2.60 mg/dl [95% CI: (−5.27; 0,08)] [15].
Contrarywise, in the 2009 Conn meta-analysis the authors had assessed the efficacy of physical activity-related intervention on diabetes risk, fasting blood glucose levels and anthropometric measurement of the employees. Most of the included studies encompassing physical activity programs focused on the motivational/educational sessions (80% of the studies) and supervised exercises conducted at workplace (27% of the studies). The intervention efficacy was measured by size effect for comparing two groups. According to the meta-analysis results, the intervention had positive influence on reducing the diabetes risks, showing the size effect for two-group comparison ranged from 0.90 to 0.98 (two-group post-test = 0.98 [95% CI: (0.06; 1.90)]; two-group pre-post = 0.90 [95% CI: (0.27; 0.53)]; 6 groups), where the size effect had been influenced by small sample size. The mean size effect for diabetes risk had been −12.6 mg/dl for fasting blood glucose levels. Moreover, the intervention had also positively influenced reduction of anthropometric parameters (BMI, weight, abdominal girth, and body fat %), indicating the size effect for two-group post-test at 0.08 [95% CI: (0.02; 0.15); 44 groups] [9].
The detailed characteristics and results of the studies on the prophylactics programs aimed at preventing type 2 diabetes conducted at the workplace have been shown in Table 2.
Discussion
In the study, the analysis of the conducted at workplace interventions aimed at diabetes prevention was made. Most (4 out of 7) included in the review studies were based on the US Diabetes Prevention Program (DPP) or other, similar programs [8, 11•, 13•, 14]. A single study assessed conducting multicomponent wellness programs at workplace and its influence on the anthropometric parameters, as well as the blood glucose levels [12•]. The use of single-component interventions (i.e., dietary interventions [15], physical activity-related [9] had also been noted.
It should be noted that the type 2 diabetes risk is related to another significant health issue—the obesity [16,17,18,19]. Therefore the actions aimed at reducing body-weight may also influence diabetes risk reduction. To that effect the analysis presented in this paper had been not only of the parameters directly related to diabetes (i.e., fasting blood glucose levels or glycated hemoglobin), but of those indirectly related also (i.e., body-weight and BMI changes).
According to results of the found studies the interventions conducted at workplace can be an efficient diabetes risk reducing method. The best results were noted for interventions comprising several components, i.e., health education, diet changes or increase in physical activity [8, 11•, 12•, 13•]. The key parameters of the physical activity seem to be the intensity and longevity of the intervention (the longer and the more intensive, the better results of the analyzed parameters).
Among different types of programs, the most common are those based on DPP. Every study analyzing DPP-based programs achieved statistically significant results representing improvement of parameters such as physical activity levels, blood pressure, body-weight, BMI, HbA1c levels, and fasting blood glucose levels [8, 11•, 13•, 14]. In the 2017 Hafez study the authors had analyzed and compared non-DPP-based programs (encompassing lower than DPP intensity interventions aimed at supporting life-style changes through educational sessions, websites, and individual consultations) described in 3 studies [8]. In 2 out of 3 studies those interventions only slightly influenced body-mass reduction after 6–12 months and decrease in HbA1c levels [20, 21], while the remaining study showed an increase in blood glucose levels 2.5 years after the intervention [22].
When single component interventions were utilized separately, the effects were much smaller or inconclusive (i.e., some parameters showed improvement, while others did not change). One such example was a 2018 Shrestha study, where utilized dietary interventions in form of group or individual sessions (mean time of intervention—12 months) noted slight decrease in HbA1c levels, yet no statistical significant results were obtained for fasting blood glucose level [15].
In most of the studies found, the observation period was about 12 months. Such time is not long enough to make a clear statement about the effectiveness of the measures. It seems necessary to carry out further analyses showing the size effect after several years after the implementation of the interventions. Longevity is one of the key elements for assessing the effectiveness of interventions.
For the purpose of the discussion, current recommendations on diabetes prevention were reviewed. They referred to the types and ways of implementing interventions in people in diabetes risk groups, including overweight and obesity, low levels of physical activity, cases of diabetes in the family and the pre-diabetic state. According to recommendations, the aforementioned factors can occur both separately and simultaneously [23,24,25,26,27,28,29].
As part of preventive measures aimed at type 2 diabetes, it is recommended to implement broad educational activities focused on making the patient aware of the health risks associated with type 2 diabetes [23, 27, 29, 30]. It is also recommended to implement interventions aimed at lifestyle modification, including limiting the intake of products increasing the risk of type 2 diabetes (including fats, simple sugars, and sweetened beverages), while increasing products showing a preventive effect on the disease. Moreover, if it is deemed necessary, specific dietary patterns such as the DASH diet or the Mediterranean diet should be recommended [25, 27, 29, 31,32,33]. Increasing the level of physical activity among people at risk for type 2 diabetes should also be an important part of an intervention aimed at lifestyle modification. The main goal of encouraging the introduction of physical activity should be to reduce body weight and increase energy expenditure, especially in overweight or obese individuals [23, 25, 27,28,29, 32, 33]. Ultimately, it is recommended for people at risk for type 2 diabetes to engage in moderate-intensity physical activity tasks (e.g., volleyball, tennis, intermediate or long-distance running) at a minimum of 150 min per week [23, 25, 28, 32].
The recommendations also emphasize the need for implementation of screening aimed at type 2 diabetes. The included recommendations currently recommend the use of fasting blood glucose measurement, oral glucose tolerance test and blood glucose measurement as target screening tools. These technologies, according to the recommendations, can be used interchangeably, and the age for starting regular screening in the most recent documents is set at 35 years [23,24,25].
Some guidelines also emphasize the importance of conducting activities in the workplace [27, 29]. The National Institute for Health and Clinical Excellence recommendations emphasize that awareness-raising activities should be carried out in multiple locations. In addition to the workplace, these could include primary care facilities, pharmacies, dental offices, offices, stores, libraries, nursing homes, assisted living centers, or churches. The document also stresses that comprehensive programs should be conducted in the easily accessed workplace (at various times of the day) [27]). Conversely, another European recommendation indicates that behavioral interventions aimed at diabetes prevention may be conducted in health care facilities, the workplace, and the participant's home [29].
Review Limitations
The review included exclusively publications in English. The studies included in the systematic reviews found analysed a diverse population in terms of health status. Some studies analyzed pre-diabetic or diagnosed diabetic population, while others looked at the impact of the intervention on healthy adults. The studies also included different endpoints, intervention time and follow-up period. They used varied methods of data presentation. The aforementioned elements created a considerable heterogeneity among the studies, which in some cases made a meta-analysis impossible. As a result, it is also not possible to make simple comparisons of results between publications.
The review focused only on parameters that are directly or indirectly related to the incidence of diabetes. Sometimes the included publications analyzed a broader spectrum of measures and endpoints (e.g., relating to cholesterol levels). However, for the sake of data transparency and clarity, the authors deemed it impossible to describe them all in detail.
Conclusions
Based on available studies, it is possible to conclude that multicomponent programs that include elements such as educational activities, interventions directed at changing diet and increasing physical activity are effective in reducing the risk of type 2 diabetes. Multicomponent interventions are more effective than those undertaken separately. Therefore, multicomponent interventions based on best practices and global recommendations should be implemented in the workplace first and foremost, with appropriate intensity and duration (a minimum of several months). An example would be programs based on the National Diabetes Prevention Program implemented in the USA.
Activities undertaken as part of programs aimed at diabetes prevention simultaneously have a positive impact on a number of other diseases by, for example, reducing body weight or lowering the risk of cardiovascular disease. The benefits of introducing health-promoting measures are therefore undeniable, and should be considered both for people at risk for diabetes (to reduce their risk levels), as well as for healthy people, who will be able to improve their knowledge of diabetes and make health-promoting changes in their daily lives.
Due to the relatively short follow-up period of the studies found, further analyses and high-quality RCTs would need to be conducted to assess the durability of the effect over time, several years after its application.
Data Availability
Not applicable.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
International Diabetes Federation. IDF diabetes atlas. 2021. https://diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_Edition_2021.pdf. Accessed 16 Mar 2023.
World Health Organization. Diabetes. 2022. https://www.who.int/news-room/fact-sheets/detail/diabetes. Accessed 16 Mar 2023.
Centers for Disease Control and Prevention. Research behind the national DPP. 2022. https://www.cdc.gov/diabetes/prevention/research-behind-ndpp.htm. Accessed 16 Mar 2023. Publication describing the National Diabetes Prevention Program (DPP) from the USA. The results of the study showed that a structured lifestyle program resulted in a weight loss of 5 to 7% of the participants’ body weight and reduced the risk of developing type 2 diabetes in high-risk adults by 58%.
Centers for Disease Control and Prevention. What is the national DPP? 2022. https://www.cdc.gov/diabetes/prevention/what-is-dpp.htm. Accessed 16 Mar 2023.
Centers for Disease Control and Prevention. Employer testimonials. 2022. https://www.cdc.gov/diabetes/prevention/employer-testimonials.htm. Accessed 16 Mar 2023.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page M, Welch V. Cochrane handbook for systematic reviews of interventions; Version 6.2; The Cochrane Collaboration in London. London, UK; 2021.
Proper KI, van Oostrom SH. The effectiveness of workplace health promotion interventions on physical and mental health outcomes - a systematic review of reviews. Scand J Work Environ Health. 2019;45(6):546–59. https://doi.org/10.5271/sjweh.3833.
Hafez D, Fedewa A, Moran M, O’Brien M, Ackermann R, Kullgren JT. Workplace interventions to prevent type 2 diabetes mellitus: a narrative review. Curr Diab Rep. 2017;17(2):9.
Conn VS, Hafdahl AR, Cooper PS, Brown LM, Lusk SL. Meta-analysis of workplace physical activity interventions. Am J Prev Med. 2009;37(4):330–9. https://doi.org/10.1016/j.amepre.2009.06.008.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, Moher D, Tugwell P, Welch V, Kristjansson E, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include andomized or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008.
Fitzpatrick-Lewis D, Ali MU, Horvath S, Nagpal S, Ghanem S, Sherifali D. Effectiveness of workplace interventions to reduce the risk for type 2 diabetes: a systematic review and meta-analysis. Can J Diabetes. 2022;46(1):84–98. https://doi.org/10.1016/j.jcjd.2021.04.003. The publication at the top of the hierarchy of scientific evidence according to EBM (systematic review with RCT meta-analysis). As part of the publication, all relevant endpoints relating to intervention programs reducing the risk of type 2 diabetes in the workplace were included. The interventions in the review are based on the DPP program, which is widely recognized around the world as a program of good practice for the prevention of type 2 diabetes.
Peñalvo JL, Sagastume D, Mertens E, Uzhova I, Smith J, Wu JHY, Bishop E, Onopa J, Shi P, Micha R, Mozaffarian D. Effectiveness of workplace wellness programmes for dietary habits, overweight, and cardiometabolic health: a systematic review and meta-analysis. Lancet Public Health. 2021;6(9):e648–60. https://doi.org/10.1016/S2468-2667(21)00140-7. The publication at the top of the hierarchy of scientific evidence according to EBM (systematic review with RCT meta-analysis). As part of the publication, 121 studies were found, on the basis of which a numerical synthesis of results was carried out, depending on the components of programs aimed at wellbeing. According to the results, the effectiveness of such programs in the workplace was confirmed in reducing the risk factors for type 2 diabetes in this respect.
Inolopú J, Hilario-Huapaya N, Tantaleán-Del-Águila MA, Hurtado-Roca Y, Ugarte-Gil C. Interventions for the prevention of risk factors and incidence of type 2 diabetes in the work environment: a systematic review. Rev Saude Publica. 2019;53:101. https://doi.org/10.11606/s1518-8787.2019053001084. The review was based on common assumptions and recommendations indicated as effective in the fight against risk factors as part of the prevention of type 2 diabetes. Structured interventions based on the above-mentioned the assumptions of national organizations allow for a systemic approach to the problem related to this disease entity, and the publication indicates those programs that have proven effective in the prevention of type 2 diabetes in the workplace.
Brown SA, García AA, Zuñiga JA, Lewis KA. Effectiveness of workplace diabetes prevention programs: a systematic review of the evidence. Patient Educ Couns. 2018;101(6):1036–50. https://doi.org/10.1016/j.pec.2018.01.001.
Shrestha A, Karmacharya BM, Khudyakov P, Weber MB, Spiegelman D. Dietary interventions to prevent and manage diabetes in worksite settings: a meta-analysis. J Occup Health. 2018;60(1):31–45. https://doi.org/10.1539/joh.17-0121-RA.
Boles A, Kandimalla R, Hemachandra RP. Dynamics of diabetes and obesity: epidemiological perspective. Iochim Biophys Acta Mol Basis Dis. 2017;1863(5):1026–36.
Abuyassin B, Laher I. Obesity-linked diabetes in the Arab world: a review. East Mediterr Health J. 2015;21(6):420–39. https://doi.org/10.26719/2015.21.420.
Pulgaron ER, Delamater AM. Obesity and type 2 diabetes in children: epidemiology and treatment. Curr Diab Rep. 2014;14(8):508. https://doi.org/10.1007/s11892-014-0508-y.
Piché ME, Tchernof A, Després JP. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ Res. 2020;126(11):1477–500. https://doi.org/10.1161/CIRCRESAHA.120.316101.
Bevis CC, Nogle JM, Forges B, Chen PC, Sievers D, Lucas KR, et al. Diabetes wellness care: a successful employer-endorsed program for employees. J Occup Environ Med. 2014;56:1052–61.
Burton WN, Chen C-Y, Li X, Erickson D, McCluskey M, Schultz A. A worksite occupational health clinic-based diabetes mellitus management program. Popul Health Manag. 2015;18:429–36.
Viitasalo K, Hemiö K, Puttonen S, Hyvärinen H-K, Leiviskä J, Härmä M, et al. Prevention of diabetes and cardiovascular diseases in occupational health care: feasibility and effectiveness. Prim Care Diabetes. 2015;9:96–104.
ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 2. Classification and diagnosis of diabetes: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S19–40. https://doi.org/10.2337/dc23-S002.
US Preventive Services Task Force, Davidson KW, Barry MJ, Mangione CM, Cabana M, Caughey AB, Davis EM, Donahue KE, Doubeni CA, Krist AH, Kubik M, Li L, Ogedegbe G, Owens DK, Pbert L, Silverstein M, Stevermer J, Tseng CW, Wong JB. Screening for prediabetes and type 2 diabetes: US preventive services task force recommendation statement. JAMA. 2021;326(8):736–43. https://doi.org/10.1001/jama.2021.12531.
Alawadi F, Abusnana S, Afandi B. Emirates diabetes society consensus guidelines for the management of type 2 diabetes mellitus – 2020. Dubai Diabetes Endocrinol J. 2020;26:1–20.
The Royal Australian College of General Practitioners. Management of type 2 diabetes: a handbook for general practice. East Melbourne, Vic: RACGP; 2020.
National Institute for Health and Clinical Excellence (2017). Preventing type 2 diabetes: risk identification and interventions for individuals at high risk. https://www.nice.org.uk/search?q=ph38. Accessed 13 March 2023.
Cosentino F, Grant P, Aboyans V. The Task Force for diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD). Eur Heart J. 2019;41:255–323.
Paulweber B, Valensi P, Lindström J. A European evidence-based guideline for the prevention of type 2 diabetes. Horm Metab Res. 2010;42(Suppl 1):S3–36.
International Diabetes Federation (2012). Global guideline for type 2 diabetes. https://www.idf.org/e-library/guidelines/79-global-guideline-for-type-2-diabetes. Accessed 13 March 2023.
Dyson P, Twenefour D, Breen C. Diabetes UK evidence-based nutrition guidelines for the prevention and management of diabetes. Diabetic Med. 2019;28(11):1282–8.
Prebtani A, Bajaj H, Goldenberg R. Reducing the risk of developing diabetes. Diabetes Canada Clinical Practice Guidelines Expert Committee. Canad J Diabetes. 2018;42:S20–6.
Pronk NP, Remington PL. Community preventive services task force. Combined Diet and Physical Activity Promotion Programs for Prevention of Diabetes: Community Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163:465–8.
Author information
Authors and Affiliations
Contributions
Conceptualization: J.Ś. and K.W.; methodology: K.W., J.Ś., and T.T.; formal analysis: K.W. and J.Ś.; writing—original draft preparation: K.W., J.Ś., W.M., and S.J.; writing—review and editing K.W., J.Ś., A.A., and U.R.; supervision: T.T., A.A., and U.R. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
We certify that figure and tables in the article are original.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 35 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wnuk, K., Świtalski, J., Tatara, T. et al. Workplace Interventions for Type 2 Diabetes Mellitus Prevention—an Umbrella Review. Curr Diab Rep 23, 293–304 (2023). https://doi.org/10.1007/s11892-023-01521-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11892-023-01521-3