
Abstract
Electronic fetal monitoring is used to evaluate fetal well-being by assessing fetal heart activity. The signals produced by the fetal heart carry valuable information about fetal health, but due to non-stationarity and present interference, their processing, analysis and interpretation is considered to be very challenging. Therefore, medical technologies equipped with Artificial Intelligence algorithms are rapidly evolving into clinical practice and provide solutions in the key application areas: noise suppression, feature detection and fetal state classification. The use of artificial intelligence and machine learning in the field of electronic fetal monitoring has demonstrated the efficiency and superiority of such techniques compared to conventional algorithms, especially due to their ability to predict, learn and efficiently handle dynamic Big data. Combining multiple algorithms and optimizing them for given purpose enables timely and accurate diagnosis of fetal health state. This review summarizes the currently used algorithms based on artificial intelligence and machine learning in the field of electronic fetal monitoring, outlines its advantages and limitations, as well as future challenges which remain to be solved.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The electronic fetal monitoring (EFM) is used nowadays particularly for monitoring the heart activity of fetus and assessing its well-being. The main objective of monitoring is an early detection of life-threatening fetal hypoxia. If the fetal hypoxia is not detected and rectified on time, the oxygen saturation of blood becomes extremely low and the fetal hypoxia progresses to asphyxia. The consequence of a serious asphyxia is a hypoxic-ischemic damage of organs which may, inter alia, lead to a brain and heart damage and a nervous system failure [1, 2]. An accurate and reliable fetal monitoring during pregnancy and birth may lead to an early detection of states which may adversely affect the health of fetus or cause perinatal death.
The fetal heart monitoring has its origins in the first half of the 19th century when fetal heart sounds (fHSs) were detected thanks to the invention of stethoscope. The assessment of fetal well-being was based on intermittent auscultation of fHSs and subsequent determination of fetal heart rate (fHR) [3]. The EFM became the basis of prenatal care and a common part of clinical practice as late as in the 1960s when the first cardiotocograph (CTG), which was supposed to help doctors in detecting fetal hypoxia, was introduced thanks to the development in science and technology [4]. Nevertheless, some studies in the past [5,6,7] argued that the number of executed caesarian sections had increased after introducing the CTG equipment to delivery rooms but at the same time there had been no decrease in perinatal mortality caused by the influence of hypoxia. This was attributed to a difficult interpretation of CTG data influenced by subjective assessment and experience of doctors which led to a high false positivity when determining the hypoxia leading to a high number of unnecessarily executed caesarian sections [4, 5]. This tendency from the past persists and the numbers of caesarian sections are still high. The numbers of caesarian sections should move within 10–15% [8] according to the World Health Organization statement on caesarean section rates, however the world average ranges around 21.1% according to the data from 2015. In some countries (Dominican Republic, Egypt or Brazil for instance), the numbers of caesarian sections are exceeding 55% [9], which is alarming. Since the caesarian section is an invasive procedure after which the incidence of complications is more frequent than after a spontaneous delivery [10], the current research is focused on the development of both the classical CTG [11,12,13], and alternative techniques for non-invasive EFM such as fetal electrocardiography (fECG) [14, 15], fetal phonocardiography (fPCG) [16] or fetal magnetocardiography (fMCG) [17].
Such alternative techniques bring very important clinical information about the fetal health and have a great potential to become complement to the conventional CTG or substitute the CTG entirely thanks to its non-invasiveness and absence of ultrasound radiation. Nevertheless, the processing, analysis and interpretation of these biological signals is a challenging task, because it is rather difficult and computationally demanding to model a function of human body with classical mathematics [18]. This is mainly due to the nonlinear and non-stationary nature of these biological signals and the presence of many types of interference. In addition, useful signal and interference often overlap in the time and frequency domains, causing conventional algorithms to fail to process these signals [18]. According to the latest research [19,20,21,22] the algorithms based on artificial intelligence (AI) have appeared to be very promising for the processing and analysis of these real-world signals, especially due to their ability to predict and learn.

Principle of literature search strategy for finding relevant literature
1.1 Structure of the Review
This review focuses on the use of AI in the field of non-invasive electronic monitoring of fetal heart activity, provides the summary of advantages and limitations of presented methods, and also the list of future challenges. The structure of the contribution includes Sect. 2 which provides a general overview of both the non-invasive techniques for EFM and AI-based approaches used in these fields. Section 3 describes three main application areas of AI in EFM (noise suppression, feature detection and fetal state classification). Section 4 summarizes the efficiency of presented algorithms, highlights the most important findings and outlines directions for further research. In Sect. 5, the remaining challenges associated with the fetal monitoring and AI are discussed. The conclusion of the contribution is in Sect. 6.
1.2 Literature Search Strategy
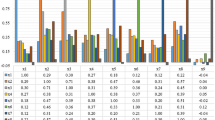
To find relevant literature for this review, Google Scholar, PubMed, and the Scopus search engines were used. The search used phrases combining terms from the field of artificial intelligence: “Artificial intelligence”, “Machine learning”, “Artificial neural networks”, “Fuzzy logic”, “Nature-inspired optimization” combined with fetal monitoring techniques: “Cardiotocography”, “Fetal electrocardiography”, “Fetal phonocardiography”, “Fetal magnetocardiography”. A total of 20 queries were used for the search, see Fig. 1. All results found were inspected and evaluated. Only studies that were published after 2000 were selected. A large part of the conference papers was excluded.
2 Background
In the field of EFM, as in other areas, there is a rapid development with the advancement of science and technology. The goal of scientists and obstetricians is to develop a highly reliable system, using the most modern approaches and technologies, through which it would be possible to detect fetal hypoxia with a high accuracy and decrease the number of unnecessarily executed caesarian sections. AI technologies, which excels in solving complex tasks and processing of great number of data, appear to be promising for the processing and interpretation of fetal signals [23]. This section gives an overview of basic techniques for EFM and AI-based approaches used in these fields.
2.1 Electronic Fetal Monitoring
The term EFM was used in the past exclusively as a synonym for the CTG technique. It turned out to be misleading and since 2015, based on the consensus of The International Federation of Gynecology and Obstetrics, only the term CTG has been reserved for this monitoring technique. The term EFM will be used in this article only as a general term [4] comprising more methods of fetal monitoring, for example:

Illustration of different monitoring methods, their signals and placement of sensing electrodes and sensors. In CTG monitoring, uterine contractions are measured using a toco sensor (TS) and the fHR trace is obtained using an ultrasound transducer (UT). In the case of fECG measurements, aECG signals are obtained using AE\(_1\) and AE\(_2\) electrodes. AE\(_0\) refers to the reference electrode and N refers to the active ground. The placement of the sensing electrodes was inspired by Matonia et al. [38] and examples of aECG signals from the Fetal electrocardiograms, direct and abdominal with reference heartbeat annotations dataset were used. The fMCG signals are measured using a magnetometer system (MS). In examples of fECG and fMCG signals, the maternal and fetal components are labeled with m and f, respectively. The fPCG signal is measured by phonocardiographic sensor (PS). The diagram shows ideal fPCG signal (upper trace) and fPCG signal with ambient interference (lower trace) with S\(_1\) and S\(_2\) sounds labeled
-
1.
Cardiotocography CTG is based on the simultaneous measuring of uterine contractions and fHR (see Fig. 2). The trace of fHR is obtained by scanning the movements of fetal heart recorded with Doppler-based ultrasound transducer [4]. Subsequently, the recorded signal passes through the modulation and the autocorrelation to ensure its sufficient quality. This process leads to the approximation of the true fHR intervals. Uterine contractions are scanned by a pressure sensor. Nevertheless, the quality of records strongly depends on the sensor placement and belt tightening [1]. However, this method is associated with a number of disadvantages which include, in particular, an important influence of the examining doctor’s experience upon the interpretation of CTG records (commonly leading to an inaccurate detection of fetal hypoxia), an influence of sensor placement on the quality of signals, a sensitivity to the movements of fetus as well as the mother and a lower sensitivity of women with higher values of body mass index (BMI) [24].
-
2.
Fetal Electrocardiography The non-invasive fECG (NI-fECG), based on recording electrical signals from the mother’s abdominal area, appears to be the most promising technique of fetal monitoring. At present, the invasive variant (the so-called direct fECG), measuring fECG signal by means of scalp electrode directly from the fetal head. This makes it highly accurate, but many critics disparage its contributions due to the negatives related to its invasiveness (for example the mother’s discomfort or the risk of infection). Apart from the fHR, the fECG signal provides also additional information about pathological states connected in particular with fetal hypoxia or metabolic acidosis [4, 25]. They manifest as changes in the morphology of fECG traces, such as changes of T:QRS ratio or QT interval [26, 27]. It has been demonstrated that during the simultaneous recording of fHR and T:QRS ratio (known as ST analysis or STAN) there has been both an early detection of acidosis and a decrease in the number of unnecessary caesarian sections [25, 28], thus eliminating the main aspects for which the CTG has been criticized [5, 29]. Due to these reasons, NI-fECG has a huge potential to become a complementary method to the CTG or to replace it completely in clinical practice. Moreover, in case of NI-fECG, neither the mother nor the fetus are exposed to ultrasound radiation which allows a continual recording, even within the framework of home monitoring. An advantage is its use for women who have higher values of BMI. The main obstacle of NI-fECG recording is the presence of other disturbing signals, in particular the maternal electrocardiographic signal (mECG), which must be eliminated in order to obtain clinical information from NI-fECG [4, 25]. In Fig. 2 there is a schematic example of the electrode placement and recorded abdominal signals (aECG) containing a mixture of mECG and fECG.
-
3.
Fetal Phonocardiography The method of fPCG is low-cost and a completely passive technique based on the monitoring of fHSs, cardiac acoustic vibrations and murmurs by means of microphone-transducer [30, 31]. The attention has been recently paid to understanding the nature and the origin of this signal, especially because the fPCG signal recorded in high quality may provide more information about cardiac pathologies than commonly used CTG [32]. According to the research focused on the development of fPCG [33], this technique might become a complement of the classical CTG. The fPCG could find its use especially in a long-term monitoring and home monitoring which might lead to a reduction in the number of physical visits to the doctor [34]. In contrary to CTG, additional information about the fetal health state could be obtained through a complex analysis of heart murmurs. Unfortunately, the main disadvantage of fPCG is a high sensitivity to the disturbing signals and necessity of proper placement of the recording sensor [32, 33]. When fPCG signals from maternal abdominal area are recorded, the useful signal is contaminated especially with ambient noise (e.g. speech, cough, radio, air conditioning, door closings or alarms). Moreover, maternal as well as fetal movement artifacts, such as breathing artifacts, uterine contractions, bowel sounds and maternal heart sounds (mHSs) are also considered to be disturbing [32]. In Fig. 2 there is a schematic example of the recording sensor placement, ideal fPCG signal and fPCG signal disturbed by ambient noise.
-
4.
Fetal Magnetocardiography The fMCG is an alternative method based on recording magnetic fields created by conduction currents in the fetal heart. The fMCG signal shows the same information as the fECG (i.e. the electrical activity of the fetal heart in the form of the PQRST complex) [35]. Figure 2 shows a schematic diagram of magnetometer system and the recorded fMCG signals. The magnetic field produced by the fetal heart is sensed by magnetometer system from outside the maternal abdomen above the fetal heart [36]. The fMCG signals have much higher value of signal-to-noise ratio (SNR) than the NI-fECG signals since the propagation of magnetic fields is not that affected by surrounding tissue as in the case of NI-fECG [35]. Moreover, the NI-fECG is almost impossible to be recorded between the 28th and 32nd weeks of pregnancy due to the fetal coverage with the layer of vernix caseosa, which isolates the fetal electrical cardiac activity [25]. However, this very promising method is not often used in clinical practice due to high financial costs and the complexity of the measuring device. The superconducting quantum interference device technology is used for recording which requires cooling by liquid helium and measuring must be conducted in a large and magnetically shielded room [17, 37]. Moreover, the fMCG must be measured by an experienced doctor and a skilled technical support must be available [4]. Nevertheless, the current research focuses on the development of new magneto-metric technologies, such as optically pumped magnetometers [17], which are less costly and their use is more practical and simple. This progress in the development might allow the fMCG to become a part of common clinical practice and the priceless information about the fetal health could be obtained from it [17].
All four of the above-mentioned EFM techniques are of great benefit to clinical practice. However, in order to obtain all important information regarding fetal and maternal health state, further research and development is needed, especially in the field of signal-processing algorithms. There is a great need to design and implement reliable and intelligent methods that can improve the processing, analysis and interpretation of fetal and maternal heart
2.2 Artificial Intelligence Methods
The function of most real systems, including human body, is represented by non-linear dynamic behaviour with a certain degree of variability and uncertainty. The processing of such data is difficult and computationally demanding for conventional algorithms [18]. AI-based algorithms are able to deal with this inaccuracy and uncertainty. In addition to that, these algorithms can use these properties to create an adaptive low-cost solution [18, 39]. AI-based algorithms generally imitate human intelligence to solve complex tasks and, at the same time, improve iteratively on the basis of obtained information [23]. There are many partial sub-areas of AI using scientific findings, in particular from the fields of mathematics, statistics or biology. With respect to EFM, it is possible to encounter algorithms based on machine learning (ML), artificial neural networks (ANNs), fuzzy logic or nature-inspired optimization techniques. This section and Fig. 3 provide a basic overview of these sub-areas.

An overview of AI-based approaches used in EFM
-
1.
Machine Learning ML-based algorithms are able to learn and automatically increase their efficiency through experience based on data they work with [40]. According to learning methods, ML algorithms can be divided into four categories: supervised learning, unsupervised learning, semi-supervised learning and reinforcement learning. In case of supervised learning, a mathematical model of a data set, containing both inputs and outputs (a class for classification or a value for regression) assigned by human experts, is created [40, 41]. According to [39, 42], we can include, for example, decision trees (random forest [12] or C4.5 algorithm [43]), support vector machines (SVM) [11, 44], regressive analysis [45], k-nearest neighbor (k-NN) [11] or naive Bayes [46] into this category. As for unsupervised learning, an algorithm has only input (unlabeled) data and the output is unknown to the ML technique. The algorithm learns to recognize complex processes and formulas and usually creates a proper and simpler representation of input data which it subsequently clusters into groups without the possibility to assess the correctness of clustering [40]. According to [39, 42], some of the most well-regarded algorithms in this category are k-means [47, 48], k-medoids [47, 49], hierarchical clustering [47] or fuzzy c-means [47]. The semi-supervised learning combines both approaches described above in such a way that a part of the input data also contains the required output, but the other part of the data (usually larger) does not contain the required output [40]. Reinforcement learning is based on rewarding the required behaviour and, vice-versa, punishing the non-required behaviour [41]. Thus, the learning functions on the basis of the trial and error principle because there are no training data available. Nevertheless, neither the semi-supervised learning nor the reinforcement learning are very widespread in the field of EFM.
-
2.
Artificial Neural Networks ANNs-based algorithms are computing models inspired by biological structures behaviour. Such techniques mimic the learning and adapting mechanisms of biological neurons in brains [39, 50]. The basic network unit is the neuron which may have a random number of inputs but only one output. Neurons forming ANNs are mutually connected and transmit signals which are transformed by means of transfer functions. According to the topology (structure) of network, ANNs may be divided into feed-forward networks and recurrent neural networks (RNNs) [50]. The simplest model of feed-forward network for binary classification composed of a single neuron is called a perceptron or a more powerful adaptive linear neuron (ADALINE) [51, 52]. Due to the limited use of perceptron, this model was expanded to a multilayer perceptron (MLP), which represents a special type of multilayer network where each layer is fully connected (each layer neuron is connected with all neurons in the preceding layer) [52]. Multilayer networks are usually organized in several layers composed of an input layer, intermediate hidden layers and an output layer [50]. ANNs with a large number of layers (tens of layers) are called deep ANNs and form a basis for deep learning to solve very complex linear and non-linear problems. In order to estimate the parameters (training) of ANNs, the back propagation (BP) algorithm is of the most popular techniques [39]. This group of networks may include, for example, convolutional neural networks (CNNs) [12, 19, 53], probabilistic ANNs [54], polynomial ANNs [55, 56], deep belief ANNs [57]. Adaptive neuro-fuzzy inference system (ANFIS) [58,59,60] is also used very often in this field. As far as RNNs are concerned, there is also a reverse transmission of information from higher layers back to lower layers in addition to signal propagation from the input layer in the direction of the output layer, which is in contradiction with multilayer ANNs [50]. Within the framework of EFM, it is possible to encounter especially an echo state network (ESN) [61, 62] or a long short-term memory (LSTM) [22].
-
3.
Fuzzy Logic Fuzzy logic is a powerful tool for solving tasks where a solution cannot be found through classical statement logic using only two logic values 1 a 0. Fuzzy logic allows to work with all values in the interval \(\langle \)0;1\(\rangle \), and the number of values is infinite [63]. It allows to catch an approximate reasoning better which is characteristic of human reasoning and environment full of uncertainties and inaccuracies [64]. The fuzzy model is usually created on the basis of fuzzy rules implemented as a series of if-then rules. Since the fuzzy concept is based on the qualitative rather than the quantitative expression, it is easier to connect mathematics with real-world applications [63, 64]. In the field of EFM, we may also encounter, for example, a fuzzy unordered rule induction algorithm (FURIA) [65] in addition to the classical fuzzy logic [66,67,68].
-
4.
Nature-Inspired Optimization Techniques Nature-inspired algorithms are often inspired by the evolution, biological systems or chemical or physical processes. Such approaches have been demonstrated to be very flexible and effective for solving highly non-linear problems and their use is appropriate especially for challenging optimization tasks [69, 70]. In order to find an optimal solution effectively (or a solution close to being optimal), they use iterative processes and intelligent learning strategies for the exploration and exploitation of the search space [42]. Within the framework of EFM we may encounter, in particular, evolutionary algorithms which are inspired by biological evolution, such as genetic algorithms (GA) [71, 72], differential evolution (DE) [73, 74], or evolution strategy (ES) [75]. The second large group of algorithms are swarm-based algorithms inspired by the behaviour of biological swarms, such as particle swarm optimization (PSO) [76, 77], firefly algorithm (FA) [78] or moth-flame optimization algorithm (MFO) [79].
3 Application Areas of Artificial Intelligence
In the field of EFM, we may come across three main areas in which AI-based algorithms are used. The first area is the suppression of noise especially in fECG signals (the elimination of mECG) [19, 22, 57, 61, 80], but also in the processing of fPCG [60]. The second area is represented by the feature detection which includes the detection of fetal QRS (fQRS) complexes [47, 49, 53, 81,82,83,84,85] and the estimate of fHR without the necessity to detect R peaks [20] in fECG signals. Similarly, in fPCG signals, AI-based algorithms were used to detect fHSs [45, 48]. The last area is the classification of fetal health using signals recorded by means of CTG [11, 43, 86,87,88,89], but also by means of alternative techniques of fPCG [66, 90, 91] or fMCG [44]. Figure 4 illustrates the areas where the AI was used in the past marked by the red frame.

A schematic illustration of individual steps for obtaining, processing and classifying the fetal health by means of CTG, fECG, fPCG, and fMCG signals. Red frames indicate three areas where the AI was already used in the past
3.1 Noise Suppression
It is essential to have a quality signal for a precise signal analysis and obtaining correct clinical information. In case of CTG or fMCG, signal filtration is not such a difficult task as in the case of fECG or fPCG. The extraction of fECG is a challenging task due to a relatively low SNR of the useful signal (fetal component) which is overlapped by mECG and other noise both in temporal and frequency domains [4, 25]. Therefore, the past research in the field of fECG extraction focused on testing especially advanced signal processing methods such as blind source separation methods [92, 93], wavelet transform (WT) [14], empirical mode decomposition (EMD) based algorithms [94, 95] or adaptive filters [15, 96]. Hybrid methods combining adaptive and non-adaptive algorithms turned out to be the most promising [97]. However, in low quality recordings, even these algorithms failed to provide satisfactory results.
A number of authors (e.g. in [21, 98]) have recently shown that non-linear fECG domain could be modelled more accurately by means of AI approaches. In case of fPCG signal extraction, an effective suppression of most types of interference was achieved by means of the modified finite impulse response filter [99] or WT [100]. A more difficult task arises in suppressing mHSs where there is a room for using AI-based algorithms as in case of fECG.
The AI-based methods for fetal component extraction (both in fPCG and fECG) work on the same principle as adaptive algorithms. The principle will be illustrated on the fECG extraction example, see Fig. 5. These methods use the following inputs: (1) composed aECG signal, i.e. mixture of maternal and fetal components (mECG\(_\text{A}\), fECG) and noise, and (2) reference thoracic mECG\(_\text{T}\). The thoracic mECG\(_\text{T}\) is adapted by AI-based algorithm into the form of mECG\(_\text{A}\) included in the aECG input. The distortion of mECG\(_\text{A}\) is caused by measuring this signal far from the source (the heart of mother) and non-linear transformation of the signal passing through different layers and tissues in the abdominal area [55]. The mECG\(_\text{T}\) signal adapted by the algorithm into the form of mECG\(_\text{A}\) is finally subtracted from aECG to obtain the fECG.

A general schema of fECG extraction by means of AI-based algorithms. The thoracic electrode records the reference mECG\(_\text{T}\) signal and the electrodes on the mother’s abdomen record aECG which is a mixture of mECG\(_\text{A}\), fECG and noise. The mECG\(_\text{T}\) and aECG signal enters the AI-based algorithm and it adjusts the mECG\(_\text{T}\) signal into the form of mECG\(_\text{A}\) signal contained in aECG. The adjusted mECG\(_\text{T}\) is finally deducted from the aECG and the final fECG is obtained
3.1.1 Artificial Neural Networks in Noise Suppression
Different types of ANNs are appropriate for fECG extraction especially due to their adaptability to the non-linear and time-varying features of fECG signal [101]. Thanks to their ability to learn and predict, ANNs are able to separate useful signal (i.e. fECG) and noise (i.e. mECG), which overlap in time and frequency domain and reach higher accuracy in fECG extraction in comparison with classical adaptive algorithms, such as the least mean squares (LMS) [102], the normalized LMS (NLMS) [103] or the recursive least squares (RLS) [104]. Moreover, a lower number of calculations is necessary as demonstrated in [21].
-
Polynomial Neural Networks Polynomial ANNs are multilayer networks using polynomial exponentiation activation function [105]. Although, according to Ayat et al. [56], this method managed to extract the fECG and outperform the algorithm of singular value decomposition (SVD). In some cases, however, it did not provide a satisfactory results. If the thoracic mECG\(_\text{T}\) and aECG signals were recorded from different locations, the morphology of mECG\(_\text{T}\) and mECG\(_\text{A}\) was different and the final fECG signal was contaminated with significant maternal residue. During experiments conducted by Assaleh et al. [55], the polynomial ANN managed to sufficiently suppress the maternal component, even in the cases when fetal and maternal beats overlapped. On the other hand, there was a noise present in the extracted fECG signal due to muscular activity, therefore, the use of additional post-processing techniques was recommended for its elimination. It was also interesting to discover that polynomial expansions of higher order than three did not lead to further quality improvement of the extracted signal according to a visual assessment. Ahmadi et al. [106] dealt with the pre-processing and post-processing of signal by means of WT before or after the application of polynomial ANN. Three scenarios were tested: a) the WT method filtered aECG signal before the application of polynomial ANN, b) WT was applied to an extracted fECG signal obtained by the application of polynomial ANN and c) WT was used for pre-processing of aECG and subsequently also for post-processing of the extracted fECG. Although SNR improved in all three scenarios in contrast to the use of basic polynomial ANN, the biggest improvement was achieved in the case of b) variant, i.e. in the application of WT as post-processing.
-
Convolutional Neural Networks CNNs belong to deep, feed-forward, multi-layer networks composed of an input layer, multiple hidden layers and an output layer. Hidden layers contain a convolutional layer, activation layer, pooling layer, fully-connected layer and normalization layers [107]. In convolutional layer, the operation of convolution is applied and multiple feature maps are obtained, which leads to the reduction of memory bulk used by CNNs. The activation layer maps the output of convolutional layer through the activation function to form the feature mapping relationship. The normalization layer serves for standardizing the input data of each layer during the training. Pooling layers appear periodically between convolutional layers going one after another to reduce the amount of data, the complexity of network, to speed up the calculation and to prevent overfitting. Thus, more information intensive features for final classification finally enter into the fully-connected layer (this is a classical MLP). After the fully-connected layer, there is a dropout layer preventing the overfitting in such a way that during the training process, there are several neural units which are with a certain probability temporarily dropped from the network. At the end, the classification network using the function of softmax is used to separate outputs [108]. The CNN-based approach introduced by Fotiadou et al. [19] was used to remove residual noise in extracted fECG signals in which the maternal component was already suppressed. The technique used the convolutional encoder-decoder network with symmetric skip-layer connections. The encoder as well as decoder contained eight convolutional layers, but the convolutional layers of the decoder were symmetrically transposed. Skip connections were placed between every two convolutional as well as transposed convolutional layers. When testing the algorithm on simulated signals, its efficiency was evaluated according to the SNR improvement (SNR\(_{\text{imp}}\)) parameter. The final fECG signals were improved (SNR\(_{\text{imp}}\) = 9.5 dB) and the benefit was the keeping of beat-to-beat morphological variations. Moreover, there was no need of any prior information on the power spectra of the noise. To increase the accuracy of fECG extraction, Almadani et al. [109] proposed a combination of two parallel fully CNNs (U-Nets [110]) with transformer encoding. In addition to efficient fECG extraction, the system was able to operate in real time and, according to the authors, could be implemented in a portable device. The CNN turned out to be powerful in combination with Bayesian filter as showed by Jagannath et al. [98] in 2019. The Bayesian filter managed to provide accurate mECG\(_\text{A}\) estimate in the aECG signal and the deep CNN estimated a non-linear relationship between the mECG\(_\text{A}\) and the thoracic mECG\(_\text{T}\), which was non-linearly transformed. A nine-layer network was used with three convolutional layers, three max-pooling layers for the compression of signal features and reduction of complexity and three fully-connected layers. The last layer contained one neuron representing the final fECG signal. The linear activation function was used for all layers, excluding the last one, and the softmax function was used in case of the last fully-connected layer. In terms of efficiency, this combined algorithm surpassed the classical adaptive LMS algorithm. The disadvantage of the algorithm is the high computational time during the training process, and therefore it was not suitable for training large datasets. In 2020, the same authors [57] compared their previously designed combination of CNN with the Bayesian filter to two other networks (the deep belief ANN and the conventional ANN using BP algorithm) which were also combined with the Bayesian filter. The input layer of conventional ANN contained 72 neurons, the hidden layer contained 2 layers with 84 neurons in each of them and 1 output neuron. In the input layer of the deep belief ANN, there were 98 neurons, 2 hidden layers were composed of the total number of 84 neurons and 1 neuron was used in the output layer. All three methods extracted a high-quality fECG, but it was the CNN (SNR\(_{\text{imp}}\) = 39.73 dB) that achieved the best results in terms of the SNR improvement. The limitation of all three algorithms was their high time complexity, which would not allow their implementation in real-time operating devices.
-
Multilayer Perceptron It is a feed-forward multi-layer network with one or more hidden layers. The main feature of the network is that every neuron in a specific layer is connected with all neurons in the preceding layer [52, 54]. In order to select the number of neurons in the hidden layer, two rules are generally used: a) their number should not be higher than the double of neurons in the input layer and b) their number should move between the number of neurons in the input layer and the output layer [54]. Golzan et al. [80] suggested a MLP where the connections between the input and hidden neurons were weighted by an adjustable weight parameter. The authors compared the efficiency of two different training methods: maximum likelihood (it presumes that weights have a fixed unknown value) and Bayesian learning (it considers the uncertainties of weight vector and assigns them probability distribution). The algorithms were tested on real recordings and their efficiency was evaluated according to the accuracy (ACC), sensitivity (SE), and positive predictive value (PPV) parameters. The algorithm based on Bayesian learning turned out to be superior with ACC = 94.86%, SE = 96.49% and PPV = 93.79% which may be attributed to its more effective use of training data.
-
Long Short Term Memory LSTM networks are a specific type of RNN able to remember information for a long period of time and learn a long-term dependency. The chain structure with recurring modules of ANNs, each containing four layers, is typical for the LSTM. The classic LSTM unit contains an input and an output gate, a forget gate and a cell. The cell remembers values in time intervals and gates decide which information will be removed and which will be retained [111]. The two-stage architecture combining slow and fast LSTM was employed by Zhou et al. [22]. The principle of the method was the implementation of slow LSTM for filtering mECG and the fast LSTM in order to highlight fECG, eliminate the remaining noise and improve the computing efficiency. Compared to the classic LSTM, the improved method reduced the total number of calculations by 50% without degrading the efficiency of the algorithm (vice versa the SNR was slightly improved: SNR\(_{\text{imp}}\) = 4.9 dB). Moreover, the high adaptability method was demonstrated on different types of signals with different levels of noise. However, the algorithm has been tested only on synthetic signals and thus the verification of its efficiency using the real signals is needed. The LSTM combined with the autoencoder (AE) model was tested on real data by Ghonchi et al. [112]. AE is a multilayer symmetric network containing an encoder and decoder that was able to improve the feature representation of the input data. Extensive testing was performed on two datasets and in both cases an average F1 > 92% was achieved. The advantage of the approach was the preservation of prior and posterior information of the input signal. However, the performance of the algorithm decreased significantly for signals with low SNR.
-
Echo State Networks ESN algorithm is a type of RNN where the reservoirs (weights between the input and the hidden layers) are generated accidentally, only the weights of output layer are trained and updated [4, 61]. The hidden layer is very sparsely connected (typically 1% connectivity) [113]. In contrast to adaptive algorithms, the benefit of ESN is that they can work with a certain degree of uncertainty. The limitation was the strong dependence on the optimal setting of hyper-parameters for the ESN algorithm to be effective. The challenge in implementation of this method is the optimization of a relatively large number of parameters, especially: the size of units of the reservoir weight matrix, the spectral radius of the reservoir connection matrix, the input scaling of the input weight matrix, and the leakage rate [4, 62]. Behar et al. [62] used a grid search for the optimization of ESN method parameters. Although this type of optimization led to an effective suppression of mECG and a quality extracted fECG, it was not an effective procedure in terms of time. Therefore, the same authors, Behar et al. in [61], suggested a random search for optimizing the ESN whose efficiency was compared with the grid search. The efficiency of ESN in using the random search was slightly lower (F1 = 85.6%) than in optimizing the ESN by means of the grid search (F1 = 87.9%). However, only 512 repetitions were used for the random search, whereas the grid search was repeated 798 times. The final optimal parameters were different for both methods. The optimal value for the size of units of the reservoir weight matrix was 90 according to the grid search and 135 for random search. The spectral radius of the reservoir connection matrix was set to 0.4 according to the grid search and 0.821 according to the random search. The input scaling of the input weight matrix was set to the value of 1 for grid search, whereas the optimal value was found to be 0.622 for the random search. No conformity was found for the leakage rate, which was set to the value of 0.4 for the grid search and 0.974 for the random search.
-
Adaptive Linear Neural Network ADALINE is a one-layer network with multiple neurons. The principle of the network consists in minimizing the mean squared error of the predictions of a linear function. Therefore, the objective is to find weight values in such a way that the lowest error is obtained (a difference between the required signal and the output signal) [114]. ADALINE has the same characteristics as the perceptron, e.g. it is a single-layer neural model, has linear decision boundary, is used for binary classification. However, it is considered as its improved version. This is because ADALINE uses a continuous response to update the scales, unlike the perceptron, which uses a binary response to update the scales. The continuous response allows the scale updates to reflect the actual error and the thus make resulting extraction more efficient [52, 114]. The efficiency of the algorithm depends on the following parameters: the dimensionality of the input space, the learning rate, the momentum and initial weights which are adjusted as long as the difference between the thoracic mECG\(_\text{T}\) signal and the mECG\(_\text{A}\) in the aECG signal is not minimized (in case of the fECG extraction). Based on the research by Amin et al. [115] and Reaz et al. [116], the algorithm worked efficiently, if the high learning rate with the value of 0.8, the low momentum with the value of 0.5, and very small non-zero initial weights were used. Nevertheless, according to the results of Kahankova et al. [51], the lower learning rate with the value of 0.07 performed better. The optimal value of the input space dimensionality lay in the interval 20–30.
-
Adaptive Neuro-Fuzzy Inference System One of the most tested AI approaches for noise suppression and extraction of usable fECG signal is the ANFIS method. It combines the ANN and the Takagi-Sugeno fuzzy inference system. It is therefore a very effective method that utilizes the advantages of fuzzy expert systems (it works with inaccurate data) and the ANN (learning from the environment) [4]. Apart from the classic Takagi-Sugeno type-1 structure, the implementation of Takagi-Sugeno type-2 structure proved to be suitable according to Ahmadieh et al. [117] which surpassed the type-1 structure. The superiority of the type-2 to the type-1 is given mainly by its ability to capture the non-linearity of the model. The basic structure of ANFIS consists of five layers: the first is an adaptive input layer with two inputs (aECG and mECG\(_\text{T}\)), which performs fuzzification of the input language variables, the second is a non-adaptive rule layer for multiplying output signals from the first layer in order to determine the weight of the rules, the third is a non-adaptive normalising layer for determining the proportion of each rule’s weight to the sum of weights of all rules, the fourth is an adaptive defuzzification layer, and the last is a summary layer represented by a single non-adaptive node for determining the output (fECG) [58]. According to Assaleh [58], the proper setting of the algorithm parameters had a substantial impact on the resulting quality of fECG extraction. Based on this research, the author recommended using four membership rules (this corresponded to 16 fuzzy rules, 53 nodes, 48 linear and 24 non-linear parameters). However, the setting was chosen based on the trial and error principle, and the efficiency of the algorithm in real recordings was performed by visual assessment of the extracted fECG signals. The authors of Emuoyibofarhe et al. [118] made an important remark concerning the use of the ANFIS method—the morphology of the resulting extracted fECG signal with respect to the original fetal component in the aECG signal remains unchanged. However, the extracted fECG signal obtained visible residues of the maternal component. Combination of the ANFIS method and other techniques was recommended for enhancing the filtration. For these reasons, many authors including Saranya et al. [59], Nasiri et al. [77], or Elmansouri et al. [119], tuned the ANFIS structure using PSO, which led to extraction of high-quality fECG. A combination of DE, ANFIS and extended Kalman smoother (EKS) designed by Panigrahy et al. [74] was also used to enhance the efficiency of ANFIS. The combined approach allowed fECG extraction with ACC = 90.66%, without requiring any user interaction for initialization of the parameters. However, when implementing the algorithm, one must consider high computational cost of PSO. Another method that can be used to enhance the quality of ANFIS extraction, especially in the post-processing phase, is the WT method. This combination was proposed for instance by Swarnalath et al. [120], Jothi et al. [121], and Hemajothi et al. [122]. An interesting comparison was published in Swarnalath et al. [120], who tested three different scenarios which include a) ANFIS only, b) WT for signal pre-processing and ANFIS, and c) ANFIS and WT for post-processing. The results showed that the variant c), combination of ANFIS and WT for post-processing, was able to extract higher-quality fECG than the other two variants. Jothi et al. [121] used the undecimated WT combined with ANFIS instead of the classic discrete WT. Combining the undecimated WT and ANFIS turned out to be superior to the combination of discrete WT and ANFIS. Current research also incorporates ANFIS and WT into systems for remote monitoring. Kumar et al. [123] used orthogonal frequency division multiplexing for the transmission of mECG\(_\text{T}\) and aECG signals, followed by using the combination of ANFIS and WT for the extraction of fECG in the received signals. Thus, in the fECG extraction, the WT algorithm was very effective as a post-processing method that could enhance fetal R-peaks. However, according to the findings in [4], its application was more suitable for the determination of fHR than for morphological analysis. The application of the WT altered the morphology of fQRS complexes and the subsequent morphological analysis was less accurate. Most of the studies mentioned above used aECG and mECG\(_\text{T}\) signals acquired from the mother’s chest as inputs of the ANFIS algorithm. However, the morphology of mECG\(_\text{T}\) is different than that of mECG\(_\text{A}\), and is usually sensed with poor quality, resulting in deteriorated extraction by the ANFIS structure [4]. For these reasons, Al-Zaben et al. [124] focused on using aECG signals and SVD algorithm only. SVD was able to carry out high-quality estimation of mECG\(_\text{A}\) and aECG with emphasised fetal component from the aECG signals, which were subsequently used in ANFIS. ANFIS was also proved suitable for suppressing interferences according to Skutova et al. [60]. Two synthetic input signals were used for each tested recording; the first one contained only a maternal PCG signal, the other contained an abdominal PCG signal with a combination of mHSs, fHSs, biological and ambient noise. The number of tested membership functions ranged between 2 and 9, the number of epochs was 10 to 30, and 4 shapes of membership function were tested (triangular, trapezoidal, bell-shaped, and Gaussian). The research proved that the growing number of membership functions and epochs and the use of trapezoidal and bell-shaped membership functions led to a higher-quality filtration (higher SNR values). From the perspective of compromise between the extraction quality and the computation time, the setting with 6 membership functions and 10 to 20 epochs has been considered optimal. Nevertheless, the authors recommended using the ANFIS method combined with another algorithm such as PSO or GA to suppress the residual mHSs.
3.1.2 Nature-Inspired Optimization Techniques in Noise Suppression
Nature-inspired optimization algorithms are suitable for estimating the global optima for challenging optimization problems. They are usually implemented in combination with other algorithms to achieve a better result from the perspective of accuracy [42, 125]. Algorithms that require optimization of higher number of parameters (e.g. adaptive methods or ANNs) [59, 76, 79], can provide accurate and time-effective solutions thanks to the nature-inspired intelligence algorithms, and could be implemented in a device operating in real-time.
-
Differential Evolution DE is an evolutionary algorithm, which is inspired by biological evolution. Similarly to other algorithms, DE uses conventional operations such as mutation, crossover, and selection [73, 126]. The search is based on the selection of initial population and a subsequent simulation of its development, while being under the control of evolution mechanisms. As the population evolves one generation after another, bad solutions tend to disappear, while good solutions frequently “interbreed,” creating even better solutions (the fitness function of the algorithm improves). The aim is therefore to find such generation of the population that offers the best solution to a problem [42]. Beside the ANFIS-EKS [74] (mentioned in the ANFIS subsection), DE was also implemented in combination with an adaptive algorithm for the purpose of fECG extraction [73]. The DE method helped with the optimization of the adaptive filter coefficients. DE parameters were set to population size of 20, a scaling factor of 0.5, a crossover ratio of 0.9, and a maximum number of cycles of 500. The results were compared to the classic LMS filter. According to the visual comparison of the extracted fECG, residues of maternal QRS (mQRS) complexes were visible when LMS was used. These residues were fully suppressed by the use of DE and adaptive filter and allowed accurate detection of the fQRS complexes.
-
Particle Swarm Optimization The PSO algorithm belongs to a group of algorithms inspired by the behaviour of biological swarms, in this case of a flock of birds searching for food. Particles defined by its position, speed, and memory of the previous successful searches are created and then moved around the defined search space. Their position and speed are updated in iterations based on the fitness function. The pattern for searching individual particles is influenced by its own experience and by the experience of more successful particles within the flock [127]. During their tests of non-linear fECG extraction, most authors [59, 77, 119] used the PSO method in combination with ANFIS, as mentioned earlier. Optimizing an adaptive algorithm using the PSO method is also a suitable tool as mentioned by Anoop et al. [76]. According to Panigrahy et al. [128], another option is to use PSO to initialize and optimize EKS parameters which participate on the modelling of the mECG\(_\text{T}\) signal according to the morphology of mECG\(_\text{A}\) in aECG. The combination of PSO and EKS yielded ACC = 89.7%, surpassing the basic EKS and adaptive RLS method.
-
Moth-Flame Optimization Current research in the field of fECG focuses on implementing relatively new algorithms, one of which is MFO designed in 2015 [129]. The algorithm was inspired by the navigation method used by moths. Moths maintain a fixed angle with respect to the moon, allowing them to travel long distances in a straight line. When moths see artificial light, they try to maintain angle similar to the light. However, the artificial light is closer than the moon, causing the moths to spiral around the light instead of flying forward [129, 130]. Moths are therefore considered as search agents moving in search space, while the flames are the best position. At first, the positions of moths within the search space are randomly generated, followed by their evaluation with fitness function, resulting in the designation of the best position. The positions of moths are updated to achieve better positions with respect to flames. The whole procedure recurs until the termination criterion is reached [130]. MFO with adaptive LMS algorithm designed by Jibia et al. [79] proved to be a suitable combination, where the MFO method excelled in high global search capability, simplicity, flexibility, and easy implementation.
3.2 Feature Detection
In order to analyse the filtered signals, the key signal features must be detected and extracted. For these purposes, AI was used to detect fQRS complexes in an fECG signal [47, 49, 53, 81,82,83,84,85] to estimate fHR [20], or to detect fHSs in an fPCG signal [45, 48]. There are two types of fHSs in a noiseless fPCG signal (S\(_1\) and S\(_2\)). The S\(_1\) sound is generated by closing the mitral and tricuspid valves, while the S\(_2\) sound is generated by closing the aortic and pulmonary valves [32, 131]. The S\(_1\) sound is usually detected to determine the fHR in a fPCG signal and corresponds to the R peak in an fECG signal.
3.2.1 Artificial Neural Networks in Feature Detection
Analysis of fECG recordings, including the detection of fQRS complexes is generally considered as a challenging task. This is mainly due to the complicated suppression of mQRS complexes, residues of which make accurate detection of fQRS complexes difficult [47]. Various types of ANNs proved to be very promising for this task [53, 81,82,83,84,85]. According to [20], fHR could be estimated without having to detect R peaks.
-
Convolutional Neural Networks In 2018, Lee et al. [53] implemented a network of CNN with 10 layers for detecting fQRS complexes, which was able to reliably detect fQRS complexes without having to eliminate mECG from the input signal. The aECG signals were brought into the CNN by small portions of 100 samples and the network output yielded a probability of the input being in the group marked 0 (not an fQRS complex) or 1 (is an fQRS complex). The network comprised a total of seven convolutional layers, two fully-connected layers, and one softmax layer. The designed approach provided better detection of fQRS with SE = 89.06%, PPV = 92.77% compared to the earlier-tested CNN mentioned in Zhong et al. [85], which achieved SE = 80.54%, PPV = 75.33%, F1 = 77.85%. This was probably caused by the fact that the first mentioned CNN was multi-channelled and comprised a deeper architecture than the less-effective CNN, which had a single channel and only three convolutional layers. In addition to a time domain, CNN can also detect fQRS complexes in time-frequency domain. This approach has been used by Lo et al. [81] who normalized and segmented four input aECG signals in the pre-processing phase, followed by application of a short-time Fourier transform (STFT) to acquire time and frequency representation of signals. The representation was used as CNN input containing two convolutional layers, two pooling layers, and one fully-connected layer. Individual features were classified into four groups representing (1) mQRS complexes, (2) fQRS complexes, (3) overlapping mQRS and fQRS complexes, and (4) noise. The results of classification of each aECG recording were merged to derive final detection of fQRS complexes. With its ACC = 87.58%, CNN substantially surpassed the k-NN algorithm with its average ACC = 77.78%. Vo et al. [84] designed an innovative approach using a 1-D octave CNN for detecting fQRS complexes without the necessity to have a reference mECG\(_\text{T}\) available. The method combined CNN and RNN with residual network architecture. Although the combined approach did not require any substantial data pre-processing, it achieved very high performance (F1=91.1%). The method was able to acquire more contextual information and reduce temporal redundancy, thus decreasing the computational complexity. However, the need to set a large number of parameters appropriately can be considered a limitation of this algorithm. Fotiadou et al. [20] used a combination of dilated inception CNN and LSTM for fHR estimate, which they used to capture the short-term and long-term temporal dynamics of the fHR. The fHR could be estimated without having to detect R peaks. They selected this approach because the SNR was low in some cases, making the detection of R peaks difficult. CNN was used to extract features in an fECG signal, while LSTM was used to model temporal dynamics and subsequently estimate fHR. The combination of algorithms was tested on real recordings and its effectiveness was evaluated using a positive predictive agreement (PPA). High accuracy of determining the fHR was achieved, with average PPA = 98.45%, however, the authors stated that the method is limited by the necessity to set up many parameters (e.g. number of layers, dilation rates, number of nodes for each layer, type of layers). To eliminate these disadvantages of CNNs, i.e. the high computational complexity and the need to set a large number of parameters, Krupa et al. [132] proposed to use a MobileNet-based approach for the detection of fQRS complexes. MobileNet is an improved type of CNN that is not very computationally intensive, is low-latency and low-power. The network uses a much lower number of parameters since its architecture is composed of depthwise separable convolutions. The efficiency of the network is not reduced, as high accuracy (ACC = 91.32%) was achieved when tested on real signals. According to the authors, this solution is also suitable for the Internet of Things environment and thus for remote fetal monitoring.
-
Echo State Networks An approach based on a data-driven statistical learning approach, combining ESN and statistics-based dynamic programming algorithms for detecting fQRS complexes, was explored by Lukosevicius et al. [82]. ESN trained to mark fetal R-peaks in a signal with cancelled mECG was used in the first step. The setting of the ESN approach was as follows: ESN reservoirs of size 1000 or 500, leakage rate value of 0.9, spectral radius of the reservoir connection matrix of 0.9 or 0.94, input scaling of the input weight matrix of 0.1 or 0.08. Dynamic programming used the signal with marked fetal R-peaks created by the ESN and interpreted it in a probabilistic way. Various probabilistic interpretations were tested such as direct interpretation based on threshold settings, interpretation assessing the length of R-R interval, interpretation assessing the R-R interval variation, or a combination of the second and third probabilistic interpretation. It has been proved that using substantially less reservoirs had lower impact on the accuracy of the algorithm than using the less powerful dynamic programming algorithm. The benefit of the algorithm is the lack of necessity to have a reference mECG\(_\text{T}\) signal.
3.2.2 Machine Learning in Feature Detection
ML-based algorithms are able to automatically identify patters in fECG or fPCG signal and classify them in an uncertain environment [42]. Both supervised and unsupervised learning algorithms proved to be effective.
-
K-means and K-medoids Both algorithms are based on unsupervised learning and belong to a group of partitioning clustering methods [49]. The goal of the algorithm is to partition the objects into pre-selected number of clusters. The objects are grouped into clusters based on minimizing the sum of squares distances between the objects and the cluster centroids. The algorithm is iteration-based and randomly selects a location of centroids, assigns objects to the closest centroids and creates clusters. The position of centroids is recalculated so that they represent the new mean of the cluster of objects assigned to it. In the next step, objects are again assigned to newly determined centroids and the process repeats until the position of centroids stabilizes [133, 134]. However, the k-means algorithm is susceptible to outliers. This drawback is eliminated by the k-medoids method, which uses medoids instead of centroids [133]. The k-means method proved to be more suitable for smaller datasets, while the k-medoids method was more effective for the larger ones [134]. Castillo et al. [49] used the k-medoids clustering algorithm for partitioning the features of aECG signals. The input signals were pre-processed using WT and the features were clustered with k-medoids into three groups: (1) mQRS, (2) fQRS, and (3) noise. The clustering process was based on information regarding the amplitude and time distance of all the local maxima followed by a local minimum. The method proved to offer high accuracy (ACC = 97.19%) of detection of fQRS complexes and the subsequent determination of fHR in a wide scale of signals with various characteristics and in signal with noisy sections and managed to surpass classic threshold techniques. For the purpose of determining fHR from the fECG, Alvarez et al. [47] compared k-means, k-medoids, and two more clustering algorithms—hierarchical and fuzzy c-means. The input signals were pre-processed using the WT method and signal features were clustered into three groups: mQRS, fQRS complexes and noise, using the same rule as in [49]. The most accurate detection of fQRS complexes and determination of fHR, with ACC = 94.8%, was achieved using k-means based on city-block distances, followed by a k-medoids algorithm based on squared Euclidean distances, which yielded ACC = 94.5%. Fuzzy c-mean yielded even less accurate detection (ACC = 93.7%), while hierarchical clustering provided the worst results (ACC = 87.8%). The k-means method combined with independent component analysis (ICA) for processing fPCG signals was presented by Jimenez-Gonzalez et al. [48]. Real abdominal recordings were decomposed by the ICA method to individual source components. With k-means, patterns of individual ICA components were distinguished and these components were effectively grouped into clusters corresponding to fHSs, mHSs, maternal respiration and noise based on their spectral similarities. The authors evaluated the effectiveness of the combined method using specificity (SP) and SE parameters and achieved high SP = 99%, but low SE = 68% values.
-
Random Forest Supervised learning classifiers called decision trees [135, 136] are based on recursive partition of the instance space. The decision trees are designed using a sequence of nodes (a spot where a decision is made) and edges (decision-making variants, e.g. weight or probabilistic evaluation). Each node represents one signal feature, where the root node is the highest-level node with no incoming edges while the other nodes have one incoming edge. Nodes with outgoing edges are called internal nodes and other nodes with no outgoing edges are called leaves or terminal nodes and represent class labels [136]. The whole classification procedure starts with root node and ends with a decision at the leaves. Advantages of decision trees algorithms include particularly low demands on data pre-processing, and the ability to process data containing errors or missing values. The drawback of this algorithm is its computational complexity compared to a single decision tree [135, 136]. In general, random forest profits from creating many (hundreds to thousands) decision trees. The class that is most frequently selected by individual trees is then considered as the outcome class. The selection of features is random and is based on the idea of bagging, allowing to create a group of trees with controlled variance [137]. The random forest algorithm proved to be the most suitable for detecting fetal S\(_1\) sounds in fPCG compared to other three methods (logistic regression, SVM, MLP) according to the results of experiments conducted by Vican et al. [45]. All algorithms were tested in combination with EMD. The EMD method decomposed the input fPCG signal to three intrinsic mode functions (IMFs) which correspond to individual frequency bands of the input signal. Each IMF was split to 200 ms long windows with a hop of 50 ms, and a total of 18 statistical and 9 spectral features were extracted. The extracted features were used to predict the presence of S\(_1\) sounds. Accuracy of the classifiers was validated through the presence of peaks in Doppler signals acquired concurrently with the fPCG signals. With the exception of random forest with ACC = 72.8%, all other algorithms yielded ACC below 67%.
3.3 Fetal State Classification
CTG recordings are currently used in clinical practice as the most common indicator of fetal medical condition and indicator of fetal hypoxia. However, accurate identification of fetal hypoxia using a visual evaluation of fHR trace and the curve of uterine contractions by medical personnel did not lead to satisfactory results in the past. High variability of opinions in doctors interpreting of CTG recordings led to large inter- and extra-observer disagreement [138].
In order to eliminate the inconsistencies and variability, The International Federation of Gynaecology and Obstetrics (FIGO) implemented a standard for evaluating CTG recordings and classifying them as normal, suspicious, and pathological. The newest FIGO2015 system [1] recommends evaluating the fHR baseline, fHR variability, or decelerations, see Table 1. Despite the implementation of these recommendations into clinical practice, interpretation of CTG recordings, or detection of fetal hypoxia, remains inaccurate even today [139]. This may be due to the length of the recording or its poor quality, as well as due to its dynamics and complexity. Visual interpretation of these recordings is still very difficult for medical experts and highly influenced by human factor and experience of the respective doctors [139, 140].
For these reasons, several recent works in the literature focuses on developing automatic AI-based systems for evaluating fetal medical condition using computerised interpretation of the CTG recordings [87, 89, 108, 141]. Since the alternative techniques of fECG, fPCG a fMCG also allow determining fHR traces (in addition, fECG and fMCG allow extracting electrohysterographic signal providing information about uterine contractions, same as with CTG), several authors focused on classification of fetal medical condition through fPCG [66, 90, 91] or fMCG [44]. These fHR traces were subsequently classified via AI-based algorithm, similar to CTG. Automated AI-based systems could distinguish and analyse fHR and uterine contraction patterns better than a human expert, allowing obstetricians to determine the fetal diagnosis faster and with higher accuracy. The processing and analysis of records using the AI consist of the following three main steps: pre-processing and noise suppression, feature detection and extraction, and fetal state classification.
-
1.
Pre-processing and noise suppression CTG signals measured in clinical practice are usually noisy, which is caused mainly by movements of the mother or the fetus [142]. This leads to poor contact of the sensors with the mother, thus creating artefacts and short-term signal losses. This may also result in a situation where maternal heart rate is measured instead of fHR, leading to fHR signal drops to a lower value [143]. Signal pre-processing, noise suppression [12, 13, 142, 143], and elimination of outliers [13, 43] therefore proved to be an important step for the follow-up accurate classification of the fetal health state.
-
2.
Feature detection and extraction Detection, extraction, and selection of appropriate signal features that will be used as classification algorithm inputs are key for successful classification as well. The combination of features in the time and frequency domain seems to the optimal. Cardiotocography dataset [144] containing prepared CTG signal features that are acquired from 2126 CTG recordings recorded in clinical practice is broadly used in many studies [46, 65, 72, 78, 88, 89, 145]. Each recording contains 21 features extracted from an fHR trace as well as from a uterine contractions curve (e.g. fHR baseline, number of accelerations per second, minimum/maximum of fHR histogram, or number of uterine contractions per second), and reference classification of the recording into one of three classes (normal, suspect, pathological) done by expert obstetricians. Georgieva et al. [146] also used clinical features such as fetal gestation age or maternal temperature during labour for the classification. For optimal feature subset selection, the FA [78] or GA [72] have proven to be effective. Many studies [72, 86, 147, 148] proved that lower amount of appropriate features leads to a more accurate classification compared to having a higher number of features that do not carry important information or distort the resulting classification.
-
3.
Fetal state classification After selecting an appropriate classification algorithm, training, and parameter tuning, resulting classification is done using the test dataset. The fetal state classification usually comprised two classes (normal, abnormal) [147, 149, 150] or three classes (normal, suspect, pathological) [54, 86, 87].
3.3.1 Artificial Neural Networks in Classification
In order to successfully classify a fetal state using ANNs, a suitable type of ANN must be selected as well as its architecture and hyper-parameter setting [87]. Using a classic feed-forward multilayer network requires setting up the number of neurons in the input layer, the number of hidden layers including the number of neurons, the number of neurons in the output layer, training algorithms (e.g. gradient descent BP, Levenberg-Marquardt BP, quasi-Newton BP) [87, 151], training concept (incremental-weights are updated in each iteration, or batch-weights are updated only when all inputs are available in the network) [87], number of epochs, learning rate (usually a small positive value ranging between 0 and 1) [152], and an activation function (e.g. linear, sigmoid, Gaussian) [151].
Comert et al. [87] achieved accurate fetal state classification by means of the CTG recordings and feed-forward ANN, a structure that included 21 input variables, 10 nodes in a hidden layer, and 3 nodes in an output layer. A test was conducted on a total of 12 training algorithms, including, for example, gradient descent BP, gradient descent with adaptive learning rate BP, resilient BP, conjugate gradient BP with Fletcher-Reeves restarts, or one-step secant BP. The authors achieved the best results with the resilient BP training algorithm and an average of 5707 epochs. Noguchi et al. [153] used substantially more nodes (30) in the hidden layer. The authors used 24 nodes in the input layer and 3 nodes in the output layer in combination with the BP training algorithm. The study outcomes proved that evaluating a CTG recording longer than 50 min was difficult and recommended a shorter measuring period to make the analysis more accurate, e.g. 15 min and analysing it every 5 min. Georgieva et al. [146] employed only 2 neurons in a hidden layer, 12 neurons in an input layer, and 2 neurons in an output layer. Instead of implementing a single ANN, the authors tested a combination of 10 ANNs so that each network was trained in a different section of the dataset and that the result was determined as an average of all 10 outputs. Quasi-Newton BP algorithm [154] and the hyperbolic tangent transfer function were used in all networks. The basic assumption that multiple networks tested on different parts of the dataset can provide better performance, was confirmed.
In 2007, Jezewski et al. [147] used a feed-forward ANN to classify fetal condition from CTG recordings and testing several configurations of the used signal features. The best results were achieved by reducing the number of the used features from 21 to 7 (some features did not carry important information about the fetal condition). Since more than 50% of the recordings were of the female patients, where multiple CTG recordings were made, the recording acquired the closest to the date of labour proved to be the most suitable.
Comert et al. designed an interesting extension for selecting and extracting features in [149]. In addition to the usual morphological, spectral, and statistical characteristics, they used new features such as contrast, correlation, energy, and homogeneity. This was ensured by transforming signal spectra containing time and frequency information into 8-bit grey images and creating a grey-level co-occurrence matrix (GLCM). The subsequent classification with ANN led to a more accurate classification of the fetal condition by means of CTG compared to using traditional features only. However, using solely GLCM features without the traditional ones did not yield satisfactory results.
-
Convolutional Neural Networks CNN was used to classify fetal medical state using CTG recordings by Tang et al. [12]. The network contained five convolution blocks (each convolution block contained three convolution layers), three full connection layers, and one softmax layer. CNN was able to classify the fetal medical state into two groups with substantially higher accuracy (ACC = 94.7%) compared to the SVM method (ACC = 83.46%), random forest (ACC = 84.5%), and RNN (ACC = 90.3%). The self-training CNN with eight layers (input, convolution, activation, normalization, pooling, fully-connected, dropout, and classification layer with softmax function) were implemented by Zhao et al. [108] to predict fetal acidaemia based on features acquired from CTG by means of continuous WT (CWT). Daubechies wavelets and symlet with an order of two and wavelet scales of four, five and six were used. CWT was used to extract the features due to its ability to capture hidden signal characteristics concurrently in the time and frequency domain. In addition, the classic signal features were susceptible to distortion during extraction. The same authors, Zhao et al. [141] slightly improved the classification using a combination of CNN and recurrence plot, which was able to capture non-linear signal characteristics. However, the disadvantage of CNN is the computational complexity and the need to optimally set a large number of parameters for the network to work effectively.
-
Probabilistic Neural Networks Probabilistic ANN is an implementation of Parzen windows probability density approximation. It is a feed-forward network consisting of four layers (input, pattern, summation and output) [54]. In 2016, Yılmaz [54] presented probabilistic ANN for fetal medical state classification using the CTG. The number of neurons in an input layer was given by the number of features in a dataset (21 neurons). The number of neurons in a pattern layer was given by the number of used training patterns, while each neuron was connected to all neurons in an input layer (1913 neurons for 6 iterations and 1914 for 4 iterations), 3 neurons (number of classes) in a summary layer, 1 neuron in an output layer, which applied Bayes decision rule and carried out classification. The optimum value of the smoothing parameter was 0.13. The performance of the method was compared, among other, with MLP containing 2 hidden layers with 20 neurons in each. The classification accuracy was similar in both methods, probabilistic ANN with ACC = 92.15% slightly surpassed MLP with ACC = 90.35%. The high storage needs can be considered as limitation of the method.
-
Legendre Neural Networks Legendre ANNs are single-layer networks consisting of functional Legendre expansion block based on Legendre polynomials and an output layer. Hidden layers are eliminated, since the input is transformed into higher dimensional space using Legendre polynomials. These networks excel particularly with their simple implementation and speed [155]. Highly accurate classification of fetal state using CTG recordings and the second-order Legendre ANN was designed by Alsayyari [86]. When using 21 attributes, 4 signals out of 1000 were misclassified, with 10 attributes, only 2 signals out of 1000 were misclassified. In addition, only several iterations (5 to 10) were required for training. Legendre ANN had lower computational requirements compared to the Volterra ANN and converged faster with a lower mean square error. The Legendre ANN performance could be improved by increasing the Legendre polynomial order in the testing phase.
3.3.2 Machine Learning in Classification
The ML algorithms also proved effective for classification of fetal medical state. The research in this area focused particularly on testing the supervised learning algorithms [43, 46, 72, 88, 89].
-
Support Vector Machine One of the important representatives of ML is the SVM method [156] based on supervised learning. The main goal of the algorithm is to assemble a hyperplane so that the space of features has optimal distribution (data belonging to different classes will lie in opposite semi-spaces). In optimal situation, the minimum value of distance of points from the hyperplane is as high as possible. In other words, the maximal margin is as high as possible on both sides around the hyperplane [89, 142]. The hyperplane can be described by only the points on the edge of the band, while there is usually not many of them; these are called support vectors. The kernel transformation allows transforming the originally inseparable task to a linearly separable one, on which an algorithm for finding the separating hyperplane can be applied [89]. SVM seems to be a very promising technique for classification and prediction of fetal medical state using CTG recordings. In the study of Nagendra et al. [88], the SVM method yielded accuracy similar to random forest (the average ACC > 99% in both cases). However, the SVM algorithm performed slightly better with suspect signals. Comparison studies [11, 13] had similar outcomes and concluded that the SVM method performed better than algorithms such as ANN, k-NN, or decision tree. The SVM method had another particular advantage over ANNs—it did not require many model parameters and always found a global solution during the training. An important factor for acquiring high-quality results from CTG recordings is to select suitable signal features that will serve as the classification algorithm input. Lunghi et al. [148] used a total of nine features for the classification, originating from the time and frequency domains, morphological features, and regularity parameters. They achieved the most accurate classification in a test phase, using only six features. Other features carried less information and could be therefore omitted. Appropriate feature selection and dataset balancing were also highlighted as key prerequisites for accurate CTG classification using SVM by Ricciardi et al. [157]. The optimal feature subset could be found with FA according to Subha et al. [78] or GA according to Ocak et al. [72], which was able to detect the most important features and ignore the irrelevant ones. This led to the maximization of the subsequent classification by means of SVM and, at the same time, to the reduction of the number of used features (from 21 to 13). As Krupa et al. [142] proved, feature extraction from CTG could also be done with the EMD method, which decomposed the input signal to individual IMFs. High-frequency IMFs were eliminated and a standard deviation value was calculated for the remaining ones. Standard deviations were considered as signal features and served as the input of a SVM classifier, which classified them into two groups: normal and at risk. Silwattananusarn et al. [89] proposed improving the stability of CTG signal features in order to improve the performance of SVM with polynomial kernel function. To do this, a combination of two feature search strategy approaches (correlation-based feature selection and information gain) was used. The selected features entered an ensemble of seven SVM classifiers that yielded ACC = 99.85%. A modified version of the classic SVM - least squares SVM (LS-SVM) was designed by Yilmaz et al. [145]. In addition, PSO was used to optimize parameters, leading to an effective classification, but at the cost of increasing the computational complexity of the algorithm. When classifying a fetal state by means of an fHR trace estimated from fMCG, SVM proved to be the best choice compared to MLP and J48 decision tree (also known as C4.5 algorithm), as shown in the experiments in Snider et al. [44]. Signals were acquired from fetuses with the age of 24–39 gestation weeks, and features used in the classifications were selected from the time (e.g. RR interval mean, RR interval standard deviation) and frequency domain (e.g. peak frequency, kurtosis). All three methods yielded similar accuracy, but SVM with ACC = 66.2% was slightly more accurate than the C4.5 algorithm with ACC = 65.4% and MLP with an overall ACC = 61.4%.
-
Naive Bayes The naive Bayes probabilistic classification algorithm is the simplest Bayesian network model based on an assumption that there is a strong (naive) independence between the extracted features. Despite its simplicity and unrealistic independence assumption, this algorithm is effective and correct in real-world tasks [158]. The algorithm was tested for classification of fetal state with CTG recordings by Avuclu et al. [46] and achieved ACC = 97.18%.
-
Decision Trees Among the leading representatives of decision trees used for the interpretation of fetal medical state with CTG is the random forest published by Subasi et al. [150], who achieved ACC = 99.02% in their experiments. Based on the research conducted by Jacob et al. [43], after detecting and eliminating outliers from the CTG recordings, the use of both, the classic random forest and the C4.5 algorithm yielded ACC = 100% (C4.5 is a single tree algorithm based on the concept of information entropy [159]). In some cases, the presence of outliers caused inaccurate diagnosis. Reducing computational cost while maintaining high classification accuracy using random forest was achieved in experiments conducted by Sharma et al. [160]. They combined random forest with enhanced binary bat algorithm (EBBA), which was used for optimized feature set selection and hence for dimensionality reduction. EBBA selected only a set of 11 out of 21 possible features for classification while achieving ACC = 96.21%. A similar results were obtained when EBBA was combined with decision tree (ACC = 94.36%) or with k-NN (ACC = 94.67%). According to the authors, further improvements could be achieved by hybridization of various nature inspired algorithms.
3.3.3 Fuzzy Logic in Classification
Fuzzy logic classification is based on determining the degree of truth of an feature into a fuzzy class represented by a membership function. Features are classified by means of a set of fuzzy rules based on linguistic values of its attributes [161, 162]. The relevance and redundancy of the resulting classification should be considered in the final decision [161].
Jezewski et al. [68] implemented fuzzy logic in the classification of fetal medical state with CTG recordings. To simplify the fuzzy classifier rule base, they combined the fuzzy classifier with \(\epsilon \)-insensitive distance. When classifying CTG signals into 2 classes using 12 signal features and evaluating the accuracy of classification using negative predictive value (NPV) and PPV parameters, very high NPV=97.63% was achieved, but with low PPV=40.17%. The drawback of the algorithm was the necessity of \(\epsilon \) parameter tuning, which could be overcome by implementing the ES algorithm, as shown in their previous research [75].
The classification of fetal state using fHR traces acquired from fPCG signals into three groups (normal, abnormal and suspicious) by means of fuzzy logic was presented by Chourasia et al. [66]. An envelope of the signal filtered by the WT method was detected by means of the Hilbert transform (HT) and converted into a series of rectangular pulses. These pulses were used to identify S\(_1\) and S\(_2\) sounds and calculate the fHR. Four features were extracted from each signal (baseline fHR, baseline variability, accelerations, and decelerations), followed by their classification by means of the fuzzy logic. The testing was conducted on real recordings and CTG was measured concurrently with fPCG. Medical experts used a CTG recording to create a reference classifications, which were used to evaluate the accuracy of classification by means of fPCG and fuzzy logic. Application of type-2 fuzzy logic with Mamdani type fuzzy inference system and Gaussian membership functions yielded ACC = 92.24%, which was substantially better than type-1 fuzzy logic, which yielded ACC = 81.03%. The results acquired with type-2 fuzzy logic were comparable with the results of the classification with ANFIS (ACC=92%) presented by the same authors in [91]. The five-layered ANFIS, the first-order Sugeno model, Gaussian membership functions were used, 961 epochs and 2–5 membership functions. Chourasia et al. used the same methodology to classify fetal state from an fHR trace acquired from fPCG also in [90], but for the final classification, MLP trained by an adaptive BP algorithm was used. The input network layer consisted of ten neurons, two tan-sigmoid hidden layers (ten and five neurons) and a linear output layer of three neurons. MLP yielded ACC = 95.7%, surpassing fuzzy logic and ANFIS. Recording and analysis of fPCG signals was difficult in women with high BMI values.
-
Fuzzy Unordered Rule Induction Algorithm FURIA is a fuzzy rule-based classification algorithm that excels primarily in datasets with many features. Its characteristic attribute is that the rule set is generated for each class as one-vs-rest [65, 163]. Each class is therefore separated from other classes and no single class is prioritized as a default prediction. In addition, there is no default rule and the order of rules is irrelevant [163]. An estimate of membership function plays a key role in the application of fuzzy sets. According to the study of Das et al. [65] conducted in 2014, ANN proved suitable for estimating a membership function. Compared to the FURIA approach presented earlier in 2013 by the same authors [164], using the combination of ANN and FURIA for classification of fetal medical state using CTG led to a reduction of error rate with pathological recordings and to an increase of suspicious recordings detection accuracy.
4 Summary and Discussion
The review showed that the current research in this area focuses on improving conventional CTG as well as on alternative fECG, fPCG, and fMCG techniques for monitoring fetal cardiac activity. Fetal cardiac signals acquired by these techniques carry very important information about the medical state of the fetus. However, these complex and often very long signals are relatively difficult to analyse and correctly interpret without using information technology. In addition, the environmental effects, biological tissues, and movements of the mother and the fetus make the use of clinical information difficult, rendering the use of signal processing methods inevitable. With the developments in science and technology, it was possible to implement and test plenty of AI-based and ML-based algorithm in the recent past, which appear to be more effective than conventional signal processing methods.
Unfortunately, it was rather difficult to objectively compare the algorithms mentioned in this review, as the authors used different signals (real or synthetic) originating from different sources (publicly accessible databases or their own measured signals) with different quality (various types and noise levels) and they were not unified even in the applied evaluation parameters (ACC, SE, PPV, F1, SP, PPA, NPV or SNR\(_{\text{imp}}\)). The authors did not evaluate the quality of extraction by means of statistic parameters in some cases, but merely visually evaluated the extracted signals. These criteria should be unified in future research and create one extensive dataset (similar to the case of CTG and the existing UCI CTG dataset [144]), which would be the only dataset used for objective comparison of the algorithms. For these reasons, we tried to summarize the performance of the presented algorithms both objectively and subjectively and to highlight the most important findings and outline the directions, in which researchers in the field of EFM related to AI should be heading in the future.
4.1 Noise Suppression
Effective noise suppression appears to be a great challenge, particularly in the case of fECG and fPCG. Based on the statistic results of each method summarized in Table 2 and based on a subjective comparison of the extracted signals in each study, one could summarize that most of the tested ANNs were effective. The different performances of algorithms could be caused by a different dataset used in the testing or by using less suitable algorithm parameter settings, which have a major impact on the extraction quality.

Influence of parameter setting (p and \(\eta \)) on the performance of ADALINE algorithm during extraction of fECG in a form of 3D plot and extracted fECG signals. Example (a) shows 3D plot, example (b) demonstrates an incorrect parameter setting, leading to insufficient suppression of mECG, and example (c) shows optimal parameter setting leading to sufficient elimination of mECG

Influence of input aECG signals quality on the resulting efficiency of fECG extraction. Example (a) shows high-quality aECG signals and effective extraction of fECG using the ANFIS method. On the other hand, example (b) shows poor-quality aECG signals, the use of which leads to insufficient suppression of the maternal component and to an unsatisfactory quality of the fECG
The need to set up large number of parameters and the rather demanding computation are among the main limitations of ANNs. In case the parameters are set up incorrectly, the performance of the methods is substantially affected, leading to reduction of the method’s effectiveness. This effect of suitable parameter settings on the resulting performance of an algorithm for extracting fECG for a simple ADALINE network is demonstrated using a 3D plot and extracted fECG signals in Fig. 6. The example shows the effect of the input space (p) and the learning rate (\(\eta \)) parameters on the ACC parameter value. As shown in Fig. 6a, the algorithm working area is marked red and corresponds to an area of p\(\in \)(50;100)\(\bigcap \eta \in \)(0.001;0.06). It is an area where the algorithm was stable and reached ACC > 85%. Setting the algorithm parameters outside the working area led to a deteriorated performance of the algorithm. As illustrated in Fig. 6b, the algorithm was unable to eliminate the maternal component with the p=20 and \(\eta \)=0.064 setting, which led to a very low ACC = 66.20%. The global maximum was reached with p=100 and \(\eta \)=0.026 setting and led to (Fig. 6c) sufficient suppression of the mECG resulting in ACC = 88.84%.
Further, this review showed that nature-inspired optimization algorithms are effective for finding optimal parameter values of extraction algorithms. However, despite improvements in the performance of extraction algorithms, they might be computationally more expensive than conventional learning algorithms (e.g. BP). To improve the algorithm performance and to determine of the optimal setting faster, the ANNs should be combined with modern optimization algorithms (e.g. grey wolf optimizer (GWO) [170] or whale optimization algorithm [171]) or other improved hybrid versions of these algorithms (e.g. improved PSO-GWO algorithm with chaos and a new adaptive inertial weight [172]). The use of an accurate and time effective extraction algorithm would allow its implementation in devices operating in real time.
Nevertheless, in some cases, even after optimizing the algorithm parameters, it is almost impossible to eliminate the maternal component. These are cases that use input aECG signals with poor quality (low magnitude of fetal component compared to the maternal one, presence of other interferences). Influence of input aECG signals quality on the resulting efficiency of fECG extraction using the ANFIS algorithm is shown in Fig. 7. Figure 7a represents aECG signals acquired with high quality and adequate magnitude of fetal component compared to the maternal one, leading to a high-quality extraction of fECG signal by the ANFIS method. Conversely, Fig. 7b shows the effect of poor-quality aECG signals, where the fetal component has low magnitude compared to the maternal component and where the useful fECG signal is contaminated by other interferences. The extraction is very difficult in this case and leads to insufficient suppression of the mECG and to a decrease in filtration quality.
The quality of aECG signals is given primarily by the positioning of sensing electrodes, which is currently not a standardised matter and should be a subject of further research. One of the possible solutions to securing effective extraction even with poorly sensed signals might be the implementation of hybrid algorithms that combine the advantages of several AI-based methods (e.g. hybrid fuzzy CNN [173] or CNN-LSTM [174]). When designing and implementing extraction algorithms, the tested algorithms should not alter the morphology of the extracted fECG signals so that a morphological analysis can be done (ST segment or QT interval analysis), thus helping to make the detection of fetal hypoxia more accurate.
4.2 Feature Detection
Feature detection in this review included detection of fQRS complexes, estimation of fHR without having to detect R-peaks, and detection of fHSs. AI-based algorithms proved to be very promising for these tasks, even in signals with lower SNR values, which pose a risk of false positive detection of a peak that is not generated by a fetal heart (e.g. mQRS complex, mHS, or residue of another interference). Based on the results summarised in Table 3, it can be stated that the most accurate detection was provided by k-means and k-medoids algorithms, which surpassed most of the other algorithms. In addition to that, these algorithms are far quicker than ANNs and simpler from the perspective of algorithm parameter settings.
However, very few authors addressed this area in the past and further research is needed. Therefore, it would be useful to test a broader range of AI-based algorithms in the future, especially nature-inspired optimization algorithms for feature selection. These algorithms (e.g. FA algorithm [78] and GA algorithm [72]) has proved to be effective as feature selectors for fetal state classification. It would also be beneficial to conduct research for the purposes of detecting S\(_2\) sounds in fPCG, which are difficult to distinguish and detect in signals with low SNR ratio [175]. Research in the field of fPCG signal analysis might be also beneficial to doctors in detecting pathological heart murmurs. These may be caused by tissue vibrations or when the laminar blood flow changes to turbulent [176], while the detection thereof may contribute to the identification of heart abnormalities (e.g. aortic valve stenosis or mitral stenosis) [16, 176, 177].
4.3 Fetal State Classification
In order to overcome the human intra- and inter-observer variation during the evaluation of fetal state, using an automatic intelligent classification system is inevitable. The research focused on testing the classification algorithms used particularly with CTG recordings. Several authors decided to classify a fetal state using fPCG and fMCG recordings as well. Table 4 lists the results achieved by individual algorithms used for classification along with corresponding dataset, number of classification classes and number of signal features used. Even in this case, the comparison of individual algorithms was difficult due to the different datasets used. However, when comparing study results that utilized the same UCI CTG dataset [144], it can be concluded that ANN achieved worse results than ML-based algorithms and thus were less suitable for this task. The SVM method and the random forest proved the most effective. The use of fuzzy logic seems to be promising as well. However, this approach was implemented and tested by only a few authors. Therefore, further research in this area is necessary.
The research also demonstrated that the selection of algorithm as well as the selection of suitable signal features play a key part in the correct classification. Some authors conducted the classification only based on extracted fHR features [12, 66, 91, 148], some combined these fHR features with uterine contraction features (number of uterine contractions per second) [54, 87, 145, 150], while some others included additional features such as fetal gestation age and maternal temperature during labour [146]. The combination of uterine contraction features and fHR features could substantially affect the classification accuracy, since evaluating the isolated fHR features only might not provide accurate information about the fetus’ reaction to the labour. Fetal pathology may be therefore indicated incorrectly in relation to the fetus’ reaction to uterine contractions [143]. For these reasons, it would be interesting to include other uterine contraction features in the future research such as their length or frequency.
One of the areas that have not been addressed enough so far is the classification of fetal medical state by means of fECG signals. Nevertheless, the ability to acquire fECG signal from abdominally acquired recordings for estimating fHR traces as well as the electrohysterographic signal that provides reliable information about uterine contractions (their frequency as well as intensity) makes this technique a very promising instrument.
5 Remaining Challenges and Open Research Questions
The aim of this section is to discuss the remaining challenges and future directions concerning the monitoring of a fetus, as well as the use of AI. Among the main challenges is the issue of selecting suitable input signals when measuring fECG via the mother’s abdomen using a higher number of sensing electrodes. Another important area, particularly with fECG, fPCG, and fMCG, is the absence of high-quality and extensive dataset with a broad range of data that could be used to test conventional algorithm as well as AI-based algorithms. The last area discussed is the use of parallel processing to reduce the computational cost of AI-based algorithms in connection with the use of Big data.
5.1 Selection of Input Signals
One of the interesting areas that might utilize AI is the selection of suitable input signals when measuring fECG. As mentioned earlier, unlike with the ECG performed on adults, the positions of sensing electrodes and their number is not standardised for fECG. Most authors recommend using larger number of sensing electrodes (e.g. Vullings [178] proposed using 8, while Taylor et al. [179] proposed 12 sensing electrodes) so that most of the mother’s abdomen is covered. Sensing electrodes location, as well as fetal position and pregnancy stage, affects the quality of the acquired signals, particularly from the perspective of magnitude and polarity [4]. The quality of each signal can therefore vary with individual sensing electrodes as well as over the course of pregnancy. Since the quality of input signals greatly affects the extraction efficiency, it would be desirable to suggest an AI-based algorithm for automated selection of the high-quality signals. With this, the extraction could be performed effectively and without unnecessary degradation.
This approach proved effective for example in Yang et al. [181] for channel selection and classification of electroencephalogram signals using a combined ANN-GA method. A similar approach in the field of NI-fECG for the selection of high quality input aECG signals was proposed by Baldazzi et al. [182]. First, signal quality indices were determined for each aECG signal. And then, these indices served as signal feature for subsequent classification using an ensemble tree classifier into two groups (informative or non-informative aECG signal).
5.2 Lack of Large Datasets
The key element for the correct use of AI- and ML-based algorithm is to have an extensive dataset available with large amount of diverse data (Big data), ideally with a reference class determined by experts. Such dataset is available only for CTG (UCI CTG dataset [144]) created particularly for classification tasks. However, there is no such dataset for fECG, fPCG, and fMCG, which is one of the reasons for limited research in these areas. There are several databases containing units or tens of real recordings that can be used with fECG and fPCG. Most databases contain physiological recordings, while pathological or abnormal signals are rarely included. In the case of fMCG, there is not a single publicly available database with real recordings, which is probably due to the costly and complicated acquisition of fMCG signals. Moreover, determining the reference class can be problematic in some cases, since even doctors might disagree with each other (low extra-observer agreement).
A possible solution to overcome this barrier would be to create an extensive database using simulated signals. Although real signals are considered more suitable, there are cases where the use of simulated signals is inevitable. These are, for instance, situations where the acquisition of real signals is very costly or where obtaining large amounts of data or a certain type of data is difficult (signals with abnormalities, pathology, signals of twins, etc.). AI-based algorithms, which seem to be suitable for generating dynamic biomedical signals [183], could be used for this task. According to Adamupoulos et al. [71], who created a model of synthetic fMCG signals by combining GA, multimodel partitioning theory, and extended Kalman filter, the modelled signals (physiological and abnormal) were visually almost indistinguishable from real signals.
5.3 Parallel Processing
The use of large datasets and Big data can significantly improve decision making or prediction by AI-based algorithms. However, due to the huge amount of data contained in the datasets, their diversity and high-dimensionality, it is not possible to process them by commonly used software tools in real time. The solution and the direction that AI and ML research should take is parallel processing, which allows to solve many computations in parallel and thus reduce computational costs. According to research by Liu et al. [184], who have successfully designed a parallel random forest algorithm based on distributed cloud computing platform for medical data classification, the future is likely to belong to remote distributed cloud computing.
6 Conclusion
This review has shown that the AI-based and ML-based approaches offer superior results to conventional algorithms and allow efficient processing and analysis of fetal signals obtained using both conventional CTG and alternative methods of fECG, fPCG or fMCG. Three main areas of application that are currently addressed were mentioned. The first focused on noise suppression, especially in fECG signals (elimination of mECG), where the extraction of an effective signal was difficult due to the overlapping fetal and maternal components in the time and frequency domain. This was similar in fPCG processing, where the challenge lay in eliminating various noise acquired along with the fHS. The second area focused on feature detection, including detection of fQRS complexes and estimation of fHR in fECG signals or detection of fHSs in fPCG signals. The last area addressed fetal state classification, particularly with CTG recordings, but also with recordings acquired by the alternative fPCG or fMCG methods.
Unfortunately, objective comparison of algorithms and selection of the most suitable algorithm in a given category was difficult because different authors used different datasets with signals of different quality. Moreover, the evaluation criteria and parameters were not unified. This was particularly due to the fact that there is no high-quality dataset with large amount of real physiological or pathological recordings available for the alternative fECG, fPCG, and fMCG techniques. Future research should focus on creating an extensive dataset that would contain various types of signals acquired with various quality, accompanied by references/annotation, with adequate signal lengths and originating from fetuses at various gestation age. Such dataset could be used for testing and objectively comparing different AI-based algorithms.
The results showed that most of the tested ANNs were effective in noise suppression in terms of objective and subjective evaluation, but they were limited by the computational complexity and the dependency of the filtration quality on the optimal settings of the algorithm parameters. Therefore, it would be beneficial in the future to focus on combining ANNs with modern nature-inspired optimization algorithms, which might help achieve more effective extraction in terms of accuracy and computational speed, and thus allow implementing these methods in devices operating in real-time. In the area of feature detection, the k-means and k-medoids algorithms were particularly effective, even for signals with lower SNR values. As for fPCG signals, it would be valuable to test these methods also for the purpose of detecting S\(_2\) sounds and pathological heart murmurs. When it comes to the area of fetal health classification, using SVM and random forest obtained the most promising results. For future research, it would be useful to test the fetal health state classification with fECG signals. Further research should also address less-explored areas, such as parallel processing, the use of AI-based algorithms to model synthetic signals or to select the most suitable input aECG signals to be used for processing and analysis.
Abbreviations
- ACC:
-
Accuracy
- ADALINE:
-
Adaptive linear neuron
- AE:
-
Autoencoder
- aECG:
-
Abdominal electrocardiography
- AI:
-
Artificial intelligence
- ANFIS:
-
Adaptive neuro-fuzzy inference system
- ANN:
-
Artificial neural network
- BMI:
-
Body mass index
- BP:
-
Back propagation
- CNN:
-
Convolutional neural network
- CTG:
-
Cardiotocography
- CWT:
-
Continuous wavelet transform
- DE:
-
Differential evolution
- EBBA:
-
Enhanced binary bat algorithm
- EFM:
-
Electronic fetal monitoring
- EKS:
-
Extended Kalman smoother
- EMD:
-
Empirical mode decomposition
- ES:
-
Evolution strategy
- ESN:
-
Echo state network
- FA:
-
Firefly algorithm
- fECG:
-
Fetal electrocardiography
- fHR:
-
Fetal heart rate
- fHS:
-
Fetal heart sound
- FIGO:
-
The International Federation of Gynaecology and Obstetrics
- fMCG:
-
Fetal magnetocardiography
- fPCG:
-
Fetal phonocardioraphy
- fQRS:
-
Fetal QRS
- FURIA:
-
Fuzzy unordered rule induction algorithm
- GA:
-
Genetic algorithm
- GLCM:
-
Grey-level co-occurrence matrix
- GWO:
-
Grey wolf optimizer
- HT:
-
Hilbert transform
- ICA:
-
Independent component analysis
- IMF:
-
Intrinsic mode function
- K-NN:
-
K-nearest neighbor
- LMS:
-
Least mean square
- LS-SVM:
-
Least squares singular value decomposition
- LSTM:
-
Long short-term memory
- mECG:
-
Maternal electrocardiography
- MFO:
-
Moth-flame optimization
- mHS:
-
Maternal heart sound
- ML:
-
Machine learning
- MLP:
-
Multilayer perceptron
- mQRS:
-
Maternal QRS
- MS:
-
Magnetometer system
- NI-fECG:
-
Non-invasive fetal electrocardiography
- NLMS:
-
Normalized least mean square
- NPV:
-
Negative predictive value
- PPA:
-
Positive predictive agreement
- PPV:
-
Positive predictive value
- PS:
-
Phonocardiographic sensor
- PSO:
-
Particle swarm optimization
- RLS:
-
Recursive least squares
- RNN:
-
Recurrent neural network
- SE:
-
Sensitivity
- SNR:
-
Signal-to-noise ratio
- SNR\(_{\text{imp}}\) :
-
Signal-to-noise ratio improvement
- SP:
-
Specificity
- STFT:
-
Short-time Fourier transform
- SVD:
-
Singular value decomposition
- SVM:
-
Support vector machines
- TS:
-
Toco sensor
- UT:
-
Ultrasound transducer
- WT:
-
Wavelet transform
References
Ayres-de-Campos D, Spong CY, Chandraharan E et al (2015) FIGO consensus guidelines on intrapartum fetal monitoring: cardiotocography. Int J Gynecol Obstet 131(1):13–24. https://doi.org/10.1016/j.ijgo.2015.06.020
Hutter D, Kingdom J, Jaeggi E (2010) Causes and mechanisms of intrauterine hypoxia and its impact on the fetal cardiovascular system: a review. Int J Pediatr 2010:1–9. https://doi.org/10.1155/2010/401323
Hanna IR, Silverman ME (2002) A history of cardiac auscultation and some of its contributors. Am J Cardiol 90(3):259–267. https://doi.org/10.1016/S0002-9149(02)02465-7
Kahankova R, Martinek R, Jaros R et al (2020) A review of signal processing techniques for non-invasive fetal electrocardiography. IEEE Rev Biomed Eng 13:51–73. https://doi.org/10.1109/RBME.2019.2938061
Sartwelle TP (2012) Electronic fetal monitoring: a bridge too far. J Leg Med 33(3):313–379. https://doi.org/10.1080/01947648.2012.714321
Pinas A, Chandraharan E (2016) Continuous cardiotocography during labour: analysis, classification and management. Best Pract Res Clin Obstet Gynaecol 30:33–47. https://doi.org/10.1016/j.bpobgyn.2015.03.022
Khangura T, Chandraharan E (2014) Electronic fetal heart rate monitoring: the future. Curr Women’s Health Rev 9(3):169–174. https://doi.org/10.2174/157340480903140131111807
Betran A, Torloni M, Zhang J et al (2016) WHO Statement on caesarean section rates. BJOG 123(5):667–670. https://doi.org/10.1111/1471-0528.13526
Boerma T, Ronsmans C, Melesse DY et al (2018) Global epidemiology of use of and disparities in caesarean sections. The Lancet 392(10155):1341–1348. https://doi.org/10.1016/S0140-6736(18)31928-7
Sandall J, Tribe RM, Avery L et al (2018) Short-term and long-term effects of caesarean section on the health of women and children. The Lancet 392(10155):1349–1357. https://doi.org/10.1016/S0140-6736(18)31930-5
Cömert Z, Şengür A, Budak Ü et al (2019) Prediction of intrapartum fetal hypoxia considering feature selection algorithms and machine learning models. Health Inf Sci Syst 7(1):17. https://doi.org/10.1007/s13755-019-0079-z
Tang H, Wang T, Li M et al (2018) The design and implementation of cardiotocography signals classification algorithm based on neural network. Comput Math Methods Med 2018:1–12. https://doi.org/10.1155/2018/8568617
Alsaggaf W, Cömert Z, Nour M et al (2020) Predicting fetal hypoxia using common spatial pattern and machine learning from cardiotocography signals. Appl Acoust 167:107429. https://doi.org/10.1016/j.apacoust.2020.107429
Alshebly Y, Nafea M (2020) Isolation of fetal ECG signals from abdominal ECG using wavelet analysis. IRBM 41(5):252–260. https://doi.org/10.1016/j.irbm.2019.12.002
Ziani S, El Hassouani Y (2020) Fetal electrocardiogram analysis based on LMS adaptive filtering and complex continuous wavelet 1-D. In: Farhaoui Y (ed) Big data and networks technologies, vol 81. Springer, Cham, p 360–366. https://doi.org/10.1007/978-3-030-23672-4_26
Ganguly A, Sharma M (2017) Detection of pathological heart murmurs by feature extraction of phonocardiogram signals. J Appl Adv Res. https://doi.org/10.21839/jaar.2017.v2i4.94
Strand S, Lutter W, Strasburger JF et al (2019) Low-cost fetal magnetocardiography: a comparison of superconducting quantum interference device and optically pumped magnetometers. J Am Heart Assoc. https://doi.org/10.1161/JAHA.119.013436
Martinek R, Kahankova R, Skukova H, et al (2016) Nonlinear adaptive signal processing improves the diagnostic quality of transabdominal fetal electrocardiography. In: Advanced biosignal processing and diagnostic methods. IntechOpen
Fotiadou E, Vullings R (2020) Multi-channel fetal ECG denoising with deep convolutional neural networks. Front Pediatr 8:508. https://doi.org/10.3389/fped.2020.00508
Fotiadou E, van Sloun RJG, van Laar JOEH et al (2021) A dilated inception CNN-LSTM network for fetal heart rate estimation. Physiol Meas 42(4):045007. https://doi.org/10.1088/1361-6579/abf7db
Kaleem AM, Kokate RD (2019) An efficient adaptive filter for fetal ECG extraction using neural network. J Intell Syst 28(4):589–600. https://doi.org/10.1515/jisys-2017-0031
Zhou Z, Huang K, Shen H, et al (2020) Morphology extraction of fetal electrocardiogram by slow-fast LSTM network. Preprint. https://doi.org/10.36227/techrxiv.12645878
Lai K, Twine N, O’Brien A, et al (2019) Artificial intelligence and machine learning in bioinformatics. In: Encyclopedia of Bioinformatics and Computational Biology. Elsevier, p 272–286. https://doi.org/10.1016/B978-0-12-809633-8.20325-7
Cohen WR, Hayes-Gill B (2014) Influence of maternal body mass index on accuracy and reliability of external fetal monitoring techniques. Acta Obstet Gynecol Scand 93(6):590–595. https://doi.org/10.1111/aogs.12387
Sameni R (2010) A review of fetal ECG signal processing issues and promising directions. Open Pacing Electrophysiol Ther J. https://doi.org/10.2174/1876536X01003010004
Neilson JP (2015) Fetal electrocardiogram (ECG) for fetal monitoring during labour. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD000116.pub5
Oudijk MA, Kwee A, Visser GH et al (2004) The effects of intrapartum hypoxia on the fetal QT interval. BJOG 111(7):656–660. https://doi.org/10.1111/j.1471-0528.2004.00178.x
Kazmi T, Radfer F, Khan S (2011) ST analysis of the fetal ECG, as an adjunct to fetal heart rate monitoring in labour: a review. Oman Med J 26(6):459–460. https://doi.org/10.5001/omj.2011.118
Euliano TY, Nguyen MT, Darmanjian S et al (2013) Monitoring uterine activity during labor: a comparison of 3 methods. Am J Obstet Gynecol 208(1):66.e1-66.e6. https://doi.org/10.1016/j.ajog.2012.10.873
Ibrahim EA, Al Awar S, Balayah ZH et al (2017) A comparative study on fetal heart rates estimated from fetal phonography and cardiotocography. Front Physiol 8:764. https://doi.org/10.3389/fphys.2017.00764
Abbas AK, Bassam R (2009) Phonocardiography signal processing. Synth Lect Biomed Eng 4(1):1–194. https://doi.org/10.2200/S00187ED1V01Y200904BME031
Chetlur Adithya P, Sankar R, Moreno WA et al (2017) Trends in fetal monitoring through phonocardiography: challenges and future directions. Biomed Signal Process Control 33:289–305. https://doi.org/10.1016/j.bspc.2016.11.007
Kovács F, Horváth C, Balogh ÁT et al (2011) Fetal phonocardiography–past and future possibilities. Comput Methods Programs Biomed 104(1):19–25. https://doi.org/10.1016/j.cmpb.2010.10.006
Kovács F, Török M, Horváth C et al (2010) A New, Phonocardiography-Based Telemetric Fetal Home Monitoring System. Telemedicine and e-Health 16(8):878–882. https://doi.org/10.1089/tmj.2010.0039
Quartero HWP, Stinstra JG, Golbach EGM et al (2002) Clinical implications of fetal magnetocardiography: clinical use of Fetal MCG. Ultrasound Obstet Gynecol 20(2):142–153. https://doi.org/10.1046/j.1469-0705.2002.00754.x
Grimm B, Haueisen J, Huotilainen M et al (2003) Recommended standards for fetal magnetocardiography. Pacing Clin Electrophysiol 26(11):2121–2126. https://doi.org/10.1046/j.1460-9592.2003.00330.x
Peters MJ, Stinstra JG, Uzunbajakau S, et al (2005) Fetal magnetocardiography. In: Lin JC (ed) Advances in electromagnetic fields in living systems, vol 4. Springer, New York, pp 1–40. https://doi.org/10.1007/0-387-24024-1_1
Matonia A, Jezewski J, Kupka T et al (2020) Fetal electrocardiograms, direct and abdominal with reference heartbeat annotations. Sci Data 7(1):200. https://doi.org/10.1038/s41597-020-0538-z
Ertel W (2017) Introduction to artificial intelligence. Undergraduate topics in computer science. Springer, Cham. https://doi.org/10.1007/978-3-319-58487-4
Alzubi J, Nayyar A, Kumar A (2018) Machine learning from theory to algorithms: an overview. J Phys 1142:012012. https://doi.org/10.1088/1742-6596/1142/1/012012
Rasheed K, Qayyum A, Qadir J et al (2021) Machine learning for predicting epileptic seizures using EEG signals: a review. IEEE Rev Biomed Eng 14:139–155. https://doi.org/10.1109/RBME.2020.3008792
Antonopoulos I, Robu V, Couraud B et al (2020) Artificial intelligence and machine learning approaches to energy demand-side response: a systematic review. Renew Sustain Energy Rev 130:109899. https://doi.org/10.1016/j.rser.2020.109899
Jacob SG, Ramani RG (2012) Evolving efficient classification rules from cardiotocography data through data mining methods and techniques. Eur J Sci Res 78(3):468–480
Snider D, Xiaowei Xu (2011) Mining fetal magnetocardiogram data for high-risk fetuses. In: 2011 IEEE international conference on bioinformatics and biomedicine workshops (BIBMW). IEEE, Atlanta, GA, pp 1066–1068. https://doi.org/10.1109/BIBMW.2011.6112563
Vican I, Kreković G, Jambrošić K (2021) Can empirical mode decomposition improve heartbeat detection in fetal phonocardiography signals? Comput Methods Programs Biomed 203:106038. https://doi.org/10.1016/j.cmpb.2021.106038
Avuçlu E, Abdullah E (2019) Classification of cardiotocography records with Naïve Bayes. Int Sci Voc Stud J 3(2):105–110
Álvarez P, Romero FJ, García A, et al (2017) Classification algorithms for fetal QRS extraction in abdominal ECG signals. In: Rojas I, Ortuño F (eds) Bioinformatics and biomedical engineering, vol 10208. Springer, Cham, pp 524–535. https://doi.org/10.1007/978-3-319-56148-6_47
Jiménez-González A, James CJ (2010) Time-structure based reconstruction of physiological independent sources extracted from noisy abdominal phonograms. IEEE Trans Biomed Eng 57(9):2322–2330. https://doi.org/10.1109/TBME.2010.2051226
Castillo E, Morales DP, García A et al (2018) A clustering-based method for single-channel fetal heart rate monitoring. PLoS ONE 13(6):e0199308. https://doi.org/10.1371/journal.pone.0199308
Mago VK, Bhatia N, Giannoccaro I (2012) Cross-disciplinary applications of artificial intelligence and pattern recognition: advancing technologies. Advances in computational intelligence and robotics. IGI Global. https://doi.org/10.4018/978-1-61350-429-1
Kahankova R, Martinek R, Mikolasova M, et al (2018) Adaptive linear neuron for fetal electrocardiogram extraction. In: 2018 IEEE 20th international conference on e-health networking, applications and services (Healthcom). IEEE, Ostrava, pp 1–5. https://doi.org/10.1109/HealthCom.2018.8531135
Sharkawy AN (2020) Principle of neural network and its main types: review. J Adv Appl Comput Math 7(1):8–19. https://doi.org/10.15377/2409-5761.2020.07.2
Lee JS, Seo M, Kim SW, et al (2018) Fetal QRS detection based on convolutional neural networks in noninvasive fetal electrocardiogram. In: 2018 4th International conference on frontiers of signal processing (ICFSP). IEEE, Poitiers, pp 75–78. https://doi.org/10.1109/ICFSP.2018.8552074
Yılmaz E (2016) Fetal state assessment from cardiotocogram data using artificial neural networks. J Med Biol Eng 36(6):820–832. https://doi.org/10.1007/s40846-016-0191-3
Assaleh K, Al-Nashash H (2005) A novel technique for the extraction of fetal ECG using polynomial networks. IEEE Trans Biomed Eng 52(6):1148–1152. https://doi.org/10.1109/TBME.2005.844046
Ayat M, Assaleh K, Al-Nashash H (2015) Extracting fetal ECG from a single maternal abdominal record. In: 2015 IEEE 8th GCC Conference & Exhibition. IEEE, Muscat, Oman, pp 1-4. https://doi.org/10.1109/IEEEGCC.2015.7060027
Jagannath D, Raveena Judie Dolly D, Dinesh Peter J (2020) Deep learning strategies for foetal electrocardiogram signal synthesis. Pattern Recogn Lett 136:286–292. https://doi.org/10.1016/j.patrec.2020.06.016
Assaleh K (2007) Extraction of fetal electrocardiogram using adaptive neuro-fuzzy inference systems. IEEE Trans Biomed Eng 54(1):59–68. https://doi.org/10.1109/TBME.2006.883728
Saranya S, Priyadharsini MS (2010) A novel hybrid soft computing technique for extracting fetal ECG from maternal ECG signal. Int J Comput Appl 3(8):7–13. https://doi.org/10.5120/751-1061
Skutova H, Martinek R, Jaros R et al (2018) A noise suppression technique for fetal phonocardiogram monitoring using adaptive neuro-fuzzy interference system. IFAC-PapersOnLine 51(6):456–461. https://doi.org/10.1016/j.ifacol.2018.07.103
Behar J, Johnson AE, Oster J, et al (2013) An echo state neural network for foetal ECG extraction optimised by random search. Proc Adv Neural Inf Process Syst pp 1–5
Behar J, Johnson A, Clifford GD et al (2014) A comparison of single channel fetal ECG extraction methods. Ann Biomed Eng 42(6):1340–1353. https://doi.org/10.1007/s10439-014-0993-9
Mendel JM (2000) Uncertainty, fuzzy logic, and signal processing. Signal Process 80(6):913–933. https://doi.org/10.1016/S0165-1684(00)00011-6
Singh H, Gupta MM, Meitzler T et al (2013) Real-life applications of fuzzy logic. Adv Fuzzy Syst 2013:1–3. https://doi.org/10.1155/2013/581879
Das S, Roy K, Saha CK (2015) Fuzzy membership estimation using ANN: a case study in CTG analysis. In: Satapathy SC, Biswal BN, Udgata SK, et al (eds) Proceedings of the 3rd International conference on frontiers of intelligent computing: theory and applications (FICTA) 2014, vol 327. Springer, Cham, p 221–228. https://doi.org/10.1007/978-3-319-11933-5_25
Chourasia VS, Tiwari AK, Gangopadhyay R (2014) Interval type-2 fuzzy logic based antenatal care system using phonocardiography. Appl Soft Comput 14:489–497. https://doi.org/10.1016/j.asoc.2013.08.016
Czabanski R, Jezewski M, Horoba K et al (2016) Fuzzy analysis of delivery outcome attributes for improving the automated fetal state assessment. Appl Artif Intell 30(6):556–571. https://doi.org/10.1080/08839514.2016.1193717
Jezewski M, Czabanski R, Leski JM et al (2021) On \(\epsilon \) -insensitive simplification of fuzzy rules for fetal distress assessment. Expert Syst Appl 179:115052. https://doi.org/10.1016/j.eswa.2021.115052
Vassiliadis V, Dounias G (2009) Nature-inspired Intelligence: a review of selected methods and applications. Int J Artif Intell Tools 18(04):487–516. https://doi.org/10.1142/S021821300900024X
Wang Z, Qin C, Wan B et al (2021) A comparative study of common nature-inspired algorithms for continuous function optimization. Entropy 23(7):874. https://doi.org/10.3390/e23070874
Adamopoulos A, Anninos P, Likothanassis S, et al (2002) Evolutionary self-adaptive multimodel prediction algorithms of the fetal magnetocardiogram. In: 2002 14th International conference on digital signal processing proceedings. DSP 2002 (Cat. No.02TH8628), vol 2. IEEE, Santorini, Greece, pp 1149–1152. https://doi.org/10.1109/ICDSP.2002.1028296
Ocak H (2013) A medical decision support system based on support vector machines and the genetic algorithm for the evaluation of fetal well-being. J Med Syst 37(2):9913. https://doi.org/10.1007/s10916-012-9913-4
Kockanat S, Kockanat S (2018) Analysis and extraction of fetal electrocardiogram signal with adaptive filtering using differential evolution algorithm. Cumhuriyet Sci J pp 294–302. https://doi.org/10.17776/csj.407424
Panigrahy D, Sahu PK (2017) Extraction of fetal ECG signal by an improved method using extended Kalman smoother framework from single channel abdominal ECG signal. Australas Phys Eng Sci Med 40(1):191–207. https://doi.org/10.1007/s13246-017-0527-5
Czabanski R, Jezewski M, Leski JM, et al (2020) Clustering with \(\epsilon \)-hyperballs based simplification of fuzzy rules to support the assessment of fetal state. In: 2020 IEEE 20th International conference on bioinformatics and bioengineering (BIBE). IEEE, Cincinnati, OH, USA, pp 358–364. https://doi.org/10.1109/BIBE50027.2020.00065
Anoop SSVKK, Prabhu CM, Penumala SK (2009) Detection of QRS complex of fetal ECG using biologically inspired soft-computing tools. In: 2009 Annual IEEE India conference. IEEE, Ahmedabad, India, pp 1–4. https://doi.org/10.1109/INDCON.2009.5409366
Nasiri M (2012) Fetal electrocardiogram signal extraction by ANFIS trained with PSO method. Int J Electr Comput Eng (IJECE) 2(2):247–260. https://doi.org/10.11591/ijece.v2i2.231
Subha V, Murugan D (2014) Foetal state determination using support vector machine and firefly optimisation. Int J Knowl Comput Syst 2(2):7–12
Jibia MS, Jibia AU (2021) Fetal electrocardiogram extraction using moth flame optimization (MFO)-based adaptive filter. Adv Sci Technol Eng Syst J 6(2):303–312. https://doi.org/10.25046/aj060235
Golzan SM, Hakimpour F, Toolou A (2009) Fetal ECG extraction using multi-layer perceptron neural networks with Bayesian approach. In: Magjarevic R, Nagel JH, Vander Sloten J et al (eds) 4th European conference of the international federation for medical and biological engineering, vol 22. Springer, Berlin, pp 311–317. https://doi.org/10.1007/978-3-540-89208-3_74
Lo FW, Tsai PY (2018) Deep learning for detection of fetal ECG from multi-channel abdominal leads. In: 2018 Asia-Pacific signal and information processing association annual summit and conference (APSIPA ASC). IEEE, Honolulu, HI, USA, pp 1397–1401. https://doi.org/10.23919/APSIPA.2018.8659503
Lukoševičius M, Marozas V (2014) Noninvasive fetal QRS detection using an echo state network and dynamic programming. Physiol Meas 35(8):1685–1697. https://doi.org/10.1088/0967-3334/35/7/1685
Septiyani F, Nuryani N, Nugroho AS (2019) Identification of fetal QRS with base of abdominal electrocardiogram using backpropagation artifical neural network. In: International conference on science and applied science (ICSAS) 2019, Surakarta, Indonesia, p 020099. https://doi.org/10.1063/1.5141712
Vo K, Le T, Rahmani AM et al (2020) An efficient and robust deep learning method with 1-D octave convolution to extract fetal electrocardiogram. Sensors 20(13):3757. https://doi.org/10.3390/s20133757
Zhong W, Liao L, Guo X et al (2018) A deep learning approach for fetal QRS complex detection. Physiol Meas 39(4):045004. https://doi.org/10.1088/1361-6579/aab297
Alsayyari A (2019) Fetal cardiotocography monitoring using Legendre neural networks. Biomed Eng / Biomedizinische Technik 64(6):669–675. https://doi.org/10.1515/bmt-2018-0074
Cömert Z, Kocamaz A (2017) A study of artificial neural network training algorithms for classification of cardiotocography signals. Bitlis Eren Univ J Sci Technol 7(2):93–103. https://doi.org/10.17678/beuscitech.338085
Nagendra V, Gude H, Sampath D, et al (2017) Evaluation of support vector machines and random forest classifiers in a real-time fetal monitoring system based on cardiotocography data. In: 2017 IEEE conference on computational intelligence in bioinformatics and computational biology (CIBCB). IEEE, Manchester, United Kingdom, pp 1–6. https://doi.org/10.1109/CIBCB.2017.8058546
Silwattananusarn T, Kanarkard W, Tuamsuk K (2016) Enhanced classification accuracy for cardiotocogram data with ensemble feature selection and classifier ensemble. J Comput Commun 04(04):20–35. https://doi.org/10.4236/jcc.2016.44003
Chourasia VS, Tiwari AK (2011) Fetal heart rate variability analysis from phonocardiographic recordings. J Mech Med Biol 11(05):1315–1331. https://doi.org/10.1142/S0219519411004174
Chourasia VS, Tiwari AK, Gangopadhyay R (2014) A novel approach for phonocardiographic signals processing to make possible fetal heart rate evaluations. Digit Signal Process 30:165–183. https://doi.org/10.1016/j.dsp.2014.03.009
Ghazdali A, Hakim A, Laghrib A et al (2015) A new method for the extraction of fetal ECG from the dependent abdominal signals using blind source separation and adaptive noise cancellation techniques. Theor Biol Med Model 12(1):25. https://doi.org/10.1186/s12976-015-0021-2
Ramli DA, Shiong YH, Hassan N (2020) Blind source separation (BSS) of mixed maternal and fetal electrocardiogram (ECG) signal: a comparative study. Procedia Comput Sci 176:582–591. https://doi.org/10.1016/j.procs.2020.08.060
Bin Queyam A, Kumar Pahuja S, Singh D (2017) Quantification of feto-maternal heart rate from abdominal ECG signal using empirical mode decomposition for heart rate variability analysis. Technologies 5(4):68. https://doi.org/10.3390/technologies5040068
Ghobadi Azbari P, Abdolghaffar M, Mohaqeqi S et al (2017) A novel approach to the extraction of fetal electrocardiogram based on empirical mode decomposition and correlation analysis. Australas Phys Eng Sci Med 40(3):565–574. https://doi.org/10.1007/s13246-017-0560-4
Swarnalath R, Prasad D (2010) A novel technique for extraction of FECG using multi stage adaptive filtering. J Appl Sci 10(4):319–324. https://doi.org/10.3923/jas.2010.319.324
Barnova K, Martinek R, Jaros R et al (2021) A novel algorithm based on ensemble empirical mode decomposition for non-invasive fetal ECG extraction. PLoS ONE 16(8):e0256154. https://doi.org/10.1371/journal.pone.0256154
Jagannath DJ, Raveena Judie Dolly D, Peter JD (2019) A novel Bayesian deep learning methodology for enhanced foetal cardiac signal mining. J Exp Theor Artif Intell 31(2):215–224. https://doi.org/10.1080/0952813X.2018.1544283
Zahorian SA, Zuckerwar AJ, Karnjanadecha M (2012) Dual transmission model and related spectral content of the fetal heart sounds. Comput Methods Programs Biomed 108(1):20–27. https://doi.org/10.1016/j.cmpb.2011.12.006
Gavrovska A, Slavkovic M, Reljin I, et al (2013) Application of wavelet and EMD-based denoising to phonocardiograms. In: International symposium on signals, circuits and systems ISSCS2013. IEEE, Iasi, Romania, pp 1–4. https://doi.org/10.1109/ISSCS.2013.6651264
Hasan MA, Reaz MBI, Ibrahimy MI (2011) Fetal electrocardiogram extraction and R-peak detection for fetal heart rate monitoring using artificial neural network and correlation. In: The 2011 International joint conference on neural networks. IEEE, San Jose, CA, USA, pp 15–20. https://doi.org/10.1109/IJCNN.2011.6033193
Haykin S, Widrow B (2003) Least-mean-square adaptive filters: Haykin/least-mean-square adaptive filters. Wiley, Hoboken. https://doi.org/10.1002/0471461288
Jo SE, Kim SW (2005) Consistent normalized least mean square filtering with noisy data matrix. IEEE Trans Signal Process 53(6):2112–2123. https://doi.org/10.1109/TSP.2005.847845
Paleologu C, Benesty J, Ciochina S (2008) A robust variable forgetting factor recursive least-squares algorithm for system identification. IEEE Signal Process Lett 15:597–600. https://doi.org/10.1109/LSP.2008.2001559
Kileel J, Trager M, Bruna J (2019) On the expressive power of deep polynomial neural networks. Adv Neural Inf Process Syst 32:10310–10319
Ahmadi M, Ayat M, Assaleh K, et al (2008) Fetal ECG signal enhancement using polynomial classifiers and wavelet denoising. In: 2008 Cairo international biomedical engineering conference. IEEE, Cairo, Egypt, pp 1–4. https://doi.org/10.1109/CIBEC.2008.4786095
Dhillon A, Verma GK (2020) Convolutional neural network: a review of models, methodologies and applications to object detection. Prog Artif Intell 9(2):85–112. https://doi.org/10.1007/s13748-019-00203-0
Zhao Z, Deng Y, Zhang Y et al (2019) DeepFHR: intelligent prediction of fetal Acidemia using fetal heart rate signals based on convolutional neural network. BMC Med Inform Decis Mak 19(1):286. https://doi.org/10.1186/s12911-019-1007-5
Almadani M, Hadjileontiadis L, Khandoker A (2023) One-dimensional W-NETR for non-invasive single channel fetal ECG extraction. IEEE J Biomed Health Inform 27(7):3198–3209. https://doi.org/10.1109/JBHI.2023.3266645
Ronneberger O, Fischer P, Brox T (2015) U-Net: convolutional networks for biomedical image segmentation. In: Navab N, Hornegger J, Wells WM, et al (eds) Medical image computing and computer-assisted intervention – MICCAI 2015, vol 9351. Springer, Cham, pp 234-241. https://doi.org/10.1007/978-3-319-24574-4_28
Hamarashid HK (2021) Modified Long Short-Term memory and Utilizing in Building sequential model. Int J Multidiscip Curr Res pp 1–5. https://doi.org/10.14741/ijmcr/v.9.3.2
Ghonchi H, Abolghasemi V (2022) A dual attention-based autoencoder model for fetal ECG extraction from abdominal signals. IEEE Sens J 22(23):22908–22918. https://doi.org/10.1109/JSEN.2022.3213586
Jeong DH, Jeong J (2020) In-ear EEG based attention state classification using echo state network. Brain Sci 10(6):321. https://doi.org/10.3390/brainsci10060321
Demuth HB, Beale MH, De Jess O et al (2014) Neural network design. Martin Hagan, Stillwater
Amin MS, Mamun M, Hashim FH et al (2011) Separation of fetal electrocardiography (ECG) from composite ECG using adaptive linear neural network for fetal monitoring. International Journal of Physical Sciences 6(24):5871–5876
Reaz M, Lee Sze Wei (2004) An approach of neural network based fetal ECG extraction. In: Proceedings. 6th international workshop on enterprise networking and computing in healthcare industry - Healthcom 2004 (IEEE Cat. No.04EX842). IEEE, Odawara, Japan, pp 57-60. https://doi.org/10.1109/HEALTH.2004.1324471
Ahmadieh H, Asl BM (2017) Fetal ECG extraction via Type-2 adaptive neuro-fuzzy inference systems. Comput Methods Programs Biomed 142:101–108. https://doi.org/10.1016/j.cmpb.2017.02.009
Emuoyibofarhe JO, Alamu FO, Opiarighodare DK, et al (2014) Extraction of fetal electrocardiogram using an adaptive neuro-fuzzy system. Extraction 4(1)
Elmansouri K, Latif R, Maoulainine F (2014) Improvement of fetal electrocardiogram extraction by application of fuzzy adaptive resonance theory to adaptive neural fuzzy system. Int J Innov Appl Stud 9(1):95
Swarnalath R, Prasad D (2010) Maternal ECG cancellation in abdominal signal using ANFIS and wavelets. J Appl Sci 10(11):868–877. https://doi.org/10.3923/jas.2010.868.877
Jothi S, Prabha K (2012) Fetal electrocardiogram extraction using adaptive neuro-fuzzy inference systems and undecimated wavelet transform. IETE J Res 58(6):469. https://doi.org/10.4103/0377-2063.106753
Hemajothi S, Prabha KH (2012) Fetal electrocardiogram extraction using let techniques. J Comput Sci 8(9):1547–1553. https://doi.org/10.3844/jcssp.2012.1547.1553
Kumar P, Prasad AS (2019) Fetus electrocardiogram by using neuro-fuzzy systems and remote sensing through OFDM. Int J Innov Technol Explor Eng 8(11S2):1–3. https://doi.org/10.35940/ijitee.K1001.09811S219
Al-Zaben A, Al-Smadi A (2006) Extraction of foetal ECG by combination of singular value decomposition and neuro-fuzzy inference system. Phys Med Biol 51(1):137–143. https://doi.org/10.1088/0031-9155/51/1/010
Yang XS (2020) Nature-inspired optimization algorithms: challenges and open problems. J Comput Sci 46:101104. https://doi.org/10.1016/j.jocs.2020.101104
Das S, Suganthan PN (2011) Differential evolution: a survey of the state-of-the-art. IEEE Trans Evol Comput 15(1):4–31. https://doi.org/10.1109/TEVC.2010.2059031
Wang D, Tan D, Liu L (2018) Particle swarm optimization algorithm: an overview. Soft Comput 22(2):387–408. https://doi.org/10.1007/s00500-016-2474-6
Panigrahy D, Rakshit M, Sahu P (2015) An efficient method for fetal ECG extraction from single channel abdominal ECG. In: 2015 International conference on industrial instrumentation and control (ICIC). IEEE, Pune, India, pp 1083–1088. https://doi.org/10.1109/IIC.2015.7150908
Mirjalili S (2015) Moth-flame optimization algorithm: a novel nature-inspired heuristic paradigm. Knowl-Based Syst 89:228–249. https://doi.org/10.1016/j.knosys.2015.07.006
Shehab M, Abualigah L, Al Hamad H et al (2020) Moth-flame optimization algorithm: variants and applications. Neural Comput Appl 32(14):9859–9884. https://doi.org/10.1007/s00521-019-04570-6
Cesarelli M, Ruffo M, Romano M et al (2012) Simulation of foetal phonocardiographic recordings for testing of FHR extraction algorithms. Comput Methods Programs Biomed 107(3):513–523. https://doi.org/10.1016/j.cmpb.2011.11.008
Jaba Deva Krupa A, Dhanalakshmi S, Lai KW et al (2022) An IoMT enabled deep learning framework for automatic detection of fetal QRS: a solution to remote prenatal care. J King Saud Univ 34(9):7200–7211. https://doi.org/10.1016/j.jksuci.2022.07.002
Madhulatha TS (2011) Comparison between K-means and K-medoids clustering algorithms. In: Wyld DC, Wozniak M, Chaki N, et al (eds) Advances in computing and information technology, vol 198. Springer, Berlin, pp 472–481. https://doi.org/10.1007/978-3-642-22555-0_48
Velmurugan T (2010) Computational Complexity between K-means and K-medoids clustering algorithms for normal and uniform distributions of data points. J Comput Sci 6(3):363–368. https://doi.org/10.3844/jcssp.2010.363.368
Kingsford C, Salzberg SL (2008) What are decision trees? Nat Biotechnol 26(9):1011–1013. https://doi.org/10.1038/nbt0908-1011
Rokach L, Maimon O (2005) Decision trees. In: Maimon O, Rokach L (eds) Data mining and knowledge discovery handbook. Springer, New York, p 165–192. https://doi.org/10.1007/0-387-25465-X_9
Fawagreh K, Gaber MM, Elyan E (2014) Random forests: From early developments to recent advancements. Syst Sci Control Eng 2(1):602–609. https://doi.org/10.1080/21642583.2014.956265
Sholapurkar SL (2013) Interpretation of British experts’ illustrations of fetal heart rate (FHR) decelerations by Consultant Obstetricians, registrars and midwives: a prospective study–reasons for major disagreement with experts and implications for clinical practice. Open J Obstet Gynecol 03(06):454–465. https://doi.org/10.4236/ojog.2013.36085
Knupp RJ, Andrews WW, Tita AT (2020) The future of electronic fetal monitoring. Best Pract Res Clin Obstet Gynaecol 67:44–52. https://doi.org/10.1016/j.bpobgyn.2020.02.004
Petrozziello A, Redman CWG, Papageorghiou AT et al (2019) Multimodal convolutional neural networks to detect fetal compromise during labor and delivery. IEEE Access 7:112026–112036. https://doi.org/10.1109/ACCESS.2019.2933368
Zhao Z, Zhang Y, Comert Z et al (2019) Computer-aided diagnosis system of fetal hypoxia incorporating recurrence plot with convolutional neural network. Front Physiol 10:255. https://doi.org/10.3389/fphys.2019.00255
Krupa N, Ma M, Zahedi E et al (2011) Antepartum fetal heart rate feature extraction and classification using empirical mode decomposition and support vector machine. Biomed Eng Online 10(1):6. https://doi.org/10.1186/1475-925X-10-6
Warrick PA, Hamilton EF, Kearney RE et al (2012) A machine learning approach to the detection of fetal hypoxia during labor and delivery. AI Mag 33(2):79. https://doi.org/10.1609/aimag.v33i2.2412
Frank A (2010) UCI machine learning repository. University of California, School of Information and Computer Science, Irvine, CA. http://archive.ics.uci.edu/ml
Yılmaz E, Kılıkçıer Ç (2013) Determination of fetal state from cardiotocogram using LS-SVM with particle swarm optimization and binary decision tree. Comput Math Methods Med 2013:1–8. https://doi.org/10.1155/2013/487179
Georgieva A, Payne SJ, Moulden M et al (2013) Artificial neural networks applied to fetal monitoring in labour. Neural Comput Appl 22(1):85–93. https://doi.org/10.1007/s00521-011-0743-y
Jezewski M, Wrobel J, Horoba K, et al (2007) The prediction of fetal outcome by applying neural network for evaluation of CTG records. In: Kacprzyk J, Kurzynski M, Puchala E, et al (eds) Computer recognition systems 2, vol 45. Springer, Berlin, pp 532–541. https://doi.org/10.1007/978-3-540-75175-5_67
Lunghi F, Magenes G, Pedrinazzi L, et al (2005) Detection of fetal distress though a support vector machine based on fetal heart rate parameters. In: Computers in cardiology, 2005. IEEE, Lyon, France, pp 247–250. https://doi.org/10.1109/CIC.2005.1588083
Cömert Z, Kocamaz AF (2016) A study based on gray level co-occurrence matrix and neural network community for determination of hypoxic fetuses. In: International artificial intelligence and data processing symposium (IDAP), pp 569–573
Subasi A, Kadasa B, Kremic E (2020) Classification of the cardiotocogram data for anticipation of fetal risks using bagging ensemble classifier. Procedia Comput Sci 168:34–39. https://doi.org/10.1016/j.procs.2020.02.248
Khosrow-Pour, D.B.A. M (ed) (2015) Encyclopedia of information science and technology, 3rd Edition. IGI Global, Hershey https://doi.org/10.4018/978-1-4666-5888-2
Wilson D, Martinez T (2001) The need for small learning rates on large problems. In: IJCNN’01. International joint conference on neural networks. Proceedings (Cat. No.01CH37222), vol 1. IEEE, Washington, DC, USA, pp 115–119. https://doi.org/10.1109/IJCNN.2001.939002
Noguchi Y, Matsumoto F, Maeda K et al (2009) Neural network analysis and evaluation of the fetal heart rate. Algorithms 2(1):19–30. https://doi.org/10.3390/a2010019
Lu PX (2014) Research on BP neural network algorithm based on Quasi-Newton method. Appl Mech Mater 686:388–394. https://doi.org/10.4028/www.scientific.net/AMM.686.388
Mall S, Chakraverty S (2016) Application of Legendre Neural Network for solving ordinary differential equations. Appl Soft Comput 43:347–356. https://doi.org/10.1016/j.asoc.2015.10.069
Suthaharan S (2016) Support vector machine, vol 36, Springer, Boston, pp 207–235. https://doi.org/10.1007/978-1-4899-7641-3_9
Ricciardi C, Amato F, Tedesco A et al (2023) Detection of suspicious cardiotocographic recordings by means of a machine learning classifier. Bioengineering 10(2):252. https://doi.org/10.3390/bioengineering10020252
Rish I (2001) An empirical study of the naive Bayes classifier. In: IJCAI 2001 workshop on empirical methods in artificial intelligence, pp 41–46
Sharma S, Agrawal J, Sharma S (2013) Classification through machine learning technique: C4. 5 algorithm based on various entropies. Int J Comput Appl 82(16):28–32. https://doi.org/10.5120/14249-2444
Sharma P, Sharma K (2022) Fetal state health monitoring using novel Enhanced Binary Bat Algorithm. Comput Electr Eng 101:108035. https://doi.org/10.1016/j.compeleceng.2022.108035
Amo A, Montero J, Biging G et al (2004) Fuzzy classification systems. Eur J Oper Res 156(2):495–507. https://doi.org/10.1016/S0377-2217(03)00002-X
Jain R, Abraham A (2004) A comparative study of fuzzy classification methods on breast cancer data. Australas Phys Eng Sci Med 27(4):213–218. https://doi.org/10.1007/BF03178651
Hühn J, Hüllermeier E (2009) FURIA: an algorithm for unordered fuzzy rule induction. Data Min Knowl Disc 19(3):293–319. https://doi.org/10.1007/s10618-009-0131-8
Das S, Roy K, Saha CK (2013) Application of FURIA in the classification of cardiotocograph. In: IEEE-international conference on research and development prospects on engineering and technology, pp 120–124
Jezewski J, Matonia A, Kupka T et al (2012) Determination of fetal heart rate from abdominal signals: evaluation of beat-to-beat accuracy in relation to the direct fetal electrocardiogram. Biomedizinische Technik/Biomed Eng. https://doi.org/10.1515/bmt-2011-0130
De Moor B, De Gersem P, De Schutter B et al (1997) DAISY: A database for identification of systems. JOURNAL A 38:4–5
Goldberger AL, Amaral LAN, Glass L et al (2000) PhysioBank, PhysioToolkit, and PhysioNet: components of a new research resource for complex physiologic signals. Circulation. https://doi.org/10.1161/01.CIR.101.23.e215
Clifford GD, Silva I, Behar J et al (2014) Non-invasive fetal ECG analysis. Physiol Meas 35(8):1521–1536. https://doi.org/10.1088/0967-3334/35/8/1521
Andreotti F, Behar J, Zaunseder S et al (2016) An open-source framework for stress-testing non-invasive foetal ECG extraction algorithms. Physiol Meas 37(5):627–648. https://doi.org/10.1088/0967-3334/37/5/627
Mirjalili S, Mirjalili SM, Lewis A (2014) Grey wolf optimizer. Adv Eng Softw 69:46–61. https://doi.org/10.1016/j.advengsoft.2013.12.007
Mirjalili S, Lewis A (2016) The whale optimization algorithm. Adv Eng Softw 95:51–67. https://doi.org/10.1016/j.advengsoft.2016.01.008
Cheng X, Li J, Zheng C et al (2021) An improved PSO-GWO algorithm with chaos and adaptive inertial weight for robot path planning. Front Neurorobot 15:770361. https://doi.org/10.3389/fnbot.2021.770361
Liu Y, Wang L, Zhao L, et al (eds) (2020) Advances in natural computation, fuzzy systems and knowledge discovery. Volume 1. No. 1074 in Advances in intelligent systems and computing. Springer, Cham
Cai Z, Zhu Y (2021) A hybrid CNN-LSTM network for hand gesture recognition with surface EMG signals. In: Jiang X, Fujita H (eds) Thirteenth international conference on digital image processing (ICDIP 2021). SPIE, Singapore, p 74. https://doi.org/10.1117/12.2601074
Koutsiana E, Hadjileontiadis LJ, Chouvarda I et al (2017) Fetal heart sounds detection using wavelet transform and fractal dimension. Front Bioeng Biotechnol 5:49. https://doi.org/10.3389/fbioe.2017.00049
Balogh AT (2012) Analysis of the heart sounds and murmurs of fetuses and preterm infants. PhD thesis, Pazmany Peter Catholic University, Budapest
Kovács F, Kersner N, Kádár K et al (2009) Computer method for perinatal screening of cardiac murmur using fetal phonocardiography. Comput Biol Med 39(12):1130–1136. https://doi.org/10.1016/j.compbiomed.2009.10.001
Vullings R (2010) Non-invasive fetal electrocardiogram: analysis and interpretation. Citeseer
Taylor MJ, Smith MJ, Thomas M et al (2003) Non-invasive fetal electrocardiography in singleton and multiple pregnancies. BJOG 110(7):668–678. https://doi.org/10.1046/j.1471-0528.2003.02005.x
Chudacek V, Spilka J, Bursa M et al (2014) Open access intrapartum CTG database. BMC Pregnancy Childbirth 14(1):16. https://doi.org/10.1186/1471-2393-14-16
Yang J, Singh H, Hines EL et al (2012) Channel selection and classification of electroencephalogram signals: an artificial neural network and genetic algorithm-based approach. Artif Intell Med 55(2):117–126. https://doi.org/10.1016/j.artmed.2012.02.001
Baldazzi G, Sulas E, Vullings R et al (2023) Automatic signal quality assessment of raw trans-abdominal biopotential recordings for non-invasive fetal electrocardiography. Front Bioeng Biotechnol 11:1059119. https://doi.org/10.3389/fbioe.2023.1059119
Hazra D, Byun YC (2020) SynSigGAN: generative adversarial networks for synthetic biomedical signal generation. Biology 9(12):441. https://doi.org/10.3390/biology9120441
Liu J, Liang X, Ruan W et al (2021) High-performance medical data processing technology based on distributed parallel machine learning algorithm. J Supercomput. https://doi.org/10.1007/s11227-021-04060-4
Acknowledgements
This article was supported by the Ministry of Education of the Czech Republic (Project No. SP2024/059). This work was partially funded by project no. FW03010392: The comprehensive system for the development of non-invasive fetal ECG monitoring. This work was also partially funded by project no. FW06010498: MR Relaxometry of Basal Ganglia Damage in Newborns With Hypoxic-Ischemic Encephalopathy.
Funding
Open access publishing supported by the National Technical Library in Prague.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Confict of interest
The authors declare that they have no confict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Barnova, K., Martinek, R., Vilimkova Kahankova, R. et al. Artificial Intelligence and Machine Learning in Electronic Fetal Monitoring. Arch Computat Methods Eng (2024). https://doi.org/10.1007/s11831-023-10055-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11831-023-10055-6