
Abstract
Background
This cross-sectional and longitudinal study of breast cancer survivors (BCSs) examines the associations between arm/shoulder problems (ASPs), which consist of pain, restricted mobility and lymphedema, and different aspects of quality of life (QoL).
Methods
BCSs who had breast surgery, axillary lymph node dissection and radiotherapy (n = 255) were examined in 2004 (mean 4.1 years post-surgery) and a sub-sample (n = 187) was re-examined in 2007. ASPs was rated clinically in 2004 and by self-report (EORTC BR23) in 2004 and 2007. QoL was self-reported with The Short Form-36 (SF-36) and The Impact of Cancer scale (IOC).
Results
In 2004 BCSs with ASPs showed significantly poorer mean scores in most SF-36 domains compared to those without. No group differences were observed for positive IOC domains, while BCSs with ASPs showed significantly poorer mean scores in the negative ones. BCSs with clinically defined movement restriction showed significantly poorer SF-36 and negative IOC mean scores than those with clinically defined lymphedema. The longitudinal sub-study of self-rated pain, restricted mobility and lymphedema showed significant changes over time only for negative IOC domains in the pain group. Self-rated restricted mobility and lymphedema were significantly associated with most SF-36 domains both in 2004 and 2007, while few were associated with pain. Self-rated pain and restricted mobility showed significant associations with negative IOC domains.
Implications for cancer survivors
Not only lymphedema, but pain and restricted mobility in the arm/shoulder are significantly associated with poor QoL in BCSs at long-term. These problems should be diagnosed and treated in order to improve QoL.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Arm/shoulder problems (ASPs), defined as restricted shoulder mobility, lymphedema, and/or arm/shoulder pain are common in breast cancer survivors (BCSs). At the 5 year follow-up the prevalence of arm/shoulder pain is 30–40%, of lymphedema 10–15%, and of restricted arm/shoulder mobility is 15–30% among BCSs who had axillary lymph node dissection [1–5].
An extensive review of QoL in BCSs by Montazeri [6] found that although ASPs were among the most common adverse effects, most studies focused on the relation between lymphedema and QoL, rather than on restricted mobility and pain or ASPs in general. One study from 2003 of long-term ASPs following axillary node dissection, found ASPs to be the most important source of poor QoL in BCSs [7]. Later studies on physical and mental QoL have found that ASPs contribute significantly to poor QoL [1, 8], but most studies concern lymphedema [9, 10]. However, one of these studies demonstrated that BCSs with other arm problems other than lymphedema had reduction in scores of mental health that were not observed in BCSs with lymphedema [1].
Since Bentzen et al. [11] found that 90% of post-radiotherapy effects in the arm/shoulder tissues occurred during the first 3.9 years post-treatment, the maximum effects of ASPs should be seen approximately 4 years after radiotherapy. Further, in order to catch the full effects on QoL, use of more than one QoL instrument has been recommended [12]. Therefore in this study we examined BCSs treated for stage II–III disease at a mean of 4 and 7 years after diagnosis using both the SF-36 and the Impact of Cancer scale (IOC). While the SF-36 is a well-established generic QoL instrument, the IOC is a recently introduced scale developed by Ganz et al. intended to specifically “assess a range of problems, issues and changes that long-term survivors ascribe to their cancer experience” [13]. The IOC was considered an instrument with good specific qualities for long-term cancer survivors according to Pearce et al. [14]. Both QoL instruments were used to examine associations between ASPs and QoL in this study.
Our BCSs sample was examined both clinically and by questionnaire in 2004, and a sub-sample was re-examined with questionnaire in 2007. Since most QoL studies of BCSs had focused on lymphedema, we also wanted to study the associations of restricted arm/shoulder mobility and arm/shoulder pain as well as lymphedema with QoL. Restricted mobility and lymphedema were rated by clinical examination in 2004. Arm/shoulder pain, restricted mobility and lymphedema were also self-rated in both 2004 and 2007, which gave us an opportunity for a longitudinal sub-study.
Our study therefore had three aims: 1) To study the associations between ASPs and QoL domains cross-sectionally 4 years post-surgery (2004 sample). 2) To compare associations between restricted shoulder mobility versus lymphedema and QoL (2004 sample). 3) To study longitudinal changes in self-rated ASPs scores and QoL and to compare their associations in 2004 and 2007.
Methods
Patient sampling
BCSs treated for stage II breast cancer between 1998 and 2002 at The Norwegian Radium Hospital (NRH), were invited to take part in a follow-up survey in 2004/2005. The survey consisted of a mailed questionnaire and an outpatient clinical examination. The inclusion criterias were: 1) Curatively intended surgery, followed by loco-regional radiotherapy; 2) No evidence of relapse since primary treatment; 3) No other malignant diagnosis; 4) Age ≤75 years at survey.
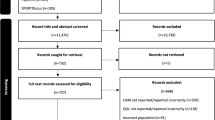
Among the 415 BCSs fulfilling the inclusion criteria, 23 (6%) declined to participate, and 43 (10%) did not respond, resulting in 349 BCSs (84%) returning questionnaires in 2004. Among them 318 (91%) also had the outpatient examination. Fifty-five (17%) BCSs with primary inoperable cT3-cT4 tumours, who received neo-adjuvant chemotherapy, were excluded in order to obtain a homogenously treated sample of BCSs. Thus, all included BCSs had pT1-pT2 tumours and axillary lymph node metastases. However, eight patients were omitted due to incomplete questionnaires, resulting in a 2004 sample of 255 BCSs. Among these, 195 women also took part in the 2007 follow-up survey (2007 longitudinal sample). A flowchart of the study is shown in Fig. 1.

Flowchart of the sample of the study
Treatment modalities
Treatment was based on the guidelines of the Norwegian Breast Cancer Group (www.nbcg.no). All BCSs had either modified radical mastectomy or lumpectomy, and all had axillary lymph node dissection at level I–II. The target volume of radiotherapy included the breast after lumpectomy, and the chest wall after mastectomy. All BCSs had adjuvant radiotherapy to the regional lymph nodes, with 50 Gy in 25 fractions. From October 1999, patients who had removed ≥ 10 axillary nodes without perinodal infiltration had irradiation only to the axillary apex, as opposed to those with <10 nodes removed and those having radiotherapy before that time, who had radiotherapy to the entire axilla. Post-operative adjuvant chemotherapy with CMF or FEC and/or tamoxifen was given according to the patient’s age and the hormone receptor status of the tumour [15].
Measures
Demographic variables
Information on socio-demographic variables was obtained from the questionnaire and the medical records. Relationship status was dichotomized as paired (married/cohabiting) and non-paired (single/separated/divorced/widow) and level of education into ≤ 12 years or >12 years of basic education. Employment status was categorized as employed (full or part-time jobs or students), and not employed.
Cancer-related variables and BMI
Information on the type of breast cancer and its treatment was obtained from the medical records. Weight and height was collected at the 2004 survey, and the body mass index (BMI) was calculated as kg/m2.
Clinical assessments of shoulder mobility and lymphedema in 2004
At the clinical examination arm/shoulder mobility was assessed by two experienced physiotherapists. Goniometer-based measurements of flexion (forward elevation of the arm) and abduction (lateral elevation of the arm) were done on both arms. Based on clinical experience, a reduced range of motion of ≥ 25° difference between the operated side and the other was defined as impaired shoulder mobility either for flexion, abduction or both (n = 85).
Lymphedema was assessed by volumetric calculation using five circumferential measurements on both arms [16]. Lymphedema was defined as either: 1) a difference of ≥ 10% in volume between the operated side and the other; or 2) For BCSs with either current use of compression garment or received treatment for lymphedema and ≥ 2 cm increase of any circumference of the operated arm versus the other arm (n = 43).
Self-rating of ASPs in 2004
Self-rating was done by Kwan’s arm problem scale (KAPS) [8]. The KAPS consists of the Problem subscale rating arm/shoulder symptoms including pain, swelling, stiffness, use, and numbness, and the ADL subscale rating impairment in dressing and other daily activities. All 13 KAPS items were rated on five point Likert scales from 1 (no symptom or same as before) to 5 (severe symptom or unable to perform), and the KAPS score was the sum score of the items. The KAPS has shown good psychometric properties in our sample of BCSs [17]. Clinically significant self-rated ASPs were defined by a KAPS score of ≥ 21.5 [17], and that was present in 121 BCSs in 2004.
Definition of ASPs present (+) or absent (−) in 2004
We used the findings on the clinical assessment and the self-rated KAPS scores in 2004 to define two groups regarding ASPs in both the 2004 and 2007 samples. The ASPs+ (present) group fulfilled at least two of three criteria: 1) having impaired shoulder mobility; 2) having lymphedema; or 3) KAPS score ≥ 21.5. The ASP- (absent) group fulfilled one or none of these criteria.
Definition of self-rated ASPs in the longitudinal substudy (2004–7)
Since BCSs had filled in the EORTC QLQ-BR23 (BR23) a specific breast cancer module of QoL in both 2004 and 2007 [18], the ASPs questions of the BR23 was used for the longitudinal study of ASPs in relation to QoL domains over time. These questions were: During the past week: “Did you have pain in your arm or shoulder?”; “Did you have a swollen arm or hand?” and “Was it difficult to raise your arm or to move it sideways?” The items were rated on a four point Likert scale with the categories ‘not at all’ = 1, ‘a little’ = 2, ‘quite a bit’ = 3 and ‘very much’ = 4, which were used both as continuous measures and dichotomized as BR23-defined arm/shoulder pain, restricted mobility, and lymphedema present (quite a bit/very much) or absent (not at all/a little) [18].
The IOC version 1 (IOCv1)
The IOCv1 is a specific QoL instrument for long-term cancer survivors [13]. The IOCv1 covers six domains with 10 dimensional subscales, five positive (+) and five negative (−). The Physical Domain includes Health Awareness (+) and Body Changes (−). The Psychological Domain concerns Positive Self-evaluation (+) and Negative Self-evaluation (−). The Spiritual/Existential Domain covers Positive Life Outlook (+) and Negative Life Outlook (−). The Social Domain consists of Life Interference (−) and Values of Relationships (+). Meaning of Cancer (+) and Health Worries (−) are separate domains (10). All 41 IOC items are scored by five response categories: 1 (strongly disagree), 2 (disagree), 3 (neutral), 4 (agree) and 5 (strongly agree). The mean dimension score is calculated by summation of the dimensional item scores divided by the number of items, and mean scores <3 implies disagreement and >3 means agreement on the domains [13].
Ganz approved the use of the IOCv1 by our group. The translation of the IOC into Norwegian was made by professional translators with forward and backward translations. In the current study the Cronbach’s coefficient alphas were ≥0.75 for the positive domains and ≥0.85 for the negative ones.
The SF-36
The SF-36 is a generic QoL measure in common international use with well-documented psychometric properties and with normative data of the Norwegian general population [19]. The items are combined into four physical domain scales: Physical functioning, Physical role functioning, Bodily pain, General health, summarized as the Physical Component Summary Scale (PCS); and four mental domain scales: Vitality, Social functioning, Emotional role functioning and Mental health summarized as the Mental Component Summary Scale (MCS). The PCS and MCS are T-transformed so that the Norwegian general population mean scores were 50 [20].
Statistical analysis
Continuous variables were analyzed with t-tests and categorical variables with chi-square tests. In case of skewed distributions, non-parametric tests were applied. Statistically significant differences in continuous and 2 × 2 contingency tables were tested for clinical significance using effect sizes (ESs). For continuous variables we used Cohen’s coefficient d, and for 2 × 2 contingency tables we used differences between arcsine transformed proportions. ES values ≥ 0.40 were considered as clinically significant based on the recommendations of Cohen [21–23]. Changes of the BR-23 defined ASPs scores from 2004 to 2007 were tested with paired sample t-tests. Correlations were calculated with Spearman’s coefficient rho. Internal consistencies of scales and subscales were examined by Cronbach’s coefficient alpha.
Bivariate and multivariate logistic regression analyses were used to explore associations between demographic, cancer-related variables, and the SF-36 and IOCv1 domain scores as independent variables, and ASPs groups in 2004 and BR-23 defined arm/shoulder pain, restricted mobility, and lymphedema in 2004 and 2007 as dependent variables. The strength of the associations was expressed as odds ratios (OR) with 95% confidence intervals (95%CI). The analyses were done on SPSS for Windows, version 16.0. The level of significance was set at p < 0.01 due to multiple comparisons, and all tests were two-sided.
Ethical considerations
The study was approved by the Regional Ethical Committee of Health Region South of Norway and by the National Data Inspectorate. All patients gave written informed consent.
Results
Socio-demographic and cancer-related findings (2004 sample)
Of the 255 tumour-free BCSs included, 80 (31%, 95%CI 26–37%) BCSs belonged to the ASP+ group and 175 (69%, 95%CI 63–74%) belonged to the ASP-group.
The following comparisons between the ASP+ and ASP-groups showed statistical significance: ASP+ had longer follow-up time, lower proportion of employed BCSs, and higher proportions with mastectomy and radiotherapy to the entire axilla (Table 1). The differences in follow-up time and type of surgery were clinically significant, while extent of radiotherapy came close (ES = 0.39). None of the other socio-demographic or cancer-related variables showed significant intergroup differences (Table 1).
ASP groups and QoL (2004 sample)
Compared to the ASP- group, the ASP+ group had significantly poorer scores in all physical and mental domains of the SF-36, except for MCS (Table 2). All statistically significant differences were also clinically significant.
No significant differences were found between the two ASP groups on the positive IOC domains. However, all the negative IOCv1 domains, except Health Worry, showed significantly higher agreement scores in the ASP+ compared to the ASP- group. All these differences were clinically significant (Table 2).
We did a multivariate logistic regression analyses with the significant socio-demographic and cancer–related variables (Table 1). The SF-36 Bodily pain and Role emotional and the IOCv1 of Body changes (highest ES for physical, mental and negative domains, respectively) were the independent variables and ASP group was the dependent variable. Only Bodily pain and Body changes showed significant associations with the ASP+ group (data not shown)
Clinically rated restricted mobility versus lymphedema and QoL (2004 sample)
Based on the clinical assessments 85 out of 255 BCSs (33%) had restricted mobility and 43 (17%) had lymphedema. In bivariate logistic regression analyses all the SF-36 domains except Social functioning, Mental health and MCS were significantly associated with restricted arm/shoulder mobility, while none were significantly associated with lymphedema based on clinical examinations (Table 3). No significant associations were detected between the positive IOCv1 domains and reduced mobility or lymphedema. As to negative IOCv1 domains, Life interference was significantly associated with both reduced mobility and lymphedema, while Body changes was significantly associated only with reduced mobility.
Longitudinal study findings 2004–2007
Of the 255 BCSs participating in 2004, 187 (73%) delivered valid ratings both in 2004 and 2007. BR23 defined arm/shoulder pain was present in 71 of these BCSs (38%) in 2004 and 66 (35%) in 2007. Correspondingly, 30 BCSs (16%) had self-rated restricted mobility in 2004 and 29 (16%) in 2007, while lymphedema was reported by 40 (21%) in 2004 and by 42 (22%) in 2007. The correlation coefficients (rho) for the raw scores were: pain versus swelling 0.50, pain versus movement 0.64, and swelling versus movement 0.43 in the 2004 sample. The correlation between clinically assessed and self-rated BR23 restricted mobility was 0.46 and for BR23 lymphedema 0.43 in the 2004 sample.
Bivariate logistic regression analyses showed that BR23 restricted arm/shoulder mobility was most often associated with the SF-36 domains, although BR23 lymphedema showed nearly as many significant associations both in 2004 and 2007 (Table 4). The BR23 arm/shoulder pain showed much fewer significant associations with the SF-36 domains, and they all belonged to the 2007 ratings. Comparisons of the SF-36 domain mean scores in 2004 and 2007 showed no significant differences neither for pain, mobility nor lymphedema.
Bivariate logistic regression analyses showed that neither BR23 pain, nor restricted mobility or lymphedema showed any significant associations with any of the positive IOCv1 domains (Table 5). BR23 arm/shoulder pain was significantly associated with all negative IOCv1 domains both in 2004 and 2007. BR23 restricted mobility also showed many significant associations with the negative IOCv1 domains particularly in 2004. In contrast, BR23 lymphedema showed few such associations.
For BCSs reporting BR23 arm/shoulder pain, the IOCv1 domains of Negative outlook, Life interferences and Health worry showed significant improvement from 2004 to 2007. No such changes over time were observed for any of the IOCv1 negative domains in the BR23 reduced mobility or lymphedema groups (Table 5).
Discussion
In relation to our aims we found: 1) Studied cross-sectionally, BCSs with clinically defined ASPs (2004) showed significantly poorer QoL on all SF-36 domains, except MCS, than BCSs without ASPs. No significant intergroup differences were observed for the positive IOCv1 domains, while all the negative IOCv1 domains, except Health Worry, had significantly higher scores in the ASP+ group (Table 2). 2) BCSs with clinically assessed restricted mobility showed significant associations with all SF-36 domains except MCS and no significant associations for lymphedema. Neither restricted mobility nor lymphedema showed significant associations with positive IOCv1 domains, but both showed significant associations with the negative IOCv1 domain of Life interference (Table 3). 3) The longitudinal study of self-rated ASPs showed that BR23 restricted mobility and lymphedema were significantly associated with most SF-36 domains both in 2004 and 2007, while pain was not (Table 4). Longitudinally there were no significant changes in the SF-36 domain scores in any of the three ASPs measures. As for the IOCv1 domain scores, BR23 pain and restricted mobility showed significant associations with the negative domains, while lymphedema hardly did so. Only the BR23 pain group showed significant improvement over time in some of the negative IOCv1 domains (Table 5).
Our results where BCSs with other self-reported arm symptoms than lymphedema had significantly poorer QoL in more domains of IOCv1, complement the findings of Ahmed et al. reporting similar findings using SF-36 [1]. We were also in agreement with Ahmed et al. [1] who reported that self-reported ASPs were associated with low QoL 8 years after diagnosis. Among the SF-36 domains with the lowest scores in 2004 were Role physical and Vitality and PCS all of which were significantly associated with restricted mobility. This indicates that BCSs with such impairment, more than with lymphedema, have problems in daily activities and poorer emotional well-being. This is also confirmed by the stronger associations with Body changes and Life interferences observed on the IOCv1 scale.
Generally, the mean QoL scores did not change significantly from 2004 to 2007. This finding indicates that the QoL of BCSs seems firmly established at a mean of 4 years since diagnosis. The exception is the score reduction in three negative IOCv1 domains in BCSs with self-rated arm/shoulder pain, which may be due to response shift of the patients’ ability to adapt to their limitations over time [24]. Our findings are in contrast to those of Engel et al. who found a reduction of self-reported arm problems from year 1 to 5 after diagnosis, which indicated that QoL changes were more common in the first years after diagnosis [7].
Our findings of strong associations between restricted mobility and several QoL domains as opposed to findings in lymphedema, complement findings of Thomas-Maclean et al. [25] reporting disability related to shoulder dysfunctions. Studies of lymphedema have mainly compared QoL in BCSs with and without lymphedema or with normative data [10]. An interesting finding in this regard is the weak associations between clinically rated lymphedema and the SF-36 domains, but the strong associations with self-rated lymphedema. Perhaps the moderate correlation of 0.43 (18.5% explained variance) between the two measures of lymphedema could explain this divergence. Another explanation could be that self-rating of both lymphedema and QoL leads to higher concordance than when lymphedema is rated clinically by physiotherapists. Smoot et al. [26], in a study of BCSs found low correlations between objective and self-reported measures of physical impairments such as range of movement and functional activities. The same observations are reported in other studies, with higher incidence and severity of arm/shoulder symptoms in self-reported ASPs compared to clinical evaluation [27].
It is well known that pain has a strong influence on both physical and mental QoL in BCSs [4]. Lauridsen et al. reported that BCSs with impaired shoulder mobility had significantly higher frequency of pain in shoulder, arm or neck compared to BCSs with normal shoulder function [28]. Although not an aim in our study, we confirmed these results on the self-rated data both in 2004 and 2007, but we also found such differences at both time points in BCSs with self-rated lymphedema.
A recent review, studying the consequences of axillary dissection and radiotherapy, showed more shoulder morbidity after these treatment modalities than in patients who did not receive them [29]. This conclusion was supported by both Peuckman et al. [4] and Hopwood et al. [30] who reported associations between radiotherapy and arm/shoulder pain. BCSs with the longest follow-up time had more frequently mastectomy and radiotherapy to the entire axilla. This may explain the association between increasing follow-up time and presence of ASPs observed in 2004. However, in our study there were few significant differences in the mean QoL domain scores from 4 to 7 years post-surgery, indicating established stability of QoL.
New treatment modalities for breast cancer have been introduced during the last decade, and the incidence of ASPs is decreasing [31]. Significantly lower proportions of severe lymphedema were found after breast conserving surgery compared to radical modified mastectomy [32, 33]. Further, the ALMANAC trial reported less lymphedema, but no significant difference in impaired shoulder mobility, 12 months after sentinel node biopsy compared to axillary dissection [34]. Other studies have reported similar results [35].
After surgery about 90% of BCSs in our 2004 sample had received information about lymphedema including clinical manifestations and treatment opportunities. Ahmed et al. [1] found that the information about lymphedema was insufficient, but lymphedema still received treatment priority compared to other arm/shoulder problems. Interestingly, in that study BCSs with other arm/shoulder problems showed more mental distress than BCSs with lymphedema.
However, we did not find significant associations of BCSs with clinically reduced mobility and lymphedema and SF-36 Mental health, but on self-rating such an association was observed in 2004 but not in 2007.
Our results have to be considered in the light of some limitations. One is that the Norwegian health care system gives treatment close to free of charge to all citizens, and this fact may limit the generalizability of our findings to samples from countries with different organization of their health care systems. Our design could be criticized for not having more focus on clinical examination of arm/shoulder pain which only was rated by two of 13 items of the KAPS. Our findings concerning pain in 2004 should be considered in this perspective. Some of our study groups had small sample sizes, which imply considerable risk of type II statistical errors, and non-significant findings in small groups could be significant in bigger samples. With the smallest groups of n = 29/30 (restricted self-rated mobility in 2004 and 2007), only the big group differences with effect sizes of Cohen’s coefficient d >0.90 would be significant. However, many of our other subgroup had sample sizes in which moderate effects sizes would show significance.
Some strengths of our study also should be mentioned. The classification of impaired abduction and lymphedema were based on objective assessment, thereby reducing the risk of misclassification. Including the 2007 follow-up, data enabled us to study eventual changes in the associations between ASPs and QoL over a longer time span. By setting the p at <0.01 we also reduced the risk for spurious positive associations in our analyses.
Our study has an important clinical message concerning BCSs, namely that attention to ASPs other than lymphedema is important, in particular restricted mobility. The efficacy of physiotherapy upon arm/shoulder function and pain has mainly been studied during the first months after primary surgery [36]. To our knowledge no studies have been published showing results of interventions for shoulder mobility on a long term basis. We therefore see the need for more clinical trials, studying different interventions aimed at preventing long-term ASPs or achieving improvement of ASPs.
In conclusion, ASPs in BCSs seem to have a considerable and long-lasting effect on physical QoL and negative aspects of the IOC measurements. Only self-rated lymphedema show significant associations with QoL in our study. However, reduced arm/shoulder mobility had a strong and lasting influence on QoL. More clinical attention should therefore be given to other aspects of ASPs in addition to lymphedema.
References
Ahmed RL, Prizment A, Lazovich DA, Schmitz KH, Folsom AF. Lymphedema and quality of life in breast cancer survivors: The Iowa Women’s Health Study. J Clin Oncol. 2008;26:5689–96.
Norman SA, Russel Locario A, Potashnik SL, Simoes Torpey HA, Kallan MJ, Weber AL, et al. Lymphedema in breast cancer survivors: incidence, degree, time course, treatment, and symptoms. J Clin Oncol. 2009;27:390–97.
Nesvold IL, Dahl AA, Løkkevik E, Mengshoel AM, Fosså SD. Arm and shoulder morbidity in breast cancer patients after breast-conserving therapy versus mastectomy. Acta Oncol. 2008;47:835–42.
Peuckmann V, Ekholm O, Rasmussen NK, Groenvold M, Christiansen P, Møller S, et al. Chronic pain and other sequelae in long-term breast cancer survivors: nationwide survey in Denmark. Eur J Pain. 2009;13:478–85.
Sagen A, Kåresen R, Risberg MA. Changes in arm morbidities and health-related quality of life after breast cancer surgery—a five year follow-up study. Acta Oncol. 2009;48:1102–10.
Montazeri A. Health-related quality of life in breast cancer patients: a bibliographic review of the literature from 1974 to 2007. J Exp Clin Ca Res. 2008;27:1–31.
Engel J, Kerr J, Schlesinger-Raab A, Sauer H, Hölzel D. Axillary surgery severely affects quality of life: results of a 5-year prospective study in breast cancer patients. Breast Cancer Res Treat. 2003;79:47–57.
Kwan W, Jackson J, Weir LM, Dingee C, McGregor Greg, Olivotto IA. Chronic arm morbidity after curative breast cancer treatment: prevalence and impact on quality of life. J Clin Oncol. 2002;20:4242–48.
Chachaj A, Malyszczak K, Pyszel K, Lukas J, Tarkowski R, Pudelko M, et al. Physical and psychological impairments of women with upper limb lymphedema following breast cancer treatment. Psycho-Oncol. 2010;19:299–305.
Pyszel A, Malyszczak K, Pyszel K, Andrejak R, Szuba A. Disability, psychological distress and quality of life in breast cancer survivors with arm lymphedema. Lymphology. 2006;39:185–92.
Bentzen SM, Overgaard AM, Thames HD. Fractionation sensitivity of a functional endpoint: impaired shoulder movement after post-mastectomy radiotherapy. Int J Radiat Oncol Biol Phys. 1989;17:531–37.
Mols F, Vingerthoets AJ, Coebergh JW, van de Poll-Franse LV. Quality of life among long-term breast cancer survivors: a systematic review. Eur J Cancer. 2005;41:2613–19.
Zebrack BJ, Ganz PA, Bernaards CA, Petersen L, Abraham L. Assessing the impact of cancer: development of a new instrument for long-term survivors. Psycho-Onco. 2006;15:407–21.
Pearce NJM, Sanson-Fisher R, Campell HS. Measuring quality of life in cancer survivors:a methodological review of exisaitng scale. Psycho-Oncol. 2008;17:629–40.
Reinertsen KV, Cvankarova M, Wist E, Fosså SD, et al. Thyroid function in women after multimodal treatment for breast cancer stage II/III: comparison with controls from a population sample. Int J Radiat Oncol Biol Phys. 2009;75:764–70.
Karges JR, Mark BE, Stikeleather SJ, Worrell TW. Concurrent validity of upper-extremity volume estimates: comparison of calculated volume derived from girth measurements and water displacement volume. Phys Therapy. 2003;83:134–45.
Nesvold IL, Fosså SD, Naume B, Dahl AA. Kwan´s arm problem scale: psychometric examination in a sample of stage II breast cancer survivors. Breast Cancer Res Treat. 2008;117:281–88.
Sprangers MAG, Groenvold M, Arraras JI, Franklin J, te Velde A, Muller M, et al. The European Organization for Research and Treatment of Cancer breast cancer-specific quality-of-life questionnaire module: first results from a three-country field study. J Clin Oncol. 1996;14:2756–68.
Ware JE, Snow KK, Kosinski M, et al. SF-36® health survey: manual and interpretation guide. Lincoln: Quality Metric Inc; 2000.
Ware JE, Gandek B, Kosinski M, et al. The equivalence of the SF-36 summary health scores estimating using standard and country-specific algorithms in 10 countries: results from the IQOLA project. J Clin Epidemiol. 1998;11:1167–70.
Lipsey MW, Wilson DB. Practical meta-analysis Thousand Oaks. CA: Sage; 2001.
Nakagawa S, Cuthill IC. Effect size, confidence interval and statistical significance: a practical guide for biologists. Biol Rev. 2007;82:591–605.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: Earlbaum; 1988.
Schwartz CE, Bode R, Repucci N, Becker J, Sprangers MAG, Fayers PM. The clinical significance of adaptation to changing health: a meta-analysis of response shift. Quality of Life Res. 2006;15:1533–50.
Thomas-Maclean RL, Hack T, Kwan W, Towers A, Miedema B, Tilley A. Arm morbidity and disability after breast cancer: new directions of care. Oncol Nurs Forum. 2008;35:65–71.
Smoot B, Wong J, Cooper B, Wanec L, Topp K, Byl N, et al. Upper extremity impairments in women with or without lymphedema following breast cancer treatment. J Cancer Surviv 2010;4:167–78.
Kuehn T, Klauss W, Darsow M, Regele S, Flock F, Kreienberg R, et al. Long-term morbidity following axillary dissection in breast cancer patients—clinical assessment, significance for life quality and the impact of demographic, oncologic and therapeutic factors. Breast Cancer Res Treat. 2000;64:275–86.
Lauridsen MC, Overgaard M, Overgaard J, Hessow IB, Christiansen P. Shoulder disability and late symptoms following surgery for early breast cancer. Acta Oncol. 2008;47:569–75.
Levangie PK, Drouin J. Magnitude of late effects of breast cancer treatment on shoulder function: a systematic review. Breast Cancer Res Treat. 2009;116:1–15.
Hopwood P, Haviland JS, Sumo G, Mills J, Bliss JM, Yarnold JR. Comparison of patient-reported breast, arm, and shoulder symptoms and body image after radiotherapy for early breast cancer: 5-year follow-up in the randomised Standardisation of Breast Radiotherapy (START) trials. Lancet Oncol. 2010;11:231–40.
Liu C, Guo Y, Shi J, Sheng Y. Late morbidity associated with a tumour-negative sentinel lymph-node biopsy in primary breast cancer patients: a systematic review. Eur J Cancer. 2009;45:1560–8.
Vignes S, Arrault M, Dupuy A. Factors associated with increased breast cancer-related lymphedema volume. Acta Oncol. 2007;46:1138–42.
Koul R, Dufan T, Russell C, Guenther W, Nugent Z, Sun X, et al. Efficacy of complete decongestive therapy and manual lymphatic drainage on treatment-related lymphedema in breast cancer. Int J Radiat Oncol Biol Phys. 2007;67:841–46.
Mansel RE, Fallowfield L, Kissin M, Goyal A, Newcombe RG, Dixon JM, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC Trial. J Natl Cancer Inst. 2006;98:599–609.
Purushotham AD, Upponi S, Klevesath MB, Bobrow L, Millar K, Myles JP, et al. Morbidity after sentinel lymph node biopsy in primary breast cancer: results form a randomized controlled trial. J Clin Oncol. 2005;23:4312–21.
McNeely ML, Campbell K, Ospina M, Rowe BH, Dabbs K, Klassen TP, et al. Exercise interventions for upper-limb dysfunction due to breast cancer treatment (Review). 2010; The Cochrane Collaboration.
Acknowledgments
The first author holds a phd-grant sponsored by The Norwegian Research Council and the Legacies of Radiumhospitalet and National Resource Centre for Women´s Health, Oslo University Hospital, Rikshospitalet.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Nesvold, IL., Reinertsen, K.V., Fosså, S.D. et al. The relation between arm/shoulder problems and quality of life in breast cancer survivors: a cross-sectional and longitudinal study. J Cancer Surviv 5, 62–72 (2011). https://doi.org/10.1007/s11764-010-0156-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-010-0156-4