
Abstract
Objective
We reviewed the available literature on patients with coronary artery disease undergoing isolated coronary artery bypass grafting (CABG) with either single (SAG) or multiple arterial grafting (MAG).
Methods
Original research studies that evaluated the long-term survival of MAG versus SAG were identified, from 1995 to 2022. The median overall survival (OS) and event-free OS were the primary endpoints. Comparison of median OS between the right internal mammary artery (RIMA) and radial artery (RA) as a second arterial conduit was the secondary endpoint. Subgroup analyses were performed regarding patients older than 70 years, with diabetes mellitus, and females. A sensitivity analysis was performed with the leave-one-out method.
Results
Forty-four studies were included in the qualitative and thirty-nine in the quantitative synthesis. After pooling data from 180 to 459 patients, the MAG group demonstrated a higher OS (HR, 0.589; 95% CI, 0.58–0.60; p < 0.0001) and event-free OS compared with the SAG group (HR, 0.828; 95% CI, 0.80–0.86; p < 0.0001). In addition, RITA was associated with superior OS compared with RA as a second arterial conduit (HR, 0.936; 95% CI, 0.89–0.98; p = 0.009). MAG was also superior to SAG in patients over 70 years, females, and patients with diabetes mellitus. Sensitivity analysis demonstrated a small-size study effect on the female subgroup analysis.
Conclusion
The present meta-analysis indicates that MAG is associated with enhanced survival outcomes compared to SAG for patients undergoing isolated CABG.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Despite the progress in cardiac surgery, whether coronary artery bypass grafting (CABG) should be performed with multiple arterial grafts remains highly debated. Numerous observational studies and meta-analyses have reported the benefit of using multiple arterial grafting (MAG) [1,2,3]. The radial artery (RA), the right internal thoracic artery (RITA), along with the saphenous vein (SV) are all grafts that are routinely being used, although a significant part of the surgeons still favors the use of SV. The main reason is that previous RCTs have failed to demonstrate a survival benefit of MAG over single arterial grafting (SAG) because they were either underpowered [4] or inconclusive due to discrepancies between the treatment allocated and the treatment that was received [5]. Nonetheless, a recently published post hoc analysis of the SYNTAXES trial has demonstrated the superiority of MAG over SAG for patients undergoing CABG [6]. In the same context, the results of the ongoing ROMA trial comparing MAG with single internal thoracic artery (SITA) grafting, which was conceptualized to address the drawbacks of ART mentioned above, are not expected until 2025 [7].
Although there is a previous meta-analysis on the topic [3], it failed to provide any sensitivity analysis, subgroup analyses regarding diabetes and sex were not performed, it did not use independent patient data and no Kaplan–Meier curves were constructed. To provide credible evidence on this topic in the interim period until the publication of ROMA outcomes, we decided to perform a meta-analysis on long-term survival endpoints comparing MAG and SAG as two different CABG strategies for patients with coronary artery disease (CAD), using independent patient data, thus enhancing the level of evidence.
Materials and methods
Search strategy and articles selection
The present study was conducted according to the protocol agreed by all authors and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses [8]. A thorough literature search in Pubmed (Medline), Scopus (ELSEVIER), and Cochrane Central Register of Controlled Studies (CENTRAL) (last search: October 18th, 2022) was performed. The following terms were employed in every possible combination: “coronary artery bypass grafting”, “cabg”, “multiple arterial grafting”, “multiple arterial graft”, “multiple arteries”, “mag”, “single arterial graft”, “sag”, “radial artery”, “ra”, “right internal thoracic artery”, “rita”, “rima”, “sima”, “bima”, and “bilateral internal mammary artery”. Inclusion criteria were (1) original reports with ≥ 10 patients, (2) written in English, (3) published from 1995 to 2022, (4) conducted on human subjects, and (5) reporting outcomes of patients with CAD undergoing isolated CABG with either MAG or SAG (SAG was defined as the anastomosis of left internal thoracic artery (LITA) to the left anterior descending (LAD) arterial target). Duplicate articles were excluded. The reference lists of all included articles were also reviewed for additional studies. Two independent reviewers (DEM, MPF) extracted data from the included studies. Any discrepancies between the investigators were discussed with the senior author (TA) to include articles that best matched the criteria until consensus was reached. The authors had personal equipoise regarding the best intervention.
Data extraction and endpoints
For each eligible study, data were extracted relative to demographics (number of patients, gender, age, ejection fraction (EF), comorbidities, the use of either off-pump (OPCAB) or on-pump coronary artery bypass (ONCAB), and follow-up), along with the long-term survival endpoints (median overall survival (OS) and median event-free survival). Although multiple studies analyzed the same population, only the larger study or the one with the longest follow-up was included.
Median OS and event-free OS were the primary endpoints. Event-free OS was defined as OS free of a major adverse cardiac and cerebrovascular event (MACCE) or reintervention/reoperation. Median OS in patients receiving either the right internal mammary artery (RIMA) or radial artery (RA) as a second arterial conduit was the secondary endpoint. Pooled analysis of overall survival was performed based on the published Kaplan–Meier graphs from the included studies, using the 2-stage approach as described by Liu et al. [9]. In the first stage, raw data coordinates (time, survival probability) were extracted from each treatment arm in the Kaplan–Meier curves. In the second stage, the data coordinates were processed based on the raw data coordinates from the first stage in conjunction with the numbers at risk at certain time points, and individual patient data (IPD) were reconstructed. Finally, the reconstructed IPD were pooled and visualized in Kaplan–Meier graphs. The Gehan–Breslow–Wilcoxon test was employed to compare the OS and event-free OS between the two groups. A p value < 0.05 was set as the threshold indicating a statistically significant result. Finally, the Mantel–Haenszel method was employed to calculate the hazard ratio (HR) with 95% confidence intervals (95% CI).
Sensitivity analysis on primary endpoints
To further validate our outcomes, we performed additional sensitivity analyses regarding OS and DFS using the leave-one-out method. The leave-one-out method involves performing a meta-analysis on each subset of the studies obtained by leaving out exactly one study. Furthermore, we constructed Kaplan–Meier curves using adjusted patient groups regarding OS to further assess our outcomes. Finally, we performed subgroup analyses on females, patients aged > 70 years, and patients with diabetes mellitus (DM).
Quality and publication bias assessment
The Newcastle–Ottawa Quality Assessment Scale (NOS) [10] was used as an assessment tool to evaluate non-RCTs. The scale’s range varies from zero to nine stars, and studies with a score equal to or higher than five were considered to have adequate methodological quality. The Risk of Bias in Non-Randomized Studies of Interventions tool (ROBINS-I) was also systematically used to assess the included studies for risk of bias [11]. The RCTs were assessed for their quality according to the Cochrane Handbook for Systematic Reviews of Interventions [12]. Two reviewers (DEM, MPF) rated the studies independently and a final decision was reached by consensus.
Results
Search strategy and patient demographics
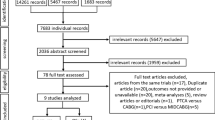
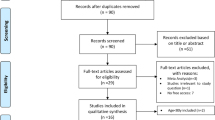
The flow diagram regarding the search strategy is shown in Fig. 1 and the Prisma Checklist 2020 (Supplementary material). The characteristics of the included studies are summarized in Table 1. Among the 117 articles in Pubmed, Scopus, and CENTRAL that were retrieved, forty-four studies [5, 6, 13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54] were included in the qualitative and thirty-nine in the quantitative synthesis [5, 6, 13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36, 42,43,44,45,46,47,48,49,50,51,52,53,54]. The level of agreement between the two reviewers was “almost perfect” (kappa = 0.946; 95% CI:0.885, 1.000). The study design was randomized-controlled in eight studies [5, 6, 25, 37,38,39, 41, 49], and retrospective in thirty-six studies [13,14,15,16,17,18,19,20,21,22,23,24, 26,27,28,29,30,31,32,33,34,35,36, 40, 42,43,44,45,46,47,48, 51,52,53,54]. Propensity score matching (PSM) was performed in thirty-two studies [13,14,15,16, 18, 20,21,22,23,24, 26,27,28, 30,31,32,33,34,35,36, 42,43,44,45,46,47,48, 52,53,54]. The included studies were conducted in UK [13,14,15, 35, 43, 44], Italy [16, 19, 37], Australia [17], USA [21, 24,25,26,27, 30,31,32,33,34, 36, 38, 40, 47, 48], Canada [19, 20, 22, 28, 42, 45, 50, 53], Japan [51, 52, 54], Sweden [29], Portugal [46], Serbia [41], and three were multinational [5, 6, 49]. The studies were published between 1995 and 2022. The total sample size was 180,459 patients (MAG:56,175; SAG:124,284). The baseline characteristics and the NOS assessment of the included studies are provided in Table 1. The mean follow-up period ranged from 1 to 14 years. Figure 2a, b shows the qualitative assessment with the ROBINS-I tool. The authors’ main concerns are related to biases owing to the selection of participants and performance. The qualitative assessment of RCTs is demonstrated in Table S1.

MAG vs. SAG trial flow


Risk of Bias in Non-Randomized Studies of Interventions with a. traffic lights. b. summary plot
Primary endpoints: OS and event-free OS
Figure 3A depicts the pooled Kaplan–Meier curves for overall survival in the total, unadjusted for risk factors, population. Patients in the MAG group demonstrated a significantly higher OS (HR:0.59; 95% CI:0.58–0.60; p < 0.0001). Median OS was 17.54 years for the MAG group and 11.63 years for the SAG group. Figure 3b depicts the pooled Kaplan–Meier curves for event-free survival, incorporating data from 47 to 376 patients (MAG:23, 569 patients; SAG:23,807 patients). Patients in the MAG group were associated with a significantly higher event-free OS (0.83; 0.80–0.86; p < 0.0001).

Pooled Kaplan–Meier curves comparing multiple arterial grafting (MAG) versus single arterial grafting (SAG) for a. overall survival (OS), b. event-free OS, and c. difference in OS between right internal thoracic artery (RITA) and radial artery (RA) as a second arterial conduit. CI confidence interval; HR hazard ratio
Secondary endpoints: RIMA vs RA as a second arterial conduit in terms of OS
Figure 3C depicts the pooled Kaplan–Meier curves regarding OS for patients that received either a RITA or a RA as a second arterial conduit. The data of 31,178 patients (RITA:13,575 patients; RA:20,245 patients) were incorporated. Patients in the RITA group demonstrated a significantly higher OS (HR:0.936; CI:0.89–0.98; p = 0.009).
Subgroup analyses
Finally, we performed subgroup analyses comparing MAG vs SAG in (a) patients > 70 years, (b) patients with DM, and (c) female patients. MAG was superior in terms of OS in all three subgroup analyses, as demonstrated in Figs. 4a, b, c, and Table 2.

Subgroup pooled Kaplan–Meier curves regarding overall survival (OS) for patients a. > 70 years, b. with diabetes mellitus (DM), and c. female. CI confidence interval, HR hazard ratio
Sensitivity analysis
No difference in the survival outcomes was found after performing the leave-one-out sensitivity analysis. This should be especially highlighted in the secondary outcomes, given the longer follow-up of the RITA group. Nonetheless, it should be noted that in the subgroup analysis regarding females, there was a significant superiority of MAG over SAG when excluding either the study by Pullan et al. [43] or Gaudino et al. [24], which is in accordance with previous evidence [54]. In fact, the outcomes did not change, after curing data to include comparable follow-up periods. In a second step, we adjusted the patient data for potential cofounders (age, gender, comorbidities, prior myocardial infraction (MI), prior cardiac intervention/surgery, ejection fraction, presence/absence of LMCAD) regarding median OS. The outcomes were similar to the total analysis, as demonstrated in Fig. 5.

Risk-adjusted pooled Kaplan–Meier curve regarding overall survival (OS). CI confidence interval, HR hazard ratio
Discussion
The present meta-analysis identified forty-three articles and provides additional value to the existing literature since it is the first meta-analysis pooling reconstructed time-to-event data of 180,459 patients at the independent patient level and producing pooled Kaplan–Meier curves. According to our outcomes, MAG is associated with enhanced long-term survival outcomes compared to SAG. These results are further validated by the sensitivity/subgroup analyses. Although a previous meta-analysis [3] was conducted in 2019 (study period until 12/2018), it was associated with several methodological limitations, such as the absence of important subgroup analyses (gender, DM), while no Kaplan–Meier curves were constructed, and the data extraction was not at the patient level.
Defining the optimal CABG grafting strategy is crucial to enhance quality in terms of clinical outcomes, along with economic efficiency. Nonetheless, the recent evidence on long-term survival provided by large RCTs has been contradictory [25, 49] and the conundrum still exists. In the same context, outcomes from the ROMA trial are expected no earlier than 2025 [7]. According to the present study, patients in the MAG group demonstrated higher OS in both the unadjusted and adjusted analyses. Furthermore, they were associated with superior event-free OS compared with those patients receiving SAG.
The evidence provided in the literature regarding the comparison between the RITA and RA as a second arterial conduit is discordant. Two previous meta-analyses performed by the same team [55, 56] demonstrated contradicting outcomes. According to the earlier one [55], RITA was associated with a 25% relative reduction in the risk of long-term mortality. On the other hand, the most recent meta-analysis showed similar long-term survival between the two arterial conduits [56]. According to our outcomes, which were produced by building a pooled Kaplan–Meier curve, RITA was associated with a higher long-term survival when used as a second arterial conduit compared with RA. Potential reasons underlying these discrepancies might be (a) the different sample size and follow-up period (the present study is the biggest incorporating 180,459 patients), (b) the different data extraction (reconstructed time-to-event data in the present study) and statistical methods (construction of pooled Kaplan–Meier curves), (c) differences regarding the surgical technique (e.g., skeletonized or not regarding RITA, differences in RA harvesting protocol), (d) potential differences in treatment protocol regarding the extend of stenosis of target vessels for RA conduits, (e) differences in the post-discharge treatment protocols, and (f) potential differences regarding baseline characteristics of the included patients in spite of the risk-adjusted nature of the comparisons. In fact, a crucial point when using the RA for CABG is the degree of target vessel stenosis. It has been shown that the patency rate of RA grafts is strongly influenced by the degree of target stenosis [57].
The present meta-analysis also demonstrated the superiority of MAG over SAG for two groups of high-risk patients, those aged > 70 years and those with DM. Evidence remains contradicted regarding the usefulness of MAG in elderly patients, along with the cutoff age to define a patient as elderly [58]. In the present meta-analysis, we used the age of 70 years as a cutoff point and we demonstrated that MAG is superior to the SAG strategy in terms of OS in the > 70 years group. This outcome is in accordance with previous evidence [59]. However, it would be interesting to examine the value of MAG in elderly patients with reduced EF, an endpoint that was out of the scope of the present meta-analysis. In the same context, Chikwe et al. [60] analyzed the New Jersey registry of 26,000 patients and found no significant benefits of MAG in patients > 70 years with reduced EF. The potential value of MAG in patients with DM has been another debatable topic. In fact, according to a recent post hoc analysis of the ART trial [49], MAG is associated with higher OS in patients with DM, independently of the type of DM, which is in accordance with our findings.
Another subgroup analysis we performed was the difference between the two strategies in terms of OS in female patients. Generally, women represent an under-represented patient group in observational and randomized CABG studies. For instance, women represented a 15% ratio of the 3,102 patients incorporated in the ART study [49]. Nonetheless, women have significant differences in biology and baseline characteristics compared with male patients. According to our outcomes, MAG was again superior to SAG in terms of OS in female patients. Nonetheless, this outcome was sensitive to the small-study effect, demonstrating when we performed the leave-one-out sensitivity analysis. These results are in agreement with the outcomes of a previous meta-analysis by Robinson et al. [61].
The limitations of the current meta-analysis reflect the limitations of the studies included. Although the majority of the studies were retrospective in nature, they provided either risk-adjusted or PSM analyses. Furthermore, eight studies were RCTs. In addition, the included studies are related to biases related to the selection of participants and performance. Moreover, the differences among institutions regarding the selection criteria, treatment protocols, and perioperative management pose certain limitations. In fact, the selection criteria were not homogenous and may have been based on the patients’ clinical attributes and status, thus posing a selection bias that could not be adjusted in the present study. Finally, patient data were gathered from Kaplan–Meier-derived data, thus limiting our ability to perform further multivariable analyses.
On the other hand, the strengths of this study include (a) the clear data extraction protocol, (b) the well-specified inclusion–exclusion criteria, (c) the search that was performed in three different databases, (d) the quality assessment of the included studies, (e) the detailed presentation of the results of data extraction and analysis, (f) the extraction of survival data at the level of the independent patient, and (g) the performance of sensitivity and subgroup analyses.
Conclusion
In the context of patients with central CAD undergoing isolated CABG, MAG is superior to SAG in terms of median OS and event-free OS. Furthermore, MAG was also superior for patients > 70 years, females, or patients with DM. Finally, RITA was superior to RA as a second arterial conduit on long-term OS. The present evidence represents the best currently available level of evidence and should be used as a bridge until the publication of ROMA trial outcomes.
Data availability
The data supporting this study are available from the corresponding author, upon reasonable request.
References
Buttar SN, Yan TD, Taggart DP, Tian DH. Long-term and short-term outcomes of using bilateral internal mammary artery grafting versus left internal mammary artery grafting: a meta-analysis. Heart. 2017;103:1419–26.
Athanasiou T, Saso S, Rao C, et al. Radial artery versus saphenous vein conduits for coronary artery bypass surgery: forty years of competition–which conduit offers better patency? A systematic review and meta-analysis. Eur J Cardiothorac Surg. 2011;40(1):208–20. https://doi.org/10.1016/j.ejcts.2010.11.012.
Saraiva FA, Leite-Moreira JP, Barros AS, Lourenço AP, Benedetto U, Leite-Moreira AF. Multiple versus single arterial grafting in coronary artery bypass grafting: a meta-analysis of randomized controlled trials and propensity score studies. Int J Cardiol. 2020;1(320):55–63. https://doi.org/10.1016/j.ijcard.2020.08.001.
Nasso G, Coppola R, Bonifazi R, Piancone F, Bozzetti G, Speziale G. Arterial revascularization in primary coronary artery bypass grafting: direct comparison of 4 strategies–results of the Stand-in-Y Mammary Study. J Thorac Cardiovasc Surg. 2009;137:1093–100.
Taggart DP, Benedetto U, Gerry S, et al. Arterial revascularization trial investigators. Bilateral versus single internal-thoracic-artery grafts at 10 years. N Engl J Med. 2019;380:437–46.
Thuijs DJFM, Davierwala P, Milojevic M, et al. Long-term survival after coronary bypass surgery with multiple versus single arterial grafts. Eur J Cardiothorac Surg. 2022;61:925–33.
Gaudino M, Alexander JH, Bakaeen FG, et al. Randomized comparison of the clinical outcome of single versus multiple arterial grafts: the ROMA trial-rationale and study protocol. Eur J Cardiothorac Surg. 2017;52:1031–40.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71. https://doi.org/10.1136/bmj.n71.
Liu N, Zhou Y, Lee JJ. IPDfromKM: reconstruct individual patient data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2021;21(1):111. https://doi.org/10.1186/s12874-021-01308-8.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5. https://doi.org/10.1007/s10654-010-9491-z.
Sterne JA, Hern an MA, Reeves BC, et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016;355:i4919.
Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. 2011 Available from www.cochrane-handbook.org
Benedetto U, Codispoti M. Age cutoff for the loss of survival benefit from use of radial artery in coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2013. https://doi.org/10.1016/j.jtcvs.2013.07.025.
Benedetto U, Amrani M, Gaer J, et al. Harefield cardiac outcomes research group. The influence of bilateral internal mammary arteries on short- and long-term outcomes: a propensity score matching in accordance with current recommendations. J Thorac Cardiovasc Surg. 2014;148(6):2699–705. https://doi.org/10.1016/j.jtcvs.2014.08.021.
Benedetto U, Caputo M, Mariscalco G, et al. Impact of multiple arterial grafts in off-pump and on-pump coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2017;153(2):300-309.e6. https://doi.org/10.1016/j.jtcvs.2016.10.084.
Bisleri G, Di Bacco L, Turturiello D, et al. Improved outcomes of total arterial myocardial revascularization in elderly patients at long-term follow-up: a propensity-matched analysis. Ann Thorac Surg. 2017;103(2):517–25. https://doi.org/10.1016/j.athoracsur.2016.06.028.
Buxton BF, Shi WY, Tatoulis J, Fuller JA, Rosalion A, Hayward PA. Total arterial revascularization with internal thoracic and radial artery grafts in triple-vessel coronary artery disease is associated with improved survival. J Thorac Cardiovasc Surg. 2014;148(4):1238–43. https://doi.org/10.1016/j.jtcvs.2014.06.056.
Calafiore AM, Di Giammarco G, Teodori G, et al. Late results of first myocardial revascularization in multiple vessel disease: single versus bilateral internal mammary artery with or without saphenous vein grafts. Eur J Cardiothorac Surg. 2004;26(3):542–8. https://doi.org/10.1016/j.ejcts.2004.05.028.
Carrier M, Cossette M, Pellerin M, et al. Statin treatment equalizes long-term survival between patients with single and bilateral internal thoracic artery grafts. Ann Thorac Surg. 2009;88(3):789–95. https://doi.org/10.1016/j.athoracsur.2009.04.097.
Cohen G, Tamariz MG, Sever JY, et al. The radial artery versus the saphenous vein graft in contemporary CABG: a case-matched study. Ann Thorac Surg. 2001;71(1):180–5. https://doi.org/10.1016/s0003-4975(00)02285-2.
DeSimone JP, Malenka DJ, Weldner PW, et al. Northern New England Cardiovascular Disease Study group. Coronary Revascularization With Single Versus Bilateral Mammary Arteries: Is It Time to Change? Ann Thorac Surg. 2018. https://doi.org/10.1016/j.athoracsur.2018.01.089.
Dewar LR, Jamieson WR, Janusz MT, et al. Unilateral versus bilateral internal mammary revascularization Survival and event-free performance. Circulation. 1995. https://doi.org/10.1161/01.cir.92.9.8.
Garatti A, Castelvecchio S, Canziani A, et al. Long-term results of sequential vein coronary artery bypass grafting compared with totally arterial myocardial revascularization: a propensity score-matched follow-up study†. Eur J Cardiothorac Surg. 2014;46(6):1006–13. https://doi.org/10.1093/ejcts/ezu057.
Gaudino M, Samadashvili Z, Hameed I, Chikwe J, Girardi LN, Hannan EL. Differences in Long-term outcomes after coronary artery bypass grafting using single vs multiple arterial grafts and the association with sex. JAMA Cardiol. 2020;6(4):401–9. https://doi.org/10.1001/jamacardio.2020.6585.
Goldman S, Sethi GK, Holman W, et al. Radial artery grafts vs saphenous vein grafts in coronary artery bypass surgery: a randomized trial. JAMA. 2011;305(2):167–74. https://doi.org/10.1001/jama.2010.1976.
Goldstone AB, Chiu P, Baiocchi M, et al. Second arterial versus venous conduits for multivessel coronary artery bypass surgery in California. Circulation. 2018;137(16):1698–707. https://doi.org/10.1161/CIRCULATIONAHA.117.030959.
Grau JB, Johnson CK, Kuschner CE, et al. Impact of pump status and conduit choice in coronary artery bypass: a 15-year follow-up study in 1412 propensity-matched patients. J Thorac Cardiovasc Surg. 2015;149(4):1027-33.e2. https://doi.org/10.1016/j.jtcvs.2014.12.031.
Guru V, Fremes SE, Tu JV. How many arterial grafts are enough? A population-based study of midterm outcomes. J Thorac Cardiovasc Surg. 2006;131(5):1021–8. https://doi.org/10.1016/j.jtcvs.2005.09.036.
Janiec M, Dimberg A, Nazari Shafti TZ, Lagerqvist B, Lindblom RPF. No improvements in long-term outcome after coronary artery bypass grafting with arterial grafts as a second conduit: a Swedish nationwide registry study. Eur J Cardiothorac Surg. 2018;53:448–54.
Kurlansky PA, Traad EA, Dorman MJ, Galbut DL, Zucker M, Ebra G. Thirty-year follow-up defines survival benefit for second internal mammary artery in propensity-matched groups. Ann Thorac Surg. 2010;90(1):101–8. https://doi.org/10.1016/j.athoracsur.2010.04.006.
LaPar DJ, Crosby IK, Rich JB, et al. Investigators for the virginia cardiac surgery quality initiative. Bilateral internal mammary artery use for coronary artery bypass grafting remains underutilized: a propensity-matched multi-institution analysis. Ann Thorac Surg. 2015;100(1):8–14. https://doi.org/10.1016/j.athoracsur.2015.02.088.
Lawton JS, Barner HB, Bailey MS, et al. Radial artery grafts in women: utilization and results. Ann Thorac Surg. 2005;80(2):559–63. https://doi.org/10.1016/j.athoracsur.2005.02.055.
Lin J, Cheng W, Czer LS, et al. Coronary artery bypass graft surgery using the radial artery as a secondary conduit improves patient survival. J Am Heart Assoc. 2013;2(4): e000266. https://doi.org/10.1161/JAHA.113.000266.
Locker C, Schaff HV, Dearani JA, et al. Multiple arterial grafts improve late survival of patients undergoing coronary artery bypass graft surgery: analysis of 8622 patients with multivessel disease. Circulation. 2012;126(9):1023–30. https://doi.org/10.1161/CIRCULATIONAHA.111.084624.
Luthra S, Leiva-Juarez MM, John A, Matuszewski M, Morgan IS, Billing JS. A second arterial conduit to the circumflex circulation significantly improves survival after coronary artery bypass surgery. Eur J Cardiothorac Surg. 2018;53:455–62.
Lytle BW, Blackstone EH, Sabik JF, Houghtaling P, Loop FD, Cosgrove DM. The effect of bilateral internal thoracic artery grafting on survival during 20 postoperative years. Ann Thorac Surg. 2004;78(6):2005–12. https://doi.org/10.1016/j.athoracsur.2004.05.070.
Muneretto C, Negri A, Manfredi J, et al. Safety and usefulness of composite grafts for total arterial myocardial revascularization: a prospective randomized evaluation. J Thorac Cardiovasc Surg. 2003;125(4):826–35. https://doi.org/10.1067/mtc.2003.154.
Myers WO, Berg R, Ray JF, et al. All-artery multigraft coronary artery bypass grafting with only internal thoracic arteries possible and safe: a randomized trial. Surgery. 2000;128(4):650–9. https://doi.org/10.1067/msy.2000.108113.
Nasso G, Coppola R, Bonifazi R, Piancone F, Bozzetti G, Speziale G. Arterial revascularization in primary coronary artery bypass grafting: direct comparison of 4 strategies–results of the Stand-in-Y mammary study. J Thorac Cardiovasc Surg. 2009;137(5):1093–100. https://doi.org/10.1016/j.jtcvs.2008.10.029.
Parsa CJ, Shaw LK, Rankin JS, et al. Twenty-five-year outcomes after multiple internal thoracic artery bypass. J Thorac Cardiovasc Surg. 2013;145(4):970–5. https://doi.org/10.1016/j.jtcvs.2012.11.093.
Petrovic I, Nezic D, Peric M, et al. Radial artery vs saphenous vein graft used as the second conduit for surgical myocardial revascularization: long-term clinical follow-up. J Cardiothorac Surg. 2015;10:127. https://doi.org/10.1186/s13019-015-0331-9.
Pu A, Ding L, Shin J, et al. Long-term outcomes of multiple arterial coronary artery bypass grafting: a population-based study of patients in British Columbia. Canada JAMA Cardiol. 2017;2(11):1187–96. https://doi.org/10.1001/jamacardio.2017.3705.
Pullan M, Kirmani BH, Conley T, et al. The effect of patient sex on survival in patients undergoing isolated coronary artery bypass surgery receiving a radial artery. Eur J Cardiothorac Surg. 2015;47(2):324–30. https://doi.org/10.1093/ejcts/ezu100.
Raja SG, Benedetto U, Jothidasan A, et al. Harefield Cardiac Outcomes Research Group. Right internal mammary artery versus radial artery as second arterial conduit in coronary artery bypass grafting: a case-control study of 1526 patients. Int J Surg. 2015. https://doi.org/10.1016/j.ijsu.2014.08.342.
Rocha RV, Tam DY, Karkhanis R, et al. Multiple arterial grafting is associated with better outcomes for coronary artery bypass grafting patients. Circulation. 2018;138(19):2081–90. https://doi.org/10.1161/CIRCULATIONAHA.118.034464.
Saraiva AF, Girerd N, Cerqueira JR, et al. Survival after bilateral internal mammary artery in coronary artery bypass grafting: are women at risk? Rev Port Cir Cardiotorac Vasc. 2017;24(3–4):101.
Schwann TA, Tranbaugh RF, Dimitrova KR, et al. Time-varying survival benefit of radial artery versus vein grafting: a multiinstitutional analysis. Ann Thorac Surg. 2014;97(4):1328–34. https://doi.org/10.1016/j.athoracsur.2013.09.096.
Schwann TA, Hashim SW, Badour S, et al. Equipoise between radial artery and right internal thoracic artery as the second arterial conduit in left internal thoracic artery-based coronary artery bypass graft surgery: a multi-institutional study. Eur J Cardiothorac Surg. 2016;49:188–95.
Taggart DP, Audisio K, Gerry S, et al. ART Investigators. Single versus multiple arterial grafting in diabetic patients at 10 years: the Arterial Revascularization Trial. Eur Heart J. 2022. https://doi.org/10.1093/eurheartj/ehac199.
Tam DY, Rocha RV, Fang J, et al. Multiple arterial coronary bypass grafting is associated with greater survival in women. Heart. 2021;107(11):888–94. https://doi.org/10.1136/heartjnl-2020-317737.
Hirotani T, Nakamichi T, Munakata M, Takeuchi S. Risks and benefits of bilateral internal thoracic artery grafting in diabetic patients. Ann Thorac Surg. 2003;76(6):2017–22. https://doi.org/10.1016/s0003-4975(03)01062-2.
Kinoshita T, Asai T, Suzuki T. Off-pump bilateral skeletonized internal thoracic artery grafting in patients with chronic kidney disease. J Thorac Cardiovasc Surg. 2015;150(2):315-21.e3. https://doi.org/10.1016/j.jtcvs.2015.04.058.
Mohammadi S, Kalavrouziotis D, Cresce G, et al. Bilateral internal thoracic artery use in patients with low ejection fraction: is there any additional long-term benefit? Eur J Cardiothorac Surg. 2014;46(3):425–31. https://doi.org/10.1093/ejcts/ezu023.
Yamaguchi A, Kimura N, Itoh S, et al. Efficacy of multiple arterial coronary bypass grafting in patients with diabetes mellitus. Eur J Cardiothorac Surg. 2016;50:520–7.
Gaudino M, Lorusso R, Rahouma M, et al. Radial artery versus right internal thoracic artery versus saphenous vein as the second conduit for coronary artery bypass surgery: a network meta-analysis of clinical outcomes. J Am Heart Assoc. 2019;8(2): e010839. https://doi.org/10.1161/JAHA.118.010839.
Benedetto U, Gaudino M, Caputo M, et al. Right internal thoracic artery versus radial artery as the second best arterial conduit: Insights from a meta-analysis of propensity-matched data on long-term survival. J Thorac Cardiovasc Surg. 2016;152(4):1083-1091.e15. https://doi.org/10.1016/j.jtcvs.2016.05.022.
Maniar HS, Sundt TM, Barner HB, et al. Effect of target stenosis and location on radial artery graft patency. J Thorac Cardiovasc Surg. 2002;123:45–52.
Hillis LD, Smith PK, Anderson JL, et al. 2011 ACCF/AHA guideline for coronary artery bypass graft surgery: executive summary: a report of the American college of cardiology foundation/American heart association task force on practice guidelines. Circulation. 2011;124:2610–42.
Saraiva FA, Moreira R, Cerqueira RJ, et al. Multiple versus single arterial grafting in the elderly: a meta-analysis of randomized controlled trials and propensity score studies. J Cardiovasc Surg. 2022;63(2):169–78. https://doi.org/10.23736/S0021-9509.21.11826-9.
Chikwe J, Sun E, Hannan EL, et al. Outcomes of second arterial conduits in patients undergoing multivessel coronary artery bypass graft surgery. J Am Coll Cardiol. 2019;74:2238–48.
Robinson NB, Lia H, Rahouma M, et al. Coronary artery bypass with single versus multiple arterial grafts in women: a meta-analysis. J Thorac Cardiovasc Surg. 2021. https://doi.org/10.1016/j.jtcvs.2021.07.047.
Funding
Open access funding provided by HEAL-Link Greece. The participating authors declare no sources of financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflicts of interest.
Ethical approval
Does not apply.
Informed consent
Does not apply.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Magouliotis, D.E., Fergadi, M.P., Zotos, PA. et al. Differences in long-term survival outcomes after coronary artery bypass grafting using single vs multiple arterial grafts: a meta-analysis with reconstructed time-to-event data and subgroup analyses. Gen Thorac Cardiovasc Surg 71, 77–89 (2023). https://doi.org/10.1007/s11748-022-01891-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-022-01891-7