
Abstract
We conducted a scoping review of studies on health outcomes from electronic nicotine delivery systems (ENDS). The objective was to identify, narratively synthesize, assess the strength and quality of evidence and critically appraise studies that have reported disease end points associated with the use of ENDS. We included published literature on the health impact of ENDS from 01/01/2015 until 01/02/2020 following the PRISMA guidelines using PubMed, Embase, Scopus and Google Scholar. The database search identified 755 studies, and other sources 265; 37 studies met final eligibility criteria. Levels of evidence included 24(65%) cross-sectional, one (2.7%) case–control and six (16%) case studies, four (11%) cohort studies, one (2.7%) randomized controlled trial (RCT) and one (2.7%) meta-analysis; 27(73%) studies reported only on harms, eight (22%) reported on benefits, two (2%) on benefits and harms. Quality ratings were poor in 20 (54%), fair in 9(24%) and good in 8(22%) of studies. In our review, ENDS was not shown to be causative for harmful cardiovascular disease (CVD) outcomes and shown to be beneficial for hypertensive patients. Switching from cigarettes to e-cigarettes resulted in reduced exacerbations of chronic obstructive pulmonary disease (COPD), with no evidence of long-term deterioration in lung function. Mental Health, cancer and mortality were not adequately studied to form any consensus. Our review has not demonstrated ENDS to be causative of harmful CVD outcomes; furthermore switching from cigarettes to e-cigarettes was associated with improved hypertensive control and reduced exacerbations of COPD, with no evidence of increased asthma risk or long-term respiratory harm. Mental health, cancer and mortality outcomes have not been adequately studied to form a conclusion. Overall, the findings of our review did not provide evidence to counter the consensus held by many that ENDS use is safer than the risks posed from smoking cigarettes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Smoking is the leading preventable cause of illness and premature death and one of the top causes of health inequalities, responsible for over eight million deaths a year globally [1].
The availability of tobacco harm reduction (THR) products has dramatically accelerated the reduction in the smoking prevalence rate [2]. Electronic nicotine delivery devices (ENDS), such as electronic cigarettes and vapes, are amongst the most effective smoking cessation methods [3, 4] due to a combination of successful quit rates [5] and their greater reach and accessibility compared with other smoking cessation methods [2].
The prevalence of the use of ENDS is highest in the UK (6%) and the US (4–6%) compared with 1% of the rest of Europe [2]. The vast majority of regular ENDS users are previous or current smokers: in the UK over 99% of adult users and over 99.5% of adolescent users are former smokers [2]; and in the US, 98.7% of adults aged 45 years or older and 60% of adults aged 18–24 years were former smokers [6].
To determine the net health impact of ENDs, the benefits from quitting smoking must be weighed against any harms (or benefits) from the use of ENDS. To date, there has been no clear consensus on the safety profile of ENDS and safety concerns have resulted in varying regulations and bans on their sale and use globally.
Studies investigating the safety profile of ENDS include chemical, toxicological and clinical studies. Chemical studies cannot provide novel safety information as they rely on theoretical models and pre-determined safety levels which are unavailable. Toxicological studies are mostly cytotoxicity studies on established cell lines which cannot be accurately extrapolated to the in-vivo situation as there are too many assumptions and unknowns from the behaviour of cell lines and ENDS product variables such as heat, concentrations and amount of product delivery. Despite this, policy decisions on ENDS and THR products are made using animal, in vitro and in silico studies which may not translate to health outcomes in real-world settings.
A widely used estimate for health risk by Public Health England is that e-cigarettes pose less than 5% risk of conventional cigarettes [7]. More recently the US National Academies of Sciences, Engineering and Medicine (NASEM) consensus is that e-cigarettes are “likely to be far less harmful” than combustible cigarettes [8]. There have been no meta-analyses or systematic reviews to quantify the health risk posed by ENDS to date.
The objective of our scoping review was to identify, narratively synthesize, assess the strength and quality of evidence and critically appraise studies that have reported disease end points associated with the use of ENDS.
Methods
We systematically reviewed published literature on the health impact of ENDS products. We included all electronic nicotine delivery devices (not including heat-not-burn products). The study followed PRISMA guidelines for reporting of systematic reviews [9]. We included health outcomes of new onset or control of disease end-points. We did not include other health outcomes such as short-term physiological changes which do not necessarily manifest as disease, quality of life, studies of emissions only, or those arising from departure from intended use of ENDS devices such as explosions, or use of ENDS devices to vapourise alternative products.
Search strategy and eligibility criteria
A literature search was conducted between 1st October 2019 and 26th February 2020 using the databases PubMed, Embase, Scopus and Google Scholar using medical subject headings. There were two domains for the search, one for use of ENDS and related products and one for health outcomes, specifically cardiovascular disease (CVD), cancer, respiratory, mortality and ‘other’ health outcomes.
Search terms included (“Electronic cigarette” OR “Electronic nicotine delivery system” OR “E-cigarette” OR “Vaping” OR “Vapor” OR “Reduced risk tobacco product” OR “Non cigarette tobacco” OR “Nicotine aerosol” OR “E-cigarette aerosol”) AND (“health outcome” OR “Morbidity” OR “Mortality” OR “Cancer” OR “Cardiovascular disease” OR “Chronic obstruct pulmonary disease” OR “COPD” OR “CVD” OR “Acute myocardial infarction” OR “Stroke” OR “Cardiovascular” OR “Cerebrovascular” OR “Health effects” OR “Adverse” OR “effects” OR “Respiratory”).
Search results were filtered to include only English language, human studies and published from 01/01/2015 until 01/02/2020. Because most ENDS use has fallen within this period and ENDS products have evolved considerably since 2015. The references of relevant reviews were manually searched for additional eligible citations.
The titles, abstracts and full texts of the search results were sequentially screened by two reviewers independently for inclusion using the eligibility criteria below, with disagreements resolved via blind review by a third reviewer.
Figure 1 shows the inclusion and exclusion criteria used.

Inclusion and exclusion criteria
Data extraction and quality assessment
For included studies, data were extracted including author, year, country, aim, study design, sample size, participants and relevant findings such as effect sizes and nature of impact on health outcomes. A level of evidence category was assigned using the Oxford Centre for Evidence-Based Medicine framework[10] and a similar approach used to categorise methodological quality as “good”, “fair” or “poor” utilizing the National Institutes for Health (NIH) Quality Assessment Tools [11]. The NIH quality assessment tools include features to assess the risk of bias, such as selection and reporting bias, with a “good” rating reflecting a low risk of bias, and a “poor” rating suggesting a high risk of bias. A review of common sources of bias encountered in the included literature is given in the discussion. Data extraction and synthesis were formed by two reviewers independently with blind assessment by a third reviewer for cases with rater disagreement. Findings of all studies were independently reviewed, coded and compared between studies to identify relationships and themes.
Results
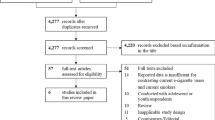
Thirty-seven studies were included in the review. Reasons for excluding studies are shown in Fig. 2.

PRISMA flow chart of included studies and selection process
Table 1 shows that the types of studies were: cross-sectional (24 studies, 65%), case–control (1, 2.7%) and case studies (6, 16%), cohort (1, 11%), randomized controlled trial (RCT; 1, 2.7%), MA/pooled study (1, 2.7%). Each of the 37 studies only examined one of the listed health outcomes. There were 17 studies on respiratory disease [12,13,14, 22,23,24,25,26,27,28,29,30,31,32,33,34,35, 52] followed by CVD (6) [16,17,18,19,20,21] mental health (7), [37,38,39,40,41,42, 54] and one each on oral health[43], two on cancer [15, 36], self-reported chronic health conditions [44], tonsillitis [35] and nickel contact allergy [46].
Table 2 summarises that 27 (73%) of the studies reported only on harms, eight (22%) on benefits, two (2%) on both harm and benefits. Although few in number, studies investigating benefits were of higher levels of evidence with one RCT, three cohort (two examining both harms and benefits), four cross-sectional, one case–control and one case study.
Table 3 summarizes the quality ratings assigned to studies by health outcome. Raters one and two agreed on 32 out of 37 (94%) assessments of quality and level of evidence. “Poor” quality studies made up 20 (54%), “fair” made up nine (24%) and “good” made up eight (22%), with reasons including insufficient follow-up, inability to determine temporality and reverse causation, inadequate accounting for confounders and poor definitions of exposures and outcomes.
Characteristics of included studies including study design, key outcomes, level of evidence and quality ratings are detailed in Table 4 and in further detail in Table 5 (appendix).
Overall results for health outcomes by category
CVD outcomes
Two studies judged to be of good quality, an RCT and observational study, reported reductions in systolic blood pressure (SBP) by 9–10 mmHg, and diastolic BP (DBP) by 6 mmHg in hypertensive patients [16, 17].
Of another four studies, two were rated as ‘fair’ and two as ‘poor’ quality. Two large cross-sectional surveys on approximately 0.5 million [18] and 60,000 [19] subjects found that users of ENDS had no increase in MI, coronary heart disease (CHD), premature CVD or CVD compared with never smokers. However, former smokers who used ENDS did have more CVD (OR 1.4) and premature CVD (OR 1.5) than never smokers in one of the studies [18]. Dual users experienced higher CVD (OR 1.36) compared with those who were current smokers not using ENDS [18]. A further study that did not account for former smokers or dual users, or for temporality and reverse causation, found users of ENDS to have increased risk of myocardial infarction (MR; OR 1.8) [20].
A large cross-sectional study investigating stroke found no excess risk in users of ENDS in never smokers [21]. The use of ENDS in ex-smokers was associated with a higher risk of stroke (OR 2.5) compared with never smokers [16].
Respiratory outcomes
Of 17 studies reporting respiratory outcomes, the majority were on chronic obstructive pulmonary disease (COPD) in adults or asthma in adolescents; only three were rated as ‘high’ quality.
The studies on COPD that were judged to be of low risk of bias were a pooled study of two cohorts [22], and an interventional study over 12 months [23], with further follow-up over 3 years [24]. They reported that COPD exacerbations reduced in frequency in heavy smokers switching to e-cigarettes from 2.3 to 1.4 annually [24], and improvements in verified COPD Assessment Test (CAT) score, walking distance and continued reductions in COPD exacerbations after 3 years [24]. The study pooling findings from two cohort studies [22], without excluding current smokers, reported e-cigarette users to have 8% higher prevalence of chronic bronchitis and COPD exacerbations in one of the two included cohort studies. After 5 years of follow-up, no increased progression of lung disease or decline in lung function was seen in e-cigarette users [22]. Current and former smoking was adjusted for but not excluded.
Five cross-sectional studies [24,25,26,27,28] investigated the association between e-cigarette use and COPD. In one study, [26] 85% of the sample were not in the age-risk category (over 55 years) for COPD [29]. One of the cross-sectional studies on a sample of almost 900,000 never-smokers showed an association (OR 1.5) between e-cigarette use and self-reported COPD compared with non-e-cigarette use [28]. Another study that segmented never and current smokers found an association between e-cigarettes and COPD in smokers (OR 1.3) but not in never-smokers (OR 0.9) [27].
Six studies investigated the development or control of asthma [27, 30,31,32,33,34]. An experimental study showed that following e-cigarette use, respiratory system resistance and impedance were impacted up to 30 min afterwards, but fractional exhaled nitric oxide did not differ between asthmatics and non-asthmatics [28]. Five of the six studies were cross-sectional in design and several relied on children and adolescents self-reporting on e-cigarette use and a diagnosis of asthma in schools and other educational facilities. The definitions of e-cigarette users included experimental and one-time use of e-cigarettes in some studies [30,31,32, 34]. One study [27] reported separately for never smokers and smokers, and found e-cigarette use to be associated with a higher rate of asthma in smokers (OR 1.3) but not in non-smokers (OR 0.9). The remaining studies reported associations between e-cigarette use and asthma, with OR’s ranging between 1.1 and 2.7 [27, 30, 32, 34].
In a cross-sectional study of 914 smokers who switched to e-cigarettes, 66% reported reductions in the frequency of respiratory infections and 6% reported worsening [35]. Single case studies reported on acute hypoxaemic respiratory failure and organizing pneumonia; organizing pneumonia; sensitivity pneumonitis and vesicular bronchial injury, but none specifically excluded other causes such as dual use, former smoking, other drug use or comorbidities.
Cancer
A small cross-sectional study demonstrated lower numbers of oral cancerous cells (50%) and cellular changes (33%) in e-cigarette users who were never smokers compared with smokers (p = 0.001) [36]. The only other study was a case study on two individuals.
Mental health
Seven studies reported on the association between ENDS use and mental health disease [37,38,39,40,41,42, 54]. Of two cohort studies rated as ‘good’ [37, 38] one found that those with depressive symptoms were more likely to take up e-cigarette use at 6 months (beta-coefficients 0.06, 0.08), but no greater depressive symptoms than non e-cigarette users at 12 months [37]. Another cohort study [38] found a greater increase in depressive symptoms in e-cigarette users after 12 months (beta = 1.27, p = 0.01) compared with non e-cigarette users, with a positive dose–response effect.
Four cross-sectional studies [39,40,41,42] reported a positive association between e-cigarette use and self-reported depressive symptoms with wide-ranging ORs from 1.03 to 4.2.
A ‘poor’rated cross-sectional study [54] found an association between e-cigarette use and attention-deficit hyperactivity disorder (ADHD; V = 0.073; p < 0.001), post-traumatic stress disorder (PTSD; V = 0.064; p = < 0.002), gambling disorder (V = 0.081, p < 0.001), anxiety (V = 0.066; p < 0.001), low self-esteem (V = 0.63; p = 0.002) and impulsivity traits (cohen’s d = 0.421; p < 0.001), without controlling for smoking, a participation rate of 38% and not stating a definition for e-cigarette use.
Oral health
A ‘poor’ rated cross-sectional study reported no association with self-reported dental health issues in e-cigarette users compared with never smokers [43].
Other health outcomes
A ‘poor’ rated cross-sectional study reported an association between e-cigarette use and obesity (OR 4.4, p < 0.05) and alcohol abuse (OR 7.0, p < 0.05) [44]. There were two single case studies of e-cigarette use being linked to the improvement of recurrent tonsillitis [35, 45] and occurrence of nickel contact allergy [46].
Mortality
No studies were found that investigated mortality related to the use of ENDS.
Discussion
This is one of the first articles to comprehensively and systematically review health outcomes from ENDS use. The 37 studies identified tended to focus on negative health impacts; the benefits of switching from cigarettes to ENDS, which is the usual pattern of use, was an uncommon outcome measure. Evidence of significant harms to health outcomes from ENDS use was lacking from our review, with most studies being unable to rigorously establish causation. In the handful of adequately rigorously designed studies, no causation was established between the use of ENDS and negative health outcomes. There was some evidence of positive health outcomes in those switching from cigarettes to e-cigarettes, for example in COPD and hypertensive patients, but these findings need replication.
Levels of evidence, quality and study design
There were no studies rated above 2a for level of evidence, i.e. there were no meta-analyses (MAs) or pooling of RCTs. The vast majority of studies (97%) in our review were observational, hence unable to adequately control for confounders and bias, with only one interventional study. The low number of RCTs perhaps reflects the difficulty of conducting interventional THR studies in real-world settings.
Cross-sectional studies were predominant (41%), without accounting for temporality and reverse causation, which is particularly relevant here as the majority of ENDS users are current or former smokers [1, 5, 47]. Furthermore, those with smoking-related medical conditions such as asthma, COPD and CVD are more likely to switch to ENDS to quit smoking [48]. Without accounting for the temporality of the exposure and outcome, as well as former smoking status, many study findings are inadequate for causal inferences.
Conventionally, guidelines and frameworks classify interventional studies such as RCTs as higher levels of evidence than observational ones. However, for lifestyle behaviours such as smoking and use of ENDS, RCTs are not common and the results would not necessarily be generalizable. Observational studies can provide useful information for the investigation of real-world interventions such as ENDS. This issue is not widely acknowledged in guidelines and frameworks used to rate the level of evidence, (e.g., by the NIH Quality Assessment Tools frameworks used in this study) [11].
Included studies were predominantly rated as being of poor quality. Studies that examined benefits to health outcomes had a relatively higher number of fair or good quality studies (75%) compared with those on harms alone (33%).
Definition of exposure
The definitions used for smoking and ENDS use varied tremendously and most studies relied on self-reported data for these exposures, which is known to underestimate their true prevalence [49]. Studies also asked children and adolescents in educational settings to self-report their use of cigarettes and ENDS, which are usually prohibited [50].
Studies with poor definitions of exposure failed to account for quantity, duration since quitting and duration of ENDS use, dual and former use of cigarettes and ENDS [17, 18, 21, 22, 39, 42], despite evidence that health outcomes from smoking are dose-dependent [51] Studies using data from the Population Assessment of Tobacco Health (PATH) and Behavioral Risk Factor Surveillance System datasets [18, 21, 26, 28, 43, 52] and others, [37, 40] defined respondents who had ever used a cigarette, other tobacco product or ENDS, even experimental use, as former or current users.
Standard definitions exist for smoking and both quantity and duration of smoking impact health outcomes [53]. Similar approaches should be used to quantify ENDS use. A handful of studies accounted for quantity, duration, dual and former use [16, 28, 38].
Definitions of outcomes
Both exposures and outcomes were self-reported in the majority of studies, and only 14 (38%) of studies utilized verified health outcomes data. Self-reporting of outcomes is known to be unreliable and prone to bias in some situations. Particularly problematic in this review were several studies that asked children and adolescents in educational settings to self-report on asthma and depressive symptoms both of which could have led to subjective and inaccurate responses [30,31,32, 34, 50, 54, 55].
Accounting for smoking status
One of the major design flaws was the failure to account for current, former and dual use of cigarettes [56,57,58] thereby ignoring that the majority of ENDS users do so to quit or cut down on cigarette smoking [56,57,58].
Several studies compared health risks for ENDS users with those of never smokers without accounting for former smoking in ENDS users. More meaningful comparisons in this regard would be between exclusive ENDS users who were never smokers against non-ENDS users who were never smokers. To quantify the benefit from switching, former smokers who now exclusively used ENDS should be compared with current smokers, accounting also for the duration of switching, duration of smoking and the quantity of cigarettes smoked.
Despite up to 70% of e-cigarette users reporting dual use, [8] studies did not routinely account for dual use when investigating risk from ENDS, thereby attributing health outcomes to ENDS use when they may have resulted from smoking cigarettes.
Temporality and reverse causation
Of included studies, 41% were cross-sectional and therefore unable to account for temporality and reverse causation, despite the fact that the majority of ENDS users are previous or current smokers [2, 6]. Furthermore, some health outcomes such as COPD and CVD can take up to decades to develop. Cross-sectional studies in current or former smokers cannot be used to establish temporal precedence as was reported in several studies, one of which has since been retracted [59]. Studies reporting on mental health. in particular, failed to account for reverse causation.
Publication bias
The ratio of studies on harm versus benefits was high with three-quarters of studies reporting only on harms, and less than a quarter reporting on benefits.
There was more frequent reporting of harmful health outcomes rather than neutral or beneficial ones in the abstract and text of the article [28].
The NIH framework has specific areas of critique, one of which is the search for publication bias in meta-analyses. There were no meta-analyses in this study, only one pooled cohort, and therefore, presence of publication bias was not noted.
Health outcomes
The majority of health outcomes studied were of respiratory (46%), CVD (22%), cancer (5%), oral health (3%) and mental health (19%).
Mortality
Overall mortality among smokers is three times higher than non-smokers in the US [60, 61], predominantly due to cancer, respiratory disease and CVD [62,63,64] and quitting before the age of 40 reduces smoking-related deaths by 90% [2, 62].
It is surprising to find that this is not reflected in the focus of research on harms from ENDS, with zero studies identified over the last 5 years. Whilst this may be partly due to the relatively recent availability of ENDS, it would be feasible to study mortality as an outcome in studies of high-risk groups such as CVD patients.
Cardiovascular disease
An extensive body of evidence shows that smoking tobacco is causally related to almost all major forms of CVD including accelerated atherosclerosis, acute MI, CHD, stroke, peripheral arterial disease (PAD), aortic aneurysm and sudden death [65, 66] and the benefits of quitting smoking on reduced risk for CHD and CVD mortality have been well documented [67,68,69,70,71].
We had expected to see more studies on the impact of switching from cigarette smoking to ENDS on CVD outcomes. The recent availability of ENDS may be partly responsible although other diseases such as COPD have been reported within the same timelines.
Our review found that ENDS product use has not been shown to be causative for harmful CVD outcomes and, indeed, has been shown to be beneficial for hypertensive patients. The finding from one large US cross-sectional study that dual e-cigarette and combustible cigarette users had higher CVD than smokers who had never used e-cigarettes falls outside of the overall findings, although this could be due to individuals with previous CVD being more likely to start using e-cigarettes as a means to reduce tobacco use. Further interrogation using longitudinal study design and longer follow-up should continue to further confirm the lack of harm.
Respiratory disease
Smoking is recognized as the most important cause of COPD [72] with a relative risk of dying of approximately 26 for men and 22 for women [66], and early quitting is associated with reduced morbidity and mortality[73]. Smoking has also been shown to increase the development of asthma, trigger asthma attacks and worsen outcomes of attacks [61, 74]. Other lung disorders that are causally linked with smoking include tuberculosis (TB) and idiopathic pulmonary fibrosis [61].
Cross-sectional designs are particularly problematic to investigate COPD as it usually takes several decades to develop [75] and because patients with COPD may be more likely to use quit aids such as e-cigarettes.
Despite mixed findings, studies judged to be of rigorous design (accounting for temporality, and former and current smoking) suggest that switching from cigarettes to e-cigarettes results in a reduction in exacerbations of COPD, with no evidence of long-term deterioration in lung function. The best evidence found no increased risk of asthma in ENDS users who were never smokers. There is a suggestion of short-term respiratory function changes in asthmatics using ENDS, but no evidence that it would translate to long-term impact.
Cancer
Smoking-related cancers have been extensively studied [76] and include the mouth, throat, nose, sinuses, oesophagus, bladder, kidney, ureter, pancreas, stomach, liver, cervix and ovary, bowel and acute myeloid leukaemia [77].
Only two studies on cancer were identified and the association of e-cigarettes in the causation of cancer has not been explored in clinical studies to any extent, which may in part be due to the lack of a plausible biological pathway.
Oral health
Oral cancer is the eleventh most common cancer worldwide [78], but oral health issues for ENDS have not been adequately studied.
Mental health
Particular aspects in mental health patients include high prevalence of both smoking and ENDS use [79,80,81], preliminary evidence that ENDS are highly effective for smoking cessation in this group [80], and that this group is more prone to addiction [82, 83] and struggle to quit nicotine in the longer term [79]. Furthermore, nicotine itself may have an impact on symptoms and progression of the mental health condition [84].
Seven studies investigating mental health outcomes were identified in this review, but there were others reporting on mental health disease as a predictor of ENDS use [85, 86]. Interventional and longitudinal study designs are critical due to the bi-directional link between mental health disorders and ENDS use. Of two longitudinal studies in our review, one showed no deterioration in depressive symptoms and the other showed some deterioration, so no conclusion can be reached. Further studies are urgently required that are interventional in design and to investigate other health outcomes of switching from cigarettes to ENDS in this patient group.
Informing policy
The findings of our review have implications for policy makers. Our review found that very few studies were sufficiently rigorous to form conclusions on health risks and were not rigorous enough to inform policy on tobacco harm reduction.
The European Commission published recently stated strong weight of evidence for risks of long-term systemic effects for CVD, respiratory cancers and poisoning and injuries; moderate for respiratory tract irritative damage and that other long-term adverse health effects, such as pulmonary disease, central nervous system and repro-toxic effects, cannot be established due to lack of consistent data [87]. Current European policies requires packaging for ENDS products to report the same information on toxicity and addictiveness as for cigarettes and tobacco products [88]. The findings of our review do not support these conclusions and should form part of the scientific basis for such policies.
Several of the studies included in this review that were neither high level of evidence nor of ‘good’ quality have nevertheless been influential in determining health policy. One such study [59] found that current e-cigarette users were twice as likely as never users to have had a MI. However, a subsequent re-analysis of the data [89] found that the majority of the MI outomes had preceded, on average by a decade, the first use of e-cigarettes [90]. Despite being retracted by the publishing journal [91], the article had already been widely disseminated [92] and cited [93], with potential lasting impacts on the perception of CVD health risks from the use of e-cigarettes.
Another invalid health scare informing policy from the use of ENDS occurred in 2019 with the “EVALI” outbreak which was initially widely reported as an outbreak of lipoid pneumonia due to vaping of nicotine [94]. It was soon recognised and reported as being due to vaping of black-market cannabinoid (THC) oils rather than vaping of nicotine, with the CDC in the US recommending that adults using nicotine-containing e-cigarette or vaping products as an alternative to cigarettes should continue and not go back to smoking [94].
The general public’s perception of health risks from ENDS does not reflect the available evidence and has become more negative according to the findings from two large surveys [95], whose authors underscored the urgent need to accurately communicate the risks of e-cigarettes to the public, which should clearly differentiate the absolute from the relative (to smoking) harms of e-cigarettes.
Strengths and Limitations
We considered a MA of studies included in our review to be inappropriate, partly due to the common methodological flaws highlighted above and the vast heterogeneity between studies, for example in the definitions used for the exposure variable of ENDS use, and with regards to accounting for dual use, former use, duration and quantity of use.
We sought to identify only those articles where the main research question was on disease end-points from use of ENDS (not including heat-not-burn devices). The key disease end-points under investigation were mortality, CVD, respiratory and cancer as these make up the major health concerns from ENDS. We also searched for general health outcomes to identify the breadth of health outcomes being reported. There may be other research studies where health outcome was a secondary research question or fell outside of our search terms which may not have been captured in our study.
We were unable to study the differential impact from various types of ENDS products and different constituent compounds (e.g., in nicotine fluid). In addition, different types of ENDS have different levels of nicotine delivery and addictive properties, which are likely to change the harmful effects (from components other than nicotine) of any product due to type of use (e.g. magnitude, time, etc.).
The individual studies synthesized for our review may also have been included in meta-analyses that were included. This should be acknowledged, however, as we did not ourselves conduct pooling of results, we do not regard this as problematic.
Finally, the search strategy results were limited to English language reports, and there is a risk that potentially relevant studies reporting health outcomes with ENDS use were subsequently not included.
Conclusion
To determine the net health impact of ENDs, the benefits of quitting smoking must be weighed against any harms (or benefits) from the use of ENDS. The wider impacts from the use of ENDS on society, such as new uptake in never smokers and nicotine addiction, must also be factored in, which were outside of the scope of this review.
Our review suggests the majority of studies on the use of ENDS products reported on negative health impacts with few reporting on health outcomes from switching from cigarettes to e-cigarettes. Future studies will need to prioritise an exploration of both potential harms and benefits. The strength of evidence and quality of the published studies is generally poor, yet some of these studies have been used to inform policy and are likely to have influenced public perception of health risks from the use of ENDS.
Our review has not demonstrated evidence that ENDS use is causative for any harmful CVD outcomes, and to the contrary, may be beneficial for hypertensive patients. Switching from cigarettes to e-cigarettes resulted in reduced exacerbations of COPD, with no evidence of long-term respiratory harm or deterioration in lung function. There was a suggestion from one study of short-term reductions in respiratory function in asthmatics, but no increased risk of asthma in ENDS users has been shown. Other health outcomes such as mental health, cancer and mortality have not been adequately studied to form a consensus on the health impact from ENDS use. However, the findings of our review did not negate the consensus held by many that ENDS use is safer than the risks posed from smoking cigarettes.
Overall, our review found very few studies were sufficiently rigorous to form conclusions on health risks. The research on ENDS use is not yet adequate to provide quantitative estimates about health risks. Consequently, the current body of evidence is inadequate for informing policy around tobacco harm reduction.
Abbreviations
- ADHD:
-
Attention-deficit hyperactivity disorder
- BMI:
-
Body mass index
- CAT:
-
COPD assessment test
- CAD:
-
Coronary artery disease
- CHD:
-
Coronary heart disease
- COPD:
-
Chronic obstructive pulmonary disease
- CVD:
-
Cardiovascular disease
- DBP:
-
Diastolic blood pressure
- ENDS:
-
Electronic nicotine delivery systems
- EC:
-
Electronic cigarette
- HR:
-
Heart rate
- MA:
-
Meta-analysis
- MI:
-
Myocardial infarction
- NASEM:
-
National Academies of Sciences, Engineering and Medicine
- NIH:
-
National Institutes for Health
- PAD:
-
Peripheral arterial disease
- PATH:
-
Population Assessment of Tobacco Health
- PTSD:
-
Post-traumatic stress disorder
- RCT:
-
Randomized controlled trial
- SBP:
-
Systolic blood pressure
- TB:
-
Tuberculosis
- THR:
-
Tobacco harm reduction
References
World Health Organization (2020) Tobacco: Key facts. https://www.who.int/news-room/fact-sheets/detail/tobacco Accessed 5 August 2020
McNeill A et al (2018) Evidence review of e-cigarettes and heated tobacco products 2018. A report commissioned by Public Health England. Public Health England, London
Public Health England (2015) E-cigarettes: an evidence update. https://www.gov.uk/government/publications/e-cigarettes-an-evidence-update Accessed 6 August 2020
Hajek P et al (2019) A randomized trial of E-Cigarettes versus nicotine-replacement therapy. N Engl J Med 380:629–637. https://doi.org/10.1056/nejmoa1808779
Mcrobbie H, Bullen C, Hartmann-Boyce J, Hajek P (2014) Electronic cigarettes for smoking cessation and reduction. Cochrane Database of Syst Rev 12:CD010216. https://doi.org/10.1002/14651858.cd010216.pub2
QuickStats (2016) Cigarette smoking status among current adult e-cigarette users, by age group—national health interview survey United States. MMWR Morb Mortal Wkly Rep 65:1177. https://doi.org/10.15585/mmwr.mm6542a7
Public Health England (2015) E-cigarettes: an evidence update GOV.UK https://www.gov.uk/government/publications/e-cigarettes-an-evidence-update Accessed 8 August 2020
National Academies of Sciences, Engineering, and Medicine (2018) Public health consequences of e-cigarettes. The National Academies Press, Washington, DC
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. Open Med 3:e123-130
Center for Evidence-Based Medicine (2009) Oxford Centre for Evidence-based Medicine – Levels of Evidence. https://www.cebm.net/2009/06/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/ Accessed 4 January 2020
NIH (2017) Study Quality Assessment Tools. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools Accessed 8 March 2020
Carter T, Tucker D, Kilic A, Papadimos T, Barlow A, Berry E (2017) Life-threatening vesicular bronchial injury requiring veno-venous extracorporeal membrane oxygenation rescue in an electronic nicotine delivery system user. Clin Pract Cases Emerg Med 1:212–217. https://doi.org/10.5811/cpcem.2017.3.33171
Khan M, Khateeb F, Akhtar J et al (2018) Organizing pneumonia related to electronic cigarette use: a case report and review of literature. Clin Respir J 12:1295–1299. https://doi.org/10.1111/crj.12775
Sommerfeld CG, Weiner DJ, Nowalk A, Larkin A (2018) Hypersensitivity pneumonitis and acute respiratory distress syndrome from e-cigarette use. Pediatrics. https://doi.org/10.1542/peds.2016-3927
Nguyen H, Kitzmiller J, Nguyen K, Nguyen C, Chi Bui T (2017) Oral carcinoma associated with chronic use of electronic cigarettes. Otolaryngol. https://doi.org/10.4172/2161-119x.1000304
Polosa R, Morjaria J, Caponnetto P et al (2016) Blood pressure control in smokers with arterial hypertension who switched to electronic cigarettes. Int J Environ Res Public Health 13:1123. https://doi.org/10.3390/ijerph13111123
Farsalinos K, Cibella F, Caponnetto P et al (2016) Effect of continuous smoking reduction and abstinence on blood pressure and heart rate in smokers switching to electronic cigarettes. Intern Emerg Med 11:85–94. https://doi.org/10.1007/s11739-015-1361-y
Osei A, Mirbolouk M, Orimoloye O et al (2019) Association between e-cigarette use and cardiovascular disease among never and current combustible-cigarette smokers. Am J Med 132:949-954.e2. https://doi.org/10.1016/j.amjmed.2019.02.016
Farsalinos K, Polosa R, Cibella F, Niaura R (2019) Is e-cigarette use associated with coronary heart disease and myocardial infarction? Insights from the 2016 and 2017 National Health Interview Surveys. Ther Adv Chronic Dis 10:204062231987774. https://doi.org/10.1177/2040622319877741
Alzahrani T, Pena I, Temesgen N, Glantz S (2018) Association between electronic cigarette use and myocardial infarction. Am J Prev Med 55:455–461. https://doi.org/10.1016/j.amepre.2018.05.004
Parekh T, Pemmasani S, Desai R (2020) Risk of stroke with e-cigarette and combustible cigarette use in young adults. Am J Prev Med 58:446–452. https://doi.org/10.1016/j.amepre.2019.10.008
Bowler R, Hansel N, Jacobson S et al (2017) Electronic cigarette use in US adults at risk for or with COPD: analysis from two observational cohorts. J Gen Intern Med 32:1315–1322. https://doi.org/10.1007/s11606-017-4150-7
Polosa R, Morjaria J, Caponnetto P et al (2016) Evidence for harm reduction in COPD smokers who switch to electronic cigarettes. Respir Res 17:166. https://doi.org/10.1186/s12931-016-0481-x
Polosa R, Morjaria J, Prosperini U et al (2018) Health effects in COPD smokers who switch to electronic cigarettes: a retrospective-prospective 3-year follow-up. Int J Chron Obstruct Pulmon Dis 13:2533–2542. https://doi.org/10.2147/copd.s161138
Osei A, Mirbolouk M, Orimoloye O et al (2016) Association between e-cigarette use and chronic obstructive pulmonary disease by smoking status: behavioral risk factor surveillance system 2016 and 2017. Am J Prev Med 58:336–342. https://doi.org/10.1016/j.amepre.2019.10.014
Perez M, Atuegwu N, Mead E, Oncken C, Mortensen E (2019) Adult e-cigarettes use associated with a self-reported diagnosis of COPD. Int J Environ Res Public Health 16:3938. https://doi.org/10.3390/ijerph16203938
Wills T, Pagano I, Williams R, Tam E (2019) E-cigarette use and respiratory disorder in an adult sample. Drug Alcohol Depend 194:363–370
Xie Z, Ossip D, Rahman I, Li D (2019) Use of electronic cigarettes and self-reported chronic obstructive pulmonary disease diagnosis in adults. Nicotine Tob Res 22:1155–1161. https://doi.org/10.1093/ntr/ntz234
Lokke A, Lange P, Scharling H, Fabricius P, Vestbo J (2006) Developing COPD: a 25 year follow up study of the general population. Thorax 61:935–939. https://doi.org/10.1136/thx.2006.062802
Cho J, Paik S (2016) Association between electronic cigarette use and asthma among high school students in South Korea. PLoS ONE 11:e0151022. https://doi.org/10.1371/journal.pone.0151022
Choi K, Bernat D (2016) E-cigarette use among Florida youth with and without asthma. Am J Prev Med 51:446–453. https://doi.org/10.1016/j.amepre.2016.03.010
Kim S, Sim S, Choi H (2017) Active, passive, and electronic cigarette smoking is associated with asthma in adolescents. Sci Rep 7:17789. https://doi.org/10.1038/s41598-017-17958-y
Lappas A, Tzortzi A, Konstantinidi E et al (2017) Short-term respiratory effects of e-cigarettes in healthy individuals and smokers with asthma. Respirology 23:291–297. https://doi.org/10.1111/resp.13180
Schweitzer R, Wills T, Tam E, Pagano I, Choi K (2017) E-cigarette use and asthma in a multiethnic sample of adolescents. Prev Med 105:226–231. https://doi.org/10.1016/j.ypmed.2017.09.023
Astrid Miler J, Mayer B (2016) Changes in the frequency of airway infections in smokers who switched to vaping: results of an online survey. J Addict Res Ther. https://doi.org/10.4172/2155-6105.1000290
Franco T, Trapasso S, Puzzo L, Allegra E (2016) Electronic cigarette: role in the primary prevention of oral cavity cancer. Clin Med Insights Ear Nose Throat 9:1. https://doi.org/10.4137/cment.s40364
Bandiera F, Loukas A, Li X, Wilkinson A, Perry C (2017) Depressive symptoms predict current e-cigarette use among college students in Texas. Nicotine Tob Res 19:1102–1106. https://doi.org/10.1093/ntr/ntx014
Lechner W, Janssen T, Kahler C, Audrain-McGovern J, Leventhal A (2017) Bi-directional associations of electronic and combustible cigarette use onset patterns with depressive symptoms in adolescents. Prev Med 96:73–78. https://doi.org/10.1016/j.ypmed.2016.12.034
Dahal R, Adhikari K, Patten S (2020) Smoking cessation and improvement in mental health outcomes: Do people who quit smoking by switching to electronic cigarettes experience improvement in mental health? Can J Psychiatry 65:512–514. https://doi.org/10.1177/0706743720917775
King J, Reboussin B, Spangler J, Cornacchione Ross J, Sutfin E (2018) Tobacco product use and mental health status among young adults. Addict Behav 77:67–72. https://doi.org/10.1016/j.addbeh.2017.09.012
Chadi N, Li G, Cerda N, Weitzman E (2019) Depressive symptoms and suicidality in adolescents using e-cigarettes and marijuana: a secondary data analysis from the youth risk behavior survey. J Addict Med 13:362–365. https://doi.org/10.1097/adm.0000000000000506
Pham T, Williams J, Bhattarai A, Dores A, Isherwood L, Patten S (2020) Electronic cigarette use and mental health: a Canadian population-based study. J Affect Disord 260:646–652. https://doi.org/10.1016/j.jad.2019.09.026
Akinkugbe A (2018) Cigarettes, E-cigarettes, and adolescents’ oral health: findings from the population assessment of tobacco and health (PATH) study. JDR Clin Trans Res 4:276–283. https://doi.org/10.1177/2380084418806870
Lanza H, Pittman P, Batshoun J (2017) Obesity and cigarette smoking: extending the link to e-cigarette/vaping use. Am J Health Behav 41:338–347. https://doi.org/10.5993/ajhb.41.3.13
Miler J, Hajek P (2017) Resolution of recurrent tonsillitis in a non-smoker who became a vaper. a case study and new hypothesis. Med Hypotheses 109:17–18. https://doi.org/10.1016/j.mehy.2017.09.006
Maridet C, Atge B, Amici J, Taïeb A, Milpied B (2015) The electronic cigarette: the new source of nickel contact allergy of the 21st century? Contact Derm 73:49–50. https://doi.org/10.1111/cod.12373
Adkison SE et al (2013) Electronic nicotine delivery systems: international tobacco control four-country survey. Am J Prev Med 44(3):207–215
Kruse G, Kalkhoran S, Rigotti N (2017) Use of electronic cigarettes among U.S. adults with medical comorbidities. Am J Prev Med 52:798–804. https://doi.org/10.1016/j.amepre.2016.12.004
Gorber S, Schofield-Hurwitz S, Hardt J, Levasseur G, Tremblay M (2009) The accuracy of self-reported smoking: a systematic review of the relationship between self-reported and cotinine-assessed smoking status. Nicotine Tob Res 11:12–24. https://doi.org/10.1093/ntr/ntn010
Vingilis E, Wade T, Seeley J (2002) Predictors of adolescent self-rated health. Can J Public Health 93:193–197. https://doi.org/10.1007/bf03404999
Inoue-Choi M et al (2020) Dose-response association of low-intensity and nondaily smoking with mortality in the United States. JAMA Netw Open 3(6):e206436
Bhatta DN, Glantz SA (2020) Association of e-cigarette use with respiratory disease among adults: a longitudinal analysis. Am J Prev Med 58(2):182–190
Centers for Disease Control and Prevention (2017) Adult Tobacco Use Information https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm Accessed 5 August 2020
Grant J, Lust K, Chamberlain S (2019) Hallucinogen use is associated with mental health and addictive problems and impulsivity in university students. Addict Behav Rep 10:100228. https://doi.org/10.1016/j.abrep.2019.100228
Chadi N et al (2019) Depressive symptoms and suicidality in adolescents using e-cigarettes and marijuana: a secondary data analysis from the youth risk behavior survey. J Addict Med 13(5):362–365
Boyle R, Richter S, Helgertz S (2019) Who is using and why: prevalence and perceptions of using and not using electronic cigarettes in a statewide survey of adults. Addict Behav Rep 10:100227. https://doi.org/10.1016/j.abrep.2019.100227
Filippidis F, Laverty A, Gerovasili V, Vardavas C (2016) Two-year trends and predictors of e-cigarette use in 27 European Union member states. Tob Control 26:98–104. https://doi.org/10.1136/tobaccocontrol-2015-052771
Kinouani S et al (2020) Motivations for using electronic cigarettes in young adults: a systematic review. Subst Abus 41:315–322. https://doi.org/10.1080/08897077.2019.1671937
Bhatta D, Glantz S (2019) Electronic cigarette use and myocardial infarction among adults in the us population assessment of tobacco and health. J Am Heart Assoc 8:12. https://doi.org/10.1161/jaha.119.012317
Centers for Disease Control and Prevention (2020) Tobacco-Related Mortality. https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/tobacco_related_mortality/index.html Accessed 6 August 2020
US National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health (2014) The health consequences of smoking—50 years of progress: a report of the surgeon general
Jha P, Ramasundarahettige C, Landsman V et al (2013) 21st-century hazards of smoking and benefits of cessation in the United States. N Engl J Med 4:341–350. https://doi.org/10.1056/nejmsa1211128
US Office of the Surgeon General, and Office on Smoking and Health (2004) The health consequences of smoking: a report of the surgeon general
National Cancer Institute (1998) Cigars: Health Effects and Trends. Smoking and Tobacco Control Monograph No. 9. Bethesda (MD): U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Accessed 6 August 2020
US Department of Health and Human Services (2014) Surgeon general’s report: the health consequences of smoking—50 years of progress. Public Health Service, Office of the Surgeon General, Rockville
Thun M, Carter B, Feskanich D et al (2013) 50-year trends in smoking-related mortality in the United States. N Engl J Med 4:351–364. https://doi.org/10.1056/nejmsa1211127
Samet J (1990) The 1990 report of the surgeon general: the health benefits of smoking cessation. Am Rev Respir Dis 5:993–994. https://doi.org/10.1164/ajrccm/142.5.993
US Surgeon General (2004) The health consequences of smoking: a report of the Surgeon General. Atlanta. GA: Center for Disease Control and Prevention. Office of Smoking and Health. http://www.cdc.gov/tobacco/data_statistics/sgr/sgr_2004/chapters.htm
US Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion (US), and Office on Smoking and Health (US) (2010) How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General.
Anthonisen N (2005) The effects of a smoking cessation intervention on 14.5-year mortality. Ann Intern Med 8:615. https://doi.org/10.7326/0003-4819-143-8-200510180-00019
Vollset S, Tverdal A, Gjessing H (2006) Smoking and deaths between 40 and 70 years of age in women and men. Ann Intern Med 6:381. https://doi.org/10.7326/0003-4819-144-6-200603210-00004
US Department of Health, Education, and Welfare [USDHEW] (1964) p. 31
Pride NB (2001) Smoking cessation: effects on symptoms, spirometry and future trends in Copd. Thorax 56:ii7-10
US Department of Health and Human Service (2010) How Tobacco Smoke Causes Disease: What It Means to You. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
Lokke A, Lange P, Scharling H, Fabricius P, Vestbo J (2006) Developing COPD: a 25 year follow up study of the general population. Thorax 11:935–939. https://doi.org/10.1136/thx.2006.062802
Doll R, Hill A (1954) The mortality of doctors in relation to their smoking habits. BMJ 4877:1451–1455. https://doi.org/10.1136/bmj.1.4877.1451
Smoke, Tobacco, and Involuntary Smoking (2004) IARC monographs on the evaluation of carcinogenic risks to humans. IARC 1–1452
World Health Organization (2017) Global facts on tobacco or oral health https://www.who.int/oral_health/publications/fact_sheet_tobacco/en/index1.html Accessed 6 August 2020
Spears CA et al (2019) Electronic nicotine delivery system (Ends) use in relation to mental health conditions, past-month serious psychological distress and cigarette smoking status, 2017. Addiction 114:315–325
Cummins SE et al (2014) Use of E-cigarettes by individuals with mental health conditions. Tob Control 23:iii48-53
Spears C, Jones D, Weaver S, Yang B, Pechacek T, Eriksen M (2018) Electronic nicotine delivery system (ENDS) use in relation to mental health conditions, past-month serious psychological distress and cigarette smoking status, 2017. Addiction 114:315–325. https://doi.org/10.1111/add.14464
Goodkind M, Eickhoff S, Oathes D et al (2015) Identification of a common neurobiological substrate for mental illness. JAMA Psychiat 72:305. https://doi.org/10.1001/jamapsychiatry.2014.2206
Dome P, Lazary J, Kalapos M, Rihmer Z (2010) Smoking, nicotine and neuropsychiatric disorders. Neurosci Biobehav Rev 34:295–342. https://doi.org/10.1016/j.neubiorev.2009.07.013
Brown J, Gartner C, Carter A (2019) Can e-cigarettes improve the well-being of people with mental health disorders? Int J Drug Policy 73:170–171. https://doi.org/10.1016/j.drugpo.2019.07.028
Riehm K, Young A, Feder K et al (2019) Mental health problems and initiation of e-cigarette and combustible cigarette use. Pediatrics 144:e20182935. https://doi.org/10.1542/peds.2018-2935
Park S, Lee L, Shearston J, Weitzman M (2017) Patterns of electronic cigarette use and level of psychological distress. PLoS ONE 12:e0173625. https://doi.org/10.1371/journal.pone.0173625
Scientific Committee on Health, Environmental and Emerging Risks SCHEER Preliminary Opinion on electronic cigarettes (2020) https://ec.europa.eu/health/sites/health/files/scientific_committees/scheer/docs/scheer_o_017.pdf Accessed 1 October 2020
Article 20 of the Tobacco Products Directive (2014/40/EU). https://ec.europa.eu/health/tobacco/ecigarettes_en Accessed 12 October 2020.
Population Assessment of Tobacco Health (PATH). https://pathstudyinfo.nih.gov/UI/HomeMobile.aspx Accessed 6 August, 2020
Rodu, B (2019) Comment: Electronic Cigarette Use and Myocardial Infarction Among Adults in the US Population Assessment of Tobacco and Health. https://pubpeer.com/publications/F177153E02CA8B3E7B9E70BC8DB204 Accessed 6 August 2020
Retraction to: Electronic Cigarette Use and Myocardial Infarction Among Adults in the US Population Assessment of Tobacco and Health. https://www.ahajournals.org/doi/https://doi.org/10.1161/JAHA.119.014519. Accessed 6 August, 2020
Glantz, SA (2019) More evidence that e-cigs cause heart attacks, this time from PATH. Center for Tobacco Control Research and Education, University of California San Francisco https://tobacco.ucsf.edu/more-evidence-e-cigs-cause-heart-attacks-time-path
Google Scholar. Citations: Electronic cigarette use and myocardial infarction among adults in the US population assessment of tobacco and health. https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=stanton+glantz+myocardial+infarction+2019&btnG Accessed 7 August 2020
Centers for Disease Control and Prevention. Smoking and Tobbaco Use: For Healthcare Providers. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease/healthcare-providers/index.html Accessed 6 August 2020
Huang J, Feng B, Weaver S, Pechacek T, Slovic P, Eriksen M (2019) Changing perceptions of harm of e-cigarette vs cigarette use among adults in 2 US national surveys from 2012 to 2017. JAMA Netw Open 2:e191047. https://doi.org/10.1001/jamanetworkopen.2019.1047
Funding
Open access funding provided by Università degli Studi di Catania within the CRUI-CARE Agreement. This investigator initiated review was sponsored by ECLAT srl, a spin off of the University of Catania, through a grant from the Foundation for a Smoke-Free World, a US nonprofit 501 (c) (3) private foundation with a mission to end smoking in this generation. The Foundation accepts charitable gifts from PMI Global Services Inc.; under the Foundation’s Bylaws and Pledge Agreement with PMI Global Services Inc., the Foundation is independent from PMI Global Services Inc. and the tobacco industry. The contents, selection, and presentation of facts, as well as any opinions expressed herein are the sole responsibility of the authors and under no circumstances shall be regarded as reflecting the positions of the Foundation for a Smoke-Free World, Inc. ECLAT srl. is a research based company from the University of Catania that delivers solutions to global health problems with special emphasis on harm minimization and technological innovation.
Author information
Authors and Affiliations
Contributions
CH, ES and RP designed the study, conducted data extraction, analysis and review. CH and ES wrote the manuscript; SS, RN, PT and RP reviewed and edited the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
CH received reimbursement from ECLAT for research conducted on tobacco harm reduction (2019–2020) including this article; she has served as a paid member of the advisory panel for the Tobacco Transformation Index (contracted by Sustainability, Sept 2019–April 2020); she is a paid consultant to TEVA pharmaceuticals on work related to multiple chronic conditions (2017 to present). ES received reimbursement from ECLAT for research conducted on tobacco harm reduction (2019–2020) including this article. SS has no conflict of interest to declare. RN has no affiliation with, nor does he accept funding from any tobacco, nicotine or vaping commercial or charitable interests including the FSFW. PF has no conflict of interest to declare. RP is full tenured professor of Internal Medicine at the University of Catania (Italy) and Medical Director of the Institute for Internal Medicine and Clinical Immunology at the same University. In relation to his recent work in the area of respiratory diseases, clinical immunology, and tobacco control, RP has received has received lecture fees and research funding from Pfizer, GlaxoSmithKline, CV Therapeutics, NeuroSearch A/S, Sandoz, MSD, Boehringer Ingelheim, Novartis, Duska Therapeutics, and Forest Laboratories. Lecture fees from a number of European EC industry and trade associations (including FIVAPE in France and FIESEL in Italy) were directly donated to vaper advocacy no-profit organizations. RP has also received grants from European Commission initiatives (U-BIOPRED and AIRPROM) and from the Integral Rheumatology & Immunology Specialists Network (IRIS) initiative. He has also served as a consultant for Pfizer, Global Health Alliance for treatment of tobacco dependence, CV Therapeutics, Boehringer Ingelheim, Novartis, Duska Therapeutics,ECITA (Electronic Cigarette Industry Trade Association, in the UK), Arbi Group Srl., Health Diplomats, and Sermo Inc. RP has served on the Medical and Scientific Advisory Board of Cordex Pharma, Inc., CV Therapeutics, Duska Therapeutics Inc, Pfizer, and PharmaCielo. RP is also founder of the Center for Tobacco prevention and treatment (CPCT) at the University of Catania and of the Center of Excellence for the acceleration of Harm Reduction (CoEHAR) at the same University, which has received support from Foundation for a Smoke Free World to conduct 8 independent investigator-initiated research projects on harm reduction. RP currently involved in a patent application concerning an app tracker for smoking behaviour developed for ECLAT Srl. RP is also currently involved in the following pro bono activities: scientific advisor for LIAF, Lega Italiana Anti Fumo (Italian acronym for Italian Anti-Smoking League), the Consumer Advocates for Smoke-free Alternatives (CASAA) and the International Network of Nicotine Consumers Organizations (INNCO); Chair of the European Technical Committee for standardization on “Requirements and test methods for emissions of electronic cigarettes” (CEN/TC 437; WG4).
Human and animal rights statement
This review does not contain any studies directly involving participants or animals.
Informed consent
Formal consent is not required for a review.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Table 5.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hajat, C., Stein, E., Shantikumar, S. et al. A scoping review of studies on the health impact of electronic nicotine delivery systems. Intern Emerg Med 17, 241–268 (2022). https://doi.org/10.1007/s11739-021-02835-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-021-02835-4