
Abstract
Background
This investigation assesses the learning curve for dedicated bedside assistance at a facility that recently adopted robot-assisted rectal resection.
Methods
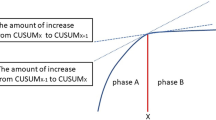
Data from patients with rectal cancer who underwent robotic rectal resections from September 2019 through April 2020 were retrospectively analyzed. Before starting robotic surgery, we set the rule that a console surgeon would not enter the sterile field and all of those maneuvers would be left to a dedicated physician. Docking time was analyzed using the cumulative sum (CUSUM) method to evaluate the learning curve. Different phases in the learning curve were identified according to CUSUM plot configuration. A comparison was made of phases 1 and 2 combined, and phase 3.
Result
The procedures were performed in 30 patients. Median docking time, console time was 13 min. A total of nine patients had histories of abdominal surgery. CUSUM analysis of docking time demonstrated 3 phases. Each docking time was longer in Phase 1 (the first 3 cases) than the average docking time over the all cases. The docking time in Phase 2 (the 9 middle cases) approximated the average time over the all cases. Phase 3 (the remaining 18 cases) showed further improvement of the docking procedure and time was reduced. A comparison of Phases 1 and 2 combined, and Phase 3, revealed that Phase 3 had a significantly higher rate of history of abdominal surgery.
Conclusion
Docking manipulation proficiency was achieved in approximately 10 cases without the influence of surgical difficulty.





Similar content being viewed by others


References
Walliczek-Dworschak U, Mandapathil M, Förtsch A, Teymoortash A, Dworschak P, Werner JA, Güldner C (2017) Structured training on the da Vinci Skills Simulator leads to improvement in technical performance of robotic novices. Clin Otolaryngol 42(1):71–80. https://doi.org/10.1111/coa.12666
Simorov A, Reynoso JF, Dolghi O, Thompson JS, Oleynikov D (2011) Comparison of perioperative outcomes in patients undergoing laparoscopic versus open abdominoperineal resection. Am J Surg 202:666–670 (discussion 670-662)
Fleshman J, Branda M, Sargent DJ, Boller AM, George V, Abbas M, Peters WR Jr, Maun D, Chang G, Herline A, Fichera A, Mutch M, Wexner S, Whiteford M, Marks J, Birnbaum E, Margolin D, Larson D, Marcello P, Posner M, Read T, Monson J, Wren SM, Pisters PW, Nelson H (2015) Effect of laparoscopic-assisted resection vs open resection of stage II or III rectal cancer on pathologic outcomes: the ACOSOG Z6051 Randomized Clinical Trial. JAMA 314:1346–1355
Stevenson AR, Solomon MJ, Lumley JW, Hewett P, Clouston AD, Gebski VJ, Davies L, Wilson K, Hague W, Simes J (2015) Effect of laparoscopic-assisted resection vs open resection on pathological outcomes in rectal cancer: the ALaCaRT Randomized Clinical Trial. JAMA 314:1356–1363
Kayano H, Okuda J, Tanaka K, Kondo K, Tanigawa N (2011) Evaluation of the learning curve in laparoscopic low anterior resection for rectal cancer. Surg Endosc 25:2972–2979
Kim YW, Lee HM, Kim NK, Min BS, Lee KY (2012) The learning curve for robot-assisted total mesorectal excision for rectal cancer. Surg Laparosc Endosc Percutaneous Tech 22:400–405
Kamali D, Reddy A, Imam S, Omar K, Jha A, Jha M (2017) Short-term surgical outcomes and patient quality of life between robotic and laparoscopic extralevator abdominoperineal excision for adenocarcinoma of the rectum. Ann R Coll Surg Engl 99:607–613
Odermatt M, Ahmed J, Panteleimonitis S, Khan J, Parvaiz A (2017) Prior experience in laparoscopic rectal surgery can minimise the learning curve for robotic rectal resections: a cumulative sum analysis. Surg Endosc 31:4067–4076
Lai F, Entin E (2005) Robotic Surgery and the Operating Room Team. In: Proceedings of the Human Factors and Ergonomics Society Annual Meeting 49: 1070–1073
Catchpole K, Mishra A, Handa A, McCulloch P (2008) Teamwork and error in the operating room: analysis of skills and roles. Ann Surg 247:699–706
McCrorey M, Kitahara H, Krienbring D, Patel B, Nisivaco S, Balkhy HH (2020) Robotic cardiac surgery impact of a new patient-side assistant on outcomes. Gen Thorac Cardiovasc Surg 68:24–29
Nayyar R, Yadav S, Singh P, Dogra PN (2016) Impact of assistant surgeon on outcomes in robotic surgery. Indian J Urol IJU 32:204–209
Potretzke AM, Knight BA, Brockman JA, Vetter J, Figenshau RS, Bhayani SB, Benway BM (2016) The role of the assistant during robot-assisted partial nephrectomy: does experience matter? J Robot Surg 10:129–134
Sgarbura O, Vasilescu C (2010) The decisive role of the patient-side surgeon in robotic surgery. Surg Endosc 24:3149–3155
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Bokhari MB, Patel CB, Ramos-Valadez DI, Ragupathi M, Haas EM (2011) Learning curve for robotic-assisted laparoscopic colorectal surgery. Surg Endosc 25:855–860
Sng KK, Hara M, Shin JW, Yoo BE, Yang KS, Kim SH (2013) The multiphasic learning curve for robot-assisted rectal surgery. Surg Endosc 27:3297–3307
Park EJ, Kim CW, Cho MS, Baik SH, Kim DW, Min BS, Lee KY, Kim NK (2014) Multidimensional analyses of the learning curve of robotic low anterior resection for rectal cancer: 3-phase learning process comparison. Surg Endosc 28:2821–2831
Park EJ, Kim CW, Cho MS, Kim DW, Min BS, Baik SH, Lee KY, Kim NK (2014) Is the learning curve of robotic low anterior resection shorter than laparoscopic low anterior resection for rectal cancer?: a comparative analysis of clinicopathologic outcomes between robotic and laparoscopic surgeries. Medicine 93:e109
Foo CC, Law WL (2016) The learning curve of robotic-assisted low rectal resection of a novice rectal surgeon. World J Surg 40:456–462
Kawai K, Hata K, Tanaka T, Nishikawa T, Otani K, Murono K, Sasaki K, Kaneko M, Emoto S, Nozawa H (2018) Learning curve of robotic rectal surgery with lateral lymph node dissection: cumulative sum and multiple regression analyses. J Surg Educ 75:1598–1605
van der Schans EM, Hiep MAJ, Consten ECJ, Broeders I (2020) From Da Vinci Si to Da Vinci Xi: realistic times in draping and docking the robot. J Robot Surg 14:835–839
Abrishami P, Boer A, Horstman K (2014) Understanding the adoption dynamics of medical innovations: affordances of the da Vinci robot in the Netherlands. Soc Sci Med (1982) 117:125–133
Kanda Y (2013) Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant 48:452–458
Katsuno H, Hanai T, Masumori K, Koide Y, Ashida K, Matsuoka H, Tajima Y, Endo T, Mizuno M, Cheong Y, Maeda K, Uyama I (2020) Robotic surgery for rectal cancer: operative technique and review of the literature. J Anus Rectum Colon 4:14–24
Jiménez-Rodríguez RM, Díaz-Pavón JM, de la Portilla de Juan F, Prendes-Sillero E, Dussort HC, Padillo J (2013) Learning curve for robotic-assisted laparoscopic rectal cancer surgery. Int J Colorectal Dis 28:815–821
Randell R, Greenhalgh J, Hindmarsh J, Honey S, Pearman A, Alvarado N, Dowding D (2021) How do team experience and relationships shape new divisions of labour in robot-assisted surgery? A realist investigation. Health (London) 25(2):250–268. https://doi.org/10.1177/1363459319874115
Acknowledgements
The authors would like to thank the departmental theater nurses, at the Gunma Cancer Center,—Nurse Umezawa, Nurse Yamazaki, Nurse Iwase, Nurse Mogi and Nurse Arashiguchi—for their generous cooperation for the creation of a new medical team.
Author information
Authors and Affiliations
Contributions
Research conception/design: KY. Drafting of manuscript: KY. Data acquisition: NK. Data analysis/interpretation: KY. Manuscript preparation final approval: HO.
Corresponding author
Ethics declarations
Conflict of interest
Author Kazunosuke Yamada, Author Norimichi Kogure, and Author Hitoshi Ojima declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yamada, K., Kogure, N. & Ojima, H. Learning curve for robotic bedside assistance for rectal cancer: application of the cumulative sum method. J Robotic Surg 16, 1027–1035 (2022). https://doi.org/10.1007/s11701-021-01322-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-021-01322-4