
Abstract
Parkinson’s Disease (PD) is hallmarked by dysfunctional circuitry between the basal ganglia and dorsolateral-prefrontal cortex. Recently progress has been made in understanding factors contributing to differential susceptibility to pathology mitigating disease-related cognitive decline. Cognitive reserve, the brain processing resources accumulated throughout life while engaged in mentally stimulating activities, can play an important protective role in cognitive performance. We tested the hypothesis that Cognitive Reserve proxies may exert an impact on the basal ganglia and dorsolateral-prefrontal atrophy in early PD. Forty-five early patients with PD and 20 age-gender-matched healthy controls (HC) completed the Cognitive Reserve Index questionnaire to quantify Cognitive Reserve proxies by three indexes (CRI-Education, CRI-Working Activity, CRI-Leisure Time) and a structural MRI examination (3T). Morphometrical indexes for basal ganglia (bilateral putamen, caudate, pallidum volume) and dorsolateral-prefrontal cortex (cortical thickness) were computed. Significant differences between HC and PD were tested by direct comparisons in demographics, cognitive level, and cognitive reserve proxies indexes. Then two multiple regression analyses were performed to identify predictors of the basal ganglia and dorsolateral-prefrontal cortex structural integrity. Regression analysis revealed that basal ganglia volume was significantly predicted by CRI-Education (pFDR = 0.029), sex (pFDR = 0.029), and Total Intracranial Volume (pFDR < 0.001). Instead, the dorsolateral-prefrontal thickness was predicted by CRI-Leisure Time (pFDR = 0.030) and age (pFDR = 0.010). Cognitive Reserve proxies, especially education and leisure-time activities, can play a protective role on the structural integrity of the basal ganglia and dorsolateral-prefrontal cortex, respectively, critical regions hallmarking brain status of early phases of PD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Parkinson’s Disease (PD), the second most common neurodegenerative disease, is hallmarked by a loss of dopaminergic neurons of the Substantia Nigra (SN) pars compacta projecting to the striatum. Non-motor symptoms are also frequently observed in patients with PD. These non-motor symptoms demonstrate phenotypic heterogeneity across disease severity. PD early phases may be characterized by fairly preserved cognitive status not significantly interfering with autonomy in daily living, while severe cognitive complaints may importantly affect daily life independence in advanced disease duration conditions (Goldman & Sieg, 2020). The frontostriatal network circuitry is typically involved in patients with early PD and no clinical evidence of cognitive impairment (Baglio et al., 2011), or restricted to the executive function complaints (Papagno & Trojano, 2018). Indeed, the alteration of basal ganglia (BG) pathways beyond the nigrostriatal system leads to complex motor and non-motor disturbances in these patients, including cognitive deficits principally for dysfunctional circuitry between the striatum and dorsolateral prefrontal cortex (DLPFC) (Williams-Gray et al., 2007).
Recently, understanding reserve-related factors contributing to coping with age-related changes and the “resilience” towards brain pathology is increasingly gaining attention (Stern, 2002; Stern et al., 2020). These factors can account for the mismatch between the severity of pathological changes and the clinical manifestations; they might specifically help understand differential susceptibility to neurodegeneration’s effects, principally on cognition and daily living functioning (Stern et al., 2020).
Cognitive reserve (CR) is a property of the brain that allows for cognitive performance and refers to the processing resources accrued over time due to being engaged in mentally-stimulating activities (Stern et al., 2020, 2023). The involvement in these activities can modify brain anatomy, promoting neurogenesis, angiogenesis, resistance to apoptosis, and neural plasticity (Alvares Pereira et al., 2022). The current evidence suggests that CR can be influenced by multiple genetic and experiential factors, operating at various points or along the lifespan. Among these, the most studied experiential factor associated with CR is education (Arenaza-Urquijo et al., 2017; Bastin et al., 2012; Anatürk et al., 2018; Conti et al., 2021). The working hypothesis is that these CR proxies moderate the relationship between cognitive status and the neurocognitive brain substratum.
In PD, data support that higher levels of education are associated with higher cognitive performance (Ciccarelli et al., 2018, 2022; Guzzetti et al., 2019; Hindle et al., 2014; Loftus et al., 2021). It is, therefore, possible that PD patients with higher CR can cope better with the disease by compensatory mechanisms (Barulli & Stern, 2013). Rouillard and colleagues (Rouillard et al., 2017) emphasize that education and work are important CR proxies showing a protective role on cognition in PD. Thus, higher educational attainment, and a highly mentally stimulating lifestyle, may support cognitive performance in PD and limit cognitive deterioration. Also, these experiential factors may support compensatory mechanisms involving brain areas within and outside the fronto-striatal circuitry in PD (Di Tella et al., 2023).
To the best of our knowledge, to date, no study has investigated the role of CR proxies on the integrity of specific regions of interest in the PD continuum. This study aimed to test whether experiential factors could modulate the peculiar BG and DLPFC damage in a cohort of patients with early PD and preserved cognitive status. In fact, neuroimaging studies investigating the disease’s impact on brain morphometry found that patients with early PD show a selective reduction in the BG volume, while in the intermediate stage, progressive cortical atrophy is observed (Li et al., 2022; Sarasso et al., 2021). The extent of structural damage may be predicted by experiential factors from the early stages of the disease, hypothesizing a protective effect of these CR proxies. Especially the non-motor loop connecting DLPFC and the caudate may be considered a good measure of brain status in the early stage of PD when the cognitive level is still preserved (de la Fuente-Fernàndez, 2012; DeLong & Wichmann, 2009; Cools, 2006; Tekin & Cummings, 2002).
Materials and methods
Participants
Forty-five early PD patients (mean age (SD): 69.19(7.87) years; 25 males; median disease duration (IQR): 4.00(5.00) years) and 20 age- gender-matched sample of healthy controls (HC) were recruited from the neurological unit of the IRCCS Fondazione Don Carlo Gnocchi ONLUS (Milan, Italy).
Patients’ inclusion criteria were: diagnosis of idiopathic PD according to the Movement Disorder Society Clinical Diagnostic Criteria for PD (Postuma et al., 2015); positive DaTscan; mild-to-moderate disease stage (Modified Hoehn and Yahr, range 1–3) (Goetz et al., 2004; Postuma et al., 2015); stable therapy with either L-Dopa or dopamine agonists; and absence of on-off fluctuations and dyskinesia due to medication.
Exclusion criteria were: clinical signs meeting criteria for other neurological disorders, including possible atypical parkinsonism; secondary or iatrogenic parkinsonism; major psychiatric disorders; contraindications to MRI scanning.
All PD patients underwent a clinical evaluation, including a neurologic examination, and both PD and HC performed a neuropsychological screening, including the Montreal Cognitive Assessment (MoCA) (Table 1).
For the neurological examination of PD patients, MDS-UPDRS Part III, in addition to the total score, four-factor scores were calculated: tremor, bradykinesia of upper and lower limb extremity, rigidity, axial (midline function), accordingly to Li et al. (2018). HC completed a neurological evaluation to rule out neuropsychiatric disorders and systemic and neurological diseases.
This study was conducted in accordance with the principles of the Helsinki Declaration and was approved by the IRCCS Don Carlo Gnocchi Foundation Ethics Committee. Each participant signed a written informed consent.
Assessment of CR proxies
Participants were administered the Cognitive Reserve Index Questionnaire (CRIq; Nucci et al., 2012), a 20-items standardized instrument to quantify the CR proxies derived from education, professional achievements, and leisure activities. Three indexes (CRI-Education; CRI-Working Activity; CRI-Leisure Time) and a single composite score (Cognitive Reserve Index – CRIq) have been calculated.
The CRI-Education index refers to years of schooling and courses taken. The CRI-Working Activity categorizes professional activities into five levels that differ in terms of the cognitive commitment required as well as the level of responsibility assumed. The CRI-Leisure Time index takes into account leisure and recreational activities. The CRIq total score is expressed on a scale with a mean of 100 and a standard deviation of 15; with more detail, it is considered low level if it is less than or equal to 70, medium-low level if between 70 and 84, medium level if between 85 and 114, medium-high level if between 115 and 130, high level if greater than or equal to 130 (Nucci et al., 2012).
MRI acquisition and data processing
MRI acquisition protocol
All subjects underwent a structural MRI examination on a 3T, Siemens PRISMA scanner equipped with a 64-channel coil, including a fluid-attenuated inversion recovery (FLAIR) (0.4 × 0.4 × 1 mm³, TR/TE: 5000/394 ms, FOV: 256 × 230 mm) sequence; diffusion-weighted echo planar images (EPI) (TR/TE: 3600/92 ms, FOV 210 × 210 mm, 50 diffusion directions b = 1000s/mm2, 50 diffusion directions b = 2000s/mm2, 5 b = 0s/mm2, repeated acquisition in Antero-Posterior and Postero-Anterior directions, voxel 2.0 mm3); and a T1-3D magnetization-prepared rapid acquisition with gradient echo (MPRAGE) (0.8 mm3, TR/TE: 2300/3.1 ms, FOV: 256 × 240 mm).
Substantia nigra MRI assessment
Diffusion-weighted MRI images were processed with FMRIB’s Software Library (FSL, http://www.fmrib.ox.ac.uk/fsl). First of all, the susceptibility-induced off-resonance field was estimated with the topup tool (Andersson et al., 2018). After that, susceptibility-induced geometric distortions, as well as distortions caused by eddy currents and subject movement, were corrected with the eddy tool (Andersson & Sotiropoulos, 2016). The estimate of the diffusion tensor was performed within each voxel with dtifit (Behrens et al., 2003). Then, fractional anisotropy (FA) maps were obtained. Individual FA maps were registered to the Montreal Neurological Institute (MNI) FA template with a nonlinear transformation (Andersson et al., 2018). The diffusion tensor was warped accordingly. Each subject’s mean diffusivity (MD) map in MNI standard space was also derived. In accordance with Bergsland et al. (2021), microstructural integrity values (FA, MD) were then extracted for the SN (pars reticulata and pars compacta) using probability maps in the MNI space, thresholded at 50% and binarized (Pauli et al., 2018), to confirm the diagnosis of PD.
Brain morphometry of BG and DLPFC
To extract morphometrical data, manual segmentation of white matter (WM) hyperintensities on FLAIR was performed, and T1-3D have been lesion-filled and analyzed using the recon-all pipeline of Freesurfer software (v.6.0, https://surfer.nmr.mgh.harvard.edu/). Parcellation of subcortical and cortical brain regions was performed according to Fischl’s et al. (2002) and Desikan’s et al. (2006) atlases. Manual quality controls were performed according to Klapwijk et al. (2019). Volumetric and cortical thickness measurements of brain areas strongly related to PD pathology were extracted and included in second-level statistics. In particular, we computed BG volume summing up the bilateral putamen, caudate, pallidum subcortical nuclei, and DLPFC summing up bilateral rostral and caudal middle frontal gyrus and inferior frontal gyrus (pars opercularis, triangularis and orbitalis). See Fig. 1 for a visual representation of regions of interest (ROIs).

Statistical analysis
Means and standard deviations or median and interquartile range (IQR) for continuous variables and frequencies for categorical variables were reported. To ensure that the two groups were comparable in terms of socio-demographic characteristics (age, education, gender), cognitive level (MoCA total score), and CRIq indexes (CRIq Education, Working Acitivity, Leisure time and Total score), an independent sample t-test (two-tailed)/Chi-squared χ2 test as appropriate, was performed.
To evaluate the level of brain neurodegeneration, the MRI morphometric data (BG normalized volumes and DLPFC thickness), the exact Total Intracranial Volume (TIV), and microstructural DTI indexes of SN (FA and MD values of pars compacta and reticulata) were compared between the two groups using an ANCOVA (age and sex as covariates). The exact Total Intracranial Volume (TIV) was calculated by summing up the total WM, GM, and Cerebrospinal fluid (CSF).
Moreover, BG volumes and DLPFC thickness (dependent variables) were inserted in two separate multiple regression analyses (BG model and DLPFC model) to detect potential predictors of their structural integrity. Correlations (using Pearson’s r, Spearman’s rho rank correlation, or rpb point-biserial coefficients as appropriate) were preliminary run to explore the link between morphometrical indexes (BG volumes and DLPFC thickness), sociodemographic (age, sex, and CRIq indexes), clinical variables (H&Y grading and UPDRS scores) and TIV. Moreover, the hierarchical backward approach was adopted in order to simultaneously maximize the predictive power of the final regression and minimize the number of variables included in the model.
Statistical analyses were performed with Jamovi (version 2.3, https://www.jamovi.org/) and SPSS (version 24) softwares. The statistical threshold was set at p < 0.05 two-tailed for all statistical tests, except for correlations (one-tailed). The False Discovery Rate (FDR) type-1 correction was performed to take into account false positive errors (Benjamini & Hochberg, 1995). The magnitude of effects was interpreted as follows: for correlation coefficients, 0.1–0.3 as a small effect; 0.3–0.5 as an intermediate effect; and 0.5 and higher as a strong effect; and for partial η2, 0.01–0.05 as a small effect, 0.06–0.13 as a medium effect, and 0.14 and higher as a strong effect coefficient (Cohen, 1988).
Results
Clinical characterization of the recruited sample
The baseline comparison revealed that HC and PD groups were matched for age, sex, education, cognitive level, and CRIq indexes (Table 1). In more detail, at the neuropsychological screening, all PD subjects scored above the cut-off of 15.5 (Santangelo et al., 2015), and both groups show medium to high CR (HC = 124.30; PD = 122.98) without significant differences in CRIq indexes (Table 1).
Differences between groups on MRI measurements
The ANCOVA results showed (see Table 2): (i) higher MD values in PD than HC in both SN subparts (pars compacta puncorr = 0.005, pFDR = 0.020, partial η2 = 0.13; pars reticulata puncorr = 0.012, pFDR = 0.024, partial η2 = 0.11); (ii) a trend of reduced putamen volumes (puncorr = 0.039, pFDR = 0.195; partial η² = 0.07) in PD compared to HC; (iii) no differences between the two groups in the thickness of DLPFC.
Regression analysis
BG model
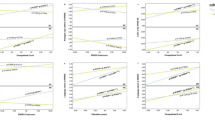
Preliminary correlations in the PD group revealed a direct relation between BG volume and TIV (r = 0.809, p < 0.001), CRI- Working Activity (r = 0.307, p = 0.020), and a trend for direct relation with CRI-Education (r = 0.218, p = 0.076); whereas a significant inverse relation emerged with age (r = -0.360, p = 0.015) and a trend for inverse relation with H&Y (rho = -0.196, p = 0.098). An association also emerged between BG volume and sex (rpb = -0.661, p < 0.001), with higher volumes associated with the sex of males. The best regression model (R2 = 0.734, p < 0.001) revealed that higher BG volume was significantly associated with the sex of males, higher TIV, and higher CRI-Education (Table 3; Fig. 2).
DLPFC model
Preliminary correlations in the PD group highlighted a direct relation between DLPFC thickness and CRI-Working Activity (r = 0.345, p = 0.010), CRI-Leisure Time (r = 0.300, p = 0.023) and an inverse relation with age (r = -0.416, p = 0.002) and H&Y (rho = -0.216, p = 0.077). The regression analyses (R2 = 0.278, p = 0.010; R2 = 0.262, p = 0.002) revealed that DLPFC thickness was significantly associated with lower age and higher CRI-Leisure Time (Table 4; Fig. 2).

Marginal effects plots of regression analyses on BG volume and DLPFC
Discussion
The purpose of this study was to test the hypothesis that the volume of regions mainly involved in the frontostriatal circuit in PD, namely the BG, and DLPFC, was modulated by CR proxies. To this aim, we involved a cohort of early PD patients cognitively fairly preserved.
Our PD cohort presented a similar cognitive level and CRIq indexes compared to an age-sex-education-matched HC group. As expected, the neural profile of patients revealed a microstructural alteration of the SN, initial atrophy in the BG, and preserved integrity in the DLPFC thickness, in line with previous studies including PD participants with the same clinical characteristics of our cohort (low disease duration and severity) (Bergsland et al., 2021; Li et al., 2022; Sarasso et al., 2021).
Considering the role of CR proxies on the integrity of the fronto-striatal circuits, our results supported the study hypothesis in terms of the modulating role of CR proxies on the brain reserve of regions mainly implicated in PD, such as BG and DLPFC. Interestingly, the integrity of BG and DLPFC seemed to be related to differential experiential factors: education exerted protective effects on BG, while leisure time activities significantly modulated DLPFC status.
In detail, concerning subcortical volumes, higher BG volumes were associated with higher CRI-Education, TIV, and male sex. PD patients with more years of education and training courses were more preserved in subcortical regions linked to the initial nigrostriatal dopaminergic denervation. In agreement with Chapko, et al. (Chapko et al., 2018) and Meng & D’Arcy (2012), that consider education as one of the main factors favoring the accumulation of CR proxies, the present research suggests a protective role of education in PD, and, as expected, the volume of these subcortical structures was associated with TIV, which is generally higher in males than females (Ruigrok et al., 2014). Although the role of BG in the control of movement is widely acknowledged, its role has been theorized as linked with other cognitive processes (Phillips & Carr, 1987), such as the acquisition and retention of procedural knowledge. With this in mind, a higher level of study can be linked to these procedural processes and related subcortical neuronal structures. However, to our knowledge, no studies concerning the link between education and the integrity of the BG have been conducted at this time, and further investigations are required.
Moving to the cortical regions involved in the frontostriatal circuit, higher DLPFC thickness was associated with CRI-q leisure time and lower age. Individuals who spent more time in cognitively stimulating leisure and recreational activities, such as reading newspapers, mobile phones use, solving puzzles, multi-day trips, and engaging in other cognitively demanding hobbies, are more preserved in the DLPFC. The positive association between engagement in social-intellectual activities and frontal areas is acknowledged (Arenaza-Urquijo et al., 2017; Bartrés-Faz & Arenaza-Urquijo, 2011). Previous studies demonstrated that CR and structural integrity are linked in older adults’ brains (Anatürk et al., 2018; Conti et al., 2021). Greater GM volumes in individuals with higher CR may correspond to a better tolerance of age-related damage (Bartrés-Faz & Arenaza-Urquijo, 2011; Mortimer et al., 2003; Stern, 2002, 2012), with GM loss concentrated in the prefrontal cortices (Allen et al., 2005; Driscoll et al., 2009; Raz et al., 2004; Schippling et al., 2017; Taki et al., 2013). Similar results were also found in neurodegenerative diseases, reporting an impact of CR, especially in the early stages of Alzheimer’s disease, contributing to the brain maintenance, with lower susceptibility to brain changes associated with the disease (Cohen et al., 2009; Dumurgier et al., 2010; Morbelli et al., 2013; Stern, 2012). Also, pieces of evidence on the effect of lifestyle habits on brain maintenance support a protective role of active social life on changes in cortical thickness, dendritic branching, spine density, neurogenesis, and gliogenesis (Mora, 2013). Our study confirmed this effect in the PD condition, especially in frontal areas, which are traditionally considered to be involved in the planning of complex activities and managing goal-directed behaviors (Badre & Nee, 2018). It has to be mentioned that our PD subjects report a high level of the CRIq-leisure time score. This data may be peculiar to the cohort of this study. In fact, our sample was enrolled in a metropolitan city context, in which cultural- and social-stimulating activities are easily accessible. On the other hand, this result could suggest that leisure time activity is a significant index of reserve in pathological conditions in which the frontostriatal circuit is involved. In fact, pivotal contributions registered the role of environmental enrichment in PD animal models on SN (Klaissle et al., 2012). In fact, an amount of data reveals a great positive effect of housing in new and composite surroundings in mice and rats (Mandolesi et al., 2008; Petrosini et al., 2009).
Concerning the predictive role of age on DLPFC thickness, this association is documented by a large amount of data (Peters et al., 2006). The impact of age on DLPFC is well recognized both in structure and function changes (Cabeza et al., 2018). Age-related neural prefrontal loss is linked with cognitive changes observed with advancing age in which working memory, executive functions, and information processing speed are typically impaired (Anderton, 2002).
Overall, our results suggest that CR proxies and brain neurophysiological status, the brain reserve, are linked through two possible mechanisms. Experiential factors may impact on cognitive performance through brain reserve-related mechanisms. Another possible explanation is the influence of these factors on cognition through mechanisms related to CR (e.g., buffering the association between brain structural integrity and cognitive functioning). Future studies may clarify the direction of this relationship by assessing the cognitive performance together with brain reserve and CR proxies.
Limitations
We acknowledged that the study presents some limitations: our study has a cross-sectional design. This approach cannot truly disentangle whether the impact of CR proxies may reflect pre-clinical differences in brain structure or differences in the rate of brain loss between PD individuals with different levels of CR. Moreover, the study is focused only on the non-motor brain loop connecting DLPFC and the BG as a marker of brain status in the early stage of PD when the cognitive level is still preserved. Future longitudinal studies are required to evaluate brain maintenance and if CR may mediate the clinical course of PD, mitigating the spread of atrophy in other cortical regions, according to Braak’s staging (Braak et al., 2003) of brain pathology related to PD. Moreover, longitudinal studies are required to evaluate if CR proxies may have a role in predicting the outcome of rehabilitative interventions. However, the strength of this research is that, to date, it is the first study investigating the protective role of CR proxies on BG circuitry in PD. Additionally, CR was considered a multidimensional construct, using a standardized proxy of CR. Future studies may also include additional measures of reserve-related aspects, such as the emerging construct of motor reserve in PD (Sunwoo et al., 2017), introduced as the possibility of the brain being made resilient to neuronal damage by an individual’s engagement in physical exercise throughout their lifespan. Finally, future studies may include an extensive neuropsychological battery to explore executive functioning and how CR proxies mediate the link between frontostriatal circuits status and executive domain behavioral levels.
Conclusion
Our study supports lower susceptibility to brain burden in PD individuals with higher educational achievement and who spent more time in activities stimulating socio-intellectual abilities before the clinical onset. This suggests that these CR proxy measures may serve as possible markers for the structural integrity of key regions involved in PD from the early stage.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Allen, J. S., Bruss, J., Brown, C. K., & Damasio, H. (2005). Normal neuroanatomical variation due to age: the major lobes and a parcellation of the temporal region. Neurobiol Aging, 26(9), 1245–1260; discussion 1279–1282.
Alvares Pereira, G., Silva Nunes, M. V., Alzola, P., & Contador, I. (2022). Cognitive reserve and brain maintenance in aging and Dementia: An integrative review. Appl Neuropsychol Adult, 29(6), 1615–1625.
Anatürk, M., Demnitz, N., Ebmeier, K. P., & Sexton, C. E. (2018). A systematic review and meta-analysis of structural magnetic resonance imaging studies investigating cognitive and social activity levels in older adults. Neuroscience and Biobehavioral Reviews, 93, 71–84.
Andersson, J. L. R., & Sotiropoulos, S. N. (2016). An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage, 125, 1063–1078.
Andersson, J. L. R., Graham, M. S., Drobnjak, I., Zhang, H., & Campbell, J. (2018). Susceptibility-induced distortion that varies due to motion: Correction in diffusion MR without acquiring additional data. Neuroimage, 171, 277–295.
Anderton, B. H. (2002). Ageing of the Brain Mechanisms of Ageing and Development, 123(7), 811–817.
Arenaza-Urquijo, E. M., de Flores, R., Gonneaud, J., Wirth, M., Ourry, V., Callewaert, W., et al. (2017). Distinct effects of late adulthood cognitive and physical activities on gray matter volume. Brain Imaging Behav, 11(2), 346–356.
Badre, D., & Nee, D. E. (2018). Frontal Cortex and the Hierarchical Control of Behavior. Trends in Cognitive Sciences, 22(2), 170–188.
Baglio, F., Blasi, V., Falini, A., Farina, E., Mantovani, F., Olivotto, F., Scotti, G., Nemni, R., & Bozzali, M. (2011). Functional brain changes in early Parkinson’s Disease during motor response and motor inhibition. Neurobiology of Aging, 32(1), 115–124.
Bartrés-Faz, D., & Arenaza-Urquijo, E. M. (2011). Structural and functional imaging correlates of cognitive and brain reserve hypotheses in healthy and pathological aging. Brain Topography, 24(3–4), 340–357.
Barulli, D., & Stern, Y. (2013). Efficiency, capacity, compensation, maintenance, plasticity: Emerging concepts in cognitive reserve. Trends in Cognitive Sciences, 17(10), 502–509.
Bastin, C., Yakushev, I., Bahri, M. A., Fellgiebel, A., Eustache, F., Landeau, B., et al. (2012). Cognitive reserve impacts on inter-individual variability in resting-state cerebral metabolism in normal aging. Neuroimage, 63(2), 713–722.
Behrens, T. E., Woolrich, M. W., Jenkinson, M., Johansen-Berg, H., Nunes, R. G., Clare, S., et al. (2003). Characterization and propagation of uncertainty in diffusion-weighted MR imaging. Magnetic Resonance in Medicine, 50(5), 1077–1088.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B (Methodological), 57(1), 289–300.
Bergsland, N., Pelizzari, L., Laganá, M. M., Di Tella, S., Rossetto, F., Nemni, R. (2021). Automated Assessment of the Substantia Nigra Pars Compacta in Parkinson’s Disease: A Diffusion Tensor Imaging Study. J Pers Med, 11(11).
Braak, H., Del Tredici, K., Rüb, U., de Vos, R. A., Steur, J., E. N., & Braak, E. (2003). Staging of brain pathology related to sporadic Parkinson’s Disease. Neurobiology of Aging, 24(2), 197–211.
Cabeza, R., Albert, M., Belleville, S., Craik, F. I. M., Duarte, A., Grady, C. L., et al. (2018). Maintenance, reserve and compensation: The cognitive neuroscience of healthy ageing. Nature Reviews Neuroscience, 19(11), 701–710.
Chapko, D., McCormack, R., Black, C., Staff, R., & Murray, A. (2018). Life-course determinants of cognitive reserve (CR) in cognitive aging and Dementia - a systematic literature review. Aging & Mental Health, 22(8), 915–926.
Ciccarelli, N., Monaco, M. R. L., Fusco, D., Vetrano, D. L., Zuccalà, G., Bernabei, R., et al. (2018). The role of cognitive reserve in cognitive aging: What we can learn from Parkinson’s Disease. Aging Clinical and Experimental Research, 30(7), 877–880.
Ciccarelli, N., Colombo, B., Pepe, F., Magni, E., Antonietti, A., & Silveri, M. C. (2022). Cognitive reserve: A multidimensional protective factor in Parkinson’s Disease related cognitive impairment. Neuropsychology, Development, and Cognition. Section B, Aging, Neuropsychology and Cognition, 29(4), 687–702.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).). Erlbaum.
Cohen, A. D., Price, J. C., Weissfeld, L. A., James, J., Rosario, B. L., Bi, W., et al. (2009). Basal cerebral metabolism may modulate the cognitive effects of Abeta in mild cognitive impairment: An example of brain reserve. Journal of Neuroscience, 29(47), 14770–14778.
Conti, L., Riccitelli, G. C., Preziosa, P., Vizzino, C., Marchesi, O., Rocca, M. A., et al. (2021). Effect of cognitive reserve on structural and functional MRI measures in healthy subjects: A multiparametric assessment. Journal of Neurology, 268(5), 1780–1791.
Cools, R. (2006). Dopaminergic modulation of cognitive function-implications for L-DOPA treatment in Parkinson’s Disease. Neuroscience and Biobehavioral Reviews, 30(1), 1–23.
de la Fuente-Fernández, R. (2012). Frontostriatal cognitive staging in Parkinson’s Disease. Parkinson’s Disease, 2012, 561046.
DeLong, M., & Wichmann, T. (2009). Update on models of basal ganglia function and dysfunction. Parkinsonism & Related Disorders, 15(03), S237–S240. Suppl 3.
Desikan, R. S., Ségonne, F., Fischl, B., Quinn, B. T., Dickerson, B. C., Blacker, D., et al. (2006). An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage, 31(3), 968–980.
Di Tella, S., De Marco, M., Baglio, F., Silveri, M. C., & Venneri, A. (2023). Resting-state functional connectivity is modulated by cognitive reserve in early Parkinson’s disease (p. 14). Front Psychol.
Driscoll, I., Davatzikos, C., An, Y., Wu, X., Shen, D., Kraut, M., et al. (2009). Longitudinal pattern of regional brain volume change differentiates normal aging from MCI. Neurology, 72(22), 1906–1913.
Dumurgier, J., Paquet, C., Benisty, S., Kiffel, C., Lidy, C., Mouton-Liger, F., et al. (2010). Inverse association between CSF Aβ 42 levels and years of education in mild form of Alzheimer’s Disease: The cognitive reserve theory. Neurobiology of Diseases, 40(2), 456–459.
Fischl, B., Salat, D. H., Busa, E., Albert, M., Dieterich, M., Haselgrove, C., et al. (2002). Whole brain segmentation: Automated labeling of neuroanatomical structures in the human brain. Neuron, 33(3), 341–355.
Goetz, C. G., Poewe, W., Rascol, O., Sampaio, C., Stebbins, G. T., Counsell, C., et al. (2004). Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: Status and recommendations. Movement Disorders, 19(9), 1020–1028.
Goldman, J. G., & Sieg, E. (2020). Cognitive impairment and Dementia in Parkinson Disease. Clinics in Geriatric Medicine, 36(2), 365–377.
Guzzetti, S., Mancini, F., Caporali, A., Manfredi, L., & Daini, R. (2019). The association of cognitive reserve with motor and cognitive functions for different stages of Parkinson’s Disease. Experimental Gerontology, 115, 79–87.
Hindle, J. V., Martyr, A., & Clare, L. (2014). Cognitive reserve in Parkinson’s Disease: A systematic review and meta-analysis. Parkinsonism & Related Disorders, 20(1), 1–7.
Klaissle, P., Lesemann, A., Huehnchen, P., Hermann, A., Storch, A., & Steiner, B. (2012). Physical activity and environmental enrichment regulate the generation of neural precursors in the adult mouse substantia nigra in a dopamine-dependent manner. Bmc Neuroscience, 13, 132.
Klapwijk, E. T., van de Kamp, F., van der Meulen, M., Peters, S., & Wierenga, L. M. (2019). Qoala-T: A supervised-learning tool for quality control of FreeSurfer segmented MRI data. Neuroimage, 189, 116–129.
Li, X., Xing, Y., Martin-Bastida, A., Piccini, P., & Auer, D. P. (2018). Patterns of grey matter loss associated with motor subscores in early Parkinson’s Disease. Neuroimage Clin, 17, 498–504.
Li, R., Zou, T., Wang, X., Wang, H., Hu, X., Xie, F., et al. (2022). Basal ganglia atrophy-associated causal structural network degeneration in Parkinson’s Disease. Human Brain Mapping, 43(3), 1145–1156.
Loftus, A. M., Gasson, N., Lopez, N., Sellner, M., Reid, C., Cocks, N., et al. (2021). Cognitive Reserve, executive function, and memory in Parkinson’s Disease. Brain Sci, 11, 8.
Mandolesi, L., De Bartolo, P., Foti, F., Gelfo, F., Federico, F., Leggio, M. G., et al. (2008). Environmental enrichment provides a cognitive reserve to be spent in the case of brain lesion. Journal of Alzheimer’s Disease, 15(1), 11–28.
Meng, X., & D’Arcy, C. (2012). Education and Dementia in the context of the cognitive reserve hypothesis: A systematic review with meta-analyses and qualitative analyses. PLoS One, 7(6), e38268.
Mora, F. (2013). Successful brain aging: Plasticity, environmental enrichment, and lifestyle. Dialogues Clin Neurosci, 15(1), 45–52.
Morbelli, S., Perneczky, R., Drzezga, A., Frisoni, G. B., Caroli, A., van Berckel, B. N., et al. (2013). Metabolic networks underlying cognitive reserve in prodromal Alzheimer Disease: A European Alzheimer Disease consortium project. Journal of Nuclear Medicine, 54(6), 894–902.
Mortimer, J. A., Snowdon, D. A., & Markesbery, W. R. (2003). Head circumference, education and risk of Dementia: Findings from the Nun Study. Journal of Clinical and Experimental Neuropsychology, 25(5), 671–679.
Nucci, M., Mapelli, D., & Mondini, S. (2012). Cognitive Reserve Index questionnaire (CRIq): A new instrument for measuring cognitive reserve. Aging Clinical and Experimental Research, 24(3), 218–226.
Papagno, C., & Trojano, L. (2018). Cognitive and behavioral disorders in Parkinson’s Disease: An update. I: Cognitive impairments. Neurological Sciences : Official Journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology, 39(2), 215–223.
Pauli, W. M., Nili, A. N., & Tyszka, J. M. (2018). A high-resolution probabilistic in vivo atlas of human subcortical brain nuclei. Sci Data, 5, 180063.
Peters, F., Perani, D., Herholz, K., Holthoff, V., Beuthien-Baumann, B., Sorbi, S., et al. (2006). Orbitofrontal dysfunction related to both apathy and disinhibition in frontotemporal Dementia. Dementia and Geriatric Cognitive Disorders, 21(5–6), 373–379.
Petrosini, L., De Bartolo, P., Foti, F., Gelfo, F., Cutuli, D., Leggio, M. G., et al. (2009). On whether the environmental enrichment may provide cognitive and brain reserves. Brain Research Reviews, 61(2), 221–239.
Phillips, A. G., & Carr, G. D. (1987). Cognition and the basal ganglia: A possible substrate for procedural knowledge. The Canadian journal of neurological sciences. Le Journal Canadien Des Sciences Neurologiques, 14(3 Suppl), 381–385.
Postuma, R. B., Berg, D., Stern, M., Poewe, W., Olanow, C. W., Oertel, W., et al. (2015). MDS clinical diagnostic criteria for Parkinson’s Disease. Movement Disorders, 30(12), 1591–1601.
Raz, N., Gunning-Dixon, F., Head, D., Rodrigue, K. M., Williamson, A., & Acker, J. D. (2004). Aging, sexual dimorphism, and hemispheric asymmetry of the cerebral cortex: Replicability of regional differences in volume. Neurobiology of Aging, 25(3), 377–396.
Rouillard, M., Audiffren, M., Albinet, C., Ali Bahri, M., Garraux, G., & Collette, F. (2017). Contribution of four lifelong factors of cognitive reserve on late cognition in normal aging and Parkinson’s Disease. Journal of Clinical and Experimental Neuropsychology, 39(2), 142–162.
Ruigrok, A. N., Salimi-Khorshidi, G., Lai, M. C., Baron-Cohen, S., Lombardo, M. V., Tait, R. J., et al. (2014). A meta-analysis of sex differences in human brain structure. Neuroscience and Biobehavioral Reviews, 39(100), 34–50.
Santangelo, G., Siciliano, M., Pedone, R., Vitale, C., Falco, F., Bisogno, R., et al. (2015). Normative data for the Montreal Cognitive Assessment in an Italian population sample. Neurological Sciences : Official Journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology, 36(4), 585–591.
Sarasso, E., Agosta, F., Piramide, N., & Filippi, M. (2021). Progression of grey and white matter brain damage in Parkinson’s Disease: A critical review of structural MRI literature. Journal of Neurology, 268(9), 3144–3179.
Schippling, S., Ostwaldt, A. C., Suppa, P., Spies, L., Manogaran, P., Gocke, C., et al. (2017). Global and regional annual brain volume loss rates in physiological aging. Journal of Neurology, 264(3), 520–528.
Stern, Y. (2002). What is cognitive reserve? Theory and research application of the reserve concept. Journal of the International Neuropsychological Society, 8(3), 448–460.
Stern, Y. (2012). Cognitive reserve in ageing and Alzheimer’s Disease. Lancet Neurology, 11(11), 1006–1012.
Stern, Y., Arenaza-Urquijo, E. M., Bartrés-Faz, D., Belleville, S., Cantilon, M., Chetelat, G., et al. (2020). Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement, 16(9), 1305–1311.
Stern, Y., Albert, M., Barnes, C., Cabeza, R., Pascual-Leone, A., & Rapp, P. (2023). A framework for concepts of reserve and resilience in aging. Neurobiology of Aging, 124, 100–103.
Sunwoo, M. K., Lee, J. E., Hong, J. Y., Ye, B. S., Lee, H. S., Oh, J. S., et al. (2017). Premorbid exercise engagement and motor reserve in Parkinson’s Disease. Parkinsonism & Related Disorders, 34, 49–53.
Taki, Y., Thyreau, B., Kinomura, S., Sato, K., Goto, R., Wu, K., et al. (2013). A longitudinal study of age- and gender-related annual rate of volume changes in regional gray matter in healthy adults. Human Brain Mapping, 34(9), 2292–2301.
Tekin, S., & Cummings, J. L. (2002). Frontal-subcortical neuronal circuits and clinical neuropsychiatry: An update. Journal of Psychosomatic Research, 53(2), 647–654.
Williams-Gray, C. H., Foltynie, T., Brayne, C. E., Robbins, T. W., & Barker, R. A. (2007). Evolution of cognitive dysfunction in an incident Parkinson’s Disease cohort. Brain, 130(Pt 7), 1787–1798.
Funding
The research has been financially supported by the Italian Ministry of Health (Ricerca-Corrente Reti program: RCR 2022).
Author information
Authors and Affiliations
Contributions
F.Ba. designed the study; F.R., F.Bo., and Ma.C. collected data; S.D.T. and S.I. analyzed experimental results; S.D.T. and S.I. wrote the manuscript; M.C.S. revised the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Fondazione Don Carlo Gnocchi-Milan Ethics Committee approved the study protocol.
Informed consent
Written informed consent was obtained from all subjects after they received a complete description of the study.
Consent to participate
Obtained.
Consent for publication
This manuscript has not been published or presented elsewhere in part or in entirety and is not under consideration by another journal. We have read and understood your journal’s policies, and we believe that neither the manuscript nor the study violates any of these policies.
Conflict of interest
None of the authors have a conflict of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Di Tella, S., Isernia, S., Cabinio, M. et al. Cognitive Reserve proxies can modulate motor and non-motor basal ganglia circuits in early Parkinson’s Disease. Brain Imaging and Behavior 18, 220–230 (2024). https://doi.org/10.1007/s11682-023-00829-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11682-023-00829-8