
Abstract
Background
Reconstruction of the proximal humerus with a locking plate is often the first surgical approach for proximal humerus fractures. Screw cut-out is a common complication and is relevant in osteoporotic bone of older adults. The Deltoid Tuberosity Index (DTI) is an indirect measure for assessing local bone quality and failure rate before surgery, providing important information for surgical planning. This was the first independent, large-sample retrospective analysis of the correlation between local bone density, indirectly measured through the DTI, and screw cut-out.
Methods
In total, 306 cases of proximal humerus fractures treated with the PHILOS plate (DePuy Synthes, Oberdorf, Switzerland) were retrospectively analyzed. The DTI was measured on anteroposterior x‑rays. The primary endpoint was screw cut-out defined as the intra-articular position of at least one screw associated with a reduction loss after surgery.
Results
The mean clinical follow-up was 935 days. The DTI varied from 1.10 to 2.28 (average: 1.45). Screw cut-out occurred on average in 8% of the cases and was positively correlated with a DTI of ≤ 1.44 (p = 0.003). However, the rate of cut-out and correlation with DTI varied widely according to age group: for ages 65–80 years, a DTI of ≤ 1.44 increased the cut-out rate from 0% to 17% (p = 0.02); in younger ages (< 65 years) the DTI did not correlate with cut-out and in the oldest group (> 80 years) cut-out rates were high (17–20%) independently of the DTI.
Conclusion
We confirm the correlation between a DTI of ≤ 1.44 and screw cut-out. High-risk groups for screw cut-out are patients over 65 years with a DTI of ≤ 1.44 or any patient older than 80 years. Applying the DTI in the age group of 65–80 years offers relevant information for surgical planning in the trauma setting via a fast, cheap, and easy-to-use tool.
Level of Evidence: Level 3, Retrospective Cohort Study.
Zusammenfassung
Hintergrund
Die Rekonstruktion des proximalen Humerus mit einer Verriegelungsplatte ist oft der erste chirurgische Ansatz bei Frakturen des proximalen Humerus. Die Häufigkeit eines Schrauben-Cut-out, insbesondere bei älteren Patienten mit osteoporotischem Knochen, bleibt jedoch eine Herausforderung. Der Deltoid Tuberosity Index (DTI) wurde vorgeschlagen, um die lokale Knochenqualität präoperativ zu beurteilen, das Risiko eines Versagens der Osteosynthese einzuschätzen und wichtige Informationen für die chirurgische Planung zu liefern. Die vorliegende Studie liefert die erste unabhängige retrospektive Analyse großer Stichproben zur Korrelation zwischen der lokalen Knochendichte, indirekt gemessen durch den DTI, und dem Schrauben Cut-out.
Methoden
Retrospektiv wurden 306 Fälle von mit PHILOS-Platten (Fa. DePuy Synthes, Oberdorf, Schweiz) versorgten proximalen Humerusfrakturen analysiert. Der DTI wurde in a.-p.-Röntgenaufnahmen gemessen. Der primäre Endpunkt war das Auftreten eines Schrauben Cut-out, definiert als die intraartikuläre Position von mindestens einer Schraube, die mit einem Repositionsverlust nach der Operation verbunden ist.
Ergebnisse
Das durchschnittliche klinische Follow-up betrug 935 Tage. Der DTI variierte von 1,10 bis 2,28 (Durchschnitt: 1,45). Ein Cut-out trat im Durchschnitt in 8 % der Fälle auf und korrelierte positiv mit einem DTI ≤ 1,44 (p = 0,003). Die Cut-out-Rate und die Korrelation zum DTI variierten jedoch stark je nach Altersgruppe: Im Alter von 65–80 Jahren erhöhte ein DTI ≤ 1,44 die Cut-out-Rate von 0 % auf 17 % (p = 0,02); Andererseits korrelierte der DTI in jüngeren Altersgruppen (< 65 Jahre) nicht mit dem Cut-out, und in der ältesten Gruppe (> 80 Jahre) waren die Cut-out-Raten unabhängig vom DTI, aber dennoch hoch (17–20 %).
Schlussfolgerungen
Die Korrelation zwischen einem DTI ≤ 1,44 und Schrauben Cut-out wurde bestätigt. Hochrisikogruppen für einen Cut-out sind Patienten über 65 Jahre mit einem DTI ≤ 1,44 oder alle Patienten über 80 Jahre. Die Anwendung des DTI in der Altersgruppe von 65 bis 80 Jahren bietet relevante Informationen für die chirurgische Planung im Traumaumfeld durch ein schnelles, kostengünstiges und einfach durchzuführendes Tool.
Evidenzgrad: Level 3, retrospektive Kohortenstudie.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Proximal humerus fractures are common and often treated with locking plates, such as the PHILOS plate (DePuy Synthes, Oberdorf, Switzerland; [1, 2]). The most common complication of this surgery is screw cut-out, which is reported in 8–57% of cases [3, 4]. This complication often affects the quality of life of patients due to its association with shoulder pain, restricted range of motion, and often the need for revision surgery. Screw cut-out may be defined as the disruption of the humeral head by the cranial screws in the context of a reduction loss. Since older age and a low local bone mineral density (BMD) are known independent predictive factors for cut-out, a preoperative assessment of bone quality is often recommended to better predict the risk of surgery failure [5,6,7,8]. However, the standard methods of osteoporosis diagnosis (dual-energy x‑ray and peripheral quantitative computed tomography) are not routinely available in the trauma setting and could significantly delay treatment [4, 6, 9]. To indirectly assess bone mineralization, several parameters have been proposed. Tingart et al. proposed measuring the combined cortical thickness of the humeral diaphysis, while Newton et al. used the cortical thickness to calculate a medial cortical ratio [10, 11]. Although a correlation between cortical thickness and BMD has been confirmed, its adoption is limited since many x‑rays of proximal humerus fractures do not include the middle diaphyseal area needed for Tingart’s and Newton’s measurements [12]. The deltoid tuberosity index (DTI), proposed by Spross et al., has the advantage of measuring the cortical thickness on the proximal humerus (above the deltoid tuberosity) and has demonstrated a strong correlation with local BMD [12]. The smaller the DTI value, the thinner the cortex and therefore the greater the correlation with osteopenia. A DTI cut-off of 1.44 predicted a low BMD (< 80 mg/cm3) of the humeral head (sensitivity, 0.9; specificity, 0.8). In a further retrospective study with 146 patients in 2017, the authors concluded that a DTI of ≤ 1.44 was a relevant predictor of cut-out in proximal humerus fractures and claimed for further research [13]. Although this index seems to be growing in popularity, there have not been any clinical studies to date supporting the use of this tool. Moreover, a recent study with a small sample size of 48 geriatric patients found no correlation between osteopenia, measured by DTI, and surgical outcome [14].
The current study aimed to provide an independent, large-sample retrospective analysis of the correlation between the local bone density, indirectly measured through the DTI, and the most common postsurgical complication after open reduction and internal fixation with locking plate osteosynthesis: screw cut-out.
Methods
The hypothesis of this retrospective observational study was that patients with a DTI of ≤ 1.44 had a significantly higher risk for screw cut-out after treatment with a PHILOS plate. This hypothesis was tested for different age groups. The primary endpoint was screw cut-out, defined as the intra-articular position of at least one screw associated with a reduction loss after surgery. Intra-articular screws identified during the first days after surgery without reduction loss were considered as iatrogenic malposition. Intra-articular screws without reduction loss and associated with a progressive bone mass reduction and deformity of the humeral head were classified as humeral head necrosis (HHN).
We retrospectively collected data from all patients operated on in our level I trauma center between 2007 and 2018. This presented us with 544 eligible patients. The inclusion criteria were: isolated proximal humerus fracture; no previous shoulder surgery; preoperative electronic anteroposterior (AP) x‑ray in internal rotation as well as outlet view; treatment with an internal locking plate (PHILOS plate) with at least five head screws. The exclusion criteria were: pathological fracture; treatment with an additive fibular graft, supplemental plate, or other augmentation strategies; follow-up of less than 6 weeks. After application of the study criteria, 306 patients were selected.
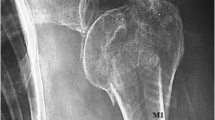
Data were collected by three of the authors, all experienced trauma surgeons. Measurements were performed through an electronic length-measuring tool provided by the IMPAXTM software (AGFA, Mortsel, Belgium), which is regularly used in our hospital. The DTI was measured from AP x‑rays immediately above the upper end of the deltoid tuberosity where the outer cortical borders become parallel, as described by the proponents of the index [12]. The DTI value is given by the ratio between the external cortex and the internal endosteal diameter (Fig. 1). Fractures were classified according to the AO/OTA classification and Neer classification. Metaphyseal head extension and medial hinge displacement were measured according to Hertel et al. [15]. The number of screws and the grade of reduction were assessed from the postoperative x‑rays (AP and outlet view) usually taken on the second day after surgery. Reduction was categorized as anatomic (< 2 mm of displacement), acceptable (< 1 cm or < 45° of displacement of any fragment), or dislocated (none of the previous). Postoperative complications were retrieved from electronic medical reports and x‑rays. All documented complications are presented in Table 1.

Measurement of the deltoid tuberosity index (DTI) = α / β: α is the distance between the outer cortexes right above the deltoid tuberosity; β is the distance between the inner cortexes at the same level. a An x‑ray example of an 87-year-old female patient with a DTI of 1.20. b A 47-year-old male patient with a DTI of 1.81
The deltopectoral approach was used in all cases. If reduction of the tubercula was needed, non-absorbable braided sutures were used to fixate the reduced tubercula to the plate. At least five head screws were used and at least one calcar screw was recommended. The rehabilitation protocol included free active range-of-motion exercises from day 1 after surgery and no lifting or pulling tensions of the injured arm for 6 weeks. Follow-up x‑rays were acquired after 6 weeks and strengthening exercises were then initiated. Further follow-ups were only performed in the case of existing symptoms.
Statistical analysis was performed using JASP (0.11.1/October 7, 2019—jasp.stats.org) provided by the University of Amsterdam (Amsterdam, The Netherlands). Descriptive statistics included means, medians, standard deviations, interquartile range (IQR), and proportions. Inferential statistics included the t test for numerical data and the chi-square test for categorical data. Exploratory data analysis was performed using multiple logistic regression. The significance level was set at a p value = 0.04. If the p value was > 0.04, this was considered not significant (n. s.). Subgroup analysis was performed for patients (a) younger than 65, (b) between 65 and 80, and (c) older than 80 years.
Approval from the Ethics and Human Research Board was given by the University of Tübingen under project reference 368/2020BO.
Results
A total of 306 patients met the inclusion criteria. The mean age was 61.5 years (±15.9) and 60% were female. The mean follow-up was 935 days (±1076), with a minimum of 42 and a maximum of 4742 days.
Deltoid tuberosity index
The DTI varied widely, from 1.10 to 2.28 (mean: 1.42 ± 0.18). A total of 173 patients (57%) had a DTI smaller or equal to the predefined cut-off value of 1.44, which included patients from a wide age spectrum (27–94 years). The average age of this group was 67 years (±14.5) and 64% were female. Factors that were significantly correlated with a smaller DTI were older age, female gender, higher ASA score, lower height, lower weight, and therefore a lower BMI. Knowing the established correlation between DTI and BMD, this correlation was expected. There was no correlation between DTI and fracture pattern. Patients with a DTI of ≤ 1.44 stayed in the hospital on average 2 days longer after surgery (p = 0.015) and had a significantly higher risk of screw cut-out (12% vs. 2%, p = 0.001). No correlation was found between DTI and other postoperative complications (Table 1) and, in particular, there was no significant difference in the conversion to shoulder prosthesis (average of 4%). Additionally, DTI did not correlate with conversion to prosthesis within different age groups: In the younger population (< 65 years) the conversion rate was 2%, 6% for the 65–80 years group, and 8% for the older group (> 80 years). Conversion to prosthesis occurred due to screw cut-out (n = 4), HHN (n = 4), infection (n = 2), iatrogenic malposition (n = 2), and non-union (n = 1).
Screw cut-out
Screw cut-out occurred in 24 cases (8%) and was diagnosed at a median of 55 days after surgery (IQR 94, range 24–726). A summary of the preoperative risk factors for cut-out can be found in Table 2. A relevant correlation with screw cut-out was found for age, DTI, and medial hinge displacement. Once a logistic regression with the independent variables was performed, the DTI retained its statistical relevance in regard to screw cut-out, while medial hinge displacement was no longer significant (p = 0.07). The average DTI for patients with screw cut-out was 1.35 (±0.11) and for patients without cut-out, 1.43 (±0.19). No cut-out occurred with a DTI of > 1.53. Gender and fracture pattern did not correlate with cut-out.
Since age played a relevant role in the occurrence of cut-out, a correlation test between DTI and screw cut-out was performed for three different age groups (< 65, 65–80, and > 80 years). Between the ages of 65 and 80, there was a significant correlation between a smaller DTI and a higher rate of screw cut-out (17% vs. 0%, p = 0.02). No correlation was found in the younger and older groups. From the total of 306 patients, a high-risk group with a cut-out rate higher than 17% was identified. This included all patients older than 80 years independently of DTI, or older than 65 years with a DTI of ≤ 1.44 (Table 3). No correlation was found between cut-out and surgical data such as quality of reduction, final neck-shaft angle, time until discharge, and wound infection rate (Table 4). The strategy chosen after the diagnosis of screw cut-out was adapted to the severity of the cut-out, resulting symptoms, age, and expectations/preferences of the patients. While in 38% of the cut-out cases physiotherapy alone was the therapy of choice, in the remaining 62% revision surgery was needed (implant removal in 33%, re-osteosynthesis with a PHILOS plate in 13%, and conversion to reverse shoulder prosthesis in 17%).
Discussion
In our sample of 306 patients, the DTI was easy to measure and had a positive correlation with older age, female gender, higher ASA score, and lower BMI. This was to be expected considering its correlation with BMD described by the proponents of the index and confirmed in subsequent independent studies [12, 14, 16]. Interestingly, a lower DTI did not correlate with fracture pattern, which remains a controversial subject with some authors confirming [17, 18] and some denying this correlation [14].
The average general complication rate was 36%, with screw cut-out being the most common complication (8%). Although there was a positive correlation between screw cut-out and a DTI of ≤ 1.44 (p = 0.003), this correlation varied widely between age groups. In the age group of 65–80, a DTI of ≤ 1.44 increased the cut-out rate from 0% to 17% (p = 0.02), while in younger ages (< 65 years) the DTI did not correlate with cut-out (Fig. 2). In the oldest group (> 80 years) cut-out rates were high, independently of the DTI (17% vs. 20%). Besides the first publication by Spross et al. on the correlation between DTI and cut-out (with 146 patients), this hypothesis has only been tested once, by Taskesen et al. (with 48 geriatric patients, 50–95 years old), in a study that failed to confirm the correlation between DTI and surgical failure [14].

A 70-year-old male patient with a right proximal humerus fracture. Anteroposterior x‑ray (a). A four-part fracture was diagnosed from the computed tomography scan (b) and a deltoid tuberosity index of 1.30 was measured. X‑ray 2 days after anatomical fixation with the PHILOS plate (c). Screw cut-out with collapse of the humeral head 120 days after surgery (d)
More than merely an academic value, the DTI has the potential to improve treatment in the trauma setting. As reported here, patients between 65 and 80 years old with a DTI of ≤ 1.44 have a significantly higher risk of developing screw cut-out and should therefore be treated with the precautions typical of the older-age population (> 80 years; Fig. 3). Recently recommended strategies for patients with high risk for failure of osteosynthesis due to osteoporosis include: restoring the medial column (if needed with addition of a fibular graft or an anterior plate); reverse drilling within the humeral head to avoid disruption of the articular surface; fixation with at least five head screws and at least one calcar screw; cement augmentation of the head screws; and careful assessment of the patients who should instead be treated primarily with a prosthetic approach since significantly lower surgical complications and better functional scores may be expected in older patients [4, 19, 20]. Moreover, conservative treatment should always be considered for high-risk patients, since good functional scores have also been achieved, for example, through non-surgical closed reduction protocols [21].

A 79-year-old male patient with right proximal humerus fracture. Three-part fracture and deltoid tuberosity index of 1.35 measured from the anteroposterior x‑ray before surgery (a). Anatomical reduction 2 days after surgery (b). Screw cut-out with reduction loss and screw dislocation 110 days after surgery (c)
Previous studies reported the relevance of an insufficient medial support (no cortical or screw support) for screw cut-out [7, 13]. In 96% of all cut-out cases there was an underlying medial hinge displacement. Although we observed a correlation between medial hinge displacement before surgery and screw cut-out, this was not confirmed in the logistic regression with multiple independent variables, such as the DTI. While the association between both three-part and four-part fractures and an inadequate reduction is often reported to correlate with surgery failure, our data failed to support such statements [6].
In 62% of the cases of screw cut-out, a revision surgery was needed, of which approximately one third of cases were converted to shoulder prosthesis. Although the DTI showed a correlation with cut-out, no correlation with its therapeutic consequence could be found. While in the group with a DTI of ≤ 1.44 a conversion to shoulder prosthesis occurred in 5% of the cases, in the rest of the population this percentage was 4% (p = n. s.). The rate of conversion to prosthesis also did not correlate with DTI in the different age groups.
Limitations, considerations, and strengths of the study
Screw cut-out was diagnosed at a median of 55 days after surgery. Our follow-up protocol recommended x‑rays after 6 weeks (42 days), which imposes a bias over the timing of diagnosis. It cannot be ruled out that the actual time of cut-out may be earlier. Similarly, asymptomatic cut-out (described to be as high as 7%) or cut-out in geriatric patients with limited mobility may remain undiagnosed [22]. Finally, an alternative x‑ray combination of AP in external rotation plus axial view in 30° (not standard in our hospital) has been reported to have a higher sensitivity for detecting screw cut-out [23]. For these reasons, it is plausible that the actual cut-out rate may be higher than the 8% we observed.
The major strength of this work is to provide a large-sample independent study of the DTI and its correlation with screw cut-out after it was first reported by its proponents in 2017. Furthermore, the combination of age groups and DTI clarifies and increases the utility of this index in the trauma setting.
Practical conclusion
-
We confirm the correlation between a low deltoid tuberosity index (DTI) and screw cut-out. This correlation alone, however, may be too simplistic and should be assessed together with the patient’s age.
-
High-risk patients for screw cut-out are those older than 65 with a DTI of ≤ 1.44 or any patient older than 80 years independently of the DTI. In these cases, the observed cut-out rate surpassed 17%.
-
Applying the DTI in the age group of 65–80 years offers relevant information for surgical planning in the trauma setting through a tool that is fast, cheap, and easy to use. Furthermore, this method does not require any additional exposure of the patient to radiation as it uses standard x‑rays.
-
Over the age of 80 years the risk of cut-out is high, independent of cortical thickness.
Abbreviations
- AO/OTA:
-
AO Foundation/Orthopaedic Trauma Association
- ASA:
-
American Society of Anesthesiology
- BMD:
-
Bone Mineral Density
- DTI:
-
Deltoid Tuberosity Index
References
Court-Brown CM, Caesar B (2006) Epidemiology of adult fractures: a review. Injury 37:691–697. https://doi.org/10.1016/j.injury.2006.04.130
DePuy Synthes 2016 PHILOS and PHILOS Long: The anatomic fixation system for the proximal humerus. https://synthes.hs.llnwd.net/o16/LLNWMB8/INT%20Mobile/Synthes%20International/Product%20Support%20Material/legacy_Synthes_PDF/207508.pdf
Murena L, Canton G, Ratti C et al (2020) Indications and results of osteosynthesis for proximal humerus fragility fractures in elderly patients. Orthop Rev (Pavia) 12:8559. https://doi.org/10.4081/or.2020.8559
McMillan TE, Johnstone AJ (2018) Primary screw perforation or subsequent screw cut-out following proximal humerus fracture fixation using locking plates: a review of causative factors and proposed solutions. Int Orthop 42:1935–1942. https://doi.org/10.1007/s00264-017-3652-6
Barlow JD, Logli AL, Steinmann SP et al (2020) Locking plate fixation of proximal humerus fractures in patients older than 60 years continues to be associated with a high complication rate. J Shoulder Elbow Surg 29:1689–1694. https://doi.org/10.1016/j.jse.2019.11.026
Krappinger D, Bizzotto N, Riedmann S et al (2011) Predicting failure after surgical fixation of proximal humerus fractures. Injury 42:1283–1288. https://doi.org/10.1016/j.injury.2011.01.017
Jung S‑W, Shim S‑B, Kim H‑M et al (2015) Factors that influence reduction loss in proximal humerus fracture surgery. J Orthop Trauma 29:276–282. https://doi.org/10.1097/BOT.0000000000000252
Schumaier A, Grawe B (2018) Proximal humerus fractures: evaluation and management in the elderly patient. Geriatr Orthop Surg Rehabil 9:2151458517750516. https://doi.org/10.1177/2151458517750516
Hertel R (2005) Fractures of the proximal humerus in osteoporotic bone. Osteoporos Int 16(Suppl 2):S65–S72. https://doi.org/10.1007/s00198-004-1714-2
Newton AW, Selvaratnam V, Pydah SK, Nixon MF (2016) Simple radiographic assessment of bone quality is associated with loss of surgical fixation in patients with proximal humeral fractures. Injury 47:904–908. https://doi.org/10.1016/j.injury.2015.12.029
Tingart MJ, Apreleva M, von Stechow D et al (2003) The cortical thickness of the proximal humeral diaphysis predicts bone mineral density of the proximal humerus. J Bone Joint Surg Br 85:611–617. https://doi.org/10.1302/0301-620x.85b4.12843
Spross C, Kaestle N, Benninger E et al (2015) Deltoid tuberosity index: a simple radiographic tool to assess local Bone quality in proximal humerus fractures. Clin Orthop Relat Res 473:3038–3045. https://doi.org/10.1007/s11999-015-4322-x
Spross C, Zeledon R, Zdravkovic V, Jost B (2017) How bone quality may influence intraoperative and early postoperative problems after angular stable open reduction-internal fixation of proximal humeral fractures. J Shoulder Elbow Surg 26:1566–1572. https://doi.org/10.1016/j.jse.2017.02.026
Taskesen A, Göçer A, Uzel K, Yaradılmış YU (2020) Effect of osteoporosis on proximal humerus fractures. Geriatr Orthop Surg Rehabil 11:2151459320985399. https://doi.org/10.1177/2151459320985399
Hertel R, Hempfing A, Stiehler M, Leunig M (2004) Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg 13:427–433. https://doi.org/10.1016/j.jse.2004.01.034
Kim DM, Park D, Kim H et al (2020) Risk factors for severe proximal humerus fracture and correlation between deltoid tuberosity index and bone mineral density. Geriatr Orthop Surg Rehabil 11:2151459320938571. https://doi.org/10.1177/2151459320938571
Koczy-Baron A, Koczy B, Mielnik M et al (2021) Influence of radiographic bone quality on the type of proximal humerus fracture. Ortop Traumatol Rehabil 23:65–77. https://doi.org/10.5604/01.3001.0014.8136
Mazzucchelli RA, Jenny K, Zdravkovic V et al (2018) The influence of local bone quality on fracture pattern in proximal humerus fractures. Injury 49:359–363. https://doi.org/10.1016/j.injury.2017.12.020
Klug A, Harth J, Hoffmann R, Gramlich Y (2020) Surgical treatment of complex proximal humeral fractures in elderly patients: a matched-pair analysis of angular-stable plating vs. reverse shoulder arthroplasty. J Shoulder Elbow Surg 29:1796–1803. https://doi.org/10.1016/j.jse.2020.01.073
Fraser AN, Bjørdal J, Wagle TM et al (2020) Reverse shoulder arthroplasty is superior to plate fixation at 2 years for displaced proximal humeral fractures in the elderly: a multicenter randomized controlled trial. J Bone Joint Surg Am 102:477–485. https://doi.org/10.2106/JBJS.19.01071
Fjalestad T, Hole MØ, Hovden IAH et al (2012) Surgical treatment with an angular stable plate for complex displaced proximal humeral fractures in elderly patients: a randomized controlled trial. J Orthop Trauma 26:98–106. https://doi.org/10.1097/BOT.0b013e31821c2e15
Little MTM, Berkes MB, Schottel PC et al (2014) The impact of preoperative coronal plane deformity on proximal humerus fixation with endosteal augmentation. J Orthop Trauma 28:338–347. https://doi.org/10.1097/BOT.0000000000000012
Spross C, Jost B, Rahm S et al (2014) How many radiographs are needed to detect angular stable head screw cut outs of the proximal humerus—a cadaver study. Injury 45:1557–1563. https://doi.org/10.1016/j.injury.2014.05.025
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Tomas Da Silva, David-Benjamin Ehrhard, Theo Manuel Chuchuy and Tobias Merkle. Statistical analysis was performed by Tomas Da Silva. The first draft of the manuscript was written by Tomas Da Silva and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
T. Da Silva, D.-B. Ehrhard, T. M. Chuchuy, C. Knop and T. Merkle declare that they have no competing interests.
This is an observational study. The Ethics Committee of the University of Tübingen has confirmed that no ethical approval is required.
Additional information
Availability of data and materials
The data presented in this study was retrospectively collected between 2008 and 2018, from the electronic files of the patients treated at our department (Department of Orthopaedics and Trauma Surgery, Klinikum Stuttgart). This data is available for independent inspection or re-evaluation at any time, given explicit permission of the Head of the Department.

Scan QR code & read article online
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Da Silva, T., Ehrhard, DB., Chuchuy, T.M. et al. Predictive value of the deltoid tuberosity index for assessing the risk of screw cut-out. Obere Extremität 18, 106–112 (2023). https://doi.org/10.1007/s11678-023-00736-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11678-023-00736-w