
Abstract
Purpose
To investigate the feasibility and dosimetric characteristics of dose painting for non-enhancing low-grade gliomas (NE-LGGs) guided by three-dimensional arterial spin labeling (3D-ASL).
Materials and methods
Eighteen patients with NE-LGGs were enrolled. 3D-ASL, T2 fluid-attenuated inversion recovery (T2 Flair) and contrast-enhanced T1-weighted magnetic resonance images were obtained. The gross tumor volume (GTV) was delineated on the T2 Flair. The hyper-perfusion region of the GTV (GTV-ASL) was determined by 3D-ASL, and the GTV-SUB was obtained by subtracting the GTV-ASL from the GTV. The clinical target volume (CTV) was created by iso-tropically expanding the GTV by 1 cm. The planning target volume (PTV), PTV-ASL were obtained by expanding the external margins of the CTV, GTV-ASL, respectively. PTV-SUB was generated by subtracting PTV-ASL from PTV. Three plans were generated for each patient: a conventional plan (plan 1) without dose escalation delivering 95–110% of 45–60 Gy in 1.8–2 Gy fractions to the PTV and two dose-painting plans (plan 2 and plan 3) with dose escalating by 10–20% (range, 50–72 Gy) to the PTV-ASL based on plan 1. The plan 3 was obtained from plan 2 without the maximum dose constraint. The dosimetric differences among the three plans were compared.
Results
The volume ratio of the PTV-ASL to the PTV was (23.49 ± 11.94)% (Z = − 3.724, P = 0.000). Compared with plan 1, D2%, D98% and Dmean of PTV-ASL increased by 14.67%,16.17% and 14.31% in plan2 and 19.84%,15.52% and 14.27% in plan3, respectively (P < 0.05); the D2% of the PTV and PTV-SUB increased by 11.89% and 8.34% in plan 2, 15.89% and 8.49% in plan 3, respectively (P < 0.05). The PTV coverages were comparable among the three plans (P > 0.05). In plan 2 and plan 3, the conformity indexes decreased by 18.60% and 12.79%; while the homogeneity index increased by 1.43 and 2 times (P < 0.05). Compared with plan 1, the D0.1 cc of brain stem and Dmax of optic chiasma were slightly increased in plan 2 and plan 3, and the absolute doses met the dose constraint. The doses of the other organs at risk (OARs) were similar among the three plans (P > 0.05).
Conclusion
The dose delivered to hyper-perfusion volume derived from 3D-ASL can increased by 10–20% while respecting the constraints to the OARs for NE-LGGs, which provides a basis for future individualized and precise radiotherapy, especially if the contrast agent cannot be injected or when contrast enhancement is uncertain.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Non-enhancing low-grade gliomas (NE-LGGs) are a special type of LGGs. Grade II Astrocytoma was the most common histological type. The vast majority of non-enhancing gliomas are LGGs, and LGGs enhanced as commonly as they lacked enhancement [1, 2]. These NE-LGGs was not enhanced on conventional enhanced computed tomography (CT) or magnetic resonance imaging (MRI). Their blood vessel wall composition is similar to that of brain-healthy tissue, with a complete blood–brain barrier. Macromolecules used for tumor enhancement cannot pass through the blood–brain barrier to enhance these lesions. Therefore, the lesions show low density on enhanced CT and T1 hypo-intensity and T2 hyper-intensity on enhanced MRI (the manifestation of edema) [3, 4]. Radiotherapy is one of the effective treatment methods for NE-LGGs, which is usually the first option for patients who are unable to operate.
Most LGGs recurrence after radiotherapy predominantly occurs in the radiation field in conventional radiotherapy, which is significantly associated with insufficient doses to the tumor target region [5, 6]. Based on conventional anatomical MR images for homogeneous dose boosting, the dose of healthy tissue increases simultaneously, and the occurrence of radiation damage is inevitable. In contrast, the dose-painting radiotherapy guided by functional images, such as functional MR and positron-emission tomography (PET), which prescripts heterogeneous dose distribution to the target volume, is expected to achieve a safe dose boost on the premise of ensuring the safety and the accuracy of dose transmission. In a prospective phase II randomized clinical trial, it investigated the region of hyper-perfused/hyper-cellular (TVHCV/TVCBV) > 1 cm3 in high b-value diffusion-weighted MRI and dynamic contrast-enhanced perfusion (DCE) MRI for glioblastoma with dose boosting (75 Gy/30 f) and found that patients treated to the combined hyper-cellular/hyper-perfused tumor volume had significantly improved 12-month overall survival (OS) rate (92%; 95% CI 78–100%) compared with historical control (P = 0.03). However, there was no significant difference in 12-month OS between patients boosted to the hyper-cellular tumor volume alone vs historical control (P = 0.9) with favorable outcomes for neurocognitive function, symptom burden, and quality of life [7].
At present, the abnormal hyper-intensity (edema area) on T2 fluid-attenuated inversion recovery (T2 Flair) is usually used as the standard for delineating gross tumor volume (GTV), which can ensure the coverage of radiotherapy dose to tumor, but it is challenge to increase the radiotherapy dose due to the large irradiation range. Although the tumor boundary of NE-LGGs is difficult to identify in conventional imaging, the blood flow and metabolism of the tumor are still significantly different from those of the brain tissue in the edema area in biology [8]. Quantifying this difference through functional imaging can clarify the distribution of tumor cell enrichment areas, which could guide the delineation of target volume during radiotherapy. Commonly functional imaging, including dynamic susceptibility contrast MRI (DSC), DCE or PET, requires intravenous administration of a contrast agent and is therefore somewhat limited.
As a non-invasive blood perfusion imaging technology, three-dimensional arterial spin labeling (3D-ASL) generates an image by magnetically labeling water molecules as an endogenous tracer. It does not require the destruction of the blood–brain barrier and can reflect microscopic changes in tissue blood perfusion and micro-vessel density [9, 10]. 3D-ASL perfusion imaging can effectively distinguish intracranial tumors from non-neoplastic lesions more sensitive than conventional MR sequences for the detection of tumor progression or recurrence [11,12,13]. The tumor cerebral blood flow (CBF) value is significantly negatively correlated with survival [14]. ASL has been used to guide stereotactic biopsy and operation for glioma. Jin et al. [15] showed that compared with conventional MRI, combined magnetic resonance spectroscopy (MRS) and ASL improved the accuracy of target selection for the stereotactic biopsy of intracranial tumors, especially three cases each of low-enhancing and non-enhancing gliomas. Lindner et al. [16] concluded that intraoperative ASL was a feasible, reproducible, and reliable tool to map CBF in brain tumors and seemed to give beneficial information compared to conventional intraoperative MRI in partial resection.
3D-ASL has been widely used in the diagnosis, grading and efficacy evaluation of gliomas [17, 18]. However, there are few reports on its application in guiding the radiotherapy planning of NE-LGGs. In this study, we investigated whether dose painting for NE-LGGs can achieve dose escalation to hyper-perfusion region derived from 3D-ASL without increasing the dose to cranial organs at risk (OARs).
Materials and methods
Patients
This study enrolled 18 patients between December 2018 and May 2021. Eligibility criteria: (1) Low-grade glioma confirmed by histopathology and molecular characteristics; (2) no enhancement on enhanced CT and MR; (4) 3D-ASL scanning prior to treatment. Patients, including 12 (67%) males and 6 (33%) females, with an average age of 42 ± 21 years (5 to 74 years). Radiological studies performed on the patients were accessed by two neuroradiologists from Picture Archiving and Communication Systems (PACS). WHO grading was reviewed by three neuropathologists according to the fifth edition of the WHO Classification of Tumors of the Central Nervous System (WHO CNS5) [19]. Patient’s characteristics are presented in Table 1.
CT and MRI images acquisition
CT
A CT scanner (Brilliance Big Bore, Philips, Netherlands) with a slice thickness of 3 mm and no inter-slice gap width was used, scanning from the foramen magnum to the end of the skull in a caudo-cranial direction.
MRI
All MR images (T2 Flair, 3D-ASL and contrast-enhanced T1-weighted (CE-T1W)) were acquired with the same 3.0 T MR scanner (Discovery 750 W, GE Healthcare, USA) using a standard 8-channel cranial coil. For CE-T1W images, gadopentetate dimeglumine was injected at doses standardized by patient’s body weight (0.2 mL/kg) at 2 mL/s, and the scan was started 3–5 min after the injection. The common scan parameters for all sequences are shown in Table 2.
3D-ASL data acquisition and post-processing
Setting a marking plane on the neck in advance, labeling with pseudo-continuity, image acquisition with single-shot gradient-echo echo planar imaging (EPI), labeling duration = 1500 ms, post spin labeling delay (PLD) = 2025 ms, number of excitation (NEX) = 3, forty pairs of control/label images were acquired and averaged. The scan duration was 5:27. For measurement of the magnetization of arterial blood and also for segmentation purposes, an M0 calibration image was acquired separately with the same geometry and the same imaging parameters as the ASL without labeling. Background suppression technology was used in the process of image acquisition.
The raw 3D-ASL data were transferred to the GE Advantage Workstation 4.7 and post-processed in the FuncTool environment. The motion correction, temporal and spatial filtering, and partial volume effect correction were performed. Subsequently, the CBF values were calculated by intensity normalization. A quantitative CBF map was generated based on the following Equation [20]:
where λ is the brain/blood partition coefficient in ml/g, SIcontrol and SIlabel are the time-averaged signal intensities in the control and label images, respectively, T1,blood is the longitudinal relaxation time of blood in seconds, α is the labeling efficiency, SIPD is the signal intensity of a proton density-weighted image, τ is the label duration, and PLD is the post-labeling delay. The parameters used in the present study were: λ = 0.9, T1,blood = 1650 ms, α = 0.85, τ = 1500 ms and PLD = 2025 ms. The SIPD was derived from the echo planar imaging M0 images. The factor of 6000 converts the units from ml/g/s to ml/100 g/ min, which is customary in the physiological literature.
Target volume delineation
All MRI images were imported into MIM Maestro software (6.8.8, USA). GTV-ASL was defined as the high-perfusion volume with a relative CBF value greater than 1.4 in 3D-ASL images, where the relative CBF value was the CBF ratio of tumor to contralateral mirror gray matter (the unilateral cerebral hemisphere) or normal gray matter of the left insula lobe (midline or widely diffuse distribution), as previously published [21]. An automatic threshold method was used to generate GTV-ASL, and a senior radiologist later reviewed and modified the report as needed. Axial T2 Flair sequences were used to contour the hyper-intense abnormality as the GTV. The GTV-SUB was obtained by subtracting the GTV-ASL from the GTV.
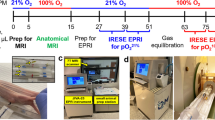
Clinical target volumes (CTV) were created by iso-tropically expanding the GTV by 1 cm. The planning target volume (PTV) and PTV-ASL were generated by adding a 0.5 and 0.3 cm margin to CTV and GTV-ASL, respectively. The PTV-SUB was obtained by subtracting the PTV-ASL from the PTV. The PTV-ASL was used to generate simultaneous integrated boost (SIB) volume. OARs used for treatment planning were: eyeballs, lenses, optic nerves, optic chiasma and brain stem. Figure 1A, B shows the target volumes delineated for two patients with NE-LGGs.

A, B Target volumes shown on a three-dimensional arterial spin labeling (3D-ASL), b fusion image of contrast-enhanced T1-weighted imaging (CE-T1WI) and 3D-ASL, c T2 fluid-attenuated inversion recovery (T2 Flair), and d fusion image of T2 Flair and 3D-ASL for two patients with non-enhancing low-grade gliomas (NE-LGGs) located in the left temporal lobe (A) and in the thalamus (B). GTV-ASL, the high-perfusion region on 3D-ASL; GTV, the hyper-intense abnormality on T2 Flair (conventional GTV); CTV clinical target volume, PTV the planning target volume
Radiotherapy planning
All treatment plans were designed in the Eclipse (Version 15.6, Varian, USA) treatment planning system using static intensity-modulated radiotherapy (IMRT). Three plans were generated for each patient: a conventional plan (plan 1) without dose escalation delivering 95–110% of 45–60 Gy in 1.8–2 Gy fractions to the PTV and two dose-painted plans (plan 2 and plan 3) with dose escalating by 10–20% (range, 50–72 Gy) to the PTV-ASL based on plan 1. Plan 1 and plan 2 were generated with the maximum dose constraint of 110% of the prescription dose, and the plan 3 was obtained from plan 2 without the maximum dose constraint. The prescription covered 95% of the target volume. The prescription dose ultimately depended on the location of tumor. Seven patients with unilateral hemispheric tumors were prescribed 60 Gy in plan 1, and the dose of PTV-ASL increased by 20% (72 Gy) in plans 2 and 3. For other patients, the prescription doses were relatively limited because the tumors were located in important functional areas such as the midline of the brain or widely distributed. The prescription doses were 45–54 Gy in plan 1, and the dose of PTV-ASL increased by 10–20% (50–60 Gy) in plan 2 and plan 3.
The dose normalizations were set to the average dose of PTV in plan 1 and PTV-ASL in plans 2 and plan 3. The field angles were constant for all three treatment plans. Dose calculation was performed in anisotropic analytical algorithm optimization mode (AAA, version 15.512) using 6 MV X-rays. The calculated grid size was 2.5 mm × 2.5 mm.
The doses of OARs were restricted as following: brain stem D0.1 cc (the dose to 0.1 cc target volume) ≤ 54 Gy, eyeballs Dmax (the maximum dose) < 45 Gy, lens Dmax < 10 Gy, and optic nerves and optic chiasm Dmax ≤ 55 Gy.
Evaluation of treatment plans
To compare the three treatment plans, cumulative dose–volume histograms (DVHs) were calculated for all target volumes and OARs for all patients. The D2% and D98% (where Dx indicates the dose to x% of the target volume) as well as average dose (Dmean) were compared for the PTV, PTV-SUB and PTV-ASL. Furthermore, the target coverage, conformity index (CI) and homogeneity index (HI) were calculated. A CI close to one indicates that the shape of the region receiving the reference dose closely matches the shape of the target region, and an HI close to zero indicates good uniformity. The formulas for calculating CI and HI are as follows:
where Vt represents the volume of the target region, Vt,ref represents the volume of the target region covered by the reference dose, and Vref represents the volume of all regions covered by the reference dose. The flow chart of this study is as shown in Fig. 2.

The working flow chart. MRI, magnetic resonance imaging, CT computed tomography, T2 Flair T2 fluid-attenuated inversion recovery, 3D-ASL three-dimensional arterial spin labeling, CE-T1W contrast-enhanced T1-weighted; GTV gross tumor volume, GTV-ASL the high-perfusion region on 3D-ASL, CTV clinical target volume, PTV planning target volume
Statistical analyses
Statistical analyses were performed using SPSS (IBM, version 25.0). Comparisons between two groups were done with paired t tests or Wilcoxon tests, depending on the distribution defined by the Shapiro–Wilk normality test. Comparisons of multiple groups were performed by 2-way analysis of variance (ANOVA), followed by least significant difference (LSD) and Friedman two-way ANOVA, followed by Friedman multiple comparison tests, depending on Levene’s test of variance homogeneity. All data were expressed as mean ± standard deviation, and P < 0.05 was considered as a significant difference.
Results
Comparison of target volumes
The volumes of the PTV and PTV-ASL were 383.95 ± 255.69 cm3 and 90.06 ± 92.03 cm3, respectively. The volume ratio of the PTV-ASL to the PTV was (23.49 ± 11.94) % (Z = -3.724, P = 0.000). Technically, it was feasible to escalate the dose to hyper-perfusion target volume up to 72 Gy without violating dose constraints of normal tissues and, meanwhile, to ensure prescribed doses to the PTVs. Figure 3 shows an example of the dose distribution for the three plans for a sample patient. Figure 4 shows the DVHs of sample target volumes and OARs.

Isodose lines are shown for conventional plan (plan 1) and dose-painted plans (plan 2 and plan 3). Plan 1 (a and d): prescribed a homogeneous dose of 60 Gy to the PTV; plan 2 (b and e) and plan3 (c and f): the dose of PTV-ASL increased by 20% (equivalent to 72 Gy) based on plan 1, without the maximum dose constraint in plan 3. In a, b, c dose distribution is projected on the computed tomography (CT) images while in d, e, f dose distribution is projected on the three-dimensional arterial spin labeling (3D-ASL) images

The dose-volume histograms (DVHs) of three treatment plans. The DVHs of the target regions and organs at risks (OARs) are shown in (a, b) respectively. PTV planning target volume
Dosimetric comparison of target volumes among the three plans
The doses of the PTV, PTV-SUB and PTV-ASL increased in plan 2 and plan 3 than plan 1. The D2% increased by 11.89%, 8.34%, and 14.67% in plan 2 and 15.89%, 8.49%, and 19.84% in plan 3, respectively, with statistically significant differences (P < 0.05); the D98% increased by 1.12%, 0.93%, and 16.17% in plan 2 and 0.7%, 0.49%, 15.52% in plan 3, respectively, but only increased significantly for the PTV-ASL in plans 2 and 3 (P < 0.05); and Dmean increased by 5.15%, 3.60%, and 14.31% in plan 2 and 4.62%, 2.71%, and 14.27% in plan 3, respectively, with statistically significant differences (P < 0.05) except for the PTV in plan 3.
Compared with plan 2, the D2% of the PTV, PTV-SUB and PTV-ASL increased by 3.58%, 0.51% and 4.52% in plan 3, respectively, with statistically significant differences for the PTV and PTV-ASL (P < 0.05); D98% and Dmean decreased by 0.41%, 0.43%, and 0.56% and 0.50%, 0.86%, and 0.03%, respectively, with no statistically significant differences (P > 0.05), as shown in Table 3 and Fig. 5.

Dosimetric comparison of target volumes among plan 1 (blue), plan 2 (orange) and plan 3 (purple). Compared with plan 1, the dose escalated more significantly in PTV-ASL than PTV-SUB in plan 2 and plan 3. The asterisk (*) indicates P < 0.05
Plan evaluation
The PTV target coverages for plan 1, plan 2 and plan 3 were comparable (98.45% ± 2.16% vs. 98.70% ± 2.31% vs. 98.20% ± 2.31%, P > 0.05). Compared with plan 1, the CIs decreased by 18.60% in plan 2 and 12.79% in plan 3, respectively, with statistically significant differences (P < 0.05), while the CIs were comparable between plan 2 and plan 3 (P > 0.05). Compared with plan 1, the HIs increased by 1.43 times in plan 2 and 2 times in plan 3, respectively; and increased by 23.53% in plan 3 than in plan 2 (P < 0.05).
Dosimetric comparison of OARs among three plans
Compared to plan 1, the brain stem D0.1 cc and optic chiasma Dmax were slightly increased by 3.98% and 4.33% in pan 2, and 4.52% and 6.27% in plan 3 respectively, with statistically significant differences (P < 0.05), while the absolute doses were safe. The Dmax of the eyeballs, lens, and optic nerves were comparable among plan 1, plan 2, and plan 3 (P > 0.05), as shown in Table 4.
Discussion
Previous study confirmed that MR 3D-ASL images can be used to quantify and analyze tumor perfusion differences in NE-LGGs, and that sub-volume segmentation of the GTV can be performed based on this perfusion difference [21]. In this study, the dose delivered to hyper-perfusion volume derived from 3D-ASL can increased by 10–20% while respecting the constraints to the OAR for NE-LGGs using of SIB technique.
Many LGGs inevitably develop into malignant high-grade gliomas, and even with effective treatment, the survival rate of patients with LGGs remains poor [22, 23]. Radiotherapy can delay the malignant transformation of LGGs, improve the local control rate of tumor, and improve the survival rate and quality of life of patients.
Previously prospective clinical trials, such as EORTC 22,844 (45 vs. 59.4 Gy) and NCCTG 86–72-51 (50.4 vs. 64.8 Gy), showed that high-dose radiotherapy did not improve the survival of patients with LGGs, but rather increased the risk of radiation necrosis and reduced the quality of life [24, 25]. However, Liu et al. [26, 27] demonstrated high-dose radiotherapy (≥ 54 Gy) improved the survival of LGGs, especially for patients with an IDH mutation/1p/19q non-co-deletion or IDH wild-type, while no radio-toxicity was reported in these retrospective studies. Therefore, increasing the radiation dose can improve the survival rates of LGGs patients with special molecular subtypes. And in this study, more than 70% the participants were patients with IDH wild-type LGGs, which may need to be considered for high-dose radiotherapy. High-dose radiotherapy often indicates high local control and efficacy, while synchronously increased the risk of radiation damage to surrounding normal tissues. How to safely and effectively escalate the dose of tumor target volume was the purpose of our study.
NE-LGGs, as a special type of LGGs with significant heterogeneity, require an individualized radiotherapy dose for the tumor target volume. Jakola et al. [28] showed that malignant transformation occurs locally and within the T2WI hyper-intensities in most NE-LGGs patients, and the region of malignant transformation in a new significant contrast enhancement due to the disruptive blood–brain barrier, was much smaller than the edema area. Although coverage of the radiotherapy dose to the tumor can be guaranteed if the edema area is directly defined as the GTV of the NE-LGGs, it is difficult to increase the radiotherapy dose due to the large irradiation range. However, we found that NE-LGGs showed no abnormalities on CE-T1W MRI but showed local high perfusion on 3D-ASL. And all the local hyper-perfusion regions were within edema areas through the fusion images of T2 Flair and 3D-ASL. The study also found that the volume of the hyper-perfusion region (GTV-ASL) was significantly smaller than the volume of the edema area (GTV) by analyzing target volumes. The target volume of dose escalation guided by 3D-ASL was smaller than conventional radiotherapy. Under the same prescription dose, the dose of surrounding healthy tissues is lower. Therefore, it is more conductive to dose escalation ensuring that surrounding healthy tissues were not damaged.
3D-ASL is a functional MRI that does not depend on the destruction of the blood–brain barrier and the paramagnetic contrast agent. It has the advantages of being non-invasive, low cost, simple to operate, and repeatable, and effectively avoids the potential risks caused by an exogenous contrast agent [29]. Related studies have shown that the CBF determined by 3D-ASL is significantly positively correlated with micro-vessel density (ρ = 0.567; P = 0.029) and vascular endothelial growth factor expression (r = 0.604; P < 0.001) but significantly negatively correlated with survival (r = -0.714, P < 0.001) and can be an independent risk factor for OS (HR = 1.028; P = 0.010) [14, 30]. More malignant tumor zones tend to have higher tumor blood flow (TBF). Chekhonin et al. [31] have shown that ASL perfusion revealed higher TBF in active tumor growth region compared to peri-focal infiltrative edema zone. Meanwhile, Vallatos et al. [32]also revealed a negative correlation between tumor cell infiltration and perfusion at the tumor margins (P = 0.0004) by MRI/histology voxel-to-voxel comparison, and concluded that the quantitative relationship between tumor cell density and perfusion identified surrounding macroscopic tumor could be used to detect marginal tumor cell infiltration with greater accuracy. We defined the high-perfusion region derived from 3D-ASL in GTV as a high-risk region, which was conducted to SIB.
In this study, plan 1 was the conventional plan, and plan 2 and plan 3 were dose-painted plans. Compared with plan 1, the D2%, D98% and Dmean of the PTV-ASL increased by more than 14% in plan 2 and plan 3; however, these values increased by less than 9% in the PTV-SUB, with D98% increased by less than 1%. This suggested that under the guidance of 3D-ASL, the dose-painted plan can achieve a significant dose boost in hyper-perfused sub-volume region for NE-LGGs while having less impact on the peripheral dose and avoiding dose boost blindness. This is similar to the study of Thureau et al., which was based on 18Flourodeoxyglucose (18FDG) PET-CT image-guided dose boost for locally advanced non-small-cell lung cancer [33]. The dose to high recurrence risk areas increased by 12.12% without increasing the radiation dose to OARs, whereas the doses to other areas of the GTV only increased by 2.88%. We also found that the D2% of the PTV, PTV-SUB and PTV-ASL gradually increased in plan 1, plan 2 and plan 3, while the D98% and Dmean of each target region were comparable between plan 2 and plan 3. Thus, the elimination of maximum dose constraints is favorable to boost the maximum dose but has no significant effect on the minimum or average dose.
The target coverages of the PTV were comparable among plan 1, plan 2 and plan 3, with the prescribed isodose line wrapping around approximately 95% of the PTV, indicating that all treatment plans for plan 2 and plan 3 met the minimum dose requirements of the target region. Because only the local hyper-perfused regions on 3D-ASL were escalated in plan 2 and plan 3, whereas the edema areas surrounding the hyper-perfused regions received standard doses, the HIs were larger in plan 2 and plan 3 than in plan 1. In this study, the conformality and homogeneity of plan 2 and plan 3 decreased. However, the dose to the tumor target region was significantly increased. Therefore, reducing the homogeneity of the radiation dose is beneficial for dose escalation and protecting OARs.
During radiotherapy for patients with NE-LGGs, radiation damage to surrounding healthy tissues should not be ignored. The dose boost to the tumor target region must be balanced with protecting OARs. The results of this study showed that the dose delivered to OARs was comparable among the three treatment plans, except for brain stem and optic chiasma. However, the absolute doses of all OARs were within a safe range. In addition, the constrained boost plan outperformed the unconstrained plan in terms of OAR protection.
The main limitations of our study were as follows: (1) The number of enrolled patients is relatively small, due to the low incidence of NE-LGGs. Meanwhile, most of patients were operated. Due to the destruction of the blood–brain barrier, the post-operative area was frequently enhanced on enhanced MRI, which cannot be enrolled in the study. (2) Although this is a preclinical technical study, it lays a foundation for future studies on the impact of this technology on the progression free survival (PFS) and OS.
Conclusion
The dose delivered to hyper-perfusion volume derived from 3D-ASL can increased by 10–20% while respecting the constraints to the OARs for NE-LGGs, which provides a basis for future individualized and precise radiotherapy, especially if the contrast agent cannot be injected or when contrast enhancement is uncertain.
Abbreviations
- LGGs:
-
Non-enhancing low-grade gliomas
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- PET:
-
Positron-emission tomography
- DCE:
-
Dynamic contrast-enhanced
- OS:
-
Overall survival
- T2 Flair:
-
T2 fluid-attenuated inversion recovery
- GTV:
-
Gross tumor volume
- DSC:
-
Dynamic susceptibility contrast
- 3D-ASL:
-
Three-dimensional arterial spin labeling
- CBF:
-
Cerebral blood flow
- MRS:
-
Magnetic resonance spectroscopy
- PACS:
-
Picture Archiving and Communication Systems
- WHO CNS5:
-
The fifth edition of the WHO Classification of tumors of the central nervous system
- NOS:
-
Not otherwise specified
- IDH:
-
Isocitrate dehydrogenase
- CE-T1W:
-
Contrast-enhanced T1-weighted
- EPI:
-
Echo planar imaging
- PLD:
-
Post-spin labeling delay
- NEX:
-
Number of excitation
- TR:
-
Repetition time
- TE:
-
Echo time
- FOV:
-
Field of view
- OARs:
-
Organs at risk
- CTV:
-
Clinical target volume
- PTV:
-
Planning target volume
- SIB:
-
Simultaneous integrated boost
- IMRT:
-
Intensity-modulated radiotherapy
- DVHs:
-
Dose–volume histograms
- Dx :
-
The dose to x% of the target volume
- Dmax :
-
The maximum dose
- Dmin :
-
The minimum dose
- Dmean :
-
The average dose
- CI:
-
Conformity index
- HI:
-
Homogeneity index
- ANOVA:
-
Analysis of variance
- LSD:
-
Least significant difference
- 18FDG:
-
18Flourode oxyglucose
References
Eichberg DG, Di L, Morell AA, Shah AH, Semonche AM, Chin CN, et al. Incidence of high-grade gliomas presenting as radiographically non-enhancing lesions: experience in 111 surgically treated non-enhancing gliomas with tissue diagnosis. J Neurooncol. 2020;147(3):671–9.
Scott JN, Brasher PM, Sevick RJ, Rewcastle NB, Forsyth PA. How often are nonenhancing supratentorial gliomas malignant? A population study. Neurology. 2002;59(6):947–9.
Afra D, Osztie E. Histologically confirmed changes on CT of reoperated low-grade astrocytomas. Neuroradiology. 1997;39(11):804–10.
Upadhyay N, Waldman AD. Conventional MRI evaluation of gliomas. Br J Radiol. 2011;84(Spec Iss 2):S107–11.
Jaspers JPM, Méndez Romero A, Wiggenraad R, Compter I, Eekers DBP, Nout RA, et al. Pattern of failure in IDH mutated, low grade glioma after radiotherapy-Implications for margin reduction. Radiother Oncol. 2021;156:43–8.
Kamran SC, Dworkin M, Niemierko A, Bussiere M, Oh KS, Loeffler JS, et al. Patterns of failure among patients with low-grade glioma treated with proton radiation therapy. Pract Radiat Oncol. 2019;9(4):e356–61.
Kim MM, Sun Y, Aryal MP, Parmar HA, Piert M, Rosen B, et al. A phase 2 study of dose-intensified chemoradiation using biologically based target volume definition in patients with newly diagnosed glioblastoma. Int J Radiat Oncol Biol Phys. 2021;110(3):792–803.
Galldiks N, Niyazi M, Grosu AL, Kocher M, Langen KJ, Law I, et al. Contribution of PET imaging to radiotherapy planning and monitoring in glioma patients—a report of the PET/RANO group. Neuro Oncol. 2021;23(6):881–93.
Grade M, Hernandez Tamames JA, Pizzini FB, Achten E, Golay X, Smits M. A neuroradiologist’s guide to arterial spin labeling MRI in clinical practice. Neuroradiology. 2015;57(12):1181–202.
Telischak NA, Detre JA, Zaharchuk G. Arterial spin labeling MRI: clinical applications in the brain. J Magn Reson Imaging. 2015;41(5):1165–80.
Soni N, Srindharan K, Kumar S, Mishra P, Bathla G, Kalita J, et al. Arterial spin labeling perfusion: Prospective MR imaging in differentiating neoplastic from non-neoplastic intra-axial brain lesions. Neuroradiol J. 2018;31(6):544–53.
Nyberg E, Honce J, Kleinschmidt-DeMasters BK, Shukri B, Kreidler S, Nagae L. Arterial spin labeling: Pathologically proven superiority over conventional MRI for detection of high-grade glioma progression after treatment. Neuroradiol J. 2016;29(5):377–83.
Ozsunar Y, Mullins ME, Kwong K, Hochberg FH, Ament C, Schaefer PW, et al. Glioma recurrence versus radiation necrosis? A pilot comparison of arterial spin-labeled, dynamic susceptibility contrast enhanced MRI, and FDG-PET imaging. Acad Radiol. 2010;17(3):282–90.
Pang H, Dang X, Ren Y, Zhuang D, Qiu T, Chen H, et al. 3D-ASL perfusion correlates with VEGF expression and overall survival in glioma patients: comparison of quantitative perfusion and pathology on accurate spatial location-matched basis. J Magn Reson Imaging. 2019;50(1):209–20.
Jin T, Ren Y, Zhang H, Xie Q, Yao Z, Feng X. Application of MRS- and ASL-guided navigation for biopsy of intracranial tumors. Acta Radiol. 2019;60(3):374–81.
Lindner T, Ahmeti H, Lübbing I, Helle M, Jansen O, Synowitz M, et al. Intraoperative resection control using arterial spin labelling—proof of concept, reproducibility of data and initial results. Neuroimage Clin. 2017;15:136–42.
Falk Delgado A, De Luca F, van Westen D, Falk DA. Arterial spin labeling MR imaging for differentiation between high- and low-grade glioma-a meta-analysis. Neuro Oncol. 2018;20(11):1450–61.
Xu Q, Liu Q, Ge H, Ge X, Wu J, Qu J, et al. Tumor recurrence versus treatment effects in glioma: a comparative study of three-dimensional pseudo-continuous arterial spin labeling and dynamic susceptibility contrast imaging. Medicine (Baltimore). 2017;96(50):e9332.
Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol. 2021;23(8):1231–51.
Buxton RB, Frank LR, Wong EC, Siewert B, Warach S, Edelman RR. A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med. 1998;40(3):383–96.
Zhu Z, Gong G, Wang L, Su Y, Lu J, Yin Y. Three-dimensional arterial spin labeling-guided sub-volume segmentation of radiotherapy in adult nonenhancing low-grade gliomas. Front Oncol. 2022;12:914507.
Jooma R, Waqas M, Khan I. Diffuse low-grade glioma - changing concepts in diagnosis and management: a review. Asian J Neurosurg. 2019;14(2):356–63.
Obara T, Blonski M, Brzenczek C, Mézières S, Gaudeau Y, Pouget C, et al. Adult diffuse low-grade gliomas: 35-year experience at the nancy france neurooncology unit. Front Oncol. 2020;10:574679.
Karim AB, Maat B, Hatlevoll R, Menten J, Rutten EH, Thomas DG, et al. A randomized trial on dose-response in radiation therapy of low-grade cerebral glioma: European organization for research and treatment of cancer (EORTC) study 22844. Int J Radiat Oncol Biol Phys. 1996;36(3):549–56.
Breen WG, Anderson SK, Carrero XW, Brown PD, Ballman KV, O’Neill BP, et al. Final report from Intergroup NCCTG 86–72-51 (Alliance): a phase III randomized clinical trial of high-dose versus low-dose radiation for adult low-grade glioma. Neuro Oncol. 2020;22(6):830–7.
Liu S, Liu Y, Li G, Feng J, Chen L, Qiu X. High-dose radiation associated with improved survival in IDH-wildtype low-grade glioma. Chin Neurosurg J. 2021;7(1):22.
Liu Y, Liu S, Li G, Li Y, Chen L, Feng J, et al. Association of high-dose radiotherapy with improved survival in patients with newly diagnosed low-grade gliomas. Cancer. 2022;128(5):1085–92.
Jakola AS, Bouget D, Reinertsen I, Skjulsvik AJ, Sagberg LM, Bø HK, et al. Spatial distribution of malignant transformation in patients with low-grade glioma. J Neurooncol. 2020;146(2):373–80.
Furtner J, Bender B, Braun C, Schittenhelm J, Skardelly M, Ernemann U, et al. Prognostic value of blood flow measurements using arterial spin labeling in gliomas. PLoS ONE. 2014;9(6):e99616.
Ningning D, Haopeng P, Xuefei D, Wenna C, Yan R, Jingsong W, et al. Perfusion imaging of brain gliomas using arterial spin labeling: correlation with histopathological vascular density in MRI-guided biopsies. Neuroradiology. 2017;59(1):51–9.
Chekhonin IV, Batalov AI, Zakharova NE, Pogosbekyan EL, Nikitin PV, Bykanov AE, et al. Magnitno-rezonansnaya relaksometriya v otsenke subregionov gliom golovnogo mozga vysokoi stepeni zlokachestvennosti—neirovizualizatsionnye i morfologicheskie korrelyaty [magnetic resonance relaxometry in high-grade glioma subregion assessment–neuroimaging and morphological correlates]. Zh Vopr Neirokhir Im N N Burdenko. 2021;85(4):41–8.
Vallatos A, Al-Mubarak HFI, Birch JL, Galllagher L, Mullin JM, Gilmour L, et al. Quantitative histopathologic assessment of perfusion MRI as a marker of glioblastoma cell infiltration in and beyond the peritumoral edema region. J Magn Reson Imaging. 2019;50(2):529–40.
Thureau S, Dubray B, Modzelewski R, Bohn P, Hapdey S, Vincent S, et al. FDG and FMISO PET-guided dose escalation with intensity-modulated radiotherapy in lung cancer. Radiat Oncol. 2018;13(1):208.
Funding
This work was supported by the Start-up fund of Shandong Cancer Hospital (YYPY2020-016), and the Key Research and Development Program of Shandong Major Science & Technology Innovation Project (2021SFGC0501).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Institutional ethics review board approval was obtained, and informed consent was waived for this retrospective study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Zhu, Z., Gong, G., Wang, L. et al. Three-dimensional arterial spin labeling-guided dose painting radiotherapy for non-enhancing low-grade gliomas. Jpn J Radiol 41, 335–346 (2023). https://doi.org/10.1007/s11604-022-01357-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-022-01357-z