
Abstract
The assessment of rotator cuff tear prior to shoulder replacement is based on the physical findings and imaging procedures, preferably magnetic resonance imaging (MRI). However, MRI is not always available, and in trauma patients, the CT-scan-based classification of glenohumeral arthritis or tendon damage is generally not applicable. In case of 4-part dislocated proximal humerus fractures the right diagnosis is crucial prior to choose between different type protheses or osteosyntheses. Therefore, there is a need for novel methods for the evaluation of rotator cuff damage. Our aim was to evaluate whether differential scanning calorimetry (DSC) could determine the grade of rotator cuff damage in patients undergoing shoulder replacement. Small samples of rotator cuff tendons of patients undergoing reversed shoulder replacement due to orthopedic or trauma indications were resected during surgery, and thermal parameters were measured using DSC. Radiological evaluation was also performed to classify the degree of rotator cuff damage and glenohumeral arthritis. In case of orthopedic samples, the consequence of advanced tendon damage was well demonstrated by the shape and the running of the curves, compared to the control sample. In trauma samples, the moderately degenerated tendons also exhibited significant difference from the control in the shape of the scans and in the thermal parameters. DSC curves demonstrated a clear difference in the thermal parameters of healthy and pathologic samples. DSC could be a useful additional method in the evaluation of rotator cuff tear arthropathies in future studies.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Rotator cuff arthropathy (RCA) is a common degenerative condition, ultimately leading to need for surgery and total shoulder replacement. The preoperative diagnosis is usually based on the physical findings and imaging procedures, preferably magnetic resonance imaging (MRI) or ultrasound (US) [1]. Since the first shoulder prosthesis developed by Neer in 1955 [2], the surgical techniques and instruments have been through a great evolution [3].
Nowadays a wide variety of shoulder prostheses are available, for both primary arthritis (rotator cuff tear arthropathy) and trauma indications [4,5,6]. The diagnostic procedures for degenerative arthropathies are well described and allows time for the medical team; however, in case of acute traumas (i.e. dislocated 4-part fractures and Neer VI type fractures with humeral head dislocation) less time is available for preparation. Furthermore, in case of trauma patients for the right choice of surgical implant, osteoporosis, existing arthritis and importantly, rotator cuff damage should be considered [7,8,9].
According to the literature, MRI supposed to be the gold-standard for the evaluation of the rotator cuff [1], however, magnetic imaging is not always feasible. Presence of older metallic implants or patient factors, such as claustrophobia could limit the application of MRI in the preoperative process. Other methods, including histology, are accurate but time-consuming procedures.
Therefore, there is a need for novel methods to further evaluate the condition of rotator cuff damage and help clinical decision for the choice of the right prosthesis implantation.
Recent studies have demonstrated that the differential scanning calorimetry (DSC) is a useful tool in the investigation of tendons and joint capsules in degenerative and inflammatory diseases [10, 11].
We hypothesized that differential scanning calorimetry could determine the grade of rotator cuff damage in patients undergoing shoulder replacement, providing more insight into the structural changes of the examined tissue samples.
Materials and methods
Sample collection
The 5 × 5 × 10 mm sized sample of the rotator cuff was resected during total reversed shoulder replacement. We preferably harvested supraspinatus tendon, approximately 1–1.5 cm proximal from the insertion into the superior facet of greater tubercle of humerus. Then, samples were properly stored for further measurements, as described in details elsewhere [11]. The rotator cuff samples—three from each different medical stages—were obtained patients whom underwent reversed shoulder replacement: (1) due to acute trauma (4-part dislocated or Neer Type VI proximal humerus fractures (samples A2–A4), (2) due to rotator cuff tear arthropathy (samples B1, B2) (Figs. 1a–b, 2a–c). The control sample (originally labeled as A1) was collected from a young patient with dislocated 4-part proximal humerus fracture and was considered macroscopically as a healthy tendon. This finding was confirmed by histological examination. All of these samples were considered as waste from the point of surgery.

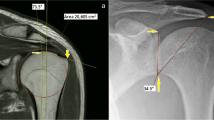
Rotator cuff tear arthropathy. Conventional X-ray (left: AP view) and CT-scan (right: CT)

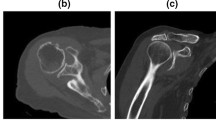
4-Part, dislocated, fragmentary articular fracture (Type Neer VI). left: CT-scan. Axial plane, middle: CT-scan. Coronal plane, right: CT-scan, 3D reconstruction
All procedures followed were in accordance with the ethical standards of the responsible Regional and Institutional Research Ethics Committee and with the Declaration of HELSINKI 1975, as revised in 2008.
Clinical and radiological evaluation of rotator cuff damage
Based on patient history and results of the physical examination on case of RCA patients, an individual score system was applied to assess the potential level of rotator cuff damage. Samples of RCA or trauma origin were also macroscopically assessed, looking for signs of rotator cuff injury.
The rotator cuff tendon damage was scored with Hamada classification [12, 13], for evaluation of primary arthropathies and cartilage damage, Walch [14] and Outerbridge [15, 16] classifications were used, respectively. Radiological analysis of conventional X-rays, CT (Siemens Somatom Perspective Dual 64/128) and MRI (Siemens Magnetom Essenza 1.5 T) images was performed by using Siemens Syngo.via software (Siemens Healthineers Global).
Histological processing
The rotator cuff samples were fixed in 4% formaldehyde for at least 2 days. After fixation two representative sections from each sample were cut. Then the tissues were dehydrated and embedded in paraffin according to the standard histopathological processing and 4-μm-thick sections were cut by microtome. The slides were stained with hematoxylin–eosin.
DSC measurements
The stored samples were washed three times in normal saline and remained in a sterile isotonic saline on 4 °C before starting the calorimetric examinations (max. half an hour). The measurements were made by a SETARAM Micro DSC-II calorimeter between 0 and 100 °C with a heating rate of 0.3 K min−1. Conventional closed Hastelloy batch vessels (V = 1 mL) were used for the experiment to perform the thermal denaturation. Samples’ masses were between in mgs: 180–240 for B1, 43–109 for B2 in case of orthopedic samples and 45–90 for A2, 38–45 for A3 and 116–122 for A4 in case of traumatic patients. The healthy control mass varied in 200–220 mg range. Normal saline was used as a reference. With the help of a two-point setting SETARAM peak integration calorimetric enthalpy was calculated from the area under the heat absorption curve then the other thermal parameters [denaturation or melting temperature (Tm), range of denaturation (ΔT), half width of transition (T1/2) and calorimetry enthalpy (Hcal) data of samples] were compared.
Results
Radiological and histological evaluation
Radiological evaluation of rotator cuff tendon damage and glenohumeral arthritis was performed based on the available conventional X-rays and CT and scans (see Figs. 1, 2). Table 1 shows the results of assessment of orthopedic shoulders, and Table 2 indicates the results of shoulders with 4-part or Neer Type VI (AO/ASIF 11 C3.2–C3.3 [5a]) proximal humerus fractures [17].
Based on Hamada classification, massive rotator cuff tears can be classified into five grades, using radiological analyses of glenohumeral joint. In case of orthopedic samples, grade 4a (glenohumeral arthritis without subacromial acetabulization) and grade 5 (humeral head collapse, which is characteristic of cuff tear arthropathy) cuff tear arthritis were found. Meanwhile, a grade 4b (glenohumeral arthritis with subacromial acetabulization) level of damage was found in trauma sample A3. The MRI-based modified Outerbridge classification also indicated a grade 2 (blister-like swelling/fraying of articular cartilage extending to surface) osteochondral lesion in B1 orthopedic sample.
Overall, based on the intraoperative macroscopical findings, the orthopedic rotator cuff tendon samples exhibited a marked damage, meanwhile, trauma samples showed signs of moderate tendon injuries.
It is important to note, that all of these classifications have been primarily developed for degenerative (RCA) shoulders, therefore, applicability for trauma shoulders is very limited. Healthy samples: in case of healthy, control samples, histological examination confirmed the absence of pathologic findings (Fig. 3).

Histological section from healthy rotator cuff tendon tissue. Hematoxylin–Eosin staining, different magnifications. left: 20× magnification, right: 2× magnification
Thermal denaturation of orthopedic samples
The denaturation process of samples of patients with orthopedic origin can be seen in Fig. 4. The heat flow curves are average of three samples and normalized on the wet sample mass.

The thermal denaturation curves of orthopedic samples (interpretation of symbols is in the text)
The consequence of the advanced tendon damage (B1) as well as specifically advanced tendon damage (B2) compared to the control is well demonstrated by the shape and the running of the curves. This trend is supported by the data of Table 3 too.
The significant decrease of the calorimetric enthalpy well demonstrates the structural consequence of the medical abnormality. The change in the baseline after the denaturation can be a sign of a heat capacity increase, demonstrating a more compact (more densely packed) structure as a consequence of less elasticity of the tendon.
Thermal denaturation of traumatic samples
In this case too, the curves are average of three different samples, and the heat flow is normalized on the wet mass. The moderately degenerated tendons (A2) exhibited significant difference from the control in the shape of the scans and in the thermal parameters too (see Table 4; Fig. 5).

The DSC scans of traumatic samples (interpretation of symbols is in the text)
The reproducibility of DSC measurements in temperature is cc. ±0.2 °C and in enthalpy below 0.05 J (on the basis of different user’s guides and according to our experience). This way we can say that this technique can be a useful tool to monitor the structural changes in tendons caused by orthopedic or traumatic side.
Discussion
The evaluation of the condition of rotator cuff tendons has a great importance in the decision making prior to the surgical treatment of different type of pathologic conditions. Although there are several types of diagnostic tools available to evaluate the rotator cuff injury, there is a need for further insight into the pathophysiology of different rotator cuff tendon conditions [15].
Utilizing differential scanning calorimetry (DSC), here we have demonstrated a marked difference in the thermal parameters of rotator cuff samples with both orthopedic and trauma origin, comparing to the healthy control.
Numerous recent publications have investigated the pathophysiology of rotator cuff injuries. However, only a limited number of studies are available utilizing differential scanning calorimetry (DSC) to assess thermal parameters [18]. In an experimental model of rabbit rotator cuff injury, Szabó et al. have demonstrated definitive differences between the muscles with normal and torn tendons, and those findings were confirmed by CT and MRI scans [19].
Furthermore, it has previously been shown that DSC indicated clear differences, examining the different magnitudes of the rotator cuff tears, examining cadaver biceps tendon samples, which findings were supported with histological examination [20]. They found a loss of thermal cooperation of the components, decreased melting temperatures and with an increase in thermal enthalpy; explaining with the higher level of collagen and secondary bindings among the collagen fibers.
In acute injuries, evaluating ruptured lower limb tendons (patellar, Achilles and quadriceps), Wiegand et al. have demonstrated that the denaturation temperature was significantly increased in the acutely injured samples. They speculated that it could be caused by a smaller amount of bound water in the ruptured tendons. Additionally, they have found that the acutely ruptured samples showed significantly lower enthalpy, compared to the intact tendons; indicating structural changes happened prior to the injury. It is important to note, that the healthy human tendons were of cadaver origin [10].
Ageing, overuse and repetitive microtraumas have all been implicated in the development of rotator cuff tear and the consequential shoulder arthropathies [21]. Bognár et al. have found clear, age-related changes in the thermal denaturation properties of long head of the biceps, using human cadaver tendon samples, the thermal parameters changing from Tm (°C): 57, ΔH (J g−1): 0.26 (age: 0 year) to Tm (°C): 62.92, ΔH (J g−1): 1.28 (age: 90 years) [22]. In their study, the age-related curve of the thermal enthalpies displayed high spreading, with a peak at 51 years (calorimetric enthalpy of 6 J g−1) [22]. It is known that in tendons the Type I. collagen is the major structural element of the extracellular matrix (ECM), and the covalent cross-linking of collagen molecules in connective tissues, like in tendons, plays a major role in the proper function. Importantly, Arnesen et al. has observed an increase in collagen cross-linking and in total amount of collagen during the ageing; leading to a decrease in both its flexibility and its ability to heal following traumas [23].
A potential limitation of our experiments is that radiological classification was performed only in a limited number of cases. However, the routinely used classifications are either developed for the assessment of RCA shoulders or based on MRI examinations. Meanwhile, CT-scan can be generally done prior to surgery, MRI is not always readily available due to the presence older metallic implant, claustrophobia, etc. On the other hand, the lack of available classifications supports the need for novel examination tools, such differential scanning calorimetry.
From the aspect of daily clinical practice, preparation of trauma patients is generally more challenging, since the acute fractures need quicker decision and surgical intervention. Meanwhile, degenerative diseases, such as rotator cuff arthropathies rarely require prompt operations, allowing more time for the surgeon to plan the operation [4,5,6]. Therefore, data showing differences in the expected condition of the rotator cuff of trauma patients vs. orthopedic patients could help the operation planning and improve therapeutic protocols as well.
Another limitation of the study is that only the average values were calculated due to the relatively small number of samples, without further statistical analyses. However, according to the marked differences between the healthy and pathologic samples and the excellent reproducibility of the measurements (in temperature is cc. ± 0.2 °C and in enthalpy below 0.05 J), we believe that DSC is a reliable tool in the evaluation of rotator cuff samples of human origin.
Conclusions
The DSC curves demonstrated a clear difference in the thermal parameters of healthy and pathologic rotator cuff samples of patients underwent reversed shoulder replacements. Therefore, DSC could be a useful additional method in the evaluation of rotator cuff tear arthropathies in future studies.
Availability of data and material
There are no additional available data to upload.
References
Chianca V, Albano D, Messina C, Midiri F, Mauri G, Aliprandi A, et al. Rotator cuff calcific tendinopathy: from diagnosis to treatment. Acta Biomed. 2018;89:186–96.
Neer CS 2nd. The classic: articular replacement for the humeral head. Clin Orthop Relat Res 2011. 1955;469:2409–21.
Flatow EL, Harrison AK. A history of reverse total shoulder arthroplasty. Clin Orthop Relat Res. 2011;469:2432–9.
Maier D, Jäger M, Strohm PC, Südkamp NP. Treatment of proximal humeral fractures—a review of current concepts enlightened by basic principles. Acta Chir Orthop Traumatol Cech. 2012;79:307–16.
Maier D, Jaeger M, Izadpanah K, Strohm PC, Suedkamp NP. Proximal humeral fracture treatment in adults. J Bone Joint Surg Am. 2014;96:251–61.
Jobin CM, Galdi B, Anakwenze OA, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for the management of proximal humerus fractures. J Am Acad Orthop Surg. 2015;23:190–201.
Stone MA, Namdari S. Surgical considerations in the treatment of osteoporotic proximal humerus fractures. Orthop Clin North Am United States. 2019;50:223–31.
Holschen M, Siemes M-K, Witt K-A, Steinbeck J. Five-year outcome after conversion of a hemiarthroplasty when used for the treatment of a proximal humeral fracture to a reverse total shoulder arthroplasty. Bone Joint J. 2018;100-B:761–6.
Mata-Fink A, Meinke M, Jones C, Kim B, Bell J-E. Reverse shoulder arthroplasty for treatment of proximal humeral fractures in older adults: a systematic review. J shoulder Elb Surg United States. 2013;22:1737–48.
Wiegand N, Naumov I, Vámhidy L, Kereskai L, Lőrinczy D, Nöt LG. Comparative calorimetric analysis of 13 different types of human healthy and pathologic collagen tissues. Thermochim Acta. 2013;568:171–4.
Bűcs G, Nőt LG, Dandé Á, Kereskai L, Lőrinczy D. Calorimetric examination of hip pseudo-capsule after secondary hip surgeries. J Therm Anal Calorim. 2019;138:397–400.
Brolin TJ, Updegrove GF, Horneff JG. Classifications in brief: Hamada classification of massive rotator cuff tears. Clin Orthop Relat Res. 2017;475:2819–23.
Hamada K, Yamanaka K, Uchiyama Y, Mikasa T, Mikasa M. A radiographic classification of massive rotator cuff tear arthritis. Clin Orthop Relat Res. 2011;469:2452–60.
Bercik MJ, Kruse K 2nd, Yalizis M, Gauci M-O, Chaoui J, Walch G. A modification to the Walch classification of the glenoid in primary glenohumeral osteoarthritis using three-dimensional imaging. J shoulder Elb Surg United States. 2016;25:1601–6.
Slattery C, Kweon CY. Classifications in brief: outerbridge classification of chondral lesions. Clin Orthop Relat Res. 2018;476:2101–4.
Elser F, Braun S, Dewing CB, Millett PJ. Glenohumeral joint preservation: current options for managing articular cartilage lesions in young, active patients. Arthrosc J Arthrosc Relat Surg Off Publ Arthrosc Assoc North Am Int Arthrosc Assoc. 2010;26:685–96.
Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and dislocation classification compendium-2018. J Orthop Trauma. 2018;32(Suppl 1):S1-170.
Csotye J, Aigner Z, Sohár G, Szabó-Révész P, Tóth K. Calorimetric properties of degenerative human shoulder joint hyaline cartilage. J Therm Anal Calorim. 2009;95:805–8.
Szabó I, Bognár G, Magda I, Garamvölgyi R, Czobel G, Nőth L, et al. DSC examination of the rotator cuff muscles in rabbits. Thermochim Acta. 2006;445:179–84.
Szabó I, Bognár G, Kereskai L, Szász K, Lőrinczy D. Differentialscanning calorimetric and histological examinations of the long head of thebiceps in cadavers. J Therm Anal Calorim. 2007;88:343–9.
Trębacz H, Szczęsna A, Arczewska M. Thermal stability of collagen in naturally ageing and in vitro glycated rabbit tissues. J Therm Anal Calorim. 2018;134:1903–11.
Bognár G, Szabó I, Pintér C, Ligeti E, Lőrinczy D. Changes in thermal denaturation properties of the long head of the biceps during lifetime. J Therm Anal Calorim. 2010;102:65–8.
Arnesen SM, Lawson MA. Age-related changes in focal adhesions lead to altered cell behavior in tendon fibroblasts. Mech Ageing Dev Ireland. 2006;127:726–32.
Acknowledgements
This work was supported by CO-272 (OTKA) grant (D.L.).
Funding
Open access funding provided by University of Pécs..
Author information
Authors and Affiliations
Contributions
Dr. László G Nöt: operations, sample collection and handling, data analysis, manuscript writing. Dr. András Bata: sample collection and handling, data analysis. Dr. János Cifra: histological examination. Dr. Hajnalka Szabó: radiological evaluation. Prof. Dr. Dénes Lőrinczy: corresponding author, principle investigator, DSC experiments, data analysis, manuscript writing.
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Consent for publication
Copyright form has been uploaded with the manuscript.
Ethics approval and consent to participate
All procedures followed were approved and in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the revised Declaration of HELSINKI 1975. Consent from patients to participate in the study has been obtained.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nöt, L.G., Bata, A., Szabó, H. et al. DSC examination of rotator cuff damage in patients with total shoulder arthroplasty. J Therm Anal Calorim 146, 165–170 (2021). https://doi.org/10.1007/s10973-020-10402-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10973-020-10402-w