
Abstract
There is little understanding of physical activity (PA) and sedentary behavior as preventive health behaviors in autistic adults. Technology has been used as an educational and social intervention tool for autistic individuals, yet it is also associated with low PA and high sedentary time (ST) in the neurotypical population. This study aimed to examine the prevalence of self-reported PA and ST and their relationships with various technology uses in autistic adults. We employed a Qualtrics online survey that consisted of the International Physical Activity Questionnaire-Short Form, Sedentary Behavior Questionnaire, and National Alliance for Mental Illness’s digital technology use survey. 229 responses (74.6% under 35 years of age; 64.1% males) satisfied the response validity criteria and were included in the analyses. The majority of participants (78%) met the recommended PA amount of ≥ 600 metabolic equivalent of task (MET)-minutes/week (median, 1,812 total MET-minutes/week), but they were also overly sedentary on both weekdays (median, 8 h/day) and weekends (median, 7 h/day). Stepwise multiple regression analyses revealed that variance of ST in weekday (45%) and weekend (43%) was largely explained by quality of life (β = -0.31; β = -0.33) and technology use time (β = 0.31; β = 0.26) (all p < .01). While technology can be an effective tool to support social and academic abilities in autistic adults, the use of technology devices needs to be monitored with care as it may put these individuals at risk for sedentary lifestyles and associated chronic diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Physical activity (PA) is any bodily movement that requires substantial energy expenditure (Caspersen et al., 1985), while sedentary behavior is defined as any waking behaviors, such as sitting, lying, or reclining, that result in energy expenditure of ≤ 1.5 metabolic equivalent of task (MET) (Tremblay et al., 2017). Despite the well-documented benefits of regular PA participation and active lifestyles across the lifespan, the understanding of PA and sedentary behavior levels in autistic individuals is largely based on research in autistic children and adolescents (Jones et al., 2017; Pan & Frey, 2006; Stanish et al., 2017). To date, there exist a limited number of studies that addressed both PA and sedentary behaviors in autistic adults, and these data must be interpreted with caution as most relied on caregiver proxy reports with small sample sizes, which is subject to a selection bias and underrepresentation of the diverse autism subgroups (Eaves & Ho, 2008; Lalonde et al., 2014; Shahane et al., 2024). Current evidence indicates that autistic adolescents and adults may lead insufficiently active or overly sedentary lifestyles. This population segment does not meet the established health-related PA guidelines, which recommend a minimum of 150 min of moderate-intensity PA or 75 min of vigorous-intensity PA per week, and for whom PA levels decline progressively with age (Liang et al., 2023; MacDonald et al., 2011). Furthermore, an early empirical study revealed that autistic adults often exhibit prolonged sedentary behavior, spending an average of 13 h per day sitting (Eaves & Ho, 2008).
The literature consistently reports the negative impact of insufficient PA on both physical and mental health, including an increased risk of noncommunicable diseases and depression (Lee et al., 2012; Poirel, 2017), along with the increasing health disparities experienced by people with disabilities including those with autism (Croen et al., 2015; Krahn et al., 2015). Insufficient PA is a leading preventable cause of death worldwide (Lee et al., 2012), but the consequences of physical inactivity in autistic adults remains largely unexplored. Although the benefits of PA in autistic youth, such as improved gross motor function, aerobic capacity, self-satisfaction, and social skills, have been reported with moderate-to-strong evidence (Lang et al., 2010; Sowa & Meulenbroek, 2012), PA benefits and outcomes in autistic adults have received little attention in the literature.
An expanding body of evidence shows that sedentary behavior should be considered an independent health risk factor for all-cause mortality and chronic diseases, such as diabetes and cardiovascular diseases (Thorp et al., 2011; Wilmot et al., 2012). At present, there is a knowledge gap regarding the levels and patterns of sedentary behaviors in autistic adults, with few studies indicating that autistic youth either spend more time in sedentary behavior than non-autistic peers (Chonchaiya et al., 2011; Must et al., 2014) or there are no differences in the levels of sedentary behavior between these two groups (McCoy et al., 2016). Emerging research suggests that autistic individuals experience high rates of lifestyle-related chronic health conditions, such as obesity, hypertension, hyperlipidemia, and type 2 diabetes (Croen et al., 2015; Matheson & Douglas, 2017; Tyler et al., 2011). These findings imply that poor physical behaviors may further exacerbate the already poor overall well-being among these individuals (Howlin & Magiati, 2017). The autistic adult population continues to grow with the advancement of diagnostic system for adults, and the existing large gap in preventive health research and resources for this population will likely expand (Croen et al., 2015; Krahn et al., 2015; Nightingale, 2012; Tyler et al., 2011). It is critical to address preventive health disparities in these individuals because their levels of PA and sedentary behavior can directly affect many other life domains, including self-care, social participation, work productivity, vitality, and emotional well-being (Lee et al., 2012; Marquez et al., 2020).
Over the past two decades, there has been a substantial and rapid increase in the use of technology, and excessive technology use is often associated with low PA and high sedentary time (ST) in neurotypical populations (Clark & Sugiyama, 2015; Hallal et al., 2012). Technology use may also be a significant but complex predictor of PA and ST in autistic adults since it is promoted as an effective educational, social, and therapeutic tool for these individuals (Ayres et al., 2013; Kientz et al., 2014). While dependence on mobile technology for social media use and digital gaming can contribute to prolonged sedentary behaviors (Lepp et al., 2013), successful technology-based interventions (e.g., wearable PA monitors, mobile health apps) can lead to positive physical behavior changes (Woessner et al., 2021). Further, many autistic people are naturally attracted to technology use because human-technology interaction creates a consistent and predictable social and learning environment, as well as the lower social burden, compared to the traditional face-to-face interaction (Goodwin, 2008; Rajendran & Mitchell, 2007). Nevertheless, limited effort has been made to investigate the prevalence of everyday technology use and its impact on PA and ST in autistic adults.
An earlier study reported that autistic adults use their mobile technology devices more than 4 hours per day, primarily for surfing the Internet, using social media, and playing games during both week and weekend days (Lee et al., 2018). This level of technology immersion could contribute to adverse social and physical outcomes in autistic adults, including a passive sedentary lifestyle, similar to findings reported in diverse neurotypical populations (Elhai et al., 2017; Hawi & Samaha, 2017). Excessive screen time, increasingly influenced by mobile technology use, has been linked to negative health behaviors such as reduced PA engagement and prolonged sitting in the neurotypical population (Fennell et al., 2019). Given the predilection for technology and online social interactions, autistic adults may be at a similar risk of an inactive and sedentary lifestyle due to the increased technology use. Therefore, the purpose of this study was to examine the prevalence of self-reported PA and ST and their relationships with everyday technology use in autistic adults. It is hypothesized that extensive technology use is associated with a low level of PA and a high level of ST in autistic adults.
Methods
The data collected and analyzed in the present study were part of a large survey that aimed to examine the following: (1) the levels of PA and ST and characteristics of technology use, (2) factors associated with PA and ST, particularly technology use, and (3) correlates of PA, ST, and physiological and mental health risk factors for cardiovascular disease in autistic adults who were able to provide informed consent and complete a self-administered survey independently.
Instrument Development
A Qualtrics online survey was developed to assess the outcome variables in the target population. Survey questions focused on the following topics: (a) demographic backgrounds (e.g., age, biological sex, ethnicity, autism traits, education level, annual household income, employment status, and Body Mass Index (BMI)); (b) level of autism traits (Autism Spectrum Quotient 10 (AQ 10)) (Baron-Cohen et al., 2001); (c) level of PA engagement using a modified International Physical Activity Questionnaire-Short Form (IPAQ-SF) (Craig et al., 2003); (d) level of ST using a modified Sedentary Behavior Questionnaire (Rosenberg et al., 2010); (e) National Alliance for Mental Illness’s digital technology use survey (Gay et al., 2016); and (f) quality of life (WHOQOL Group, 1998). The IPAQ-SF measures health-related PA and ST over the past seven days. The instrument evaluates varying types of PAs based on intensity level (e.g., walking, moderate, and vigorous) and estimates total PA in MET-minutes per week and total sitting time. The Sedentary Behavior Questionnaire measures time spent in domain-specific sedentary behaviors on an average weekday or weekend in nine different contexts (e.g., playing games, watching television, talking on the phone, doing office work, sitting while listening to music, reading, driving/riding in a car, bus, or train etc.). While there exists a significant correlation between Sedentary Behavior Questionnaire items and IPAQ sitting time (Rosenberg et al., 2010), the total sitting time estimated by the Sedentary Behavior Questionnaire was used to represent the sedentary behaviors in our sample. Time spent using technology devices (e.g., desktop computer, laptop, smartphone, tablet, and wearables) for purposes, such as surfing the Internet, entertainment, or work, were adapted from the National Alliance for Mental Illness’s digital technology use survey (Gay et al., 2016; Shpigelman et al., 2021). A question “How would you rate your quality of life?” was used to measure participants’ overall quality of life based on a 5-point Likert scale (i.e., very poor, poor, neither good or poor, good, and very good). The survey was visually modified to enhance the clarity of questions, specifically by emphasizing illustrative depictions of sample activities.
Content validity was assessed by five experts in the fields of both autism research and survey methodology, including one parent/advocate. The survey was revised in response to the feedback and suggestions provided. Further revisions for appropriate wording, formatting, and other mechanics of survey development were executed under the guidance of two survey research experts. These revisions included adding visual aids and more specific example activities to the IPAQ-SF activity intensity questions as well as the Sedentary Behavior Questionnaire to facilitate respondents’ comprehension. Customized logic metrics were inserted, and multiple-choice time scales with question headers were used to reduce response time and ensure clearer matching between each question and its respective answer choices. Additionally, we adhered to standardized recommendations for PA surveys to minimize measurement errors and improve the accuracy of estimates in self-reported PA (Ainsworth et al., 2012).
The initial version of the online survey was pretested with six autistic adults as key stakeholders to assess the survey administration process, readability, design format, flow of questions, and response time. Participatory interviews were sequentially conducted with each stakeholder, either in person or over the telephone, to gather additional information regarding the appropriateness and clarity of the questions. The survey was further revised based on this feedback, and the stakeholders completed the revised survey a second time. A total of 85 questions were finalized including follow-up questions, depending on responses. The estimated survey completion time was minimum 15–20 min. The final version of the online survey was accessible via technology devices, such as smartphones, tablets, and desktop/ laptop computers.
Procedure
Study participants were recruited via autism support groups in social networking services, such as Facebook and Reddit online community websites that promote autism awareness as well as direct contact with autism advocacy organizations in the U.S. Inclusion criteria were the following: (1) age between 18 and 55 years; (2) diagnosis of an autism spectrum conditionFootnote 1 by a qualified medical professional; (3) physical ability to walk without an assistive device (e.g., wheelchair and crutches); and (4) cognitive ability to understand the purpose of the study and complete the survey independently. The invitation messages along with a survey link and criteria for valid survey completion were posted in group pages of the social media and research resources of the autism organizations. The survey participants were navigated to the first page of the survey through the provided link in which the purpose of the study and eligibility criteria were described. Only those who provided e-consent were invited to the full survey. All participants who met the survey validity criteria and successfully completed the entire questionnaire received a $10 online gift card as a token of appreciation. This study was approved by the Institutional Review Board of Indiana University.
Data Cleaning
Survey responses
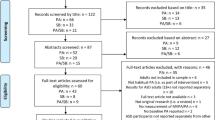
Although the online survey methodology presents increased efficiency in recruiting potential participants and minimizing discomfort of respondents compared to the traditional paper-based survey, reliability may be a major concern when using self-report methodology. This may become substantial when conducting a self-report survey with autistic individuals who often have co-occurring learning disabilities that may impede appropriate judgement and estimation for the questions requiring numeric calculations (O’Brien & Pearson, 2004). Accordingly, the response validation process was established along with time measurement blocks to identify and exclude ineligible or unreliable responses following the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) (Eysenbach, 2004). These criteria consisted of minimum duration of survey completion, total AQ 10 score, and additional questions to verify the autism traits, such as school-based services and a history of therapy for autism symptoms. Further, duplicated entries were identified and eliminated by utilizing Internet Protocol (IP) address and geographic location tracking features in the Qualtrics system. Among 802 initially recorded responses, 229 met the response validity criteria and were included in the analyses. See the flow diagram of the response validation process (Fig. 1).

Flow diagram of the response validation process
Survey data
The calculated AQ 10 score was categorized in two different levels of autism traits (low 0–5; high 6–10). The MET values for PA participation were calculated according to the IPAQ guidelines (vigorous PA (VPA) = 8.0 METs * the time reported; moderate PA (MPA) = 4.0 METs * the time reported; and walking = 3.3 METs * the time reported) (Craig et al., 2003). METs are used to estimate the intensity of PA and corresponding energy expenditure. One MET is the energy expenditure at rest or while sitting quietly. Typically, high MET values imply high-intensity PAs that result in high energy expenditure (Ainsworth et al., 2011). PA data cleaning was also sequentially performed as follows: (1) cases were excluded from the analyses if the sum of all walking, MPA and VPA times was greater than 960 min/day (16 h/day) and (2) any of the walking, MPA and VPA time variables exceeding 180 min/day were truncated to be equal to 180 min/day (Craig et al., 2003). Additional data exclusion criteria were added based on the national PA guidelines for Americans in which physically active adults may achieve 75 min of VPA per week (Piercy et al., 2018) and the recommended amount of energy expenditure is 500–1000 MET-minutes/week for adults (Ross et al., 2016). As such, given that highly active athletes may achieve > 2000 MET-minutes/week, we excluded cases of which the sum of all walking, MPA, and VPA was higher than 6000 MET-minutes/week. Participants were further classified into three categories based on total PA time: ‘physically inactive’ not meeting the minimum recommended amount of PA, ‘minimally active’ meeting the recommended amount of PA, and ‘sufficiently active’ exceeding the level of health-enhancing PA (Craig et al., 2003). Further, ST outliers were defined and excluded from the analyses as follows: (1) cases with total ST higher than 17 h/day, considering the average sleep time as 7 h/day and (2) cases with ST less than 1 h/day. Finally, we excluded 62 cases from PA and 14 cases from ST dataset, accounting for multivariate outliers based on Mahalanobis distance criterion.
Data Analysis
Descriptive analyses were performed to summarize information on demographics, PA, ST, and technology use. BMI was calculated from self-reported weight and height information (e.g., underweight < 18.5, normal weight 18.5–24.9, overweight 25.0–29.9, obese classes 1 and 2 30.0–39.9, and extremely obese ≥ 40) and was used for the classification of overweight and obesity (National Heart and Blood Institute, 1998). The assumption of normality was violated in PA and ST data and thus, the median and interquartile range (IQR) were used. Related-Samples Wilcoxon Signed Rank Tests were performed to compare the differences between PA intensities in MET-minutes/week (i.e., VPA, MPA, and walking), as well as weekday and weekend day ST (total minutes/day). Spearman’s rank and Pearson’s correlations were used to assess relationships between categorical and continuous variables (e.g., demographics with ST and PA) and two continuous variables (e.g., technology usage time with PA and ST), respectively. Following ranges of correlation coefficients were used to interpret the strength of association between variables; < 0.3 small, 0.3–0.49 moderate, and ≥ 0.5 large (Cohen, 1988).
Stepwise multiple regression models were generated to explain the variation in PA and ST with major demographic characteristics, time spent for technology use, and quality of life as predictor variables. Cases with multiple ‘prefer not to answer’ responses for demographic questions were not included in the regression analyses. All analyses were performed using IBM Statistical Package for the Social Sciences (SPSS) for Windows version 26 and the significance level was set at p < 0.05.
Results
The demographic characteristics of the study participants are shown in Table 1. 74.6% of the participants were under 35 years of age and 64.1% were males. Sex differences were analyzed for all demographic variables, but there were no statistically significant results. Self-reported estimates of PA in MET-minutes/week for VPA, MPA, and walking, as well as ST are described in Table 2. Participant were classified as physically inactive (22.3%), minimally active (62.9%), and sufficiently active (14.8%) according to the aforementioned IPAQ guidelines for data processing and analysis. The Wilcoxon-signed rank test revealed a significant difference between weekday and weekend median ST (480 vs. 420 min/day; p = 0.026) and thus, these time periods were entered separately into the regression equations. Respondents spent over 90% of their technology usage time for surfing the internet, social networking, and entertainment. Specifically, autistic participants used diverse technology devices for texting, talking on the phone, engaging in online gaming, sending emails, listening to music or podcasts, and participating in chat groups. Technology use time was higher on weekends (median, 413 min/day) compared to weekdays (median, 373 min/day; p = 0.001), particularly using smartphones (123 vs. 82 min/day; p < 0.001) and tablets (61 vs. 44 min/day; p = 0.001), while desktop computers were used more on weekdays than weekends (135 vs. 111 min/day; p = 0.001) (Fig. 2).

Characteristics of technology device use (n = 229)
Annual household income (rs = 0.20, p = 0.01), level of education (rs = 0.17, p = 0.035), employment status (rs = 0.24, p = 0.002), and BMI (rs = -0.17, p = 0.028) were weakly correlated with total PA. There was no significant correlation between technology use time and PA (r = -0.08, p > 0.05). There were moderate-to-small positive correlations between technology use time in weekday and weekend day STs (Table 3). Level of education (r = 0.19, p = 0.005) and employment (r = 0.17, p = 0.016) were weakly correlated with ST on weekdays only. Quality of life was moderately correlated with ST on both weekdays (r = -0.32, p < 0.001) and weekends (r = -0.32, p < 0.001). The weak correlation between BMI and ST failed to reach statistical significance on both weekdays (r = -0.13, p = 0.055) and weekends (r = -0.14, p = 0.051).
No multicollinearity was observed in the stepwise multiple regression models. Age, sex, education level, and BMI were automatically excluded from the models due to low significance. Autism traits, employment, time spent for technology use in weekend day, and annual household income were significant predictors of total PA level (MET-minutes/week). Overall, the predictor variables in the regression model explained 21% of the variance in total PA. The regression model for ST revealed that quality of life and technology time were the strongest predictors of ST on both weekdays and weekends (Table 4). The predictor variables in the ST regression models explained 45% and 43% of the variance in ST on weekdays and weekends, respectively (Table 4).
Discussion
The present study aimed to assess the levels of and associations between PA, ST, and technology use in autistic adults. The majority of study participants (78%) met the recommended level of PA (e.g., ≥ 600 MET-minutes/week) necessary for substantial health benefits. This finding contrasts with previous reports that suggest both autistic youth and adults typically do not meet PA guidelines (Eaves & Ho, 2008; Jones et al., 2017; Pan & Frey, 2006). According to the current findings, autistic adults may engage in sufficient amounts of moderate-to-vigorous PA as recommended by the national health organizations that can help reduce the risk for mortality and major cardiovascular disease incidence associated with physical inactivity (Lee et al., 2012). However, autistic adults were also highly sedentary, reporting 8 hours of ST per day on weekdays and 7 hours per day on weekends (median values). This is lower than the 13 hours of ST proxy-reported by caregivers for autistic adults with co-occurring intellectual disabilities (Eaves & Ho, 2008), yet higher than the 5 hours of self-reported ST in neurotypical adults from 20 different countries (Bauman et al., 2011). A growing body of evidence suggests that sedentary behavior should be viewed as an independent risk factor (Dunstan et al., 2012). Regardless of their level of PA, individuals who lead sedentary lifestyles may face elevated risks of developing adverse health outcomes, including all-cause mortality, cardiovascular diseases (e.g., myocardial infarction, angina, heart failure, stroke), and obesity (Wilmot et al., 2012). Furthermore, those exhibiting both low PA and high sedentary behavior levels are particularly susceptible to increased disease incidence, mortality, and hospitalization (Biswas et al., 2015; Dunstan et al., 2012). Excessive sedentary behaviors may contribute to the concerning rates of noncommunicable diseases, such as diabetes, obesity, and mental health disorders, increasingly observed in autistic adults (Croen et al., 2015).
Autistic adults in this study may be considered ‘active couch potatoes’, a label for the phenomenon of adequate PA occurring alongside undesirable levels of sedentary behaviors (Dunstan et al., 2012). Recent research indicates that smartphone use predicts the active couch potato dichotomy in sufficiently active neurotypical adults (Fennell et al., 2021). In the current sample, total technology use time predicted ST on both weekdays and weekends, which aligns with the previous findings in neurotypical adults (Woessner et al., 2021). Autistic adults were found to primarily use desktop computers on weekdays, which typically involves prolonged sitting and corresponds with the higher reported ST during this period. On weekends, however, smartphones were more frequently used. Since smartphones allow for movement while in use, this likely explains the relatively lower level of ST observed on weekends. While television viewing has traditionally been seen as a major contributor to a sedentary and physically inactive lifestyle, smartphone use now has mixed impact on physical behaviors. Smartphones allow people to engage in PA through mobile health apps and online exercise programs, but they can also lead to prolonged bouts of sitting due to excessive use of social media, video streaming, and gaming. (Fennell et al., 2021). Our results may be partly in line with previous research on neurotypical college students in which the increased availability of mobile platforms played a positive role in promoting PA and reducing ST in this population. Towne and colleagues (2017) found that a high level of technology use, primarily smartphones, was associated with meeting the PA recommendations in neurotypical college students, and this was attributed to increasing accessibility and affordability of mobile-friendly exercise programs that changed the common paradigm of the association between technology use, PA and ST. People can use technology devices while on the move and no longer need to remain seated while using devices (Towne et al., 2017). Future research should take into account the physical position and movement, such as sitting, standing, and walking, during technology use when investigating the effects of this complex variable on PA and ST.
Several demographic variables, including employment status and annual household income, showed moderate correlations with PA, and this is similar to findings in neurotypical populations (Kao et al., 2014; O’donoghue et al., 2016). Nonetheless, large inconsistencies in PA correlates across different groups and considerable variability in reports complicate efforts to ascertain the reliability of these associations (Rhodes et al., 2017). Based on our findings, autism traits and employment status were stronger predictors of PA compared to technology use time. These factors accounted for a small, albeit significant portion of the variance in PA behavior with approximately 80% left unexplained. Therefore, it is premature to determine the significance of this finding, and further research is needed to elucidate the multidimensional factors that influence PA behaviors in autistic adults.
The variance in ST was better explained by primary outcome variables compared to PA. On weekdays, 45% of the variance in ST was explained by quality of life and weekday technology use time. On weekends, 43% of the variance in ST was explained by quality of life, weekend technology use time, and annual household income. Technology use is increasingly associated with the level of sedentary behaviors in neurotypical adults (Fennell et al., 2021), and this association was also observed in autistic adults. Poor quality of life is generally associated with high levels of sedentary behavior (Saunders et al., 2020), but this relationship largely depends on specific and contextual domains of sedentary behavior, such as screen-viewing or reading time (Omorou et al., 2016). Research is consistent that autistic adults report a much poorer quality of life compared to non-autistic individuals (Van Heijst & Geurts, 2015), but predictors of this association include factors that are difficult to modify, such as employment and relationship status, autism traits, and co-occurring mental health conditions (Mason et al., 2018). Nevertheless, since sedentary behavior is a modifiable risk factor, addressing technology-induced ST could play a crucial role in improving health-related quality of life in autistic adults. Focusing on domain-specific and targeted behavior changes, such as reducing recreational and gaming technology use and promoting movement-oriented technology use, can be effective strategies to mitigate sedentarism and help prevent these individuals from developing lifestyle-related chronic diseases.
Self-report surveys represent the most efficient approach for assessing PA and ST within large populations. Yet, it is widely recognized that respondents, including autistic adults, tend to overestimate PA and underestimate sedentary behavior via self-report surveys (Hagstromer et al., 2010; Lee et al., 2024). In addition, even though we employed a rigorous response validation criteria to avoid the inclusion of unreliable and duplicated responses in the analyses, the inherent risk of estimation errors and relatively low reliability associated with self-reports cannot be eliminated. This issue may be further complicated by the challenges autistic adults often face in processing textual information (Haigh et al., 2018), which can interfere with the ability to comprehend and answer retrospective questions (O’Brien & Pearson, 2004). Consequently, the high levels of PA reported by our autistic participants in this study must be interpreted with caution. Another limitation lies in the target sample of the study. This study only targeted autistic adults without co-occurring intellectual disabilities who could provide informed consent and complete the survey independently, and thus, these findings cannot be generalized to autistic individuals who did not meet our eligibility criteria. Despite these limitations, this study provides novel insights into the prevalence of PA, ST, and technology use, as well as the factors influencing these behaviors, in a large sample of autistic adults, based on self-reports rather than proxy reports. Further investigation is warranted to deepen our understanding of preventive health behaviors and their associations with preferred everyday activities in this underrepresented population segment. Given the lifelong nature of autism as a neurodevelopmental condition and the growing population of autistic adults (Dietz et al., 2020), there is a critical need to amplify research efforts directed toward improving the health outcomes of these individuals.
Conclusion
Our findings indicate that although autistic adults may reach the recommended weekly levels of PA, they also spend a considerable amount of time in sedentary behaviors. ST was significantly associated with perceived quality of life and technology use time on both weekdays and weekends. While technology can be a powerful tool to support social and academic abilities in this population, technology use may also predispose autistic adults to chronic health conditions associated with excessive, uninterrupted sitting. Further research is needed to examine the context-specific associations of PA and sedentary behaviors with unique technology preferences in this population segment.
Notes
The term autism spectrum is used to refer to autism as a diagnostic condition in line with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (American Psychiatric Association, 2013).
References
Ainsworth, B. E., Caspersen, C. J., Matthews, C. E., Mâsse, L. C., Baranowski, T., & Zhu, W. (2012). Recommendations to improve the accuracy of estimates of physical activity derived from self report. Journal of Physical Activity and Health, 9(s1), S76–S84.
Ainsworth, B. E., Haskell, W. L., Herrmann, S. D., Meckes, N., Bassett, D. R., Jr., Tudor-Locke, C., & Leon, A. S. (2011). 2011 Compendium of Physical Activities: A second update of codes and MET values. Medicine & Science in Sports & Exercise, 43(8), 1575–1581.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5 (5th ed.). American psychiatric association.
Ayres, K. M., Mechling, L., & Sansosti, F. J. (2013). The use of mobile technologies to assist with life skills/independence of students with moderate/severe intellectual disability and/or autism spectrum disorders: Considerations for the future of school psychology. Psychology in the Schools, 50(3), 259–271.
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., & Clubley, E. (2001). The autism-spectrum quotient (AQ): Evidence from asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders, 31(1), 5–17. https://doi.org/10.1023/A:1005653411471
Bauman, A., Ainsworth, B. E., Sallis, J. F., Hagströmer, M., Craig, C. L., Bull, F. C., … & IPS Group. (2011). The descriptive epidemiology of sitting: A 20-country comparison using the International Physical Activity Questionnaire (IPAQ). American Journal of Preventive Medicine, 41(2), 228–235.
Biswas, A., Oh, P. I., Faulkner, G. E., Bajaj, R. R., Silver, M. A., Mitchell, M. S., & Alter, D. A. (2015). Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Annals of Internal Medicine, 162(2), 123–132.
Caspersen, C. J., Powell, K. E., & Christenson, G. M. (1985). Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Reports, 100(2), 126.
Chonchaiya, W., Nuntnarumit, P., & Pruksananonda, C. (2011). Comparison of television viewing between children with autism spectrum disorder and controls. Acta Paediatrica, 100(7), 1033–1037.
Clark, B., Sugiyama, T. (2015). Prevalence, trends, and correlates of sedentary behavior. In: Kanosue, K., Oshima, S., Cao, ZB., Oka, K. (eds) Physical Activity, Exercise, Sedentary Behavior and Health. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55333-5_8
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences (2nd ed.). Routledge. https://doi.org/10.4324/9780203771587
Craig, C. L., Marshall, A. L., Sjostrom, M., Bauman, A. E., Booth, M. L., Ainsworth, B. E., Pratt, M., Ekelund, U., Yngve, A., Sallis, J. F., & Oja, P. (2003). International physical activity questionnaire: 12-country reliability and validity. Medicine and Science in Sports and Exercise, 35(8), 1381–1395. https://doi.org/10.1249/01.mss.0000078924.61453.fb
Croen, L. A., Zerbo, O., Qian, Y., Massolo, M. L., Rich, S., Sidney, S., & Kripke, C. (2015). The health status of adults on the autism spectrum. Autism, 19(7), 814–823. https://doi.org/10.1177/1362361315577517
Dietz, P. M., Rose, C. E., McArthur, D., & Maenner, M. (2020). National and state estimates of adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(12), 4258–4266.
Dunstan, D. W., Howard, B., Healy, G. N., & Owen, N. (2012). Too much sitting–a health hazard. Diabetes Research and Clinical Practice, 97(3), 368–376.
Eaves, L. C., & Ho, H. H. (2008). Young adult outcome of autism spectrum disorders. Journal of Autism and Developmental Disorders, 38(4), 739–747. https://doi.org/10.1007/s10803-007-0441-x
Elhai, J. D., Dvorak, R. D., Levine, J. C., & Hall, B. J. (2017). Problematic smartphone use: A conceptual overview and systematic review of relations with anxiety and depression psychopathology. Journal of Affective Disorders, 207, 251–259.
Eysenbach, G. (2004). Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). In Journal of medical Internet research (Vol. 6, Issue 3, p. e34). Gunther Eysenbach Centre for Global eHealth Innovation, Toronto, Canada.
Fennell, C., Barkley, J. E., & Lepp, A. (2019). The relationship between cell phone use, physical activity, and sedentary behavior in adults aged 18–80. Computers in Human Behavior, 90, 53–59.
Fennell, C., Lepp, A., & Barkley, J. (2021). Smartphone use predicts being an “active couch potato” in sufficiently active adults. American Journal of Lifestyle Medicine, 15(6), 673–681.
Gay, K., Torous, J., Joseph, A., Pandya, A., & Duckworth, K. (2016). Digital Technology Use Among Individuals with Schizophrenia: Results of an Online Survey. JMIR Mental Health, 3(2), e15. https://doi.org/10.2196/mental.5379
Goodwin, M. S. (2008). Enhancing and accelerating the pace of autism research and treatment: The promise of developing innovative technology. Focus on Autism and Other Developmental Disabilities, 23(2), 125–128.
Hagstromer, M., Ainsworth, B. E., Oja, P., & Sjostrom, M. (2010). Comparison of a subjective and an objective measure of physical activity in a population sample. Journal of Physical Activity and Health, 7(4), 541–550.
Haigh, S. M., Walsh, J. A., Mazefsky, C. A., Minshew, N. J., & Eack, S. M. (2018). Processing speed is impaired in adults with autism spectrum disorder, and relates to social communication abilities. Journal of Autism and Developmental Disorders, 48, 2653–2662.
Hallal, P. C., Andersen, L. B., Bull, F. C., Guthold, R., Haskell, W., & Ekelund, U. (2012). Global physical activity levels: Surveillance progress, pitfalls, and prospects. The Lancet, 380(9838), 247–257.
Hawi, H., & N. S., & Samaha, M. (2017). The relations among social media addiction, self-esteem, and life satisfaction in university students. Social Science Computer Review, 35(5), 576–586.
Howlin, P., & Magiati, I. (2017). Autism spectrum disorder: Outcomes in adulthood. Current Opinion in Psychiatry, 30(2), 69–76.
Jones, R. A., Downing, K., Rinehart, N. J., Barnett, L. M., May, T., McGillivray, J. A., & Hinkley, T. (2017). Physical activity, sedentary behavior and their correlates in children with autism spectrum disorder: A systematic review. PloS one, 12(2), e0172482.
Kao, M.-C.J., Jarosz, R., Goldin, M., Patel, A., & Smuck, M. (2014). Determinants of physical activity in America: A first characterization of physical activity profile using the National Health and Nutrition Examination Survey (NHANES). PM&R, 6(10), 882–892.
Kientz, J. A., Goodwin, M. S., Hayes, G. R., & Abowd, G. D. (2014). Interactive technologies for autism.
Krahn, G. L., Walker, D. K., & Correa-De-Araujo, R. (2015). Persons with disabilities as an unrecognized health disparity population. American Journal of Public Health, 105(S2), S198–S206.
LaLonde, K. B., MacNeill, B. R., Eversole, L. W., Ragotzy, S. P., & Poling, A. (2014). Increasing physical activity in young adults with autism spectrum disorders. Research in Autism Spectrum Disorders, 8(12), 1679–1684.
Lang, R., Koegel, L. K., Ashbaugh, K., Regester, A., Ence, W., & Smith, W. (2010). Physical exercise and individuals with autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorders, 4(4), 565–576.
Lee, D., Frey, G., Cheng, A., & Shih, P. C. (2018). Puzzle walk: A gamified mobile app to increase physical activity in adults with autism spectrum disorder. In 2018 10th International Conference on Virtual Worlds and Games for Serious Applications (VS-Games) (pp. 1–4). IEEE.
Lee, D., Frey, G. C., Cothran, D. J., Harezlak, J., & Shih, P. C. (2024). Concordance between accelerometer-measured and self-reported physical activity and sedentary time in adults with autism. Journal of Autism and Developmental Disorders, 54(4), 1517–1526.
Lee, I. M., Shiroma, E. J., Lobelo, F., Puska, P., Blair, S. N., & Katzmarzyk, P. T. (2012). Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. The Lancet, 380(9838), 219–229.
Lepp, A., Barkley, J. E., Sanders, G. J., Rebold, M., & Gates, P. (2013). The relationship between cell phone use, physical and sedentary activity, and cardiorespiratory fitness in a sample of US college students. International Journal of Behavioral Nutrition and Physical Activity, 10, 1–9.
Liang, X., Haegele, J. A., Healy, S., Tse, A. C. Y., Qiu, H., Zhao, S., & Li, C. (2023). Age-related differences in accelerometer-assessed physical activity and sleep parameters among children and adolescents with and without autism spectrum disorder: A meta-analysis. JAMA Network Open, 6(10), e2336129–e2336129.
MacDonald, M., Esposito, P., & Ulrich, D. (2011). The physical activity patterns of children with autism. BMC Research Notes, 4, 1–5.
Marquez, D. X., Aguiñaga, S., Vásquez, P. M., Conroy, D. E., Erickson, K. I., Hillman, C., & Powell, K. E. (2020). A systematic review of physical activity and quality of life and well-being. Translational Behavioral Medicine, 10(5), 1098–1109.
Mason, D., McConachie, H., Garland, D., Petrou, A., Rodgers, J., & Parr, J. R. (2018). Predictors of quality of life for autistic adults. Autism Research, 11(8), 1138–1147.
Matheson, B. E., & Douglas, J. M. (2017). Overweight and obesity in children with autism spectrum disorder (ASD): A critical review investigating the etiology, development, and maintenance of this relationship. Review Journal of Autism and Developmental Disorders, 4(2), 142–156.
McCoy, S. M., Jakicic, J. M., & Gibbs, B. B. (2016). Comparison of obesity, physical activity, and sedentary behaviors between adolescents with autism spectrum disorders and without. Journal of Autism and Developmental Disorders, 46(7), 2317–2326. https://doi.org/10.1007/s10803-016-2762-0
Must, A., Phillips, S. M., Curtin, C., Anderson, S. E., Maslin, M., Lividini, K., & Bandini, L. G. (2014). Comparison of sedentary behaviors between children with autism spectrum disorders and typically developing children. Autism, 18(4), 376–384. https://doi.org/10.1177/1362361313479039
National Heart, Lung, Blood Institute, National Institute of Diabetes, Digestive, & Kidney Diseases (US). (1998). Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report (No. 98). National Heart, Lung, and Blood Institute.
Nightingale, S. (2012). Autism spectrum disorders. Nature Reviews Drug Discovery, 11(10), 745.
O’Brien, G., & Pearson, J. (2004). Autism and learning disability. Autism, 8(2), 125–140.
O’donoghue, G., Perchoux, C., Mensah, K., Lakerveld, J., Van Der Ploeg, H., Bernaards, C., … & Nazare, J. A. (2016). A systematic review of correlates of sedentary behaviour in adults aged 18–65 years: A socio-ecological approach. BMC Public Health, 16(1), 1–25.
Omorou, A. Y., Langlois, J., Lecomte, E., Briançon, S., & Vuillemin, A. (2016). Cumulative and bidirectional association of physical activity and sedentary behaviour with health-related quality of life in adolescents. Quality of Life Research, 25, 1169–1178.
Pan, C.-Y., & Frey, G. C. (2006). Physical activity patterns in youth with autism spectrum disorders. Journal of Autism and Developmental Disorders, 36(5), 597–606. https://doi.org/10.1007/s10803-006-0101-6
Piercy, K. L., Troiano, R. P., Ballard, R. M., Carlson, S. A., Fulton, J. E., Galuska, D. A., & Olson, R. D. (2018). The physical activity guidelines for Americans. JAMA, 320(19), 2020–2028.
Poirel, E. (2017). Psychological benefits of physical activity for optimal mental health. Sante Mentale Au Quebec, 42(1), 147–164.
Rajendran, G., & Mitchell, P. (2007). Cognitive theories of autism. Developmental Review, 27(2), 224–260.
Rhodes, R. E., Janssen, I., Bredin, S. S. D., Warburton, D. E. R., & Bauman, A. (2017). Physical activity: Health impact, prevalence, correlates and interventions. Psychology & Health, 32(8), 942–975.
Rosenberg, D. E., Norman, G. J., Wagner, N., Patrick, K., Calfas, K. J., & Sallis, J. F. (2010). Reliability and validity of the Sedentary Behavior Questionnaire (SBQ) for adults. Journal of Physical Activity and Health, 7(6), 697–705.
Ross, R., Blair, S. N., Arena, R., Church, T. S., Després, J.-P., Franklin, B. A., Haskell, W. L., Kaminsky, L. A., Levine, B. D., & Lavie, C. J. (2016). Importance of assessing cardiorespiratory fitness in clinical practice: A case for fitness as a clinical vital sign: A scientific statement from the American Heart Association. Circulation, 134(24), e653–e699.
Saunders, T. J., McIsaac, T., Douillette, K., Gaulton, N., Hunter, S., Rhodes, R. E., Prince, S. A., Carson, V., Chaput, J.-P., & Chastin, S. (2020). Sedentary behaviour and health in adults: An overview of systematic reviews. Applied Physiology, Nutrition, and Metabolism, 45(10), S197–S217.
Shahane, V., Kilyk, A., & Srinivasan, S. M. (2024). Effects of physical activity and exercise-based interventions in young adults with autism spectrum disorder: A systematic review. Autism, 28(2), 276–300.
Shpigelman, C. N., Tal, A., & Zisman-Ilani, Y. (2021). Digital community inclusion of individuals with serious mental illness: A national survey to map digital technology use and community participation patterns in the digital era. JMIR Mental Health, 8(9), e28123.
Sowa, M., & Meulenbroek, R. (2012). Effects of physical exercise on autism spectrum disorders: A meta-analysis. Research in Autism Spectrum Disorders, 6(1), 46–57.
Stanish, H. I., Curtin, C., Must, A., Phillips, S., Maslin, M., & Bandini, L. G. (2017). Physical activity levels, frequency, and type among adolescents with and without autism spectrum disorder. Journal of Autism and Developmental Disorders, 47(3), 785–794.
Thorp, A. A., Owen, N., Neuhaus, M., & Dunstan, D. W. (2011). Sedentary behaviors and subsequent health outcomes in adults: A systematic review of longitudinal studies, 1996–2011. American Journal of Preventive Medicine, 41(2), 207–215.
Towne, S. D., Ory, M. G., Smith, M. L., Peres, S. C., Pickens, A. W., Mehta, R. K., & Benden, M. (2017). Accessing physical activity among young adults attending a university: The role of sex, race/ethnicity, technology use, and sleep. BMC Public Health, 17(1), 721.
Tremblay, M. S., Aubert, S., Barnes, J. D., Saunders, T. J., Carson, V., Latimer-Cheung, A. E., & Chinapaw, M. J. (2017). Sedentary behavior research network (SBRN)–terminology consensus project process and outcome. International Journal of Behavioral Nutrition and Physical Activity, 14, 1–17.
Tyler, C. V., Schramm, S. C., Karafa, M., Tang, A. S., & Jain, A. K. (2011). Chronic disease risks in young adults with autism spectrum disorder: Forewarned is forearmed. American Journal on Intellectual and Developmental Disabilities, 116(5), 371–380. https://doi.org/10.1352/1944-7558-116.5.371
Van Heijst, B. F. C., & Geurts, H. M. (2015). Quality of life in autism across the lifespan: A meta-analysis. Autism, 19(2), 158–167.
WHOQOL Group. (1998). Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological Medicine, 28(3), 551–558.
Wilmot, E. G., Edwardson, C. L., Achana, F. A., Davies, M. J., Gorely, T., Gray, L. J., & Biddle, S. J. (2012). Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia, 55(11), 2895–2905.
Woessner, M. N., Tacey, A., Levinger-Limor, A., Parker, A. G., Levinger, P., & Levinger, I. (2021). The evolution of technology and physical inactivity: The good, the bad, and the way forward. Frontiers in Public Health, 9, 655491.
Acknowledgements
The authors are grateful for the commitment from our study participants and other autistic volunteers who supported our survey pretesting efforts by sharing their perspectives and lived experiences that helped us design an autism-friendly survey.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflict of interest to declare, and no grant funding was received for conducting this research.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki, and the Institutional Review Board at Indiana University approved this study.
Informed Consent
All participants provided electronic informed consent prior to their study participation.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lee, D., Cothran, D.J., Kennedy, J.M. et al. Association Between Physical Activity, Sedentary Time, and Technology Use in Autistic Adults. J Dev Phys Disabil (2024). https://doi.org/10.1007/s10882-024-09983-3
Accepted:
Published:
DOI: https://doi.org/10.1007/s10882-024-09983-3